

The Use of 3D Printing and Nanotechnologies to Prevent and Inhibit Biofilms on Medical Devices

1
Department of Biology, College of Staten Island, City University of New York, 2800 Victory Blvd, Staten Island, New York, NY 10314, USA
2
PhD Program in Biology, The Graduate Center, City University of New York, New York, NY 10016, USA
3
Macaulay Honors College, City University of New York, New York, NY 10023, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Hygiene 2023, 3(3), 325-338; https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene3030024
Submission received: 21 August 2023
/
Revised: 10 September 2023
/
Accepted: 15 September 2023
/
Published: 19 September 2023
(This article belongs to the Special Issue The Impact of Biofilms on Cleaning, Disinfection of Surfaces and Reprocessing of Reusable Medical Devices)
Abstract
:Biofilms remain one of the most pervasive complications of the medical field, representing 50–70% of all nosocomial infections and up to 80% of total microbial infections. Since biofilms contain intricately small matrices, different microenvironments, and accumulations of biodiverse microorganisms of different resistances, these structures end up being difficult to target. As we review in this paper, 3D printing and nanotechnology help overcome these unique challenges of targeting biofilms, especially within the medical field. These technologies bring versatility and more precise control to personalized reusable medical device development and implants, with enhanced antimicrobial characteristics. They allow for decreased surface roughness of the implants, smaller pores, more targeted topography, and even added antibiotic or drug-releasing abilities for the medical devices. Furthermore, combining 3D with nanoparticles allows for the creation of anodized nanosurfaces of medical implants with increased osseointegration and reduced polymerization while promoting cost efficiency, durability, and biocompatibility. In this review, we explore the potentially valuable antimicrobial consequences of applying 3D technology and nanoengineering to dental and orthodontic implants, oral prostheses, hearing aids, joint replacements, catheters, stents, endotracheal tubes, prosthetics, and bone scaffolds.
1. Introduction
With the advent of 3D printing and nanotechnologies, the possibilities to develop more versatile materials in the medical industry have vastly increased. Polymer printing and nanomaterials in the medical field provide cost-effective means to quickly produce a wide variety of highly customizable products, which include bone tissue scaffolds of enhanced strength, cardiovascular tissues and stents, patient-specific anatomical models for precision medicine, and microbe-resistant devices [1,2,3,4]. Nanoparticles have already proven themselves to be powerful and effective tools in the diagnostic and therapeutic targeting of illnesses such as chronic kidney disease [5]. Although there are concerns about the potential for some toxic adverse effects upon collection of these materials in the human body, new green or ecologically clean forms of nanoparticles help prevent or alleviate these concerns to be able to capitalize on their valuable medical potential [6,7]. Due to the versatility of such materials, this has opened up new opportunities in the development of medical equipment and implants that can prevent the formation of biofilms [8].
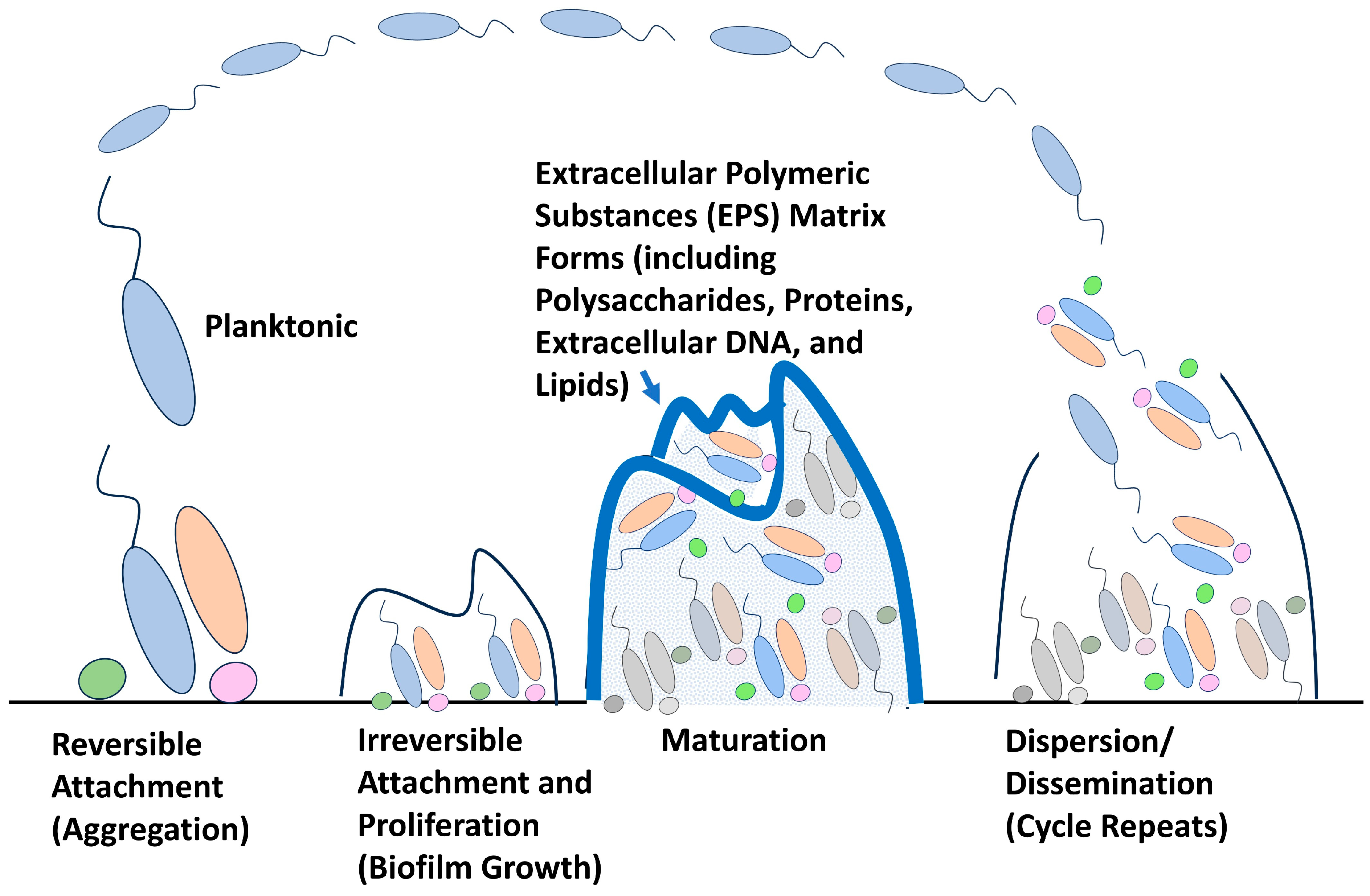
Biofilms are large multi-species matrices of bacteria or other microorganisms collecting together on surfaces through extracellular polymeric substances (EPS), creating enhanced cohesion and layers of highly resistant protection [9] (Figure 1). These biofilms tend to include bacteria that can thrive on both abiotic and biotic surfaces, with abilities to evade antibiotics or disinfectants through physical shielding as well as a variety of resistance genes obtained through lateral gene transfer in the biofilm community [10]. When cells are part of a biofilm matrix community, they have been found to have nearly 100 to 1000 times greater resistance to antimicrobials (antibiotics and disinfectants/antiseptics) compared to when they are found in their planktonic form [11,12,13]. This resistance is of growing concern in the medical field, as infections that arise from hospitalization or medical treatments are labeled as nosocomial infections, and it is estimated by the NIH and CDC that more than sixty percent of nosocomial infections are caused by biofilms [14,15]. Biofilms present many dangers in the medical field, including chronic infections with implanted devices, intravenous access line-induced bloodstream infections, surgically implanted mesh infections, orthodontic complications, and orthopedic complications [16,17,18,19,20]. Due to these significant problems, various mechanisms have been studied to reduce the dangers people face from these persistent pathogens. One area of study that has been explored is to interfere with cyclic dimeric guanosine monophosphate (c-di-GMP) metabolism and signaling, as this molecule serves as a second messenger mediating bacterial processes, including the formation of biofilms [21]. While this is an excellent strategy and can provide great benefits to the medical field, we believe it lacks the versatility and personalization abilities that 3D printing and nanotechnologies provide. As the field of 3D printing with medical technologies is fairly new, the number of studies on the microbial adhesion susceptibility of the products remains fairly low but is increasing each year [22]. By examining the potential of 3D printing and nanotechnologies in medical and dental fields, we aim to demonstrate ways to reduce complications caused by highly resistant biofilms while maximizing cost efficiency in the development and use of equipment and implant materials.
2. Use of 3D Printing to Target Biofilms in Dentistry Industry
While organ or tissue transplant and implant technologies are critical areas prone to biofilm infiltration, it is important to note that dental and orthodontic procedures also carry a major potential for biofilm risks. Dentures, retainers, occlusal splints, crowns, bridges, and other oral prostheses are all highly susceptible to microbial biofilm colonization [23,24]. The use of 3D printing technology in this field has a multi-fold benefit as it provides versatility to produce patient-specific prostheses while also providing more highly resistant material options to reduce infections in a more cost-effective and time-efficient manner [23].
In the dental industry, polymethyl methacrylate (PMMA) has been one of the most commonly used polymers for oral prostheses since its introduction in 1937 [23,25]. PMMA has long provided the benefits of natural aesthetics matching original dental characteristics, widespread availability, biocompatibility, light-curability, cost efficiency, and easy malleability of processing and repair [23,25]. Unfortunately, however, PMMA also suffers from the downside of high susceptibility to microbial growth, including its prime surface propensity for biofilm formation [23]. Enhancing antimicrobial resistance of 3D printed materials is critical, as it has been shown that while 3D printing allows for the benefit of developing personalized, well-fitted implants, in cases of printing plates for dental and craniofacial jaw or dental implants, the roughness and pores produced compared to commercial plates or implants increase bacterial adhesion for biofilms, especially with contamination during surgery [26]. To overcome this weakness, one study utilized 3D printing to produce a PMMA-based formulation that incorporated 2-methacryloyloxyethyl phosphorylcholine (MPC) and sulfobetaine methacrylate (SB), which are zwitterionic materials [23]. The zwitterionic nature of these materials means they have cationic and anionic portions with an overall neutral charge and electrostatic interactions that lead to protein-repellent and antimicrobial properties [23] (Figure 2). Protein-repellent properties are significant for biofilm prevention as proteins, such as CdrA extracellular adhesin, are a major component of the extracellular polymeric substances that comprise the biofilm matrix [27,28]. When tested against early biofilm colonizers, Streptococcus mutans, Staphylococcus aureus, Klebsiella oxytoca, and Klebsiella pneumoniae, as well as human saliva-derived biofilms, 3D printed MPC/SB-enhanced PMMA showed significantly lower amounts of attached bacteria than the control (PMMA before addition of any MPC or SB), as well as minimal biofilms compared to the robust amount on the controls (thickness and biomass were reduced with MPC/SB) [23]. Furthermore, while adding biofilm resistance, the 3D-printed MPC/SB-enhanced PMMA did not have any large losses of flexural strength or elastic modulus, which demonstrates great potential for these materials to increase antimicrobial properties without decreasing the durability or reliability of the products [23].
As already mentioned, one of the major concerns regarding 3D-printed medical devices and the potential for biofilm formation is the surface properties of printed materials [29]. It has become important to test various printing methods to ensure that low surface roughness is maintained, thus reducing bacterial adhesion and biofilm formation [29]. Testing different materials and timepoints after dental events, such as brushing or artificial aging, one study demonstrated that 3D printed resin (methacrylic oligomers and phosphine oxides) exhibited similar roughness to acrylic resin (PMMA), and bisacryl resin (dimethacrylate polymer, Bis-GMA, zirconium particles, silica, and silane) at the initial timepoint and after brushing, but after artificial aging, the printed resin significantly decreased in roughness, while acrylics significantly increased in roughness [29]. The long-term improvement in 3D printed items compared to standard materials is quite promising, especially considering the increased potential of manual and automixing manipulation defects of bubbling and pores that are more commonly observed in the standardly prepared dental resins [29]. The need to reduce pore size in dental implants to best minimize biofilm surface formation has also made nano-engineered dental implants a promising means of development [30]. For instance, electrochemical anodization has allowed for the development of anodized nano-engineered zirconia dental implants with aligned nanopores providing ideal surface topography to prevent biofilms from forming [30]. Important to dental implant placement, this use of nanopore surfaces or nanoscale surface production also increases osseointegration with the natural oral matrixes of the patient, which increases the potential for these techniques in the industry [30]. The successful antimicrobial observations of anodized nanosurfaces against common pathogens, such as Escherichia coli, Listeria monocytogenes, Staphylococcus aureus, and Staphylococcus epidermidis, have been credited to electrostatic and acid-base forces being modified due to the high density of the small pores [11]. In addition to the printing process itself, post-production processing can also be valuable in enhancing the potential of printed materials to resist biofilm formation [22]. In one study, polishing and glazing 3D-printed NextDent UV-curable resin for crowns, bridges, and prosthetics reduced the surface roughness average, which in turn reduced the affinity for bacterial adhesion and colonization [22]. Additionally, glazing alone seemed to be sufficient in reducing surface roughness and biofilm formation, including resistance against streptococci, staphylococci, and Candida, in some polymer substances, such as Mazic Temp 3D-printed materials [22]. The addition of polymerization inhibitors, such as mequinol, to the printed materials, as well as the use of resins that lack long polymerization times, has been shown to further enhance the antimicrobial benefits of 3D-printed glazed or polished materials, as extended polymerization times increase roughness and thus biofilm formation [22].
While some 3D printing focuses on the whole production of implants or devices, some of the value of 3D printing simply lies in the versatility of improving fillers that can be effectively added to the produced dental appliances, such as the printing of intra-oral PMMA appliances with nanodiamonds added as fillers [31]. The use of 3D-printed nanodiamond-enhanced oral appliances not only improved resistance to biofilms of Streptococcus mutans but also improved wear resistance and friction resistance [31]. Even more impressive in dental filler additives is the ability to now fabricate model compounds with 3D-printing technologies using known drugs from the dental field [32]. For instance, customized molds have been made with the antimicrobial tinidazole (TNZ) through thermal pressing of 3D molds to form release and compression molds capable of “on-demand” sustained release of TNZ while maintaining strong mechanical integrity [32]. Since dental caries require proper disinfection when first placed, this new method of 3D-printing custom antimicrobial modes could help provide fillers that are produced with lower cost, greater accessibility and personalization, and increased effectiveness [32]. The promising potential of 3D-printing custom implants in the dental field also expands to the orthodontic and maxillofacial fields, including facial epithesis, with far less strain or complications for patients [33].
3. Use of 3D Printing to Target Biofilms in Reusable Medical Devices
The use of 3D-printed reusable medical devices in areas other than dentistry has also brought about a new industry of medical devices that are now safer to implement without the fear of post-operative infections occurring. Chronic infections due to bacterial biofilm formation on implanted medical devices are a major concern in the field of medicine and the healthcare industry [16]. Various pathogens can cause infections in humans, such as viruses, fungi, and bacteria, but infections from bacteria are the most common type of infection, causing both acute and chronic infections in the population [34]. Bacterial infections are also becoming more untreatable due to the alarming rise of antibiotic-resistant bacteria strains [35,36,37,38]. Bacteria exist in two forms: planktonic, which is a free-floating state, and sessile, which adheres to the surface. Both states result in the production of a protective barrier that works as an endogenous defense system, making it difficult for antibiotics to rid the bacteria of infection. This exopolysaccharide matrix barrier, or “slime”, along with the accumulated microbial cell community, is what is now referred to as “biofilm” [39].
Both Gram-positive and Gram-negative bacteria form biofilms on medical devices, but some are more prevalent than others. The most common forms are Enterococcus faecalis, Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus viridans, E. coli, Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa [38]. Approximately two-thirds of medical device infections are caused by the Staphylococcus species, which can infect devices such as prosthetic heart valves and catheters, causing potential hospitalizations [40,41,42,43]. According to the National Institute of Health, biofilms account for up to 80% of the total number of microbial infections, such as endocarditis, cystic fibrosis, periodontitis, osteomyelitis, and kidney infections [44,45,46]. Biofilms are particularly challenging to treat due to their difficult diagnosis and lack of biomarkers. Due to the complexity of biofilm communities and their antibiotic-resistant nature, the problem requires new material science to find and implement solutions, particularly biofilm-resistant materials and conventional antibiotics [35,47]. Sustainable innovations in antifouling being explored include targeting bacterial processes, such as quorum sensing, biofilm-related gene expression, secondary messengers, and regulatory RNA, as well as blocking initial adhesions by using green technology, such as silicon oil-infused substrates from plant models [48,49].
A prominent medical device example is the use of hearing aid devices [50]. Approximately 5% of the world’s population suffers from hearing loss, including one-third of the population over the age of 65 years which requires the use of hearing aid devices [50]. As a result of prolonged use of these medical devices, it is common for the ear microbiota to be altered or increased, increasing the risk of fungal and bacterial infections [50]. However, this is not just a limited issue for hearing aids alone. This has been a common occurrence with most internally placed or implanted medical devices—especially implanted medical devices used in joint replacements, catheters, stents, and prosthetics [47].
To date, 3D-printed medical devices with antibiofilm properties are not very prevalent but are being researched and developed for multipurpose use [51]. Common practices for removing biofilm development on hearing aid devices require removing the device for extensive cleaning. This becomes even more complicated when an infection has already taken root. In the case of ear infections, topical antibiotics, and systemic or topical fluoroquinolones are the most effective in administering treatment [50]. Two of the most common fluoroquinolones used for ear infections are ciprofloxacin and ofloxacin [47,50]. With new 3D-printed hearing aids that can act as drug-loaded platforms, patients would avoid discontinuing the use of hearing aids due to infection [52,53].
The drugs chosen for the 3D-printed devices were based on the two most common medications used to treat ear infections. A combination of ciprofloxacin and fluocinolone acetonide were both incorporated into the hearing aid as controlled-release drugs, and this combination was then evaluated against the two most common biofilm formers—Pseudomonas aeruginosa and Staphylococcus aureus—both involved in chronic ear infections [52,53]. Flexible resin and engineering hard resin (ENG) were used to prepare the photoreactive solutions [50]. The results for 3D printed hearing aids proved to be highly efficient and cost-effective when the volume of production was kept low when compared to other manufacturing methods used, such as molding, which requires molds that come at a higher cost due to materials, machinery, and labor [54,55]. The DLP 3D-printed hearing aids preventing or treating biofilm-related infections were successful when prepared using both flexible and ENG hard resins with different drug loads. In vitro drug release studies showed that the hearing aids were able to provide sustained drug release for over seven days for both drugs, successfully demonstrating antibiofilm properties against P. aeruginosa and S. aureus [50].
While resin composite hearing aids with antibiotics are one method of combating antibiofilm resistance, it is not the only angle of approach scientists are taking. Material sciences are also playing a role by researching certain composite materials that show promising results with antibiofilm resistance. Such a material is a 3D-printed composite of polylactic acid (PLA) with the addition of MgB2 particles [56]. The PLA composite, along with MgB2, was shown to have strong antimicrobial activity and is a great candidate for future medical devices due to its range of biomedical applications and its biodegradability and biocompatibility properties [56,57]. Another application of polylactic acid (PLA) is in filament compositions along with modified carbon nanomaterials such as bidimensional graphene (PLA-G), which improves the performance of 3D-printed medical devices. Together, this composition can also be used in the production of personal protective equipment due to its properties, which allow it to be sterilized by near-infrared light exposure within three minutes. This method has even been considered for combating the efforts in the SARS-CoV-2 epidemic [58].
Another approach has been modified 3D-printed polycaprolactone (PCL) scaffolds along with antimicrobial peptides (AMPs). Currently, in Phase I and Phase II human clinical trials, melamine, a chimeric cationic peptide, was immobilized onto the surface of a 3D printed medical-grade polycaprolactone (mPCL) scaffold and showed promising results with a ~78.7% reduction of Staphylococcus aureus compared to the control sample [59,60,61]. Melimine has some interesting properties and might have many applications in the medical implant field. According to multiple studies, it has been shown to reduce bacteria adhesion and biofilm formation when covalently bound to different non-degradable materials, such as silicone, glass, and titanium [62,63,64,65].
A promising new method for orthopedic surgeries involving bone regeneration and defects involves a dual-functional 3D-printed composite scaffold. The quaternized chitosan (HACC)-grafted polylactide-co-glycoside (PLGA)/hydroxyapatite (HA) scaffold (PLGA/HA/HACC) generated by 3D-printing technology exhibited significant antimicrobial and osteoconductive properties in vitro [66,67]. The study evaluated the bone-repairing effects of the 3D-printed scaffolds using infected cortical and cancellous bone defects. The study used 80 female Sprague–Dawley rats and 36 female New Zealand white rabbits. X-ray, micro-CT, microbiological, and histopathological analyses were used to assess the anti-infection and bone-repairing potential of the dual-functional porous scaffolds, and it was observed that the HACC-grafted PLGA/HA scaffolds exhibited significantly enhanced anti-infection and bone regeneration capability in different infected bone defect models [66,67,68]. The scaffold also exhibited enhanced anti-infection and bone regeneration capability in different infected bone defect models, showing promising results in applications for repairing different types of bone defects, even under infection [66,68,69].
4. Nanotechnologies Used to Target Biofilms in the Medical Field including Reusable Devices
As stated above, antibiotic resistance and biofilms continue to cause a heightened sense of urgency to develop new treatments in the medical field [70,71]. Their complex matrices and varying levels of susceptibility lead to more severe infections, but there is hope for a new method of treatment: the use of nanoparticles [70]. Nanoparticles have the potential to combat three major advantages that biofilms have against treatment [70]. The first complication that can be overcome with nanotechnology is that the layers in a biofilm matrix make it more difficult and time-consuming for antibiotics to permeate throughout the biofilm [70]. It has been demonstrated that since nanoparticles are small, they can move throughout the matrix with less hindrance [70]. The second and third obstacles to biofilms are that different microenvironments within a biofilm and different microorganisms with varying resistance profiles make them more challenging to treat [70]. These difficulties were demonstrated in one study in which it was observed that five identical outdoor stone dog sculptures in the same location of a yard revealed varying levels of robust biodiversity and species richness, as well as the ability to intensify the deterioration of their microenvironments [72]. Nanoparticles, however, can be modified to withstand different environments and target specific microbes [70]. An advantage of nanoparticles is the numerous different types of particles that can be used, with one being polymeric particles [71,73]. These particles have stable structures, and their physical and chemical properties can be altered easily by changing surfactants or polymer length [70,73]. This allows for polymeric nanoparticles to aid in making antibiotic delivery more efficient [74]. In one study, polymeric particles containing an antimicrobial peptide for Pseudomonas aeruginosa allowed for easier delivery of the peptide to the biofilm without affecting its activity [74]. Additionally, the nanoparticles did not have any noticeable side effects in vitro or in vivo [74]. A certain type of polymer nanoparticle that is being researched for wound healing is hydrogel [75,76]. In a murine excisional wound infection model, the use of a non-leaching-based debridement followed by ex situ contact-killing (DESCK) hydrogel was able to effectively kill biofilms formed by methicillin-resistant Staphylococcus aureus (MRSA) and carbapenem-resistant P. aeruginosa (CR-PA) [75]. The hydrogel was made from polyethylene glycol dimethacrylate with a polyethyleneimine (PEI) star copolymer, and its large pore size was part of its success as it allowed for easier contact between the bacteria and the cationic pore walls [75]. Another study used a hydrogel dressing made from compounding chitosan-PEG hydrogel with upconversion nanoparticles (UCNPs) that were coated with a mesoporous silica-loaded zinc phthalocyanine (ZnPc) photosensitizer [76]. Under photodynamic therapy at 980 nm excitation, singlet oxygen is produced that provides antibacterial activity, as evidenced by in vitro experiments against S. aureus and Escherichia coli [76]. During in vivo experiments, it effectively lowered inflammation and the amount of time necessary for wound healing [76].
Lipid nanoparticles have also been demonstrated to inhibit biofilms, with one study demonstrating the potential use of nanoparticle coatings for endotracheal tubes [77]. The coatings of solid lipid nanoparticles (SLN) containing lauric acid and oleic acid resulted in the killing of P. aeruginosa bacteria on the tubes as well as lowering bacterial adhesion to approximately 1% [77]. Invasive devices such as these tubes tend to be associated with hospital-acquired pneumonia, and a coating of this style could limit the risk of biofilm formation [77]. There is also variety within the subsection of lipid nanoparticles, as nanostructured lipid carriers (NLCs) have been studied for use against biofilms [78]. Unlike SLNs, this type of nanoparticle has liquid lipids in its structure, which can improve storage ability [78,79]. In one study, when NLCs were loaded with levofloxacin and DNase, they lowered the formation of P. aeruginosa biofilms in a semisolid medium, similar to the environment in the lungs of a patient with CF [78]. The NLCs used also demonstrated a controlled release of levofloxacin, which would lead to lower doses required for a patient [78]. Liposomes have also been used to study the effectiveness of lipid nanoparticles against biofilms [80,81]. Glucosylated cationic liposomes containing (+)–Usnic acid (UA) led to increased antimicrobial activity against Staphylococcus epidermidis biofilms, although efficacy changed depending on the glucosylated amphiphile used [80]. UA’s effectiveness alone is impeded by its low solubility in water, but due to the structure and charge of the liposome, it is able to penetrate the biofilm matrix with less difficulty [80]. A similar case is seen with fusogenic liposomes encapsulating vancomycin [82]. Vancomycin’s hydrophilicity impedes its ability to enter biofilms, but while in a fusogenic liposome, it will have higher contact as the liposome can fuse with biological membranes [82]. The study showed that encapsulated vancomycin inhibited S. aureus biofilms better at the mature stage, while free vancomycin inhibited the biofilms more effectively at the early stages [82]. The likely reason is that at the mature stage, the free vancomycin would become stuck in between the peptidoglycan layer [82]. In the early stages, without this hindrance, the free version would have more antibiotics available for contact [82].
As the development of lipid nanoparticles has grown, so has the progress of metallic nanoparticles [83,84,85,86,87]. Gold nanoparticles have been studied to inhibit biofilms as, due to oxidation, they can release Ag+ ions, which results in more reactive oxidative species, and their small size provides them with more surface area to have contact with microbes [84]. One study in particular examined how surface charge on gold nanoparticles can affect biofilm inhibition [9]. Based on in vitro experiments, increasing the positive surface charge increases bactericidal effects against S. aureus and P. aeruginosa, but if the charge became too large, the nanoparticles cytotoxicity was no longer limited to just bacterial cells but epithelial cells as well [83]. Lowering the surface charge while increasing the particle concentration resulted in less toxicity to epithelial cells, but this creates a hurdle in terms of developing the treatment for therapeutic use [83]. Additionally, the effects of gold nanoparticles have been shown to vary depending on the type of nanoparticle and bacteria, which could lead to complications in future studies [88]. Silver nanoparticles have also been shown to have a possible use in the medical field [85,86,87]. An in vivo experiment for a study on silver coordination polymer coatings for metal implants showed that the coating prevented murine S. epidermidis implant infection [86]. The silver ions bind thiol groups in amino acids, which inactivates enzymes that the biofilms produce and use [86]. Additionally, the coating allowed for a slow release of silver ions and low leukocyte toxicity with the silver ions [86]. The small size of silver nanoparticles is also thought to play a role in their anti-biofilm effect, which may be why silver nanoparticles have been observed to have higher inhibitory effects than gold nanoparticles, which are larger [84,89]. Another study examined the use of silver nanoparticle coating, specifically silver nitrate, on plastic catheters [87]. The coating had significant antimicrobial activity during in vitro experiments on several microbes, including E. coli and Candida albicans [87]. In a separate study, the effects of silver nanoparticles were shown to improve when excited by light, with longer light exposure correlating to more inhibitory activity [85]. The theory behind this treatment is that silver nanoparticles oxidize bacterial proteins by direct binding, and the oxidation is light-catalyzed [85]. However, silver nanoparticles are also similar to gold nanoparticles in the fact that not all microbes respond the same way to silver nanoparticles [87,88].
Despite the great promise and value of nanoparticles, it is important to note that they are not without risks, as potential side effects pose a concern with nanotechnology’s use in biomedical circumstances. One of the largest concerns with nanotechnology use and development in the medical field is the potential for toxicity, as toxic chemicals and high-energy protocols have historically been used to develop these nanoparticles [90]. Not only could these technologies be toxic to the human body, but some production mechanisms have been atrocious for the environment. Traditionally, the methods employed to produce metal nanoparticles have included UV irradiation, aerosol technologies, lithography, laser ablation, ultrasonic fields, and photochemical reduction, which has led to increased awareness of the need to promote green, nontoxic protocols [90]. Thus, nanotechnology production methods, which may be more suitable for the medical field, have now included the use of microorganisms to induce nanoparticle assembly, including bacteria (including Pseudomonas strains), viruses (including tobacco mosaic virus and M13 bacteriophage), fungi (including Phoma and Fusarium), yeast (such as Pichia jadinii), algae, plants (including Baikal skullcap), and even human cell lines (SiHa, HeLa, SKNSH, and HEK-293) [6,90]. Furthermore, the use of surface coaters with different coating compositions and concentrations applied to the nanoparticle and tested on human skin models also successfully reduces the risks of toxicity or inflammation, with hydroxyethyl cellulose-coated samples demonstrating the most promise [91]. While the potential for cytotoxic or inflammatory responses was a concern when nanoparticles were originally developed for the medical field, their potential as a possible solution to the highly resistant nature of biofilms remains a highly viable option [70]. The large variety of nanoparticles allows for nanoparticle treatment to be effective for multiple different microbes, as for each biofilm characteristic there will be a nanoparticle type better suited to treat it [70]. For example, liposome nanoparticles may be the best option to treat a biofilm that needs a hydrophobic compound to inhibit it [92]. While further research is required to better understand how to best utilize and formulate nanoparticles, they have shown the ability to inhibit biofilms in several different forms [70].
5. Conclusions
Biofilms continue to be an ever-present threat in the medical field, as implants, prostheses, dental fillers, and other artificial patient care devices serve as prime surfaces for the accumulation of bacterial matrices, especially when exposed to contamination during implantation or surgery [93,94]. It is estimated by the National Institutes of Health that nearly 80% of chronic bacterial infections and surgical site infections in humans are attributed to biofilms [95,96,97]. Furthermore, it is believed that such infections, particularly antibiotic-resistant ones, will lead to annual death tolls above cancer and diabetes by the year 2050 globally [97,98]. Thus, it is of great importance to find ways to reduce these microbial contaminations while also maintaining cost-efficient, durable, bioavailable, and versatile aspects of the production process [99].
Two major advancements in this process of enhancing implant or artificial medical device development have been 3-D printing technologies and nanotechnologies in personalized medicine fields [100] (Table 1). While many prospective initiatives exist to try to target biofilms, such as targeting c-di-GMP metabolism or other bacterial pathways [21], we believe that the use of 3D printing and nanotechnologies presents the most versatile option with the highest levels of personalized medicine possible for patients. In reviewing the recent literature on these advancements, it has become apparent that one very important area to take into consideration is the surface roughness of prepared devices [22,26,29]. Biofilms tend to form in areas with greater surface roughness, as these surfaces have crevices and pore pits with increased surface area for microorganisms to hide and accumulate [101]. 3D printing and nanotechnologies can allow for increased versatility and decreased particle sizes to better target these pervasive, intricate infections. The surface roughness can be minimized to increase antimicrobial effectiveness by the use of 3D printing with enhanced/blended materials, as well as materials with nanopores, such as anodized nano-engineered zirconia with aligned nanopores [29,30]. Additionally, to further enhance the effectiveness of antimicrobial-resistant implants with low surface roughness, procedures to produce the printed or nanotechnology implants should have short polymerization times and add polishing and glazing post-production steps [22]. The use of zwitterion polymers in printing can also maximize antimicrobial qualities as the electrostatic and hydrophobic properties reduce protein binding abilities and thus reduce matrix formation of EPS-dependent biofilms [23]. When taking these points into consideration, along with the high levels of personalization and manual versatility of creating molds or devices in the exact specifications or patterns desired, the promise of 3D printing and nanotechnologies in reusable medical device development becomes glaringly obvious. The promise of even more advancements in the future as more compounds and quicker printing methods are discovered only increases the great value of this emerging area of biofilm targeting.
Author Contributions
All authors (M.M.E., J.R.G. and S.T.) contributed equally to all writing, editing, reviewing, and figure development. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank the CUNY College of Staten Island, the CUNY Graduate Center, and the CUNY Macaulay Honors College for their support in our research endeavors and professional development.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Haleem, A.; Javaid, M.; Khan, R.H.; Suman, R. 3D Printing Applications in Bone Tissue Engineering. J. Clin. Orthop. Trauma 2020, 11, S118–S124. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jo, H.H.; Lim, K.S.; Lim, D.; Lee, S.; Lee, J.H.; Kim, W.D.; Jeong, M.H.; Lim, J.Y.; Kwon, I.K.; et al. Heparin Coating on 3D Printed Poly (l-Lactic Acid) Biodegradable Cardiovascular Stent via Mild Surface Modification Approach for Coronary Artery Implantation. Chem. Eng. J. 2019, 378, 122116. [Google Scholar] [CrossRef]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, e5340616. [Google Scholar] [CrossRef]
- De Maio, F.; Rosa, E.; Perini, G.; Augello, A.; Niccolini, B.; Ciaiola, F.; Santarelli, G.; Sciandra, F.; Bozzi, M.; Sanguinetti, M.; et al. 3D-Printed Graphene Polylactic Acid Devices Resistant to SARS-CoV-2: Sunlight-Mediated Sterilization of Additive Manufactured Objects. Carbon 2022, 194, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Maleki Dizaj, S.; Eftekhari, A.; Mammadova, S.; Ahmadian, E.; Ardalan, M.; Davaran, S.; Nasibova, A.; Khalilov, R.; Valiyeva, M.; Mehraliyeva, S.; et al. Nanomaterials for Chronic Kidney Disease Detection. Appl. Sci. 2021, 11, 9656. [Google Scholar] [CrossRef]
- Ahmadov, I.S.; Bandaliyeva, A.A.; Nasibova, A.N.; Hasanova, F.V.; Khalilov, R.I. The Synthesis of the Silver Nanodrugs in the Medicinal Plant Baikal Skullcap (Scutellaria baicalensis georgi) and Their Antioxidant, Antibacterial Activity. Adv. Biol. Earth Sci. 2020, 5, 103–118. [Google Scholar]
- Nasibova, A. Generation of nanoparticles in biological systems and their application prospects. Adv. Biol. Earth Sci. 2023, 8, 140–146. [Google Scholar]
- Sandler, N.; Salmela, I.; Fallarero, A.; Rosling, A.; Khajeheian, M.; Kolakovic, R.; Genina, N.; Nyman, J.; Vuorela, P. Towards Fabrication of 3D Printed Medical Devices to Prevent Biofilm Formation. Int. J. Pharm. 2014, 459, 62–64. [Google Scholar] [CrossRef]
- Esposito, M.M.; Turku, S. The Use of Natural Methods to Control Foodborne Biofilms. Pathogens 2023, 12, 45. [Google Scholar] [CrossRef]
- Roy, S.; Chowdhury, G.; Mukhopadhyay, A.K.; Dutta, S.; Basu, S. Convergence of Biofilm Formation and Antibiotic Resistance in Acinetobacter baumannii Infection. Front. Med. 2022, 9, 793615. [Google Scholar] [CrossRef]
- Feng, G.; Cheng, Y.; Wang, S.-Y.; Borca-Tasciuc, D.A.; Worobo, R.W.; Moraru, C.I. Bacterial Attachment and Biofilm Formation on Surfaces Are Reduced by Small-Diameter Nanoscale Pores: How Small Is Small Enough? NPJ Biofilms Microbiomes 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Hunter, I.S. Efficacy of Common Hospital Biocides with Biofilms of Multi-Drug Resistant Clinical Isolates. J. Med. Microbiol. 2008, 57, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.S.; William Costerton, J. Antibiotic Resistance of Bacteria in Biofilms. Lancet 2001, 358, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A. Nosocomial Infections. Vet. Clin. Small Anim. Pract. 2002, 32, 1101–1126. [Google Scholar] [CrossRef]
- Devanga Ragupathi, N.K.; Veeraraghavan, B.; Karunakaran, E.; Monk, P.N. Editorial: Biofilm-Mediated Nosocomial Infections and Its Association with Antimicrobial Resistance: Detection, Prevention, and Management. Front. Med. 2022, 9, 987011. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.S.; Bjarnsholt, T. Risk Factors for Chronic Biofilm-Related Infection Associated with Implanted Medical Devices. Clin. Microbiol. Infect. 2020, 26, 1034–1038. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M.; Murga, R.; Bell, M.; Toscano, C.M.; Carr, J.H.; Novicki, T.J.; Zuckerman, C.; Corey, L.C.; Miller, J.M. Protocol for Detection of Biofilms on Needleless Connectors Attached to Central Venous Catheters. J. Clin. Microbiol. 2001, 39, 750–753. [Google Scholar] [CrossRef] [PubMed]
- Patiniott, P.; Jacombs, A.; Kaul, L.; Hu, H.; Warner, M.; Klosterhalfen, B.; Karatassas, A.; Maddern, G.; Richter, K. Are Late Hernia Mesh Complications Linked to Staphylococci Biofilms? Hernia 2022, 26, 1293–1299. [Google Scholar] [CrossRef]
- Perkowski, K.; Baltaza, W.; Conn, D.B.; Marczyńska-Stolarek, M.; Chomicz, L. Examination of Oral Biofilm Microbiota in Patients Using Fixed Orthodontic Appliances in Order to Prevent Risk Factors for Health Complications. Ann. Agric. Environ. Med. 2019, 26, 231–235. [Google Scholar] [CrossRef]
- Moore, K.; Gupta, N.; Gupta, T.T.; Patel, K.; Brooks, J.R.; Sullivan, A.; Litsky, A.S.; Stoodley, P. Mapping Bacterial Biofilm on Features of Orthopedic Implants In Vitro. Microorganisms 2022, 10, 586. [Google Scholar] [CrossRef]
- Liu, X.; Cao, B.; Yang, L.; Gu, J.-D. Biofilm Control by Interfering with C-Di-GMP Metabolism and Signaling. Biotechnol. Adv. 2022, 56, 107915. [Google Scholar] [CrossRef] [PubMed]
- Mazurek-Popczyk, J.; Nowicki, A.; Arkusz, K.; Pałka, Ł.; Zimoch-Korzycka, A.; Baldy-Chudzik, K. Evaluation of Biofilm Formation on Acrylic Resins Used to Fabricate Dental Temporary Restorations with the Use of 3D Printing Technology. BMC Oral Health 2022, 22, 442. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.-S.; Kim, J.-Y.; Mangal, U.; Seo, J.-Y.; Lee, M.-J.; Jin, J.; Yu, J.-H.; Choi, S.-H. Durable Oral Biofilm Resistance of 3D-Printed Dental Base Polymers Containing Zwitterionic Materials. Int. J. Mol. Sci. 2021, 22, 417. [Google Scholar] [CrossRef] [PubMed]
- Simoneti, D.M.; Pereira-Cenci, T.; dos Santos, M.B.F. Comparison of Material Properties and Biofilm Formation in Interim Single Crowns Obtained by 3D Printing and Conventional Methods. J. Prosthet. Dent. 2022, 127, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Saeed, F.; Muhammad, N.; Khan, A.S.; Sharif, F.; Rahim, A.; Ahmad, P.; Irfan, M. Prosthodontics Dental Materials: From Conventional to Unconventional. Mater. Sci. Eng. C 2020, 106, 110167. [Google Scholar] [CrossRef] [PubMed]
- Mazurek-Popczyk, J.; Palka, L.; Arkusz, K.; Dalewski, B.; Baldy-Chudzik, K. Personalized, 3D- Printed Fracture Fixation Plates versus Commonly Used Orthopedic Implant Materials- Biomaterials Characteristics and Bacterial Biofilm Formation. Injury 2022, 53, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Reichhardt, C.; Jacobs, H.M.; Matwichuk, M.; Wong, C.; Wozniak, D.J.; Parsek, M.R. The Versatile Pseudomonas aeruginosa Biofilm Matrix Protein CdrA Promotes Aggregation through Different Extracellular Exopolysaccharide Interactions. J. Bacteriol. 2020, 202, e00216-20. [Google Scholar] [CrossRef]
- Flemming, H.-C.; van Hullebusch, E.D.; Neu, T.R.; Nielsen, P.H.; Seviour, T.; Stoodley, P.; Wingender, J.; Wuertz, S. The Biofilm Matrix: Multitasking in a Shared Space. Nat. Rev. Microbiol. 2023, 21, 70–86. [Google Scholar] [CrossRef]
- Rizzante, F.; Bueno, T.; Guimarães, G.; Moura, G.; Teich, S.; Furuse, A.; Mendonça, G. Comparative Physical and Mechanical Properties of a 3D Printed Temporary Crown and Bridge Restorative Material. J. Clin. Exp. Dent. 2023, 15, e464–e469. [Google Scholar] [CrossRef]
- Chopra, D.; Jayasree, A.; Guo, T.; Gulati, K.; Ivanovski, S. Random, Aligned and Grassy: Bioactivity and Biofilm Analysis of Zirconia Nanostructures as Dental Implant Modification. Compos. Part B Eng. 2023, 259, 110725. [Google Scholar] [CrossRef]
- Mangal, U.; Min, Y.J.; Seo, J.-Y.; Kim, D.-E.; Cha, J.-Y.; Lee, K.-J.; Kwon, J.-S.; Choi, S.-H. Changes in Tribological and Antibacterial Properties of Poly(Methyl Methacrylate)-Based 3D-Printed Intra-Oral Appliances by Incorporating Nanodiamonds. J. Mech. Behav. Biomed. Mater. 2020, 110, 103992. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, H.; Xu, Y.; Dong, Y.; Shan, W.; Shen, J. Fabrication and Evaluation of Dental Fillers Using Customized Molds via 3D Printing Technology. Int. J. Pharm. 2019, 562, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Bachelet, J.T.; Jouan, R.; Prade, V.; Francisco, C.; Jaby, P.; Gleizal, A. Place of 3D Printing in Facial Epithesis. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Bereket, W.; Hemalatha, K.; Getenet, B.; Wondwossen, T.; Solomon, A.; Zeynudin, A.; Kannan, S. Update on Bacterial Nosocomial Infections. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1039–1044. [Google Scholar]
- Paharik, A.E.; Horswill, A.R. The Staphylococcal Biofilm: Adhesins, Regulation, and Host Response. In Virulence Mechanisms of Bacterial Pathogens; Kudva, I.T., Cornick, N.A., Plummer, P.J., Zhang, Q., Nicholson, T.L., Bannantine, J.P., Bellaire, B.H., Eds.; ASM Press: Washington, DC, USA, 2016; pp. 529–566. ISBN 978-1-68367-071-1. [Google Scholar]
- Zaborowska, M.; Tillander, J.; Brånemark, R.; Hagberg, L.; Thomsen, P.; Trobos, M. Biofilm Formation and Antimicrobial Susceptibility of Staphylococci and Enterococci from Osteomyelitis Associated with Percutaneous Orthopaedic Implants. J. Biomed. Mater. Res. 2017, 105, 2630–2640. [Google Scholar] [CrossRef] [PubMed]
- Koseki, H.; Yonekura, A.; Shida, T.; Yoda, I.; Horiuchi, H.; Morinaga, Y.; Yanagihara, K.; Sakoda, H.; Osaki, M.; Tomita, M. Early Staphylococcal Biofilm Formation on Solid Orthopaedic Implant Materials: In Vitro Study. PLoS ONE 2014, 9, e107588. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Yu, Q.; Sun, H. Novel Strategies for the Prevention and Treatment of Biofilm Related Infections. Int. J. Mol. Sci. 2013, 14, 18488–18501. [Google Scholar] [CrossRef] [PubMed]
- Bjarnsholt, T. Introduction to Biofilms. In Biofilm Infections; Bjarnsholt, T., Jensen, P.Ø., Moser, C., Høiby, N., Eds.; Springer: New York, NY, USA, 2011; pp. 1–9. ISBN 978-1-4419-6083-2. [Google Scholar]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of Orthopedic Implants with Emphasis on Bacterial Adhesion Process and Techniques Used in Studying Bacterial-Material Interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef]
- Darouiche, R.O. Treatment of Infections Associated with Surgical Implants. N. Engl. J. Med. 2004, 350, 1422–1429. [Google Scholar] [CrossRef]
- Oliveira, W.F.; Silva, P.M.S.; Silva, R.C.S.; Silva, G.M.M.; Machado, G.; Coelho, L.C.B.B.; Correia, M.T.S. Staphylococcus aureus and Staphylococcus epidermidis Infections on Implants. J. Hosp. Infect. 2018, 98, 111–117. [Google Scholar] [CrossRef]
- Zheng, Y.; He, L.; Asiamah, T.K.; Otto, M. Colonization of Medical Devices by Staphylococci: Colonization of Medical Devices by Staphylococci. Environ. Microbiol. 2018, 20, 3141–3153. [Google Scholar] [CrossRef] [PubMed]
- Arciola, C.R.; Campoccia, D.; Montanaro, L. Implant Infections: Adhesion, Biofilm Formation and Immune Evasion. Nat. Rev. Microbiol. 2018, 16, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Kiedrowski, M.R.; Horswill, A.R. New Approaches for Treating Staphylococcal Biofilm Infections: Treatments for Staphylococcal Biofilms. Ann. N. Y. Acad. Sci. 2011, 1241, 104–121. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.; Marks, L.R.; Pettigrew, M.M.; Hakansson, A.P. Streptococcus pneumoniae Biofilm Formation and Dispersion during Colonization and Disease. Front. Cell. Infect. Microbiol. 2015, 4, 194. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Luckett, J.; Begines, B.; Dubern, J.-F.; Hook, A.L.; Prina, E.; Rose, F.R.A.J.; Tuck, C.J.; Hague, R.J.M.; Irvine, D.J.; et al. Ink-Jet 3D Printing as a Strategy for Developing Bespoke Non-Eluting Biofilm Resistant Medical Devices. Biomaterials 2022, 281, 121350. [Google Scholar] [CrossRef]
- Rabin, N.; Zheng, Y.; Opoku-Temeng, C.; Du, Y.; Bonsu, E.; Sintim, H.O. Biofilm Formation Mechanisms and Targets for Developing Antibiofilm Agents. Future Med. Chem. 2015, 7, 493–512. [Google Scholar] [CrossRef] [PubMed]
- Shimura, R.; Abe, H.; Yabu, H.; Chien, M.-F.; Inoue, C. Biomimetic Antibiofouling Oil Infused Honeycomb Films Fabricated Using Breath Figures. Polym. J. 2021, 53, 713–717. [Google Scholar] [CrossRef]
- Vivero-Lopez, M.; Xu, X.; Muras, A.; Otero, A.; Concheiro, A.; Gaisford, S.; Basit, A.W.; Alvarez-Lorenzo, C.; Goyanes, A. Anti-Biofilm Multi Drug-Loaded 3D Printed Hearing Aids. Mater. Sci. Eng. C 2021, 119, 111606. [Google Scholar] [CrossRef]
- Xu, X.; Awad, A.; Robles-Martinez, P.; Gaisford, S.; Goyanes, A.; Basit, A.W. Vat Photopolymerization 3D Printing for Advanced Drug Delivery and Medical Device Applications. J. Control. Release 2021, 329, 743–757. [Google Scholar] [CrossRef]
- Kostakioti, M.; Hadjifrangiskou, M.; Hultgren, S.J. Bacterial Biofilms: Development, Dispersal, and Therapeutic Strategies in the Dawn of the Postantibiotic Era. Cold Spring Harb. Perspect. Med. 2013, 3, a010306. [Google Scholar] [CrossRef]
- Parrish, J.M.; Soni, M.; Mittal, R. Subversion of Host Immune Responses by Otopathogens during Otitis Media. J. Leukoc. Biol. 2019, 106, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Robles-Martinez, P.; Xu, X.; Trenfield, S.J.; Awad, A.; Goyanes, A.; Telford, R.; Basit, A.W.; Gaisford, S. 3D Printing of a Multi-Layered Polypill Containing Six Drugs Using a Novel Stereolithographic Method. Pharmaceutics 2019, 11, 274. [Google Scholar] [CrossRef]
- Xu, X.; Robles-Martinez, P.; Madla, C.M.; Joubert, F.; Goyanes, A.; Basit, A.W.; Gaisford, S. Stereolithography (SLA) 3D Printing of an Antihypertensive Polyprintlet: Case Study of an Unexpected Photopolymer-Drug Reaction. Addit. Manuf. 2020, 33, 101071. [Google Scholar] [CrossRef]
- Badica, P.; Batalu, N.D.; Chifiriuc, M.C.; Burdusel, M.; Grigoroscuta, M.A.; Aldica, G.V.; Pasuk, I.; Kuncser, A.; Popa, M.; Agostino, A.; et al. Sintered and 3D-Printed Bulks of MgB2-Based Materials with Antimicrobial Properties. Molecules 2021, 26, 6045. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.H. Magnesium Deficiency and Increased Inflammation: Current Perspectives. J. Inflamm. Res. 2018, 11, 25–34. [Google Scholar] [CrossRef]
- Dickson, A.N.; Abourayana, H.M.; Dowling, D.P. 3D Printing of Fibre-Reinforced Thermoplastic Composites Using Fused Filament Fabrication—A Review. Polymers 2020, 12, 2188. [Google Scholar] [CrossRef] [PubMed]
- Cometta, S.; Jones, R.T.; Juárez-Saldivar, A.; Donose, B.C.; Yasir, M.; Bock, N.; Dargaville, T.R.; Bertling, K.; Brünig, M.; Rakić, A.D.; et al. Melimine-Modified 3D-Printed Polycaprolactone Scaffolds for the Prevention of Biofilm-Related Biomaterial Infections. ACS Nano 2022, 16, 16497–16512. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Ozkan, J.; Willcox, M.D.P. Biocompatibility of Antimicrobial Melimine Lenses: Rabbit and Human Studies. Optom. Vis. Sci. 2014, 91, 570–581. [Google Scholar] [CrossRef]
- Su, Y.; Wang, H.; Mishra, B.; Lakshmaiah Narayana, J.; Jiang, J.; Reilly, D.A.; Hollins, R.R.; Carlson, M.A.; Wang, G.; Xie, J. Nanofiber Dressings Topically Delivering Molecularly Engineered Human Cathelicidin Peptides for the Treatment of Biofilms in Chronic Wounds. Mol. Pharm. 2019, 16, 2011–2020. [Google Scholar] [CrossRef]
- Dutta, D.; Cole, N.; Kumar, N.; Willcox, M.D.P. Broad Spectrum Antimicrobial Activity of Melimine Covalently Bound to Contact Lenses. Invest. Ophthalmol. Vis. Sci. 2013, 54, 175. [Google Scholar] [CrossRef]
- Willcox, M.D.P.; Hume, E.B.H.; Aliwarga, Y.; Kumar, N.; Cole, N. A Novel Cationic-Peptide Coating for the Prevention of Microbial Colonization on Contact Lenses. J. Appl. Microbiol. 2008, 105, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Rasul, R.; Cole, N.; Balasubramanian, D.; Chen, R.; Kumar, N.; Willcox, M.D.P. Interaction of the Antimicrobial Peptide Melimine with Bacterial Membranes. Int. J. Antimicrob. Agents 2010, 35, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Yasir, M.; Dutta, D.; Hossain, K.R.; Chen, R.; Ho, K.K.K.; Kuppusamy, R.; Clarke, R.J.; Kumar, N.; Willcox, M.D.P. Mechanism of Action of Surface Immobilized Antimicrobial Peptides Against Pseudomonas aeruginosa. Front. Microbiol. 2020, 10, 3053. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chu, L.; Yang, S.; Zhang, H.; Qin, L.; Guillaume, O.; Eglin, D.; Richards, R.G.; Tang, T. Dual-Functional 3D-Printed Composite Scaffold for Inhibiting Bacterial Infection and Promoting Bone Regeneration in Infected Bone Defect Models. Acta Biomater. 2018, 79, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, S.; Wang, Y.; Yu, Z.; Ao, H.; Zhang, H.; Qin, L.; Guillaume, O.; Eglin, D.; Richards, R.G.; et al. Anti-Infective Efficacy, Cytocompatibility and Biocompatibility of a 3D-Printed Osteoconductive Composite Scaffold Functionalized with Quaternized Chitosan. Acta Biomater. 2016, 46, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Inzana, J.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. Biomaterials Approaches to Treating Implant-Associated Osteomyelitis. Biomaterials 2016, 81, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-W.; Lee, S.J.; Ko, I.K.; Kengla, C.; Yoo, J.J.; Atala, A. A 3D Bioprinting System to Produce Human-Scale Tissue Constructs with Structural Integrity. Nat. Biotechnol. 2016, 34, 312–319. [Google Scholar] [CrossRef]
- Malaekeh-Nikouei, B.; Fazly Bazzaz, B.S.; Mirhadi, E.; Tajani, A.S.; Khameneh, B. The Role of Nanotechnology in Combating Biofilm-Based Antibiotic Resistance. J. Drug Deliv. Sci. Technol. 2020, 60, 101880. [Google Scholar] [CrossRef]
- Gebreyohannes, G.; Nyerere, A.; Bii, C.; Sbhatu, D.B. Challenges of Intervention, Treatment, and Antibiotic Resistance of Biofilm-Forming Microorganisms. Heliyon 2019, 5, e02192. [Google Scholar] [CrossRef]
- Meng, S.; Qian, Y.; Liu, X.; Wang, Y.; Wu, F.; Wang, W.; Gu, J.-D. Community Structures and Biodeterioration Processes of Epilithic Biofilms Imply the Significance of Micro-Environments. Sci. Total Environ. 2023, 876, 162665. [Google Scholar] [CrossRef]
- Elmowafy, M.; Shalaby, K.; Elkomy, M.H.; Alsaidan, O.A.; Gomaa, H.A.M.; Abdelgawad, M.A.; Mostafa, E.M. Polymeric Nanoparticles for Delivery of Natural Bioactive Agents: Recent Advances and Challenges. Polymers 2023, 15, 1123. [Google Scholar] [CrossRef] [PubMed]
- Cresti, L.; Conte, G.; Cappello, G.; Brunetti, J.; Falciani, C.; Bracci, L.; Quaglia, F.; Ungaro, F.; d’Angelo, I.; Pini, A. Inhalable Polymeric Nanoparticles for Pulmonary Delivery of Antimicrobial Peptide SET-M33: Antibacterial Activity and Toxicity In Vitro and In Vivo. Pharmaceutics 2023, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Yeo, C.K.; Vikhe, Y.S.; Li, P.; Guo, Z.; Greenberg, P.; Duan, H.; Tan, N.S.; Chan-Park, M.B. Hydrogel Effects Rapid Biofilm Debridement with Ex Situ Contact-Kill to Eliminate Multidrug Resistant Bacteria in Vivo. ACS Appl. Mater. Interfaces 2018, 10, 20356–20367. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Li, L.; Kang, X.; Lin, D.; Xiao, Y.; Yang, L.; Jiang, C. Multilayered Upconversion Nanocomposite-Based Photodynamic Hydrogel Dressings for Wound Sterilizing and Healing. ACS Appl. Nano Mater. 2023, 6, 12726–12735. [Google Scholar] [CrossRef]
- Taylor, E.N.; Kummer, K.M.; Dyondi, D.; Webster, T.J.; Banerjee, R. Multi-Scale Strategy to Eradicate Pseudomonas aeruginosa on Surfaces Using Solid Lipid Nanoparticles Loaded with Free Fatty Acids. Nanoscale 2013, 6, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Islan, G.A.; Tornello, P.C.; Abraham, G.A.; Duran, N.; Castro, G.R. Smart Lipid Nanoparticles Containing Levofloxacin and DNase for Lung Delivery. Design and Characterization. Colloids Surf. B Biointerfaces 2016, 143, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.; Abdin, S.M.; Kamal, L.; Orive, G. Nanostructured Lipid Carriers for Delivery of Chemotherapeutics: A Review. Pharmaceutics 2020, 12, 288. [Google Scholar] [CrossRef] [PubMed]
- Francolini, I.; Giansanti, L.; Piozzi, A.; Altieri, B.; Mauceri, A.; Mancini, G. Glucosylated Liposomes as Drug Delivery Systems of Usnic Acid to Address Bacterial Infections. Colloids Surf. B Biointerfaces 2019, 181, 632–638. [Google Scholar] [CrossRef]
- Vera-González, N.; Bailey-Hytholt, C.M.; Langlois, L.; de Camargo Ribeiro, F.; de Souza Santos, E.L.; Junqueira, J.C.; Shukla, A. Anidulafungin Liposome Nanoparticles Exhibit Antifungal Activity against Planktonic and Biofilm Candida albicans. J. Biomed. Mater. Res. Part A 2020, 108, 2263–2276. [Google Scholar] [CrossRef]
- Scriboni, A.B.; Couto, V.M.; Ribeiro, L.N.d.M.; Freires, I.A.; Groppo, F.C.; de Paula, E.; Franz-Montan, M.; Cogo-Müller, K. Fusogenic Liposomes Increase the Antimicrobial Activity of Vancomycin Against Staphylococcus aureus Biofilm. Front. Pharmacol. 2019, 10, 1401. [Google Scholar] [CrossRef]
- Giri, K.; Yepes, L.R.; Duncan, B.; Parameswaran, P.K.; Yan, B.; Jiang, Y.; Bilska, M.; Moyano, D.F.; Thompson, M.A.; Rotello, V.M.; et al. Targeting Bacterial Biofilms via Surface Engineering of Gold Nanoparticles. RSC Adv. 2015, 5, 105551–105559. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Pandit, S.; Beshay, M.; Mokkapati, V.R.S.S.; Garnaes, J.; Olsson, M.E.; Sultan, A.; Mackevica, A.; Mateiu, R.V.; Lütken, H.; et al. Anti-Biofilm Effects of Gold and Silver Nanoparticles Synthesized by the Rhodiola rosea Rhizome Extracts. Artif. Cells Nanomed. Biotechnol. 2018, 46, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Wei, Q.; Wang, Z.; Zhang, G.; Sun, X.; He, Q.-Y. Photocatalytic Protein Damage by Silver Nanoparticles Circumvents Bacterial Stress Response and Multidrug Resistance. mSphere 2019, 4, e00175-19. [Google Scholar] [CrossRef] [PubMed]
- Gordon, O.; Vig Slenters, T.; Brunetto, P.S.; Villaruz, A.E.; Sturdevant, D.E.; Otto, M.; Landmann, R.; Fromm, K.M. Silver Coordination Polymers for Prevention of Implant Infection: Thiol Interaction, Impact on Respiratory Chain Enzymes, and Hydroxyl Radical Induction. Antimicrob. Agents Chemother. 2010, 54, 4208–4218. [Google Scholar] [CrossRef] [PubMed]
- Roe, D.; Karandikar, B.; Bonn-Savage, N.; Gibbins, B.; Roullet, J.-B. Antimicrobial Surface Functionalization of Plastic Catheters by Silver Nanoparticles. J. Antimicrob. Chemother. 2008, 61, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayanan, M.B.; Balachandranath, R.; Genji Srinivasulu, Y.; Kannaiyan, S.K.; Subbiahdoss, G. The Effect of Gold and Iron-Oxide Nanoparticles on Biofilm-Forming Pathogens. Int. Sch. Res. Not. 2013, 2013, e272086. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, E.M.; Abdelgawad, M.A.; Musa, A.; Alotaibi, N.H.; Elkomy, M.H.; Ghoneim, M.M.; Badawy, M.S.E.M.; Taha, M.N.; Hassan, H.M.; Hamed, A.A. Chitosan Silver and Gold Nanoparticle Formation Using Endophytic Fungi as Powerful Antimicrobial and Anti-Biofilm Potentialities. Antibiotics 2022, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Velusamy, P.; Kumar, G.V.; Jeyanthi, V.; Das, J.; Pachaiappan, R. Bio-Inspired Green Nanoparticles: Synthesis, Mechanism, and Antibacterial Application. Toxicol. Res. 2016, 32, 95–102. [Google Scholar] [CrossRef]
- Marassi, V.; Di Cristo, L.; Smith, S.G.J.; Ortelli, S.; Blosi, M.; Costa, A.L.; Reschiglian, P.; Volkov, Y.; Prina-Mello, A. Silver Nanoparticles as a Medical Device in Healthcare Settings: A Five-Step Approach for Candidate Screening of Coating Agents. R. Soc. Open Sci. 2018, 5, 171113. [Google Scholar] [CrossRef]
- Aiello, S.; Pagano, L.; Ceccacci, F.; Simonis, B.; Sennato, S.; Bugli, F.; Martini, C.; Torelli, R.; Sanguinetti, M.; Ciogli, A.; et al. Mannosyl, Glucosyl or Galactosyl Liposomes to Improve Resveratrol Efficacy against Methicillin Resistant Staphylococcus aureus Biofilm. Colloids Surf. A Physicochem. Eng. Asp. 2021, 617, 126321. [Google Scholar] [CrossRef]
- Evangelista, S.d.S.; Guimaraes, N.R.; Garcia, N.B.; dos Santos, S.G.; Oliveira, A.C. de Effectiveness of Manual versus Automated Cleaning on Staphylococcus epidermidis Biofilm Removal from the Surface of Surgical Instruments. Am. J. Infect. Control 2020, 48, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Ding, Y.; Tao, B.; Yuan, Z.; Yang, Y.; Xu, K.; Li, X.; Liu, P.; Cai, K. Surface Modification of Titanium Substrate via Combining Photothermal Therapy and Quorum-Sensing-Inhibition Strategy for Improving Osseointegration and Treating Biofilm-Associated Bacterial Infection. Bioact. Mater. 2022, 18, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Hrynyshyn, A.; Simões, M.; Borges, A. Biofilms in Surgical Site Infections: Recent Advances and Novel Prevention and Eradication Strategies. Antibiotics 2022, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Jamal, M.; Ahmad, W.; Andleeb, S.; Jalil, F.; Imran, M.; Nawaz, M.A.; Hussain, T.; Ali, M.; Rafiq, M.; Kamil, M.A. Bacterial Biofilm and Associated Infections. J. Chin. Med. Assoc. 2018, 81, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Lundin, P.M.; Fiser, B.L.; Blackledge, M.S.; Pickett, H.L.; Copeland, A.L. Functionalized Self-Assembled Monolayers: Versatile Strategies to Combat Bacterial Biofilm Formation. Pharmaceutics 2022, 14, 1613. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; Review on Antimicrobial Resistance; Wellcome Trust: London, UK, 2014. [Google Scholar]
- He, Y.; Abdi, M.; Trindade, G.F.; Begines, B.; Dubern, J.-F.; Prina, E.; Hook, A.L.; Choong, G.Y.H.; Ledesma, J.; Tuck, C.J.; et al. Exploiting Generative Design for 3D Printing of Bacterial Biofilm Resistant Composite Devices. Adv. Sci. 2021, 8, 2100249. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, J.; de Oliveira, R.S.; de Oliveira, T.V.; Velho, M.C.; Konrad, M.V.; da Silva, G.S.; Deon, M.; Beck, R.C.R. 3D Printing and Nanotechnology: A Multiscale Alliance in Personalized Medicine. Adv. Funct. Mater. 2021, 31, 2009691. [Google Scholar] [CrossRef]
- Van Alin, A.; Corbett, M.K.; Fathollahzadeh, H.; Tjiam, M.C.; Rickard, W.D.A.; Sun, X.; Putnis, A.; Eksteen, J.; Kaksonen, A.H.; Watkin, E. Biofilm Formation on the Surface of Monazite and Xenotime during Bioleaching. Microb. Biotechnol. 2023, 16, 1790–1802. [Google Scholar] [CrossRef]
Figure 1.
Biofilm formation, in which planktonic bacteria aggregate into complex layers connected by extracellular polymeric substances that enhance resistance abilities, causes persistent issues in the medical field.
Figure 1.
Biofilm formation, in which planktonic bacteria aggregate into complex layers connected by extracellular polymeric substances that enhance resistance abilities, causes persistent issues in the medical field.

Figure 2.
Development of devices with zwitterionic surfaces serves as potent antimicrobials as they repel proteins and thus reduce the attachment potential of EPS in biofilms. Red arrows represent attracted charges and blue arrows represent repulsion. Green color represents negative charges and blue color represents positive charges.
Figure 2.
Development of devices with zwitterionic surfaces serves as potent antimicrobials as they repel proteins and thus reduce the attachment potential of EPS in biofilms. Red arrows represent attracted charges and blue arrows represent repulsion. Green color represents negative charges and blue color represents positive charges.


{kind=link}
{kind=link}
Table 1.
Summary of Biofilm prevention benefits of 3D printing and nanotechnologies in the medical field when utilized for reusable medical device development and implants.
Table 1.
Summary of Biofilm prevention benefits of 3D printing and nanotechnologies in the medical field when utilized for reusable medical device development and implants.
| Technology | Biofilm-Prevention Use/Benefit | References |
|---|---|---|
| 3D Printing |
| [23,27,28,29,30,32,33,52,53,67] |
| Nanotechnology |
| [70,73,74,76,77,78,83,84,85,86,87] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Esposito, M.M.; Glazer, J.R.; Turku, S. The Use of 3D Printing and Nanotechnologies to Prevent and Inhibit Biofilms on Medical Devices. Hygiene 2023, 3, 325-338. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene3030024
AMA Style
Esposito MM, Glazer JR, Turku S. The Use of 3D Printing and Nanotechnologies to Prevent and Inhibit Biofilms on Medical Devices. Hygiene. 2023; 3(3):325-338. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene3030024
Chicago/Turabian StyleEsposito, Michelle Marie, Jonathan Robert Glazer, and Sara Turku. 2023. "The Use of 3D Printing and Nanotechnologies to Prevent and Inhibit Biofilms on Medical Devices" Hygiene 3, no. 3: 325-338. https://0-doi-org.brum.beds.ac.uk/10.3390/hygiene3030024