Hygiene Behaviors and SARS-CoV-2-Preventive Behaviors in the Face of the COVID-19 Pandemic: Self-Reported Compliance and Associations with Fear, SARS-CoV-2 Risk, and Mental Health in a General Population vs. a Psychosomatic Patients Sample in Germany

 ,
,  ,
,
Abstract
:1. Introduction
- Keeping a distance of 1.5 m between humans;
- Avoiding mass gatherings;
- Wearing face masks;
- Complying with hand hygiene requirements [3].
1.1. COVID-19 Related Fear and Behavior
1.2. Relationship between Different Health Behaviors: Theoretical Explanation and Model
1.3. Research Questions
2. Materials and Methods
2.1. First Sample: Recruitment and Procedure of the General Population
2.2. Second Sample: Recruitment and Procedure of Psychosomatic Rehabilitation Patients
2.3. Instruments
2.3.1. Hygiene Behaviors
2.3.2. Fears of a SARS-CoV-2 Infection and COVID-19
2.3.3. Sociodemographic Characteristics
2.4. Statistical Analyses
3. Results
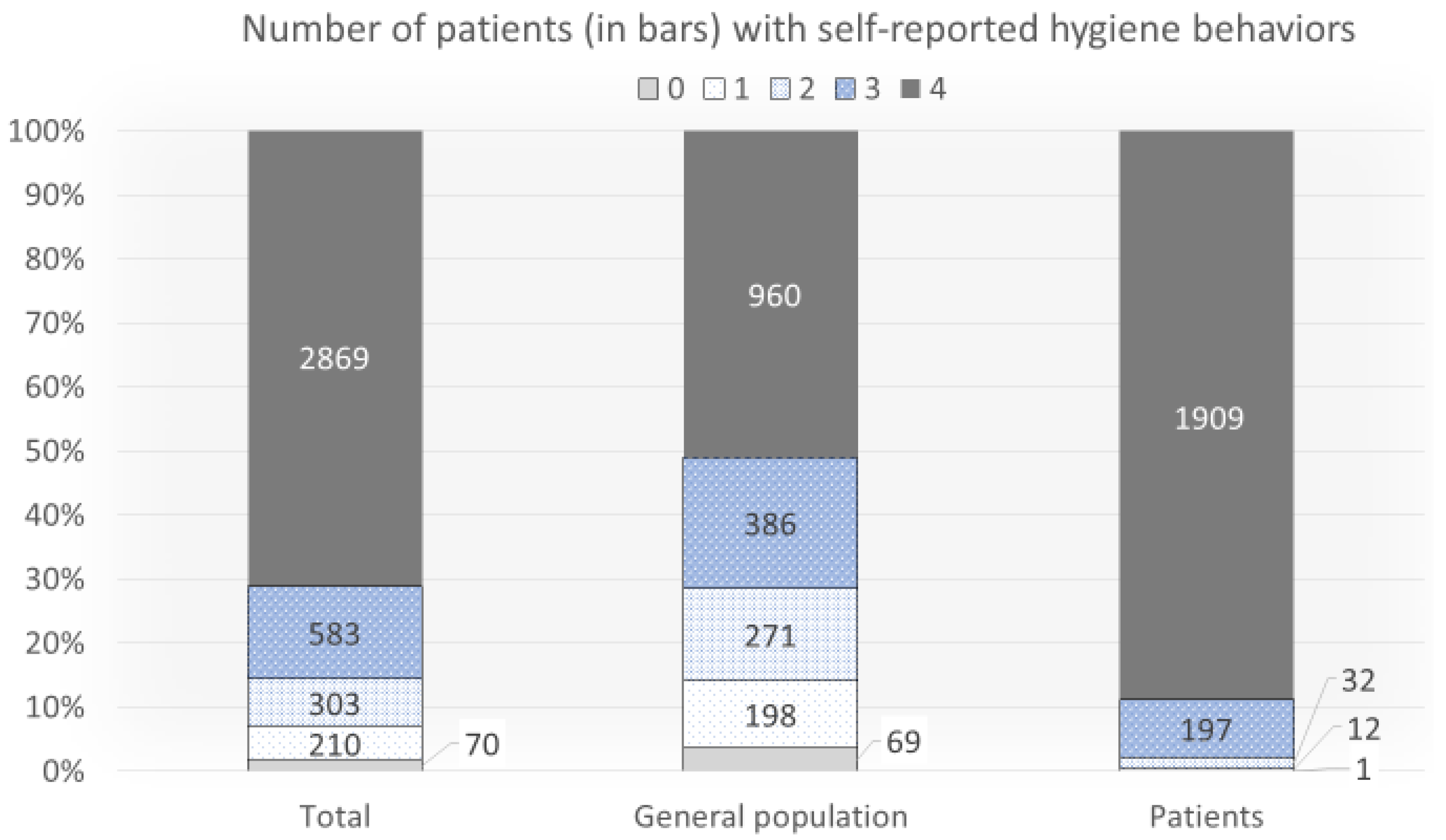
3.1. Research Question 1: What Is the Prevalence of the Behaviors, Overall and in the Two Samples Comparing General Population vs. Patients with Mental Health Problems?
3.2. Research Question 2: To What Extent Are Hygiene Behaviors (Avoiding Masses, Physical Distancing, Hand Hygiene, and Face Mask Use) Correlated with Each Other Overall and in the Two Samples?
3.3. To What Extent Are Hygiene Behaviors (Avoiding Masses, Physical Distancing, Hand Hygiene, and Face Mask Use as Well as the Aggregated Behaviors) Correlated with Overall Fear in the Two Samples?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaube, S.; Fischer, P.; Windl, V.; Lermer, E. The effect of persuasive messages on hospital visitors’ hand hygiene behavior. Health Psychol. 2020, 39, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahman, M. Personality Traits, Risk Perception, and Protective Behaviors of Arab Residents of Qatar during the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Zickfeld, J.H.; Schubert, T.W.; Herting, A.K.; Grahe, J.; Faasse, K. Correlates of Health-Protective Behavior during the Initial Days of the COVID-19 Outbreak in Norway. Front. Psychol. 2020, 11, 564083. [Google Scholar] [CrossRef]
- IFSG. Gesetz zur Verhütung und Bekämpfung von Infektionskrankheiten beim Menschen. Available online: https://www.gesetze-im-internet.de/ifsg/ (accessed on 20 August 2020).
- Eichenberg, C.; Grossfurthner, M.; Andrich, J.; Hübner, L.; Kietaibl, S.; Holocher-Benetka, S. The Relationship between the Implementation of Statutory Preventative Measures, Perceived Susceptibility of COVID-19, and Personality Traits in the Initial Stage of Corona-Related Lockdown: A German and Austrian Population Online Survey. Front. Psychiatry 2021, 12, 596281. [Google Scholar] [CrossRef] [PubMed]
- Hommes, F.; van Loon, W.; Thielecke, M.; Abramovich, I.; Lieber, S.; Hammerich, R.; Gehrke-Beck, S.; Linzbach, E.; Schuster, A.; von dem Busche, K.; et al. SARS-CoV-2 Infection, Risk Perception, Behaviour and Preventive Measures at Schools in Berlin, Germany, during the Early Post-Lockdown Phase: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2379. [Google Scholar] [CrossRef] [PubMed]
- Czeisler, M.É.; Garcia-Williams, A.G.; Molinari, N.-A.; Gharpure, R.; Li, Y.; Barrett, C.E.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; Czeisler, C.A.; et al. Demographic Characteristics, Experiences, and Beliefs Associated with Hand Hygiene among Adults during the COVID-19 Pandemic–United States, June 24–30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Magnan, R.E.; Gibson, L.P.; Bryan, A.D. Cognitive and Affective Risk Beliefs and their Association with Protective Health Behavior in Response to the Novel Health Threat of COVID-19. J. Behav. Med. 2021, 44, 285–295. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 27, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol. Health Med. 2021, 26, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Trougakos, J.P.; Chawla, N.; McCarthy, J.M. Working in a pandemic: Exploring the impact of COVID-19 health anxiety on work, family, and health outcomes. J. Appl. Psychol. 2020, 105, 1234–1245. [Google Scholar] [CrossRef]
- Bulmash, B.; Ben-Assuli, O.; Amar, M. Fear of Hospital-Acquired Infections: The Combined Impact of Patient’s Hygiene Sensitivity and Perceived Staff Preventive Behavior. J. Community Health 2020, 45, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Apisarnthanarak, A.; Apisarnthanarak, P.; Siripraparat, C.; Saengaram, P.; Leeprechanon, N.; Weber, D.J. Impact of anxiety and fear for COVID-19 toward infection control practices among Thai healthcare workers. Infect. Control Hosp. Epidemiol. 2020, 41, 1093–1094. [Google Scholar] [CrossRef]
- Blagov, P.S. Adaptive and Dark Personality in the COVID-19 Pandemic: Predicting Health-Behavior Endorsement and the Appeal of Public-Health Messages. Soc. Psychol. Personal. Sci. 2021, 12, 697–707. [Google Scholar] [CrossRef]
- Tsamakis, K.; Triantafyllis, A.S.; Tsiptsios, D.; Spartalis, E.; Mueller, C.; Tsamakis, C.; Chaidou, S.; Spandidos, D.A.; Fotis, L.; Economou, M.; et al. COVID-19 related stress exacerbates common physical and mental pathologies and affects treatment (Review). Exp. Ther. Med. 2020, 20, 159–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, M.W.; Zvolensky, M.J.; Long, L.J.; Rogers, A.H.; Garey, L. The Impact of COVID-19 Experiences and Associated Stress on Anxiety, Depression, and Functional Impairment in American Adults. Cognit. Ther. Res. 2020, 44, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Potts, H.W.W.; Michie, S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: Results from 36 national telephone surveys in the UK. Health Technol. Assess. 2010, 14, 183–266. [Google Scholar] [CrossRef] [Green Version]
- Schimmenti, A.; Billieux, J.; Starcevic, V. The four horsemen of fear: An integrated model of understanding fear experiences during the COVID-19 pandemic. Clin. Neuropsychiatry 2020, 17, 41–45. [Google Scholar]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- van der Valk, J.P.M.; Heijboer, F.W.J.; van Middendorp, H.; Evers, A.W.M.; Veen, J.C.C.M. Case-control study of patient characteristics, knowledge of the COVID-19 disease, risk behaviour and mental state in patients visiting an emergency room with COVID-19 symptoms in the Netherlands. PLoS ONE 2021, 16, e0249847. [Google Scholar] [CrossRef]
- Sharby, N.; Martire, K.; Iversen, M.D. Decreasing health disparities for people with disabilities through improved communication strategies and awareness. Int. J. Environ. Res. Public Health 2015, 12, 3301–3316. [Google Scholar] [CrossRef] [Green Version]
- Nachtigall, I.; Lenga, P.; Jóźwiak, K.; Thürmann, P.; Meier-Hellmann, A.; Kuhlen, R.; Brederlau, J.; Bauer, T.; Tebbenjohanns, J.; Schwegmann, K.; et al. Clinical course and factors associated with outcomes among 1904 patients hospitalized with COVID-19 in Germany: An observational study. Clin. Microbiol. Infect. 2020, 26, 1663–1669. [Google Scholar] [CrossRef]
- Hollis, N.D.; Thierry, J.M.; Garcia-Williams, A.G. Self-reported handwashing and surface disinfection behaviors by U.S. adults with disabilities to prevent COVID-19, Spring 2020. Disabil. Health J. 2021, 14, 101096. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Balkhi, F.; Nasir, A.; Zehra, A.; Riaz, R. Psychological and Behavioral Response to the Coronavirus (COVID-19) Pandemic. Cureus 2020, 12, e7923. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, N.; Aly, N.M.; Folayan, M.O.; Khader, Y.; Virtanen, J.I.; Al-Batayneh, O.B.; Mohebbi, S.Z.; Attia, S.; Howaldt, H.-P.; Boettger, S.; et al. Behavior change due to COVID-19 among dental academics—The theory of planned behavior: Stresses, worries, training, and pandemic severity. PLoS ONE 2020, 15, e0239961. [Google Scholar] [CrossRef] [PubMed]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neurol. Psychol. 1908, 18, 459–482. [Google Scholar] [CrossRef] [Green Version]
- Curtis, V.A.; Danquah, L.O.; Aunger, R.V. Planned, motivated and habitual hygiene behaviour: An eleven country review. Health Educ. Res. 2009, 24, 655–673. [Google Scholar] [CrossRef] [Green Version]
- Lippke, S.; Dahmen, A.; Gao, L.; Guza, E.; Nigg, C.R. To What Extent is Internet Activity Predictive of Psychological Well-Being? Psychol. Res. Behav. Manag. 2021, 14, 207–219. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Imani, V.; Majd, N.R.; Ghasemi, Z.; Griffiths, M.D.; Hamilton, K.; Hagger, M.S.; Pakpour, A.H. Using an integrated social cognition model to predict COVID-19 preventive behaviours. Br. J. Health Psychol. 2020, 25, 981–1005. [Google Scholar] [CrossRef]
- Gaube, S.; Fischer, P.; Lermer, E. Hand(y) hygiene insights: Applying three theoretical models to investigate hospital patients’ and visitors’ hand hygiene behavior. PLoS ONE 2021, 16, e0245543. [Google Scholar] [CrossRef] [PubMed]
- Buunk-Werkhoven, Y.A.B.; Dijkstra, A.; van der Schans, C.P. Oral Health-Quality of Life Predictors Depend on Population. Appl. Res. Qual. Life 2009, 4, 283–293. [Google Scholar] [CrossRef]
- Dahmen, A.; Keller, F.; Kötting, L.; Derksen, C.; Lippke, S. Angst vor dem Coronavirus, Absicht zum Befolgen der AHA-Regeln und Risikowahrnehmung bezüglich Arztbesuchen: Querschnittsstudie mit psychisch vorerkrankten Menschen. Gesundheitswesen 2021, 83, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Goebel, J.; Grabka, M.M.; Liebig, S.; Kroh, M.; Richter, D.; Schröder, C.; Schupp, J. The German Socio-Economic Panel (SOEP). Jahrbücher für Natl. und Stat. 2019, 239, 345–360. [Google Scholar] [CrossRef] [Green Version]
- Rückle, A.; Seefeld, L.; Müller, U.; Ommen, O.; Platte, A.; Stander, V.; Lang, P.; Thaiss, H.M. Infektionsschutz durch Hygiene. Einstellungen, Wissen und Verhalten der Allgemeinbevölkerung; BZgA-Forschungsbericht: Köln, Germany, 2018. [Google Scholar]
- Jabbari, P.; Taraghikhah, N.; Jabbari, F.; Ebrahimi, S.; Rezaei, N. Adherence of the General Public to Self-Protection Guidelines during the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef]
- McDonald, M.V.; Brickner, C.; Russell, D.; Dowding, D.; Larson, E.L.; Trifilio, M.; Bick, I.Y.; Sridharan, S.; Song, J.; Adams, V.; et al. Observation of Hand Hygiene Practices in Home Health Care. J. Am. Med. Dir. Assoc. 2021, 22, 1029–1034. [Google Scholar] [CrossRef]
- Derksen, C.; Keller, F.M.; Lippke, S. Obstetric Healthcare Workers’ Adherence to Hand Hygiene Recommendations during the COVID-19 Pandemic: Observations and Social-Cognitive Determinants. Appl. Psychol. Health Well Being 2020, 12, 1286–1305. [Google Scholar] [CrossRef]
- Tan, S.L.; Storm, V.; Reinwand, D.A.; Wienert, J.; de Vries, H.; Lippke, S. Understanding the Positive Associations of Sleep, Physical Activity, Fruit and Vegetable Intake as Predictors of Quality of Life and Subjective Health across Age Groups: A Theory Based, Cross-Sectional Web-Based Study. Front. Psychol. 2018, 9, 977. [Google Scholar] [CrossRef] [Green Version]
- Tong, K.K.; Chen, J.H.; Yu, E.W.-Y.; Wu, A.M.S. Adherence to COVID-19 Precautionary Measures: Applying the Health Belief Model and Generalised Social Beliefs to a Probability Community Sample. Appl. Psychol. Health Well Being 2020, 12, 1205–1223. [Google Scholar] [CrossRef]
- COSMO. Zusammenfassung und Empfehlungen Wellen 54 und 55. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/summary/54-55/ (accessed on 22 August 2021).
- Lohiniva, A.-L.; Sane, J.; Sibenberg, K.; Puumalainen, T.; Salminen, M. Understanding coronavirus disease (COVID-19) risk perceptions among the public to enhance risk communication efforts: A practical approach for outbreaks, Finland, February 2020. Eurosurveillance 2020, 25, 2000317. [Google Scholar] [CrossRef] [Green Version]
- Abrams, E.M.; Greenhawt, M. Risk Communication during COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 1791–1794. [Google Scholar] [CrossRef]
- World Health Organization. Risk Communication and Community Engagement Readiness and Response to Coronavirus Disease (COVID-19): Interim Guidance, 19 March 2020 (No. WHO/2019-nCoV/RCCE/2020.2). Available online: https://apps.who.int/iris/bitstream/handle/10665/331513/WHO-2019-nCoV-RCCE-2020.2-eng.pdf (accessed on 31 August 2021).
- Boyce, J.M. Current issues in hand hygiene. Am. J. Infect. Control 2019, 47S, A46–A52. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, M.; Reynolds, K.A.; Verhougstraete, M.; O’Rourke, M.K. Comparison of Perceived and Observed Hand Hygiene Compliance in Healthcare Workers in MERS-CoV Endemic Regions. Healthcare 2018, 6, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contzen, N.; Meili, I.H.; Mosler, H.-J. Changing handwashing behaviour in southern Ethiopia: A longitudinal study on infrastructural and commitment interventions. Soc. Sci. Med. 2015, 124, 103–114. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| General Population (First Sample) N = 1894 | Patients (Second Sample) N = 2155 | Test Statistic | |
|---|---|---|---|
| Gender | Chi2 (4036,2) = 23.707 ** | ||
| Male | 563 (29.7%) | 742 (34.6%) | |
| Female | 1312 (69.3%) | 1397 (65.2%) | |
| Divers/other | 19 (1.0%) | 3 (0.1%) | |
| Age 0 | Chi2 (4042,4) = 529.405 ** | ||
| <30 years | 441 (23.3%) | 89 (4.1%) | |
| 30–39 years | 426 (22.5%) | 271 (12.6%) | |
| 40–49 years | 374 (19.7%) | 498 (23.2%) | |
| 50–59 years | 393 (20.7%) | 984 (45.8%) | |
| 60+ years | 260 (13.7%) | 306 (14.2%) | |
| Education (years schooling) | Chi2 (4014,3) = 213.344 ** | ||
| ≤9 years | 189 (10.0%) | 66 (3.1%) | |
| 10 years | 405 (21.4%) | 482 (22.7%) | |
| 11 years | 527 (27.8%) | 979 (46.2%) | |
| ≥12 years | 773 (40.8%) | 593 (28.0%) | |
| Working | 993 (72.6%) | 1571 (73.3%) | Chi2 (3510,1) = 0.242 |
| Living with a partner/spouse | 1148 (60.0%) | 1328 (61.6%) | Chi2 (4049,1) = 0.434 |
| Living with a child/children | 666 (35.2%) | 741 (34.4%) | Chi2(4049,1) = 0.269 |
| COVID-19 risk factors | 424 (25.3%) | 878 (43.9%) | Chi2 (3680,1) = 138.520 ** |
| Disabled | 128 (7.2%) | 294 (13.8%) | Chi2 (3898,1) = 43.967 ** |
| Disability | 294 (13.8%) | 128 (7.2%) | Chi2 (3898,1) = 43.967 ** |
| Previous COVID-19 infection | 148 (9.9%) | 56 (3.0%) | Chi2 (3349,1) = 68.935 ** |
| Fear of being infected with the coronavirus | 2.27 (1.143) | 2.79 (1.036) | F (3932,1) = 223.079 ** |
| Fear of getting seriously ill with COVID-19 | 2.07 (1.130) | 2.68 (1.108) | F (3926,1) = 292.766 ** |
| Fear of infecting relatives/roommates or friends with COVID-19 | 2.51 (1.249) | 2.88 (1.144) | F (4047,1) = 98.245 ** |
| Fear (Index) | 2.29 (1.064) | 2.79 (0.967) | F (4047,1) = 246.683 ** |
| Change in physical health | 5.23 (1.991) | 4.89 (1.848) | F (3964,1) = 31.863 ** |
| Change psychological health | 4.17 (2.374) | 4.25 (1.981) | F (3865,1) = 1.551 |
| Hand Hygiene | Overall | General Population | Patients 0 |
| No, I do not intend to. | 442 (11.0%) | 404 (21.5%) | 38 (1.8%) |
| No, but I’ve thought about it. | 181 (4.5%) | 128 (6.8%) | 53 (2.5%) |
| No, but I’ve decided to do it. | 116 (2.9%) | 63 (3.4%) | 53 (2.5%) |
| Yes, but it’s hard for me. | 680 (17.0%) | 266 (14.2%) | 414 (19.4%) |
| Yes, and it’s easy for me. | 2589 (64.6%) | 1014 (54.1%) | 1575 (73.8%) |
| Face Mask Wearing | Overall | General Population | Patients 0 |
| No, I do not intend to. | 111 (2.8%) | 108 (5.7%) | 3 (0.1%) |
| No, but I’ve thought about it. | 8 (0.2%) | 7 (0.4%) | 1 (0.1%) |
| No, but I’ve decided to do it. | 2 (0.1%) | 2 (0.1%) | 0 (0.0%) |
| Yes, but it’s hard for me. | 1426 (35.4%) | 828 (44.0%) | 598 (27.8%) |
| Yes, and it’s easy for me. | 2483 (61.5%) | 936 (49.8%) | 1547 (72.0%) |
| Avoiding Large Masses | Overall | General Population | Patients 0 |
| Do not agree at all | 232 (6.0%) | 220 (12.5%) | 12 (0.6%) |
| Do rather not agree | 238 (6.1%) | 198 (11.2%) | 40 (1.9%) |
| Agree to some extent | 1210 (31.1%) | 562 (31.9%) | 648 (30.4%) |
| Agree fully | 2216 (56.9%) | 784 (44.4%) | 1432 (67.2%) |
| Keep the Physical Distance of 1.5 m to Others | Overall | General Population | Patients 0 |
| Do not agree at all | 143 (3.7%) | 132 (7.5%) | 11 (0.5%) |
| Do rather not agree | 321 (8.2%) | 284 (16.1%) | 37 (1.7%) |
| Agree to some extent | 1901 (48.7%) | 872 (49.4%) | 1029 (48.2%) |
| Agree fully | 1536 (39.4%) | 476 (27.0%) | 1060 (49.6%) |
| Hand Hygiene | Face Mask Wearing | Avoiding Large Masses | Keep the Distance | Aggregate of All Behaviors | |
|---|---|---|---|---|---|
| Hand hygiene | 1 | 0.240 ** | 0.150 ** | 0.169 ** | 0.457 ** |
| Face mask wearing | 0.405 ** (0.368 **) | 1 | 0.091 ** | 0.084 ** | 0.084 ** |
| Avoiding large masses | 0.447 ** (0.364 **) | 0.502 ** (0.360 **) | 1 | 0.498 ** | 0.266 ** |
| Keep the physical distance of 1.5 m to others | 0.420 ** (0.353 **) | 0.432 ** (0.314 **) | 0.693 ** (0.628 **) | 1 | 0.263 ** |
| Aggregate of all behaviors | 0.647 ** (0.710 **) | 0.490 ** (0.600 **) | 0.717 ** (0.752 **) | 0.671 ** (0.759 **) | 1 |
| Hand Hygiene | Face Mask Wearing | Avoiding Large Masses | Keep the Distance of 1.5 m to Others | Aggregate of All Behaviors | |
|---|---|---|---|---|---|
| Fear of being infected with the coronavirus | 0.033/0.368 ** (0.258 **) | −0.086 **/0.441 ** (0.235 **) | 0.204 **/0.566 ** (0.432 **) | 0.240 **/0.469 ** (0.394 **) | 0.175 **/0.496 ** (0.413 **) |
| Fear of getting seriously ill with COVID-19 | 0.051 */0.321 ** (0.248 **) | −0.103 **/0.393 ** (0.207 **) | 0.186 **/0.525 ** (0.410 **) | 0.226 **/0.446 ** (0.386 **) | 0.170 **/0.446 ** (0.399 **) |
| Fear of infecting relatives/roommates or friends with COVID-19 | 0.055 */0.330 ** (0.230 **) | −0.051 */0.407 ** (0.218 **) | 0.141 **/0.463 ** (0.333 **) | 0.164 **/0.386 ** (0.298 **) | 0.147 **/0.441 ** (0.345 **) |
| Aggregate of all fears | 0.056 */0.379 ** (0.273 **) | −0.094 **/0.470 ** (0.246 **) | 0.196 **/0.578 ** (0.435 **) | 0.233 **/0.483 ** (0.398 **) | 0.189 **/0.517 ** (0.430 **) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippke, S.; Keller, F.M.; Derksen, C.; Kötting, L.; Dahmen, A. Hygiene Behaviors and SARS-CoV-2-Preventive Behaviors in the Face of the COVID-19 Pandemic: Self-Reported Compliance and Associations with Fear, SARS-CoV-2 Risk, and Mental Health in a General Population vs. a Psychosomatic Patients Sample in Germany. Hygiene 2022, 2, 28-43. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene2010003
Lippke S, Keller FM, Derksen C, Kötting L, Dahmen A. Hygiene Behaviors and SARS-CoV-2-Preventive Behaviors in the Face of the COVID-19 Pandemic: Self-Reported Compliance and Associations with Fear, SARS-CoV-2 Risk, and Mental Health in a General Population vs. a Psychosomatic Patients Sample in Germany. Hygiene. 2022; 2(1):28-43. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene2010003
Chicago/Turabian StyleLippke, Sonia, Franziska M. Keller, Christina Derksen, Lukas Kötting, and Alina Dahmen. 2022. "Hygiene Behaviors and SARS-CoV-2-Preventive Behaviors in the Face of the COVID-19 Pandemic: Self-Reported Compliance and Associations with Fear, SARS-CoV-2 Risk, and Mental Health in a General Population vs. a Psychosomatic Patients Sample in Germany" Hygiene 2, no. 1: 28-43. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene2010003