
Is Metagenomics the Future Routine Diagnosis Tool for Brain Abscesses? About a Case
 , , ,
, , ,
Abstract
:1. Introduction
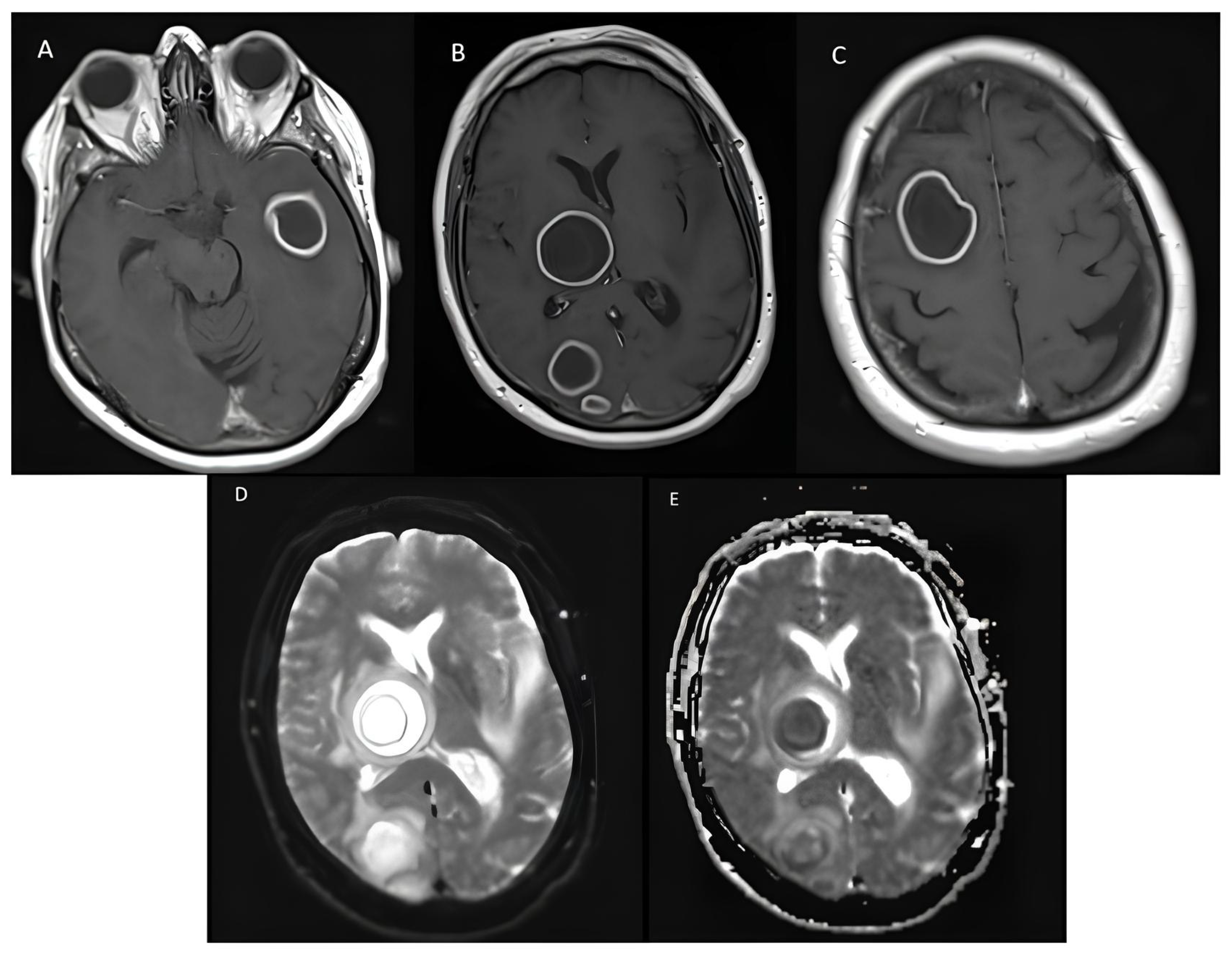
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Brouwer, M.C.; Coutinho, J.M.; van de Beek, D. Clinical characteristics and outcome of brain abscess: Systematic review and meta-analysis. Neurology 2014, 82, 806–813. [Google Scholar] [CrossRef]
- Sonneville, R.; Ruimy, R.; Benzonana, N.; Riffaud, L.; Carsin, A.; Tadié, J.M.; Piau, C.; Revest, M.; Tattevin, P.; The ESCMID Study Group for Infectious Diseases of the Brain (ESGIB). An update on bacterial brain abscess in immunocompetent patients. Clin. Infect. Dis. 2017, 23, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Jary, A.; Hua, C.; Woerther, P.-L.; Bosc, R.; Desroches, M.; Sitterlé, E.; Gricourt, G.; De Prost, N.; Pawlotsky, J.-M.; et al. Pathogen identification by shotgun metagenomics of patients with necrotizing soft-tissue infections. Br. J. Dermatol. 2020, 183, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.X.; Li, B.; Yang, H.F.; Du, Y.; Li, Y.; Wang, W.X.; Zheng, H.J.; Gong, Q.Y. Can diffusion-weighted imaging be used to differentiate brain abscess from other ring-enhancing brain lesions? A meta-analysis. Clin Radiol. 2014, 69, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Al Masalma, M.; Lonjon, M.; Richet, H.; Dufour, H.; Roche, P.-H.; Drancourt, M.; Raoult, D.; Fournier, P.-E. Metagenomic analysis of brain abscesses identifies specific bacterial associations. Clin. Infect. Dis. 2012, 54, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, C.; Surgers, L.; Fihman, V.; Gricourt, G.; Demontant, V.; Trawinski, E.; N’debi, M.; Gomart, C.; Royer, G.; Launay, N.; et al. Prospective comparison between shotgun metagenomics and Sanger sequencing of the 16S rRNA gene for the etiological diagnosis of infections. Front. Microbiol. 2022, 13, 761873. [Google Scholar] [CrossRef]
- Filkins, L.M.; Bryson, A.L.; Miller, S.A.; Mitchell, S.L. Navigating clinical utilization of direct-from-specimen metagenomic pathogen detection: Clinical applications, limitations, and testing recommendations. Clin. Chem. 2020, 66, 1381–1395. [Google Scholar] [CrossRef]
- Gu, W.; Deng, X.; Lee, M.; Sucu, Y.D.; Arevalo, S.; Stryke, D.; Federman, S.; Gopez, A.; Reyes, K.; Zorn, K.; et al. Rapid pathogen detection by metagenomic next-generation sequencing of infected body fluids. Nat. Med. 2021, 27, 115–124. [Google Scholar] [CrossRef]
- Wilson, M.R.; Sample, H.A.; Zorn, K.C.; Arevalo, S.; Yu, G.; Neuhaus, J.; Federman, S.; Stryke, D.; Briggs, B.; Langelier, C.; et al. Clinical metagenomic sequencing for diagnosis of meningitis and encephalitis. N. Engl. J. Med. 2019, 380, 2327–2340. [Google Scholar] [CrossRef]
- Zhou, H.; Larkin, P.M.; Zhao, D.; Ma, Q.; Yao, Y.; Wu, X.; Wang, J.; Zhou, X.; Li, Y.; Wang, G.; et al. Clinical impact of metagenomic next-generation sequencing of bronchoalveolar lavage in the diagnosis and management of pneumonia. J. Mol. Diagn. 2021, 23, 1259–1268. [Google Scholar] [CrossRef]
- Grumaz, S.; Stevens, P.; Grumaz, C.; Decker, S.O.; Weigand, M.A.; Hofer, S.; Brenner, T.; von Haeseler, A.; Sohn, K. Next-generation sequencing diagnostics of bacteremia in septic patients. Genome Med. 2016, 8, 73. [Google Scholar] [CrossRef]
- Thoendel, M.J.; Jeraldo, P.R.; Greenwood-Quaintance, K.E.; Yao, J.Z.; Chia, N.; Hanssen, A.D.; Abdel, M.P.; Patel, R. Identification of prosthetic joint infection pathogens using a shotgun metagenomics approach. Clin. Infect. Dis. 2018, 67, 1333–1338. [Google Scholar] [CrossRef]
- Zhao, M.; Tang, K.; Liu, F.; Zhou, W.; Fan, J.; Yan, G.; Qin, S.; Pang, Y. Metagenomic next-generation sequencing improves diagnosis of osteoarticular infections from abscess specimens: A multicenter retrospective study. Front. Microbiol. 2020, 11, 2034. [Google Scholar] [CrossRef] [PubMed]
- Miao, Q.; Ma, Y.; Wang, Q.; Pan, J.; Zhang, Y.; Jin, W.; Yao, Y.; Su, Y.; Huang, Y.; Wang, M.; et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin. Infect. Dis. 2018, 67 (Suppl. S2), S231–S240. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Wu, H.; Ruan, Q.; Jiang, N.; Chen, X.; Shen, Y.; Zhu, Y.M.; Ying, Y.; Qian, Y.Y.; Wang, X.; et al. Clinical Evaluation of Diagnosis Efficacy of Active Mycobacterium tuberculosis Complex Infection via Metagenomic Next-Generation Sequencing of Direct Clinical Samples. Front. Cell Infect. Microbiol. 2019, 9, 351. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.L.; Guo, L.Y.; Wu, H.L.; Feng, W.Y.; Chen, T.M.; Liu, G. Evaluation of next-generation sequencing for the pathogenic diagnosis of children brain abscesses. J. Infect. 2019, 78, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Yan, S.; Dong, H.; Wang, H.; Luo, Y.; Wang, X. Case report: Metagenomics next-generation sequencing can help define the best therapeutic strategy for brain abscesses caused by oral pathogens. Front. Med. 2021, 8, 644130. [Google Scholar] [CrossRef]
- Zhou, C.; Wang, K.; Li, H.; Zhang, X. Idiopathic thrombocytopenic purpura with brain abscess caused by Nocardia farcinica diagnosed using metagenomics next-generation sequencing of the cerebrospinal fluid: A case report. BMC Infect. Dis. 2021, 21, 380. [Google Scholar] [CrossRef]
- Shishido, A.A.; Vostal, A.; Mayer, R.; Ho, C.; Baddley, J.W. Diagnosis of central nervous system invasive aspergillosis in a liver transplant recipient using microbial cell-free next generation DNA sequencing. Transpl. Infect. Dis. 2021, 23, e13592. [Google Scholar] [CrossRef]
- Huang, T.; Chen, Y.; Zhang, J.; He, R.; Qu, D.; Ye, Q.; Chen, X. Rapid and accurate diagnosis of brain abscess caused by Nocardia asiatica with a combination of Ziehl-Neelsen staining and metagenomics next-generation sequencing. Eur. J. Neurol. 2021, 28, 355–357. [Google Scholar] [CrossRef]
- Deng, S.; Zhu, H.; Li, Y.; Zhao, F.; Ocak, U.; Gong, Y. An unusual case report of brain abscess caused by Prevotella loescheii identified using the metagenomic next-generation sequencing. IDCases 2020, 20, e00758. [Google Scholar] [CrossRef]
- Gao, L.Y.; Xu, G.R.; Dai, T.J. Precision diagnosis and therapy of a case of brain abscesses associated with asymptomatic pulmonary arteriovenous fistulas. BMC Infect. Dis. 2020, 20, 370. [Google Scholar] [CrossRef]
- Yang, J.; Xie, S.; Li, J.; Xia, H.; Liu, X. Brain abscess caused by Nocardia farcinica and diagnosed by metagenomic next-generation sequencing: A case report. Front. Med. 2022, 9, 803554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhu, Y.; Wan, H. Case report: Multiple abscesses caused by Porphyromonas gingivalis diagnosed by metagenomic next-generation sequencing. Front Med. 2023, 9, 1089863. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhuang, S.; He, L.; Wang, S.; Zhao, M.; Lyu, X. Brain Abscess Caused by Nocardia brevicatena in an Immunocompetent Patient: A Case Report. Infect. Drug Resist. 2022, 15, 7693–7697. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Ma, X.; Kang, Y.; Zhang, Z.; Zhang, Y.; Zhou, W.; Shen, H. Brain abscess caused by Scedosporium boydii in a systemic lupus erythematosus patient: A case report and literature review. Indian. J. Med. Microbiol. 2022, 40, 611–615. [Google Scholar] [CrossRef]
- Yao, L.; Chen, S.; Yu, Z.; Yu, T. Multifocal brain abscesses caused by invasive Streptococcus intermedia: A case report. Front. Neurol. 2022, 13, 893627. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Xue, X.H. Coinfection of Streptococcus suis and Nocardia asiatica in the human central nervous system: A case report. World J. Clin. Cases 2022, 10, 6283–6288. [Google Scholar] [CrossRef] [PubMed]
- Hirakata, S.; Sakiyama, Y.; Yoshimura, A.; Ikeda, M.; Takahata, K.; Tashiro, Y.; Yoshimura, M.; Arata, H.; Yonezawa, H.; Kirishima, M.; et al. The application of shotgun metagenomics to the diagnosis of granulomatous amoebic encephalitis due to Balamuthia mandrillaris: A case report. BMC Neurol. 2021, 21, 392. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.H.; He, X.J.; Nie, J.M.; Guan, S.S.; Chen, Y.K.; Liu, M. Central nervous system aspergillosis misdiagnosed as Toxoplasma gondii encephalitis in a patient with AIDS: A case report. AIDS Res. Ther. 2022, 19, 40. [Google Scholar] [CrossRef]
- Rodriguez, C.; Gricourt, G.; Ndebi, M.; Demontant, V.; Poiteau, L.; Burrel, S.; Boutolleau, D.; Woerther, P.L.; Calvez, V.; Stroer, S.; et al. Fatal Encephalitis Caused by Cristoli Virus, an Emerging Orthobunyavirus, France. Emerg. Infect. Dis. 2020, 26, 1287–1290. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Age | Sample | Active Antimicrobial Therapy Prior to Sampling | Culture Results | PCR Results | SMg Results | SMg Results Induced Change in Patient Management |
|---|---|---|---|---|---|---|---|
| Our case | 70-year old | Pus from brain abscess | Yes | Negative | 16S PCR: negative | Streptococcus anginosus, Fusobacterium nucleatum | Yes |
| Hu et al., 2019 [16] | 2-month old | Pus from brain abscess | Yes | Bacteroides fragilis | NA | Bacteroides fragilis | Yes |
| Hu et al., 2019 [16] | 5-year old | Pus from brain abscess | Yes | Streptococcus intermedius | NA | Streptococcus intermedius, Streptococus constellatus | Yes |
| Hu et al., 2019 [16] | 10-year old | Pus from brain abscess | Yes | Negative | NA | Streptococcus intermedius | Yes |
| Hu et al., 2019 [16] | 13-year old | Pus from brain abscess | Yes | Negative | NA | Prevotella oris, Fusobacterium nucleatum, Streptococcus intermedius | No |
| Ma et al., 2021 [17] | 75-year old | CSF | No prior to culture, Yes prior to SMg | Negative | NA | Prevotella denticola, Fusobacterium nucleatum | Yes |
| Zhou et al., 2021 [18] | 50-year old | CSF | No prior to culture, Yes prior to SMg | Negative | NA | Nocardia farcinica | Yes |
| Huang et al., 2021 [20] | 61-year old | Pus from brain abscess | Yes | Negative (Ziehl-Neelsen staining positive) | NA | Nocardia asiatica | Yes |
| Deng et al., 2020 [21] | 27-year old | Pus from brain abscess | Yes | Negative | NA | Prevotella loescheii | Yes |
| Yang et al., 2022 [23] | 58-year old | CSF | Yes | Positive | NA | Nocardia farcinica | Yes |
| Zhang et al., 2022 [24] | 65-year old | CSF | Yes | Negative | NA | Porphyromonas gingivalis | Yes |
| Li et al., 2022 [25] | 49-year old | CSF | Yes | Positive | NA | Nocardia brevicatena | No |
| Gao et al., 2022 [26] | 30-year old | CSF | Yes | Positive | NA | Scedosporium boydii | No |
| Yao et al., 2022 [27] | 67-year old | CSF | Yes | Negative | NA | Streptococcus intermedia Nocardia asiatica | Yes |
| Chen et al., 2022 [28] | 66-year old | CSF | Yes | Negative | NA | Streptococcus suis | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lars, W.; Lamoureux, C.; Picard, J.; Rodriguez, C.; Beauruelle, C.; Quaesaet, L.; Héry-Arnaud, G.; Ansart, S.; Coste, A. Is Metagenomics the Future Routine Diagnosis Tool for Brain Abscesses? About a Case. Biologics 2023, 3, 335-341. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics3040018
Lars W, Lamoureux C, Picard J, Rodriguez C, Beauruelle C, Quaesaet L, Héry-Arnaud G, Ansart S, Coste A. Is Metagenomics the Future Routine Diagnosis Tool for Brain Abscesses? About a Case. Biologics. 2023; 3(4):335-341. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics3040018
Chicago/Turabian StyleLars, William, Claudie Lamoureux, Jérémy Picard, Christophe Rodriguez, Clémence Beauruelle, Luc Quaesaet, Geneviève Héry-Arnaud, Séverine Ansart, and Anne Coste. 2023. "Is Metagenomics the Future Routine Diagnosis Tool for Brain Abscesses? About a Case" Biologics 3, no. 4: 335-341. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics3040018