
Assessment of Surgical Difficulty in Patients with Rectal Cancer—The Impact of Pelvimetry
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
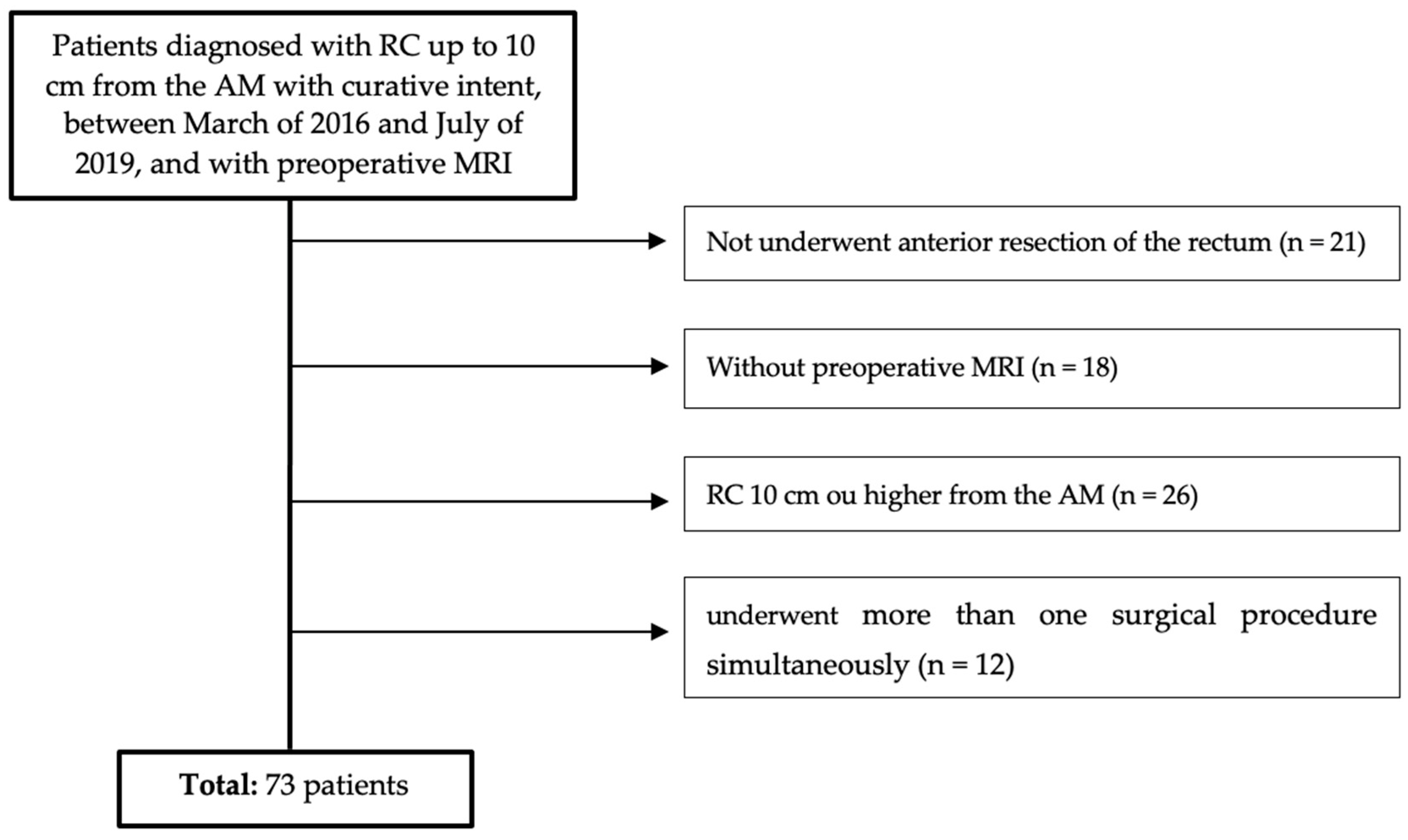
- -
- Patients diagnosed with RC up to 10 cm from the AM;
- -
- Patients underwent anterior resection of the rectum with curative intent, between March 2016 and July 2019;
- -
- With preoperative MRI.
- -
- Patients underwent more than one surgical procedure simultaneously;
- -
- Urgent or emergent surgery;
- -
- Presence of metastatic disease.
2.1. Data Collection
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
3.1. Predictive Model Validation
3.2. Creating a New Predictive Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okoshi, K.; Kono, E.; Tomizawa, Y.; Kinoshita, K. Can rectal washout reduce anastomotic recurrence after anterior resection for rectal cancer? A review of the literature. Surg. Today 2019, 50, 644–649. [Google Scholar] [CrossRef]
- Lindsetmo, R.; Joh, Y.; Delaney, C. Surgical treatment for rectal cancer: An international perspective on what the medical gastroenterologist needs to know. World J. Gastroenterol. WJG 2008, 14, 3281–3289. [Google Scholar] [CrossRef]
- Fazeli, M.; Keramati, M. Rectal cancer: A review. Med. J. Islam. Repub. Iran 2015, 29, 171. [Google Scholar] [PubMed]
- Klessen, C. Local staging of rectal cancer: The current role of MRI. Eur. Radiol. 2007, 17, 379–389. [Google Scholar] [CrossRef]
- Brown, G.; Kirkham, A.; Williams, G.T.; Bourne, M.; Radcliffe, A.G.; Sayman, J.; Newell, R.; Sinnatamby, C.; Heald, R.J. High-Resolution MRI of the Anatomy Important in Total Mesorectal Excision of the Rectum. Am. J. Roentgenol. 2013, 182, 431–439. [Google Scholar] [CrossRef]
- Jeyarajah, S.; Sutton, C.; Miller, A.; Hemingway, D. Factors that influence the adequacy of total mesorectal excision for rectal cancer. Color. Dis. 2007, 9, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, Y.; Kim, N.; Hur, H.; Lee, K.; Min, B.; Cho, H. Pelvic anatomy as a factor in laparoscopic rectal surgery: A prospective study. Surg. Laparosc. Endosc. Percutaneous Tech. 2011, 21, 334–339. [Google Scholar] [CrossRef]
- Parray, F.; Sofi, M.; Shaheen, F.; Chowdri, N.; Wani, R. Factors affecting operating time in resection of Rectal Cancer. Jms Ski. 2019, 21, 77–83. [Google Scholar] [CrossRef]
- Kawada, K.; Sakai, Y. Can we predict surgical difficulty of rectal surgery ? Ann. Laparosc. Endosc. Surg. 2018, 3, 44. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Kuroyanagi, H.; Oya, M.; Konishi, T.; Fukuda, M.; Fujimoto, Y.; Ueno, M.; Miyata, S.; Yamaguchi, T. Factors affecting the difficulty of laparoscopic total mesorectal excision with double stapling technique anastomosis for low rectal cancer. Surgery 2009, 146, 483–489. [Google Scholar] [CrossRef]
- Escal, L.; Nougaret, S.; Guiu, B.; Bertrand, M.M.; de Forges, H.; Tetreau, R.; Thézenas, S.; Rouanet, P. MRI-based score to predict surgical difficulty in patients with rectal cancer. Br. J. Surg. 2018, 105, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Salerno, G.; Daniels, I.; Brown, G.; Heald, R.; Moran, B. Magnetic resonance imaging pelvimetry in 186 patients with rectal cancer confirms an overlap in pelvic size between males and females. Color. Dis. 2006, 8, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Li, Q.; Fan, Y.; Li, D.; Jiang, L.; Qiu, P. Factors Predicting Difficulty of Laparoscopic Low Anterior Resection for Rectal Cancer with Total Mesorectal Excision and Double Stapling Technique. PLoS ONE 2016, 11, e0151773. [Google Scholar] [CrossRef]
- Bretagnol, F.; Panis, Y.; Rullier, E.; Rouanet, P.; Berdah, S.; Dousset, B.; Portier, G.; Benoist, S.; Chipponi, J.; Vicaut, E.; et al. Rectal cancer surgery with or without bowel preparation: The french greccar III multicenter single-blinded randomized trial. Ann. Surg. 2010, 252, 863–867. [Google Scholar] [CrossRef]
- Kim, H. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y. Biostatistics 102: Quantitative Data–Parametric & non-parametric tests. Singap. Med. J. 2003, 44, 391–396. [Google Scholar]
- Kumar, R.; Indrayan, A. Receiver Operating Characteristic (ROC) Curve for Medical Researchers. Indian. Pediatr. 2011, 48, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Boyle, K.M.; Petty, D.; Chalmers, A.G.; Quirke, P.; Cairns, A.; Finan, P.J.; Sagar, P.M.; Burke, D. MRI assessment of the bony pelvis may help predict resectability of rectal cancer. Color. Dis. 2005, 7, 232–240. [Google Scholar] [CrossRef]
- Ogiso, S.; Yamaguchi, T.; Hata, H.; Fukuda, M.; Ikai, I.; Yamato, T.; Sakai, Y. Evaluation of factors affecting the difficulty of laparoscopic anterior resection for rectal cancer: “Narrow pelvis” is not a contraindication. Surg. Endosc. 2011, 25, 1907–1912. [Google Scholar] [CrossRef]
- Targarona, E.M.; Balague, C.; Pernas, J.C.; Martinez, C.; Berindoague, R.; Gich, I.; Trias, M. Can we predict immediate outcome after laparoscopic rectal surgery? Multivariate analysis of clinical, anatomic, and pathologic features after 3-dimensional reconstruction of the pelvic anatomy. Ann. Surg. 2008, 247, 642–649. [Google Scholar] [CrossRef]
- Ferko, A.; Malý, O.; Örhalmi, J.; Dolejš, J. CT/MRI pelvimetry as a useful tool when selecting patients with rectal cancer for transanal total mesorectal excision. Surg. Endosc. 2016, 30, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Penninckx, F.; Fieuws, S.; Jouret-Mourin, A.; Sempoux, C.; Jehaes, C.; Van Eycken, E. Factors predicting the quality of total mesorectal excision for rectal cancer. Ann. Surg. 2010, 252, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Kawada, K.; Kiyasu, Y.; Itatani, Y.; Mizuno, R.; Hida, K.; Sakai, Y. Prediction of surgical difficulty in minimally invasive surgery for rectal cancer by use of MRI pelvimetry. BJS Open 2020, 4, 666–677. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | |
|---|---|
| Duration of surgery > 300 min | 3 points |
| Conversion to open procedure | 3 points |
| Use transanal dissetion | 2 points |
| Postoperative hospital stay > 15 days | 2 points |
| Blood loss > 200 ml | 1 point |
| Morbidity grade II and III (Clavien–DIndo classification) | 1 point |
| Total of Patients, n = 73 | |
|---|---|
| Gender (Male/Female), n (%) | 50 (68.5%):23 (31.5%) |
| Age (years) | 64 (37–88) |
| Body Mass Index (kg/m2) | 25.6 (17.3–37.3) |
| Preoperative therapy, n (%) | |
| Radiochemotherapy | 47 (64.4%) |
| No preoperative therapy | 26 (35.6%) |
| Tumor differentiation, n (%) | |
| Well differentiated | 37 (50.7%) |
| Moderately differentiated | 18 (24.7%) |
| Poorly differentiated | 1 (1.4%) |
| Pathological T category, n (%) | |
| ypT0 | 18 (24.7%) |
| ypT1 | 13 (17.8%) |
| ypT2 | 22 (30.1%) |
| ypT3 | 18 (24.7%) |
| ypT4 | 2 (2.7%) |
| Pathological N category, n (%) | |
| ypN0 | 57 (78.1%) |
| ypN1 | 12 (16.4%) |
| ypN2 | 4 (5.5%) |
| Mean ± Standard Deviation | |
|---|---|
| Interspinous distance (cm) | 9.70 ± 1.17 (7.45–12.4) |
| Intertuberous distance (cm) | 9.25 ± 1.24 (7.05–12.0) |
| Transverse diameter (cm) | 11.2 ± 1.33 (7.72–14.7) |
| Pelvic inlet (cm) | 10.7 ± 1.07 (7.9–13.0) |
| Pelvic depth (cm) | 12.3 ± 1.21 (10.1–14.6) |
| Pelvic outlet (cm) | 8.94 ± 1.01 (6.92–12.4) |
| Mesorectal fat area (cm2) | 20.7 ± 6.36 (4.80–33.9) |
| Total of Patients, n = 73 | |
|---|---|
| Surgical technique, n (%) | |
| Open | 19 (26.0%) |
| Laparoscopic | 54 (74.0%) |
| Surgical procedure, n (%) | |
| Colorectal anastomosis | 46 (63.0%) |
| Coloanal anastomosis | 13 (17.8%) |
| Terminal colostomy | 14 (19.2%) |
| Protective ileostomy, n (%) | |
| Sim | 22 (30.1%) |
| Não | 51 (69.9%) |
| Conversion to open procedure, n (%) | |
| Yes | 3 (4.1%) |
| No | 70 (95.9%) |
| Transanal dissection, n (%) | |
| Yes | 5 (6.8%) |
| No | 68 (93.2%) |
| Duration of surgery (Minutes; M ± SD) | 264.4 ± 8.5 |
| Blood loss, n (%) | |
| <200 mL | 56 (76.7%) |
| >200 mL | 17 (23.3%) |
| Postoperative hospital stay (Days; Mdn; IQR) | 6; 10 |
| Morbidity grade, n (%) | |
| No morbidity | 37 (50.7%) |
| I | 7 (9.6%) |
| II | 9 (12.3)% |
| IIIa | 12 (16.4%) |
| IIIb | 3 (4.1%) |
| IVa | 3 (4.1%) |
| IVb | 1 (1.4%) |
| V | 1 (1.4%) |
| Predictive Score < 6 | Predictive Score ≥ 6 | |
|---|---|---|
| Real score < 6 | 50 | 12 |
| Real score ≥ 6 | 9 | 2 |
| Low-Risk Group (n = 62) | High-Risk Group (n = 11) | p-Value | |
|---|---|---|---|
| Gender | |||
| Male | 39 (53.4%) | 11 (15.1%) | p = 0.013 |
| Female | 23 (31.5%) | 0 (0.0%) | |
| Age (Years; M ± SD) | 65.3 ± 12.3 | 58.6 ± 11.9 | p = 0.095 |
| BMI (kg/m2; M ± SD) | 25.5 ± 3.59 | 26.5 ± 3.73 | p = 0.403 |
| Preoperative therapy | |||
| Radiochemotherapy | 40 (54.8%) | 7 (9.6%) | p = 1.000 |
| No preoperative therapy | 22 (30.1%) | 4 (5.5%) | |
| Distance to the anal margin (cm; M ± SD) | 7.13 ± 2.50 | 7.86 ± 1.90 | p = 0.365 |
| Pathological T category | |||
| <ypT3 | 44 (60.3%) | 9 (12.3%) | p = 0.716 |
| ≥ypT3 | 18 (24.7%) | 2 (2.7%) | |
| Lymph Node—Positive | |||
| ypN0 | 48 (65.8%) | 9 (12.3%) | p = 1.000 |
| >ypN0 | 14 (19.2%) | 2 (2.7%) |
| Low-Risk Group (n = 62) | High-Risk Group (n = 11) | p-Value | |
|---|---|---|---|
| Interspinous distance (cm; M ± SD) | 9.84 ± 1.17 | 8.91 ± 0.81 | p = 0.014 |
| Intertuberous distance (cm; M ± SD) | 9.40 ± 1.26 | 8.40 ± 0.60 | p < 0.001 |
| Transverse diameter (cm; M ± SD) | 11.4 ± 1.15 | 9.97 ± 1.62 | p < 0.001 |
| Pelvic inlet (cm; M ± SD) | 10.7 ± 1.12 | 10.7 ± 0.74 | p = 0.774 |
| Pelvic depth (cm; M ± SD) | 12.2 ± 1.20 | 12.8 ± 1.19 | p = 0.109 |
| Pelvic outlet (cm; média ± M ± SD) | 9.00 ± 0.96 | 8.62 ± 0.96 | p = 0.257 |
| Mesorectal fat area (cm2; M ± SD) | 20.9 ± 6.30 | 19.6 ± 6.86 | p = 0.517 |
| Low-Risk Group (n = 62) | High-Risk Group (n = 11) | p-Value | |
|---|---|---|---|
| Surgical technique | |||
| Open | 18 (24.7%) | 1 (1.4%) | p = 0.268 |
| Laparoscopic | 44 (60.3%) | 10 (13.7%) | |
| Surgical procedure | |||
| (n = 59; LD = 48; HD = 11) | |||
| Colorectal anastomosis | 38 (64.4%) | 8 (13.6%) | p = 0.693 |
| Coloanal anastomosis | 10 (16.9%) | 3 (5.1%) | |
| Protective ileostomy | |||
| Yes | 17 (23.3%) | 5 (6.8%) | p = 0.289 |
| No | 45 (61.6%) | 6 (8.2%) |
| Variables | B | S.E | Wald | p | O.R | 95% CI |
|---|---|---|---|---|---|---|
| Constant | 11.270 | 4.491 | 6.297 | 0.012 | 78417.9 | |
| Interspinous distance | −0.001 | 0.052 | 0.000 | 0.991 | 0.999 | 0.903–1.107 |
| Intertuberous distance | −0.045 | 0.051 | 0.777 | 0.378 | 0.956 | 0.866–1.056 |
| Transversal diameter | −0.084 | 0.042 | 3.944 | 0.047 | 0.919 | 0.846–0.999 |
| Predictive Score < 6 | Predictive Score ≥ 6 | |
|---|---|---|
| Real score < 6 | 60 | 2 |
| Real score ≥ 6 | 9 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stuart, J.; Santos, P.M.D.d.; Pereira, C.C.; Martins, S.F. Assessment of Surgical Difficulty in Patients with Rectal Cancer—The Impact of Pelvimetry. Int. J. Transl. Med. 2024, 4, 163-175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm4010009
Stuart J, Santos PMDd, Pereira CC, Martins SF. Assessment of Surgical Difficulty in Patients with Rectal Cancer—The Impact of Pelvimetry. International Journal of Translational Medicine. 2024; 4(1):163-175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm4010009
Chicago/Turabian StyleStuart, João, Pedro Miguel Dias dos Santos, Carlos Costa Pereira, and Sandra F. Martins. 2024. "Assessment of Surgical Difficulty in Patients with Rectal Cancer—The Impact of Pelvimetry" International Journal of Translational Medicine 4, no. 1: 163-175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijtm4010009