
Serum Metabolic Profiling Identifies Key Differences between Patients with Single-Ventricle Heart Disease and Healthy Controls

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Blood Processing
2.3. Metabolomic Analyses
2.4. Data Integration and Statistical Analyses
3. Results
3.1. Patient Characteristics
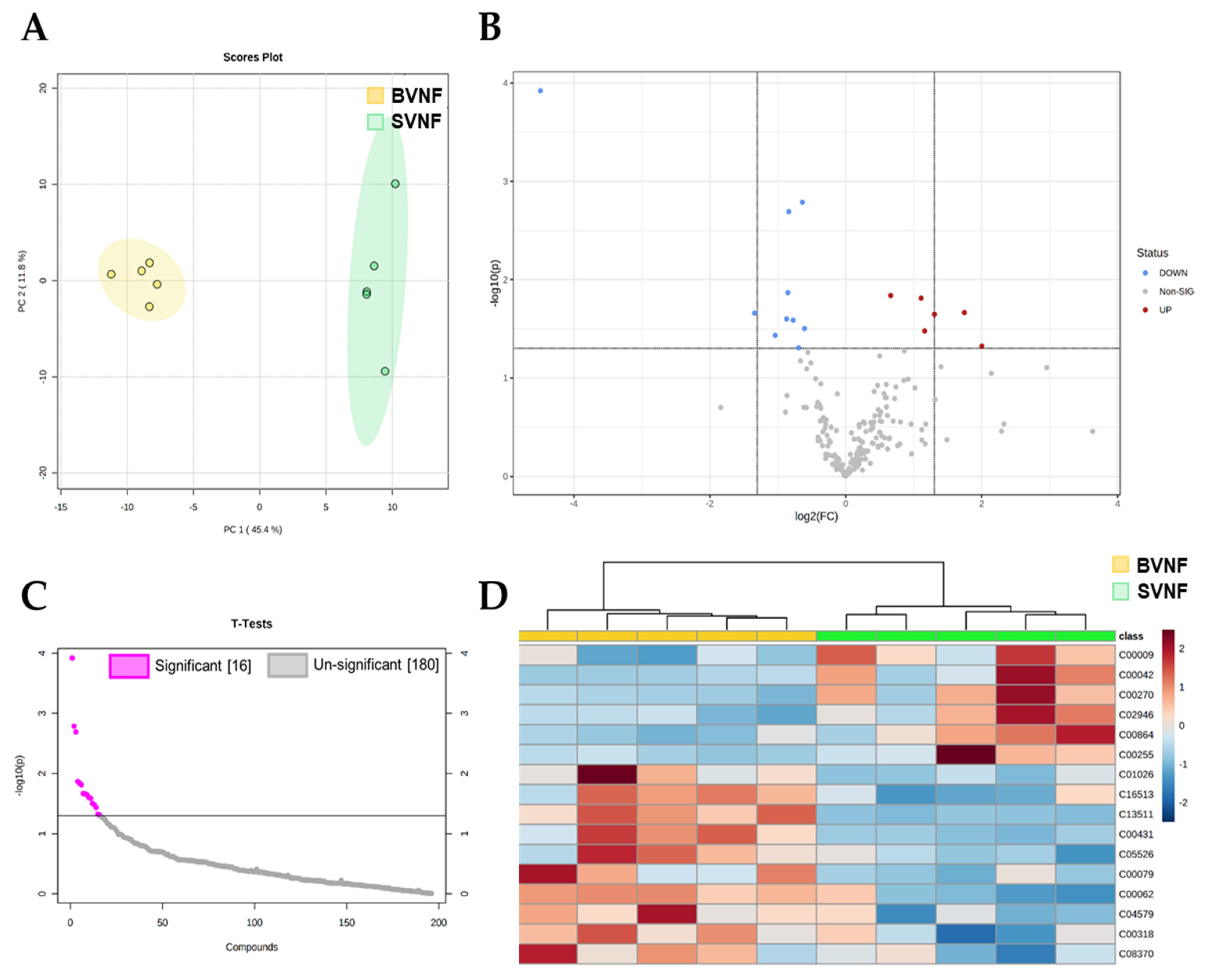
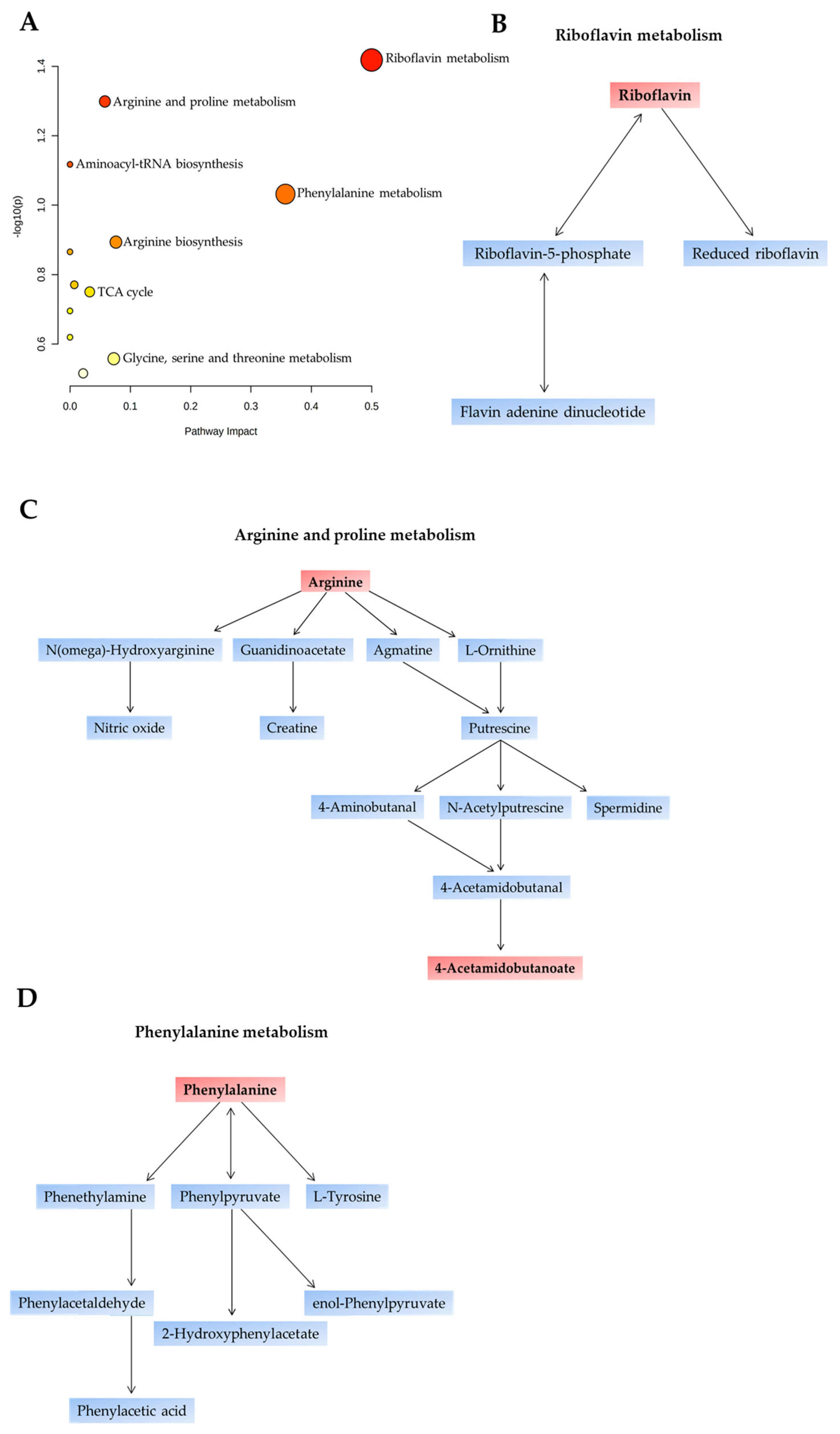
3.2. Metabolomic Profiling of Serum Circulating Factors Identified Dysregulated Amino Acid Metabolism in SVNF Subjects
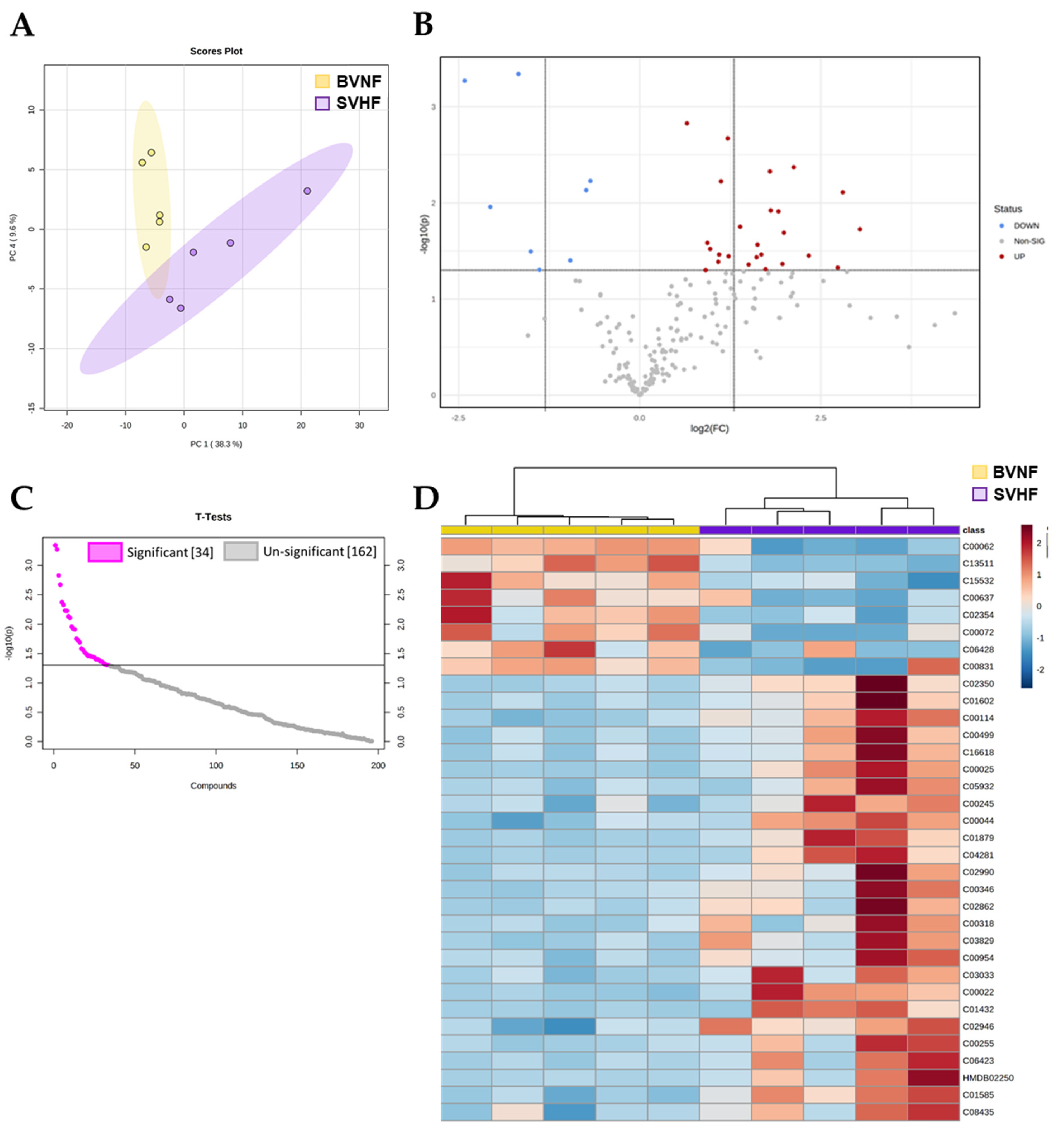
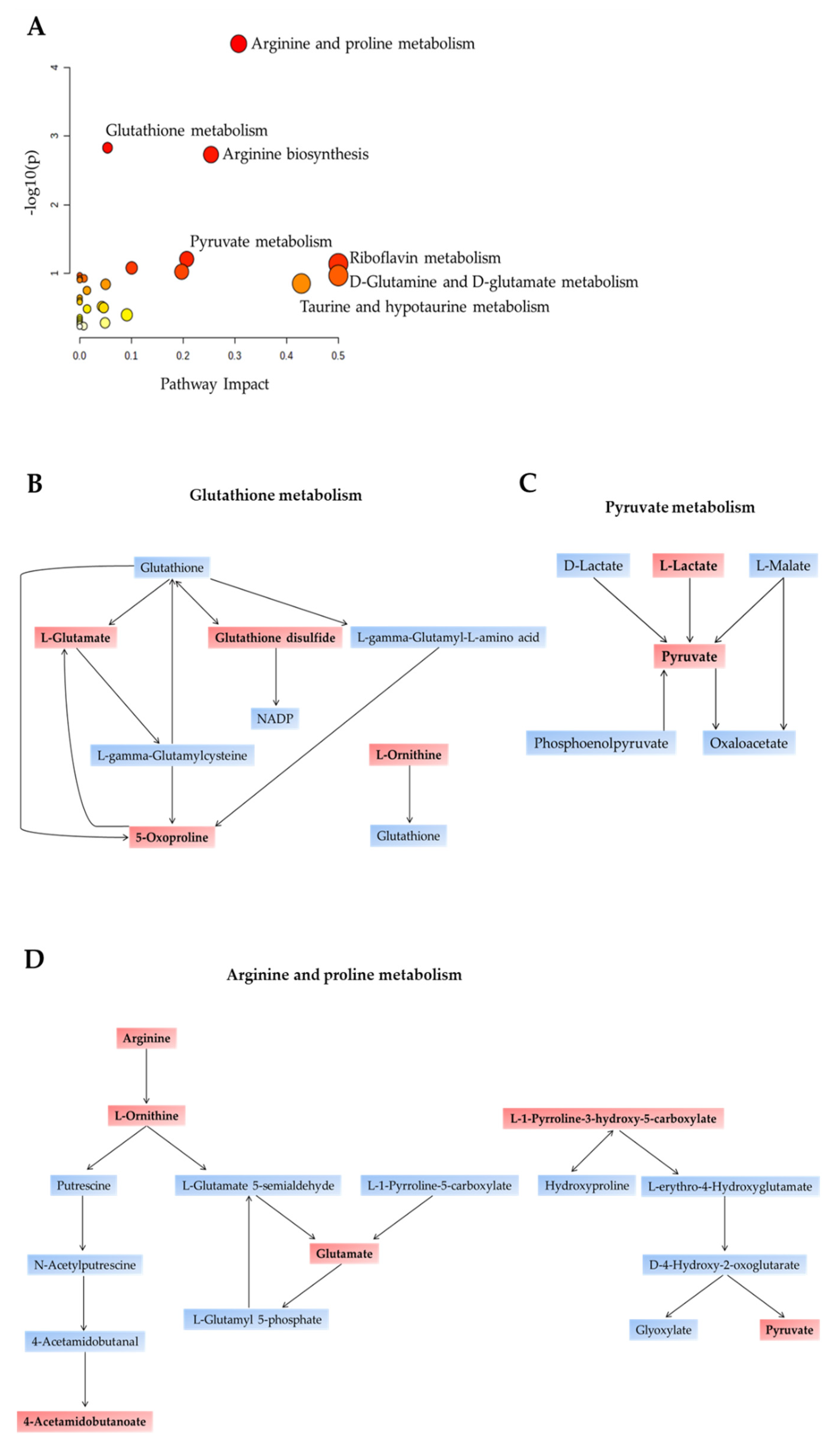
3.3. Metabolomic Profiling of Serum Circulating Factors Identified Dysregulated Amino Acid, Pyruvate and Antioxidant Metabolism in SVHF Subjects
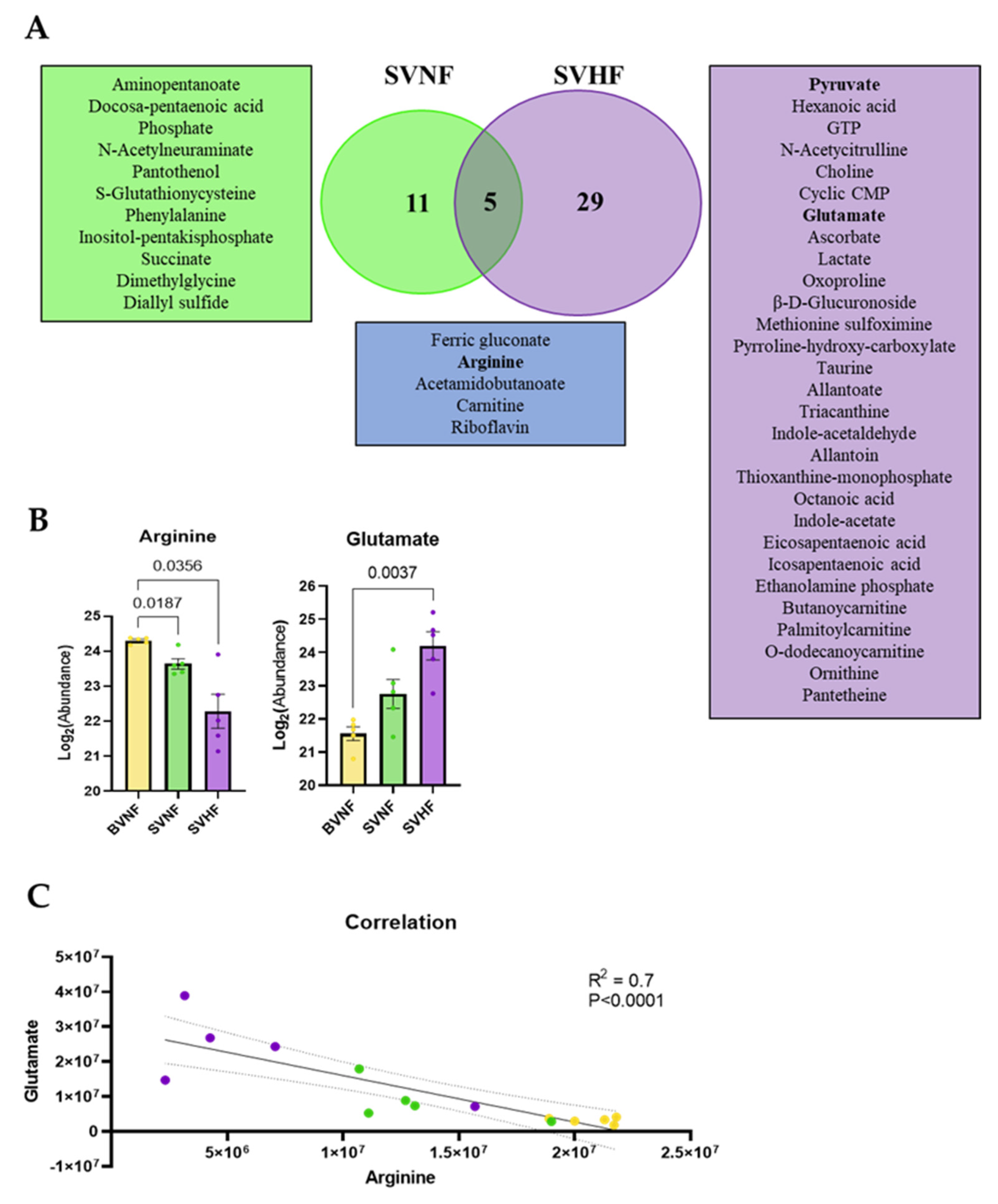
3.4. Metabolomic Profiling of Serum Circulating Factors Discriminated between SVNF and SVHF Subjects
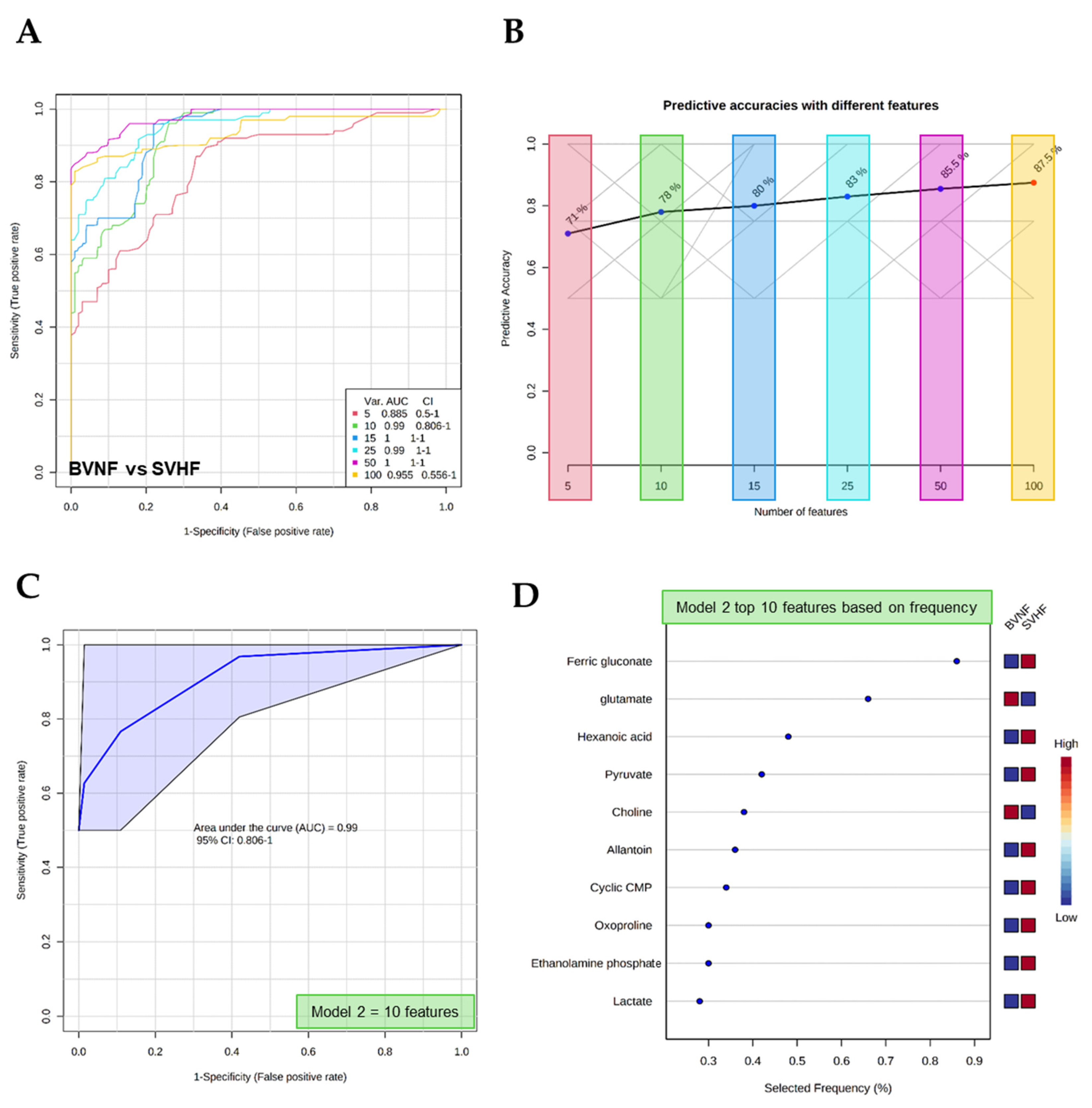
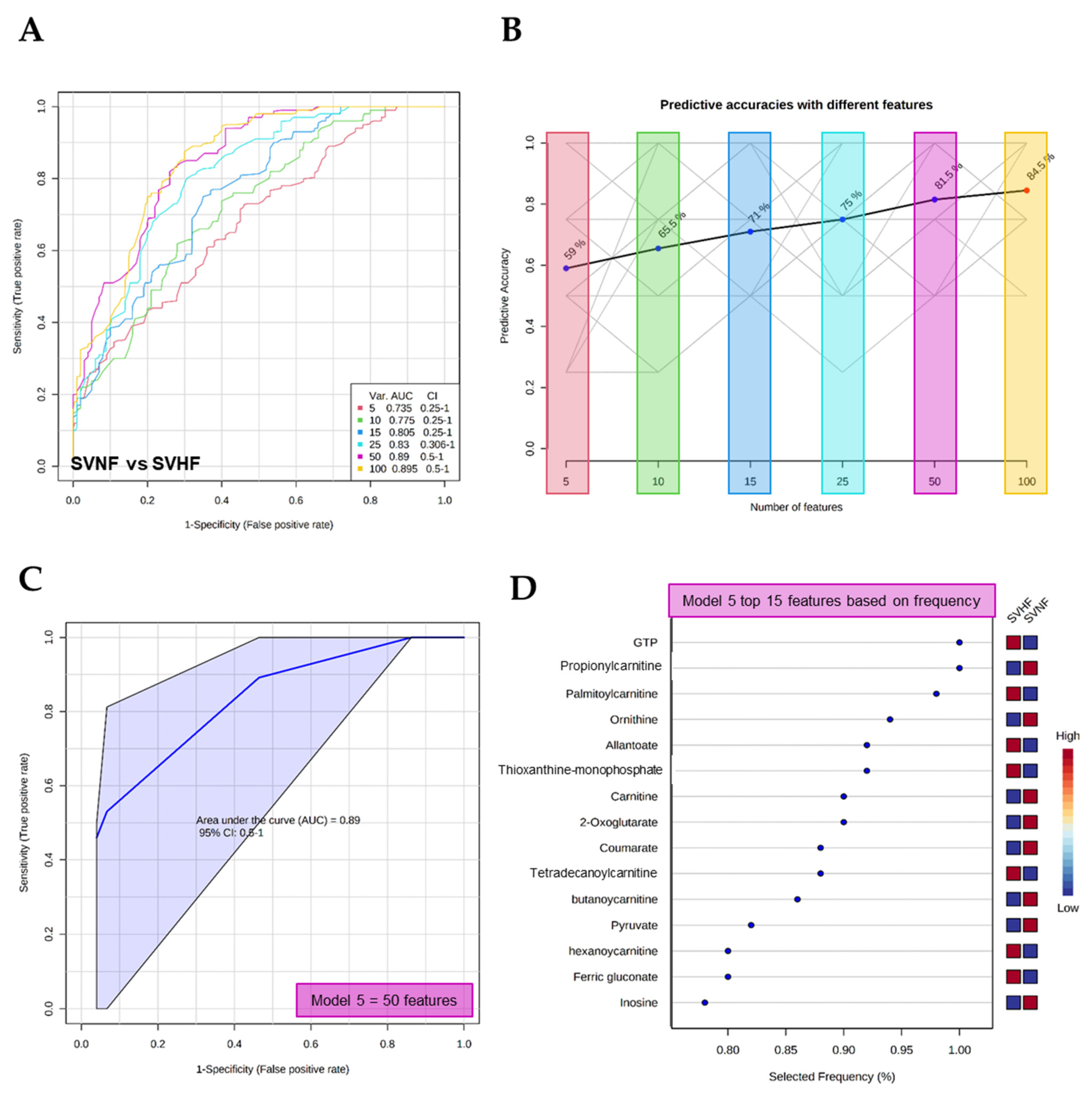
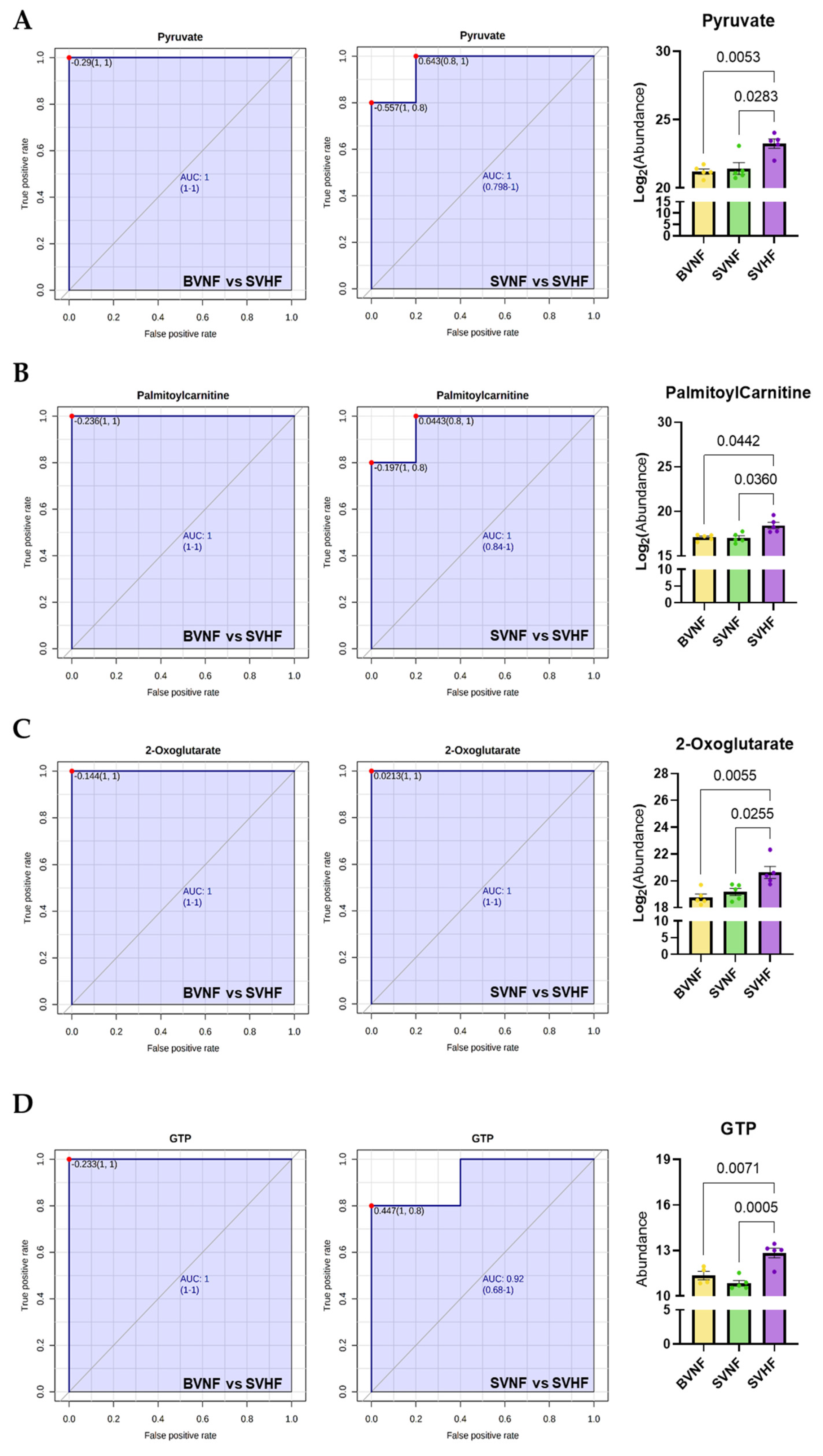
3.5. Metabolomics Profiling as a Diagnostic, Prognostic, or Monitoring Tool
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coats, L.; O’Connor, S.; Wren, C.; O’Sullivan, J. The single-ventricle patient population: A current and future concern a population-based study in the North of England. Heart 2014, 100, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Julsrud, P.R.; Weigel, T.J.; Van Son, J.A.; Edwards, W.D.; Mair, D.D.; Driscoll, D.J.; Danielson, G.K.; Puga, F.J.; Offord, K.P. Influence of ventricular morphology on outcome after the Fontan procedure. Am. J. Cardiol. 2000, 86, 319–323. [Google Scholar] [CrossRef]
- McGuirk, S.P.; Winlaw, D.S.; Langley, S.M.; Stumper, O.F.; De Giovanni, J.V.; Wright, J.G.; Brawn, W.J.; Barron, D.J. The impact of ventricular morphology on midterm outcome following completion total cavopulmonary connection. Eur. J. Cardio-Thoracic Surg. 2003, 24, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.A.; Sleeper, L.A.; Mahony, L.; Colan, S.D.; Atz, A.M.; Breitbart, R.E.; Gersony, W.M.; Gallagher, D.; Geva, T.; Margossian, R.; et al. Contemporary Outcomes After the Fontan Procedure: A Pediatric Heart Network Multicenter Study. J. Am. Coll. Cardiol. 2008, 52, 85–98. [Google Scholar] [CrossRef] [Green Version]
- Alsoufi, B.; Manlhiot, C.; Awan, A.; Alfadley, F.; Al-Ahmadi, M.; Al-Wadei, A.; McCrindle, B.W.; Al-Halees, Z. Current outcomes of the Glenn bidirectional cavopulmonary connection for single ventricle palliation. Eur. J. Cardio-Thoracic Surg. 2012, 42, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Backer, C.L. The functionally univentricular heart: Which is better--right or left ventricle? J. Am. Coll. Cardiol. 2012, 59, 1186–1187. [Google Scholar] [CrossRef]
- D’Udekem, Y.; Xu, M.Y.; Galati, J.C.; Lu, S.; Iyengar, A.J.; Konstantinov, I.E.; Wheaton, G.R.; Ramsay, J.M.; Grigg, L.E.; Millar, J.; et al. Predictors of Survival After Single-Ventricle Palliation: The Impact of Right Ventricular Dominance. J. Am. Coll. Cardiol. 2012, 59, 1178–1185. [Google Scholar] [CrossRef] [Green Version]
- Lotto, A.A.; Jones, T.J.; Brawn, W.J.; Hosein, R.; Barron, D.J. Outcome of the Norwood procedure in the setting of transposition of the great arteries and functional single left ventricle? Eur. J. Cardio-Thoracic Surg. 2009, 35, 149–155. [Google Scholar] [CrossRef]
- Kogon, B.E.; Plattner, C.; Leong, T.; Simsic, J.; Kirshbom, P.M.; Kanter, K.R. The bidirectional Glenn operation: A risk factor analysis for morbidity and mortality. J. Thorac. Cardiovasc. Surg. 2008, 136, 1237–1242. [Google Scholar] [CrossRef] [Green Version]
- Daebritz, S.H.; Nollert, G.D.; Zurakowski, D.; Khalil, P.N.; Lang, P.; Del Nido, P.J.; Mayer, J.E.; Jonas, R.A. Results of norwood stage I operation: Comparison of hypoplastic left heart syndrome with other malformations. J. Thorac. Cardiovasc. Surg. 2000, 119, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Alsoufi, B.; Gillespie, S.; Kim, D.; Shashidharan, S.; Kanter, K.; Maher, K.; Kogon, B. The Impact of Dominant Ventricle Morphology on Palliation Outcomes of Single Ventricle Anomalies. Ann. Thorac. Surg. 2016, 102, 593–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaddy, R.E.; Boucek, M.M.; Hsu, D.T.; Boucek, R.J.; Canter, C.E.; Mahony, L.; Ross, D.R.; Pahl, E.; Blume, E.D.; Dodd, D.A.; et al. Carvedilol for children and adolescents with heart failure: A randomized controlled trial. JAMA 2007, 298, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Hsu, D.T.; Zak, V.; Mahony, L.; Sleeper, L.A.; Atz, A.M.; Levine, J.C.; Barker, P.C.; Ravishankar, C.; McCrindle, B.W.; Williams, R.V.; et al. Enalapril in infants with single ventricle: Results of a multicenter randomized trial. Circulation 2010, 122, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Oldenburger, N.J.; Mank, A.; Etnel, J.; Takkenberg, J.J.M.; Helbing, W.A. Drug therapy in the prevention of failure of the Fontan circulation: A systematic review. Cardiol. Young 2016, 26, 842–850. [Google Scholar] [CrossRef]
- Dzau, V.J. Clinical implications for therapy: Possible cardioprotective effects of ACE inhibition. Br. J. Clin. Pharmacol. 1989, 28, 183S–187S. [Google Scholar] [CrossRef] [Green Version]
- Kenny, L.A.; Derita, F.; Nassar, M.; Dark, J.H.; Coats, L.; Hasan, A. Transplantation in the single ventricle population. Ann. Cardiothorac. Surg. 2018, 7, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Wishart, D.S. Emerging applications of metabolomics in drug discovery and precision medicine. Nat. Rev. Drug Discov. 2016, 15, 473–484. [Google Scholar] [CrossRef]
- Michel, M.; Dubowy, K.-O.; Entenmann, A.; Karall, D.; Adam, M.G.; Zlamy, M.; Komazec, I.O.; Geiger, R.; Niederwanger, C.; Salvador, C.; et al. Targeted metabolomic analysis of serum amino acids in the adult Fontan patient with a dominant left ventricle. Sci. Rep. 2020, 10, 8930. [Google Scholar] [CrossRef]
- Michel, M.; Dubowy, K.-O.; Zlamy, M.; Karall, D.; Adam, M.G.; Entenmann, A.; Keller, M.A.; Koch, J.; Komazec, I.O.; Geiger, R.; et al. Targeted metabolomic analysis of serum phospholipid and acylcarnitine in the adult Fontan patient with a dominant left ventricle. Ther. Adv. Chronic Dis. 2020, 11. [Google Scholar] [CrossRef]
- O’Connell, T.M.; Logsdon, D.L.; Mitscher, G.; Payne, R.M. Metabolic profiles identify circulating biomarkers associated with heart failure in young single ventricle patients. Metabolomics 2021, 17, 95. [Google Scholar] [CrossRef]
- Paridon, S.M.; Mitchell, P.D.; Colan, S.D.; Williams, R.V.; Blaufox, A.; Li, J.S.; Margossian, R.; Mital, S.; Russell, J.; Rhodes, J. A Cross-Sectional Study of Exercise Performance During the First 2 Decades of Life After the Fontan Operation. J. Am. Coll. Cardiol. 2008, 52, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alessandro, A.; Nemkov, T.; Kelher, M.; West, F.B.; Schwindt, R.K.; Banerjee, A.; Moore, E.E.; Silliman, C.C.; Hansen, K.C. Routine storage of red blood cell (RBC) units in additive solution-3: A comprehensive investigation of the RBC metabolome. Transfusion 2014, 55, 1155–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alessandro, A.; Moore, H.B.; Moore, E.E.; Wither, M.; Nemkov, T.; Gonzalez, E.; Slaughter, A.; Fragoso, M.; Hansen, K.C.; Silliman, C.C.; et al. Early hemorrhage triggers metabolic responses that build up during prolonged shock. Am. J. Physiol. Integr. Comp. Physiol. 2015, 308, R1034–R1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, J.; Psychogios, N.; Young, N.; Wishart, D.S. MetaboAnalyst: A web server for metabolomic data analysis and interpretation. Nucl. Acids Res. 2009, 37, W652–W660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, J.; Xia, J. MetaboAnalystR: An R package for flexible and reproducible analysis of metabolomics data. Bioinformatics 2018, 34, 4313–4314. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.; Kong, J.; Zhou, D.; Lai, M.; Chen, Y.; Xie, D.; Wang, X.; Wang, D. Serum metabolic characteristics and biomarkers of early-stage heart failure. Biomark. Med. 2020, 14, 119–130. [Google Scholar] [CrossRef]
- Zordoky, B.; Sung, M.M.; Ezekowitz, J.; Mandal, R.; Han, B.; Bjorndahl, T.C.; Bouatra, S.; Anderson, T.; Oudit, G.Y.; Wishart, D.S.; et al. Metabolomic Fingerprint of Heart Failure with Preserved Ejection Fraction. PLoS ONE 2015, 10, e0124844. [Google Scholar] [CrossRef]
- Hunter, W.; Kelly, J.P.; McGarrah, R.W.; Khouri, M.G.; Craig, D.; Haynes, C.; Ilkayeva, O.; Stevens, R.D.; Bain, J.R.; Muehlbauer, M.J.; et al. Metabolomic Profiling Identifies Novel Circulating Biomarkers of Mitochondrial Dysfunction Differentially Elevated in Heart Failure with Preserved Versus Reduced Ejection Fraction: Evidence for Shared Metabolic Impairments in Clinical Heart Failure. J. Am. Hear. Assoc. 2016, 5, e003190. [Google Scholar] [CrossRef] [Green Version]
- Hunter, W.G.; Kelly, J.P.; McGarrah, R.W.; Kraus, W.E.; Shah, S.H. Metabolic Dysfunction in Heart Failure: Diagnostic, Prognostic, and Pathophysiologic Insights from Metabolomic Profiling. Curr. Hear. Fail. Rep. 2016, 13, 119–131. [Google Scholar] [CrossRef] [Green Version]
- Nesterov, S.V.; Yaguzhinsky, L.S.; Podoprigora, G.I.; Nartsissov, Y.R. Amino Acids as Regulators of Cell Metabolism. Biochemistry (Mosc) [Internet]. Biochemistry 2020, 85, 393–408. [Google Scholar] [PubMed]
- Ueda, K.; Sanbongi, C.; Takai, S.; Ikegami, S.; Fujita, S. Combination of aerobic exercise and an arginine, alanine, and phenylalanine mixture increases fat mobilization and ketone body synthesis. Biosci. Biotechnol. Biochem. 2017, 81, 1417–1424. [Google Scholar] [CrossRef] [Green Version]
- Brittain, E.L.; Talati, M.; Fessel, J.P.; Zhu, H.; Penner, N.; Calcutt, M.W.; West, J.; Funke, M.; Lewis, G.D.; Gerszten, R.E.; et al. Fatty Acid Metabolic Defects and Right Ventricular Lipotoxicity in Human Pulmonary Arterial Hypertension. Circulation 2016, 133, 1936–1944. [Google Scholar] [CrossRef]
- Gray, L.R.; Tompkins, S.C.; Taylor, E.B. Regulation of pyruvate metabolism and human disease. Cell. Mol. Life Sci. 2014, 71, 2577–2604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Zhou, S.; Chen, C.; Ma, L.; Luo, D.; Tian, X.; Dong, X.; Zhou, Y.; Yang, Y.; Cui, Y. Therapeutic potential of pyruvate therapy for patients with mitochondrial diseases: A systematic review. Ther. Adv. Endocrinol. Metab. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-A.; Xu, Z.-H.; Huang, Y.-L.; Luo, Y.; Zhu, D.-J.; Wang, P.; Du, Z.-Y.; Yang, Y.; Wu, D.-H.; Lai, W.-Y.; et al. Increased serum 2-oxoglutarate associated with high myocardial energy expenditure and poor prognosis in chronic heart failure patients. Biochim. Biophys. Acta Mol. Basis Dis. 2014, 1842, 2120–2125. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | Sex | PDE3i | PDE5i | Non-PDEi Inotrope | Digoxin | ACEi | β-Blocker | Diuretic | Last Surgical Palliation | Indication for Blood Draw |
|---|---|---|---|---|---|---|---|---|---|---|
| Biventricular Non-Failing Control Subjects (BVNF) | ||||||||||
| 5.4 | M | N | N | N | N | N | N | N | - | control |
| 4.1 | M | N | N | N | N | N | N | N | - | control |
| 5.6 | F | N | N | N | N | N | N | N | - | control |
| 4.1 | M | N | N | N | N | N | N | N | - | control |
| 12.6 | M | N | N | N | N | N | N | N | - | control |
| Non-Failing Single Ventricle Subjects (SVNF) | ||||||||||
| 1.8 | F | N | N | N | N | N | N | N | Glenn/Hemi-Fontan | SVNF |
| 0.011 | F | N | N | N | N | N | N | N | Norwood | SVNF |
| 0.3 | M | N | N | N | N | N | N | N | Norwood | SVNF |
| 2.9 | F | N | N | N | N | N | N | Y | Glenn | SVNF |
| 0.6 | M | N | N | N | Y | N | N | Y | Norwood | SVNF |
| Failing Single Ventricle Subjects (SVHF) | ||||||||||
| 3.85 | F | Y | Y | Y | Y | Y | N | Y | Fontan | SV Systolic HF |
| 0.99 | F | Y | N | N | Y | Y | N | Y | Norwood | SV Systolic HF |
| 12.26 | M | N | N | N | Y | Y | N | N | Glenn/Hemi-Fontan | SV Systolic HF |
| 2.84 | F | Y | N | N | Y | Y | N | Y | Glenn | SV Systolic HF |
| 14.8 | M | N | Y | N | Y | Y | N | Y | Fontan | SV Systolic HF |
| Metabolite | Fold Change | p-Value |
|---|---|---|
| Alcohols and polyols | ||
| Inositol 1-2-3-5-6-pentakisphosphate | −1.749 | 0.026 |
| Amino acids | ||
| arginine | −1.677 | 0.002 |
| 5-Aminopentanoate | −1.802 | 0.002 |
| phenylalanine | −2.053 | 0.025 |
| Aminosugars | ||
| N-Acetylneuraminate | 2.135 | 0.015 |
| Arginine and proline metabolism | ||
| 4-Acetamidobutanoate | 2.009 | 0.023 |
| Carbohydrates and carbohydrate conjugates | ||
| Ferric gluconate | −17.737 | 0.000 |
| Carnitine and fatty acid metabolism | ||
| Carnitine | −1.373 | 0.031 |
| Essential fatty acids | ||
| Docosapentaenoic acid | −2.455 | 0.014 |
| GSH homeostasis | ||
| S-Glutathionycysteine | −2.463 | 0.022 |
| Organosulfur compounds | ||
| Diallyl sulfide | −1.432 | 0.049 |
| Panthothenate metabolism | ||
| Pantothenol | 4.590 | 0.022 |
| Phosphates | ||
| Phosphate | 1.585 | 0.014 |
| Pteridines and derivatives | ||
| Riboflavin | 4.032 | 0.047 |
| Serine biosynthesis and one-carbon metabolism | ||
| Dimethylglycine | −2.004 | 0.037 |
| TCA cycle | ||
| Succinate | 2.590 | 0.033 |
| Metabolite | Fold Change | p-Value |
|---|---|---|
| Amino acids | ||
| arginine | −5.000 | 0.000 |
| N-Acetycitrulline | −1.510 | 0.006 |
| 2′-3′-Cyclic CMP | −1.656 | 0.007 |
| glutamate | 7.232 | 0.008 |
| 2S-5S-Methionine sulfoximine | 14.341 | 0.019 |
| 1-Pyrroline-3-hydroxy-5-carboxylate | 2.927 | 0.020 |
| Arginine and proline metabolism | ||
| 4-Acetamidobutanoate | 1.925 | 0.002 |
| Azoles | ||
| (S)(+)-Allantoin | 1.850 | 0.034 |
| Carbohydrates and carbohydrate conjugates | ||
| Ferric gluconate | −6.264 | 0.001 |
| Carnitine and fatty acid metabolism | ||
| butanoycarnitine | 3.836 | 0.043 |
| Palmitoylcarnitine | 2.060 | 0.044 |
| O-dodecanoycarnitine | 5.895 | 0.047 |
| Carnitine | 1.963 | 0.050 |
| Coumarins and derivatives | ||
| Triacanthine | 1.884 | 0.030 |
| Essential fatty acids | ||
| (5Z-8Z-11Z-14Z-17Z)-Icosapentaenoic acid | −2.378 | 0.040 |
| Glycerophospholipid biosynthesis | ||
| Choline | 2.072 | 0.006 |
| Ethanolamine phosphate | 1.587 | 0.041 |
| Glycolysis | ||
| Pyruvate | 4.872 | 0.004 |
| Lactate | 4.311 | 0.012 |
| GSH homeostasis | ||
| Ascorbate | −51.419 | 0.011 |
| 5-Oxoproline | 2.925 | 0.012 |
| Indoles and derivatives | ||
| Indole-3-acetaldehyde | −4.636 | 0.032 |
| Indole-3-acetate | 1.982 | 0.037 |
| Nucleotides | ||
| GTP | 4.337 | 0.005 |
| Allantoate | 3.513 | 0.027 |
| Panthothenate metabolism | ||
| Pantetheine | −5.727 | 0.050 |
| Poly-unsaturated Fatty Acids | ||
| beta-D-Glucuronoside | 2.764 | 0.018 |
| Eicosapentaenoic acid | −2.378 | 0.040 |
| Pteridines and derivatives | ||
| Riboflavin | 5.492 | 0.035 |
| Pyrimidines and pyrimidine derivatives | ||
| 6-Thioxanthine 5--monophosphate | 4.433 | 0.034 |
| Saturated Fatty acids | ||
| Hexanoic acid (caproate) | 1.656 | 0.001 |
| Octanoic acid (caprylate) | 2.809 | 0.036 |
| Sulfur metabolism | ||
| Taurine | 1.859 | 0.026 |
| Urea cycle | ||
| Ornithine | 3.459 | 0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires da Silva, J.; Pietra, A.E.; Baybayon-Grandgeorge, A.N.; Garcia, A.M. Serum Metabolic Profiling Identifies Key Differences between Patients with Single-Ventricle Heart Disease and Healthy Controls. Int. J. Transl. Med. 2022, 2, 78-96. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm2010008
Pires da Silva J, Pietra AE, Baybayon-Grandgeorge AN, Garcia AM. Serum Metabolic Profiling Identifies Key Differences between Patients with Single-Ventricle Heart Disease and Healthy Controls. International Journal of Translational Medicine. 2022; 2(1):78-96. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm2010008
Chicago/Turabian StylePires da Silva, Julie, Ashley E. Pietra, Angela N. Baybayon-Grandgeorge, and Anastacia M. Garcia. 2022. "Serum Metabolic Profiling Identifies Key Differences between Patients with Single-Ventricle Heart Disease and Healthy Controls" International Journal of Translational Medicine 2, no. 1: 78-96. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm2010008