
High Nutritional Vulnerability and Associated Risk Factors of Bangladeshi Wetland Community People Aged 50 Years and Older

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Permission for Data Collection
2.2. Research Design, Settings, Sampling, and Participants
2.3. Data Collection
2.4. Outcomes Measures
2.5. Outcome Measures of Related Health Indicators
2.6. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Mini Nutrition Assessment of Young and Older Adults Lived in Wetland Community
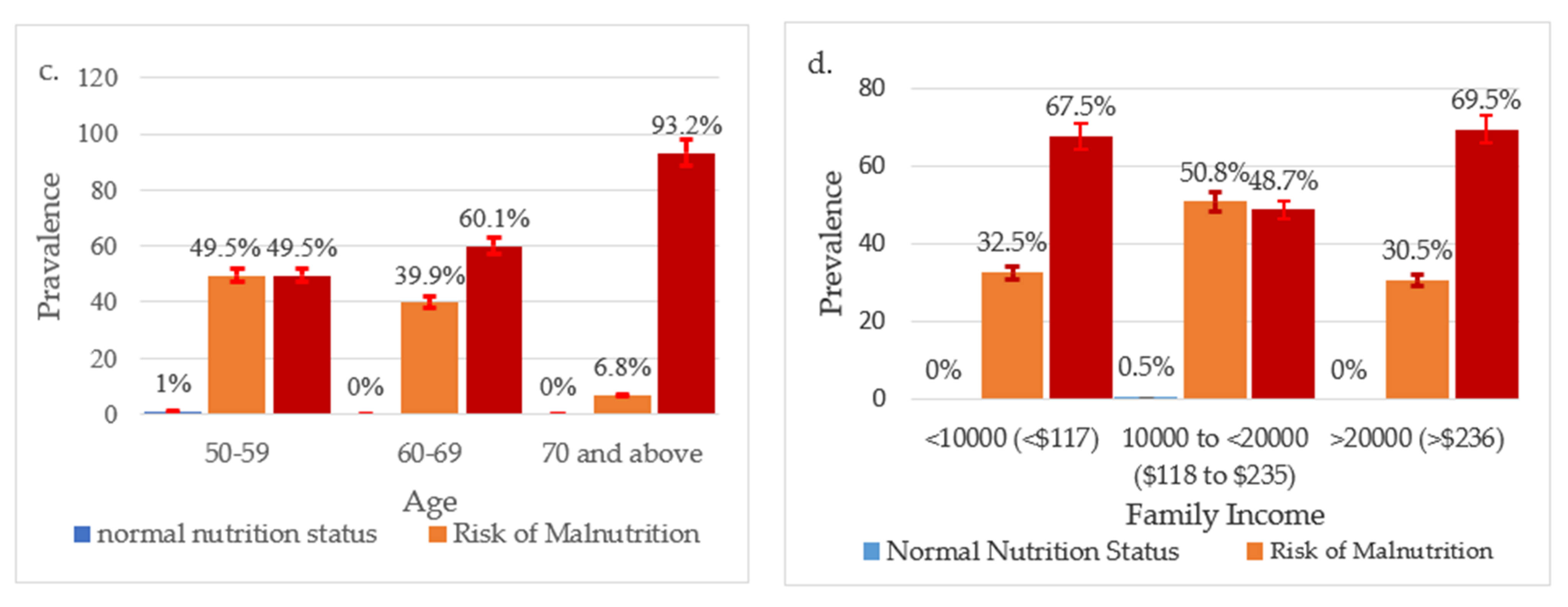
3.3. Socio-Demographic Risk Factors Related to Wetland Community-Dwelling Older Adult’s Nutrition
3.4. Health Factors Related to Wetland Community-Dwelling Older Adults’ Malnutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahman, K.M.T.; Khalequzzaman, M.; Khan, F.A.; Rayna, S.E.; Samin, S.; Hasan, M.; Islam, S.S. Factors associated with the nutritional status of the older population in a selected area of Dhaka, Bangladesh. BMC Geriatr. 2021, 21, 161. [Google Scholar] [CrossRef] [PubMed]
- Mastronuzzi, T.; Paci, C.; Portincasa, P.; Montanaro, N.; Grattagliano, I. Assessing the nutritional status of older individuals in family practice: Evaluation and implications for management. Clin. Nutr. 2015, 34, 1184–1188. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Hamiduzzaman, M.; Akter, M.; Farhana, Z.; Hossain, M.; Hasan, M.; Islam, M. Frailty indexed classification of Bangladeshi older adults’ physio-psychosocial health and associated risk factors- a cross-sectional survey study. BMC Geriatr. 2021, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Joymati, O.; Ningombam, M.; Rajkumari, B.; Gangmei, A. Assessment of nutritional status among elderly population in a rural area in Manipur: Community-based cross-sectional study. Int. J. Community Med. Public Health 2018, 5, 3125–3129. [Google Scholar]
- Clarke, L.H.; Korotchenko, A. Aging and the Body: A Review. Can. J. Aging 2014, 30, 495–510. [Google Scholar] [CrossRef] [PubMed]
- Hayes, G.; Jones, G. The Impact of the Demographic Transition on Socioeconomic Development in Bangladesh: Future Prospects and Implications for Public Policy. 2015. Available online: http://www.plancomm.gov.bd/wp-content/uploads/2015/02/22_Impact-of-Demographic-Transition-on-Socioeconomic-Development.pdf (accessed on 27 March 2022).
- Islam, M.Z.; Disu, T.R.; Farjana, S.; Rahman, M.M. Malnutrition and other risk factors of geriatric depression: A community-based comparative cross-sectional study in older adults in rural Bangladesh. BMC Geriatr. 2021, 21, 572. [Google Scholar] [CrossRef]
- Kohlmeier, M.; Nowson, C.A.; DiMaria-Ghalili, R.A.; Ray, S. Nutrition Education for the Health Care Professions. J. Biomed. Educ. 2015, 2015, 380917. [Google Scholar] [CrossRef] [Green Version]
- Vafaei, Z.; Mokhtari, H.; Sadooghi, Z.; Meamar, R.; Chitsaz, A.; Moeini, M. Malnutrition is associated with depression in rural elderly population. J. Res. Med. Sci. 2013, 18 (Suppl. 1), S15–S19. [Google Scholar]
- Spencer, P.S.; Palmer, V.S. Interrelationships of undernutrition and neurotoxicity: Food for thought and research attention. Neurotoxicology 2012, 33, 605–616. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.S.M.; Woo, J. Prevention of overweight and obesity: How effective is the current public health approach. Int. J. Environ. Res. Public Health 2010, 7, 765–783. [Google Scholar] [CrossRef] [Green Version]
- Paul, G.K.; Rahman, M.M.; Hamiduzzaman, M.; Farhana, Z.; Mondal, S.K.; Akter, S.; Naznin, S.; Islam, M.N. Hypertension and its physio-psychosocial risks factors in elderly people: A cross-sectional study in north-eastern region of Bangladesh. J. Geriatr. Cardiol. 2021, 18, 75–82. [Google Scholar] [PubMed]
- Chowdhury, M.Z.I.; Rahman, M.; Akter, T.; Akhter, T.; Ahmed, A.; Shovon, M.A.; Farhana, Z.; Chowdhury, N.; Turin, T.C. Hypertension prevalence and its trend in Bangladesh: Evidence from a systematic review and meta-analysis. Clin. Hypertens. 2020, 26, 10. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.Z.I.; Haque, M.A.; Farhana, Z.; Anik, A.M.; Chowdhury, A.H.; Haque, S.M.; Marjana, L.L.W.; Bristi, P.D.; Al Mamun, B.A.; Uddin, M.J.; et al. Prevalence of cardiovascular disease among Bangladeshi adult population: A systematic review and meta-analysis of the studies. Vasc. Health Risk Manag. 2018, 14, 165–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, M.Z.I.; Anik, A.M.; Farhana, Z.; Bristi, P.D.; Abu Al Mamun, B.M.; Uddin, M.J.; Fatema, J.; Akter, T.; Tani, T.A.; Rahman, M.; et al. Prevalence of metabolic syndrome in Bangladesh: A systematic review and meta-analysis of the studies. BMC Public Health 2018, 18, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.; Begum, M.; Uddin, M.; Rahman, M. Factors Affecting Health Status of Urban Aged Population: Evidence from Sylhet, Bangladesh. Indian J. Gerontol. 2018, 32, 103–118. [Google Scholar]
- Byomkesh, T.; Nakagoshi, N.; Shahedur, R.M. State and management of wetlands in Bangladesh. Landsc. Ecol. Eng. 2008, 5, 81. [Google Scholar] [CrossRef]
- Chaudhury, M. A Situation Analysis of Ecosystem Services and Poverty Linkages in Bangladesh; BRAC: Dhaka, Bangladesh, 2008. [Google Scholar]
- Shahed, S.S.; Rahman, M.M.; Misha, F.A. Building Resilience in the Char Area. J. Int. Dev. 2016, 1, 1–28. [Google Scholar]
- Food and Agriculture Organization of the United Nations. Scoping Agriculture–Wetland Interactions: Towards a Sustainable Multiple-Response Strategy; FAO: Rome, Italy, 2008. [Google Scholar]
- Yousuf Haroon, A.K.; Kibria, G. Wetlands: Biodiversity and Livelihood Values and Significance with Special Context to Bangladesh; Prusty, B., Chandra, R., Azeez, P., Eds.; Wetland Science Springer: New Delhi, India, 2007. [Google Scholar]
- Akter, R.; Thilsted, S.H.; Hossain, N.; Ishihara, H.; Yagi, N. Fish is the Preferred Animal-Source Food in the Rural Community of Southern Bangladesh. Sustainability 2019, 11, 5764. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, P.; Finlayson, C.M. Wetlands as Settings for Human Health: Incorporating Ecosystem Services and Health Impact Assessment into Water Resource Management. Bioscience 2011, 61, 678–688. [Google Scholar] [CrossRef]
- BRAC. Malnutrition Higher in Coastal and Haor Areas, Households Have 16% Less Income. 2018. Available online: https://www.brac.net/latest-news/item/1161-malnutrition-higher-in-coastal-and-haor-areas-households-have-16-less-income (accessed on 27 March 2022).
- Alam, M.B. Inequalities in access to primary education: An investigation on “haor” (wetland) areas in Bangladesh. In World Voices Nexus; WCCES: Ithaka, NY, USA, 2018. [Google Scholar]
- Das, S.; Mia, M.N.; Hanifi, S.M.A.; Hoque, S.; Bhuiya, A. Health literacy in a community with low levels of education: Findings from Chakaria, a rural area of Bangladesh. BMC Public Health 2017, 17, 203. [Google Scholar] [CrossRef] [Green Version]
- Agarwalla, R.; Saikia, A.M.; Baruah, R. Assessment of the nutritional status of the elderly and its correlates. J. Fam. Community Med. 2015, 22, 39–43. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Family Welfare. Bangladesh Essential Health Service Package (Esp); Ministry of Health and Family Welfare Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2016.
- Ministry of Health and Family Welfare. Bangladesh Health Observatory. Available online: https://dghs.gov.bd/index.php/en/data (accessed on 27 March 2022).
- UNFPA. Demographic Prognosis for South Asia: A Future of Rapid Ageing; United Nations Population Fund: Bangkok, Thailand, 2009. [Google Scholar]
- Bangladesh Bureau of Statistics. Population & Housing Census 2011, Zila Report: Sylhet. 2015. Available online: http://203.112.218.65:8008/WebTestApplication/userfiles/Image/PopCenZilz2011/Sylhet.pdf (accessed on 26 February 2022).
- BWDB. Perennial and Main Wetlands of Bangladesh; Ministry of Water Resources: Dhaka, Bangladesh, 2007.
- Bangladesh Bureau of Statistics. Bangladesh Population and Housing Census 2011, Volume 3: Urban Area Report. 2014; 657. Available online: http://www.bbs.gov.bd/WebTestApplication/userfiles/Image/NationalReports/PopulationHousingCensus2011.pdf (accessed on 27 February 2022).
- Platinum Dermatology. The Seven Signs of Ageing—Platinum Dermatology. 2016. Available online: https://platinumdermatology.com.au/articles/the-seven-signs-of-ageing/ (accessed on 27 March 2022).
- Bishwajit, G.; Tang, S.; Yaya, S.; Feng, Z. Participation in physical activity and back pain among an elderly population in South Asia. J. Pain Res. 2017, 10, 905–913. [Google Scholar]
- Galiana, L.; Gutiérrez, M.; Sancho, P.; Francisco, E.-H.; Tomás, J.M. Socio-Demographic Variables and Successful Aging of the Angolan Elderly. Scientifica 2016, 2016, 5306756. [Google Scholar] [CrossRef] [Green Version]
- Dartigues, J.F.; Helmer, C.; Letenneur, L. Socio-Demographic Risk Factors for Dementia and Alzheimer’s Disease in the Paquid Study. In Epidemiology of Alzheimer’s Disease: From Gene to Prevention; Research and Perspectives in Alzheimer’s Disease; Mayeux, R., Christen, Y., Eds.; Springer: Berlin/Heidelberg, Germany, 1999. [Google Scholar]
- Huhmann, M.B.; Perez, V.; Alexander, D.D.; Thomas, D.R. A self-completed nutrition screening tool for community-dwelling older adults with high reliability: A comparison study. J. Nutr. Health Aging 2013, 17, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Nestle Nutrition Institute. Mini Nutritional Assessment MNA; Nestle Nutrition Institute: La Tour-de-Peilz, Switzerland, 2009. [Google Scholar]
- Kabir, Z.N.; Ferdous, T.; Cederholm, T.; Khanam, M.A.; Streatfied, K.; Wahlin, Å. Mini Nutritional Assessment of rural elderly people in Bangladesh: The impact of demographic, socio-economic and health factors. Public Health Nutr. 2006, 9, 968–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BBS. Population and Housing Census, 2011. National Report, Volume 4, Bangladesh Bureau of Statistics (BBS). 2011. Available online: http://catalog.ihsn.org/index.php/catalog/4376 (accessed on 27 February 2022).
- Datta, P.B.; Islam, N.; Paul, G.K. Factors responsible for the health status of elderly people: A case study in Sylhet district. Int. J. Med. Health Res. 2018, 4, 72–77. [Google Scholar]
- Khan, N.; Mondal, N.I.; Hoque, N.; Islam, M.S. A study on quality of life of elderly population in Bangladesh. Am. J. Health Res. 2014, 2, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Uddin, M.T.; Islam, M.N.; Alam, M.J.; Bahar, G.U. Socio-Economic status of Elderly of Bangladesh: A Statistical Analysis. J. Appl. Sci. 2010, 10, 3060–3067. [Google Scholar] [CrossRef]
- Rahman, M.; Begum, M.; Rahman, M.; Uddin, M. Health status and modeling of urban aged population of Sylhet District in Bangladesh. Bioinform. Biostat. Agric. Health Environ. 2010, 2, 634–641. [Google Scholar]
- Hossain, Z.M.; Pal, A.; Hasan, A.M.; Parvej, S.M.; Nahar, N.; Asif, A.A. Nutritional status and socio-demographic characteristics of the people of south- west coastal region in Bangladesh. Asian Australas J. Biosci. Biotechnol. 2016, 1, 323–332. [Google Scholar]
- Masum, M.; Haqe, M.; Haque, M.; Saha, P.; Naser, M.; Mondal, S. Nutritional Status of an Aged Population in Selected Rural Area of Bangladesh. EC Nutr. 2015, 2, 278–282. [Google Scholar]
- Kaleem, S.; Parveen, S.A.; Mashori, A.; Bilal, A.; Aleem, K.; Tazeen, A.; Ayub, A. Malnutrition and its Risk Factors Particularly Family System in Elderly Population of Karachi. J. Med. Health Sci. 2014, 8, 72–75. [Google Scholar]
- Rathnayake, K.M.; Wimalathunga, M.; Weech, M.; Jackson, K.G.; Lovegrove, J.A. High prevalence of undernutrition and low dietary diversity in institutionalised elderly living in Sri Lanka. Public Health Nutr. 2015, 18, 2874–2880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamang, M.K.; Yadav, U.N.; Hosseinzadeh, H.; Kafle, B.; Paudel, G.; Khatiwada, S.; Sekaran, V.C. Nutritional assessment and factors associated with malnutrition among the elderly population of Nepal: A cross-sectional study. BMC Res. Notes 2019, 12, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damayanthi, H.D.W.T.; Moy, F.M.; Abdullah, K.L.; Dharmaratne, S.D. Prevalence of malnutrition and associated factors among community-dwelling older persons in Sri Lanka: A cross-sectional study. BMC Geriatr. 2018, 18, 199. [Google Scholar] [CrossRef]
- Kabir, Z.N.; Ferdous, T.; Cederholm, T.; Khanam, M.A.; Streatfied, K.; Wahlin, Å. Mini Nutritional Assessment of rural elderly people in Bangladesh: The impact of demographic, socio-economic and health factors–ERRATUM. Public Health Nutr. 2016, 19, 2290. [Google Scholar] [CrossRef] [Green Version]
- WHO. More than One in Three Low- and Middle-Income Countries Face Both Extremes of Malnutrition; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Akhtar, S. Malnutrition in South Asia—A Critical Reappraisal. Crit. Rev. Food Sci. Nutr. 2016, 56, 2320–2330. [Google Scholar] [CrossRef]
- Nugent, R.; Levin, C.; Hale, J.; Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet 2020, 395, 156–164. [Google Scholar] [CrossRef]
- Konda, S.; Ravi Kumar, B.P.; Giri, P.A. Prevalence of malnutrition and its determinants in an elderly people in South India. Int. J. Community Med. Public Health 2018, 5, 3570–3576. [Google Scholar] [CrossRef] [Green Version]
- Wells, J.L.; Dumbrell, A.C. Nutrition and aging: Assessment and treatment of compromised nutritional status in frail elderly patients. Clin. Interv. Aging 2006, 1, 67–79. [Google Scholar] [CrossRef]
- Rahman, M.M.; Bhattacharjee, B.; Farhana, Z.; Hamiduzzaman, M.; Chowdhury, M.A.B.; Hossain, M.S.; Siddiqee, M.H.; Islam, M.Z.; Raheem, E.; Uddin, M.J. Age-related Risk Factors and Severity of SARS-CoV-2 Infection: A systematic review and meta-analysis. J. Prev. Med. Hyg. 2021, 62, E329. [Google Scholar] [PubMed]
- Agarwal, E.; Miller, M.; Yaxley, A.; Isenring, E. Malnutrition in the elderly: A narrative review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Graham, J.E.; Mogilner, A.J.; Rockwood, K. Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr. 2002, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Mitnitski, A.; Song, X.; Rockwood, K. Improvement and decline in health status from late middle age: Modeling age-related changes in deficit accumulation. Exp. Gerontol. 2007, 42, 1109–1115. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, Y.; Jia, S.; Ge, M.; Hou, L.; Xia, X.; Liu, X.L.; Yue, J.R.; Dong, B.R. The association of sleep quality and sleep duration with nutritional status in older adults: Findings from the WCHAT study. Maturitas 2021, 145, 1–5. [Google Scholar] [CrossRef]
- Cao, Y.; Zhen, S.; Taylor, A.W.; Appleton, S.; Atlantis, E.; Shi, Z. Magnesium Intake and Sleep Disorder Symptoms: Findings from the Jiangsu Nutrition Study of Chinese Adults at Five-Year Follow-Up. Nutrients 2018, 10, 1354. [Google Scholar] [CrossRef] [Green Version]
- Goluch-Koniuszy, Z.; Fugiel, J.; Salmanowicz, M. A survey of dietary intake habits and nutritional status in women aged 60-90 years suffering from sleep disorders. Rocz. Panstw. Zakl. Hig. 2017, 68, 355–364. [Google Scholar]
- Al Anazi, N.H.; Carsula, R.P.; Tumala, R.B. Sociodemographic Determinants, Health Conditions, and Mental Status as Predictors of the Functional Status of Older Saudi People. J. Ageing Longev. 2022, 2, 1–11. [Google Scholar] [CrossRef]
- Zhao, M.; Tuo, H.; Wang, S.; Zhao, L. The Effects of Dietary Nutrition on Sleep and Sleep Disorders. Mediat. Inflamm. 2020, 2020, 3142874. [Google Scholar] [CrossRef]
- Soysal, P.; Smith, L.; Dokuzlar, O.; Isik, A.T. Relationship Between Nutritional Status and Insomnia Severity in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 1593–1598. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Indicators | Measurement Process | Used Instruments |
|---|---|---|
| Height (m) | -Stand without shoes and simple summer clothes -Look straight ahead and keep shoulders to level | Height measuring scale (Stadiometer) |
| Weight (Kg) | -Keeping normal summer clothes -Keeping the respondents simple as far as possible during the measurement | Weight measuring scale (Seca Digital) |
| BMI (Kg/m2) | Computer | |
| BP (mmHg.) | -Well seated -After 5 min’ rest -Average of three consecutive readings | Electronic BP Monitor (OMB) Model: BP-1307 |
| RBS (mmol/L) | -Time between breakfast and lunch -Time between lunch and dinner | Digital RBS Machine (VivacheckTM Ino.), Model: VGM01 |
| Characteristics | Frequency | Percentage | |
|---|---|---|---|
| Age | 50–59 | 198 | 49.5 |
| 60–69 | 143 | 35.8 | |
| 70+ | 59 | 14.8 | |
| Gender | Female | 162 | 40.5 |
| Male | 238 | 59.5 | |
| Education | Illiterate | 238 | 59.8 |
| Primary | 122 | 30.7 | |
| Above Primary | 38 | 9.5 | |
| Occupation | Public/Private Jobs | 109 | 27.5 |
| Fishing/Agriculture/Other Works | 288 | 72.5 | |
| Family Type | Nuclear | 227 | 56.7 |
| Joint | 129 | 32.2 | |
| Extended | 43 | 10.7 | |
| Monthly Income in Taka (Dollars, considering $1 = 84.79 BDT, Accessed: 6 November 2020) | <10,000 (<$117) | 126 | 33.3 |
| 10,000 to 19,999 ($118 to $235) | 195 | 51.2 | |
| >20,000 (>$236) | 59 | 5.9 | |
| Living arrangement | Single | 101 | 25.3 |
| Double | 283 | 70.9 | |
| Extended | 15 | 3.8 | |
| Characteristics | Malnutrition | At risk of Malnutrition | p-Value | |||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Education | Illiterate | 167 | 70.2 | 71 | 29.8 | 0.0001 *** |
| Primary | 48 | 40.0 | 72 | 60.0 | ||
| Above Primary | 23 | 60.5 | 15 | 39.5 | ||
| Gender | Female | 111 | 68.5 | 51 | 31.1 | 0.0001 *** |
| Male | 128 | 45.8 | 108 | 54.2 | ||
| Occupation | Public/Private Jobs | 44 | 41.1 | 63 | 58.9 | 0.0001 *** |
| Fishing/Agriculture/Other Works | 193 | 67 | 95 | 33.0 | ||
| Family Type | Nuclear | 126 | 55.8 | 100 | 44.2 | 0.001 *** |
| Joint | 76 | 58.9 | 53 | 41.1 | ||
| Extended | 37 | 86 | 6 | 14.0 | ||
| Age | 50–59 | 98 | 50 | 98 | 50 | 0.0001 *** |
| 60–69 | 57 | 39.9 | 86 | 60.1 | ||
| 70+ | 4 | 6.8 | 55 | 93.2 | ||
| Monthly Income in Taka (Dollars, considering $1 = 84.79 BDT, Accessed: 6 November 2020) | <10,000 (<$117) | 85 | 67.5 | 41 | 32.5 | 0.001 *** |
| 10,000 to 19,999 ($118 to $235) | 95 | 49.0 | 99 | 51.0 | ||
| >20,000 (>$236) | 41 | 69.5 | 18 | 30.5 | ||
| Characteristics | Screening Nutrition Status | p-Value | ||||
|---|---|---|---|---|---|---|
| Malnutrition | Risk of Malnutrition | |||||
| N | % | N | % | |||
| Health Status | Good | 131 | 50.8 | 127 | 49.2 | 0.000 |
| Not-good | 108 | 77.1 | 32 | 22.9 | ||
| Diabetes | Yes | 51 | 68.0 | 24 | 32.0 | 0.073 |
| No | 187 | 58.1 | 135 | 41.9 | ||
| Blood Pressure | High | 36 | 53.7 | 31 | 46.3 | 0.507 |
| Low | 92 | 60.9 | 59 | 39.1 | ||
| Normal | 111 | 61.7 | 69 | 38.3 | ||
| Sleeping Disorder | Yes | 122 | 53.2 | 104 | 46.8 | 0.004 |
| No | 116 | 66.0 | 55 | 34.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.M.; Farhana, Z.; Chowdhury, T.T.; Uddin, M.T.; Islam, M.Z.; Hamiduzzaman, M. High Nutritional Vulnerability and Associated Risk Factors of Bangladeshi Wetland Community People Aged 50 Years and Older. J. Ageing Longev. 2022, 2, 102-112. https://0-doi-org.brum.beds.ac.uk/10.3390/jal2020010
Rahman MM, Farhana Z, Chowdhury TT, Uddin MT, Islam MZ, Hamiduzzaman M. High Nutritional Vulnerability and Associated Risk Factors of Bangladeshi Wetland Community People Aged 50 Years and Older. Journal of Ageing and Longevity. 2022; 2(2):102-112. https://0-doi-org.brum.beds.ac.uk/10.3390/jal2020010
Chicago/Turabian StyleRahman, Mohammad Meshbahur, Zaki Farhana, Taniya Tajmin Chowdhury, Md Taj Uddin, Md. Ziaul Islam, and Mohammad Hamiduzzaman. 2022. "High Nutritional Vulnerability and Associated Risk Factors of Bangladeshi Wetland Community People Aged 50 Years and Older" Journal of Ageing and Longevity 2, no. 2: 102-112. https://0-doi-org.brum.beds.ac.uk/10.3390/jal2020010