

A Single Dose of Microencapsulated Cocoa Supplementation Does Not Speed up Muscle Force Recovery after Eccentric Exercise-Induced Muscle Damage: A Placebo-Controlled, Double-Blind, Crossover Study

Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Experimental Design
2.3. Nutritional Supplementation and Dietary Control
2.4. Exercise-Induce Muscle Damage Protocol
2.5. Maximal Voluntary Contraction Measurement
2.6. Blood Sample Analysis
2.7. Delayed Onset Muscle Soreness (DOMS) Measurement
2.8. Statistical Analysis
3. Results
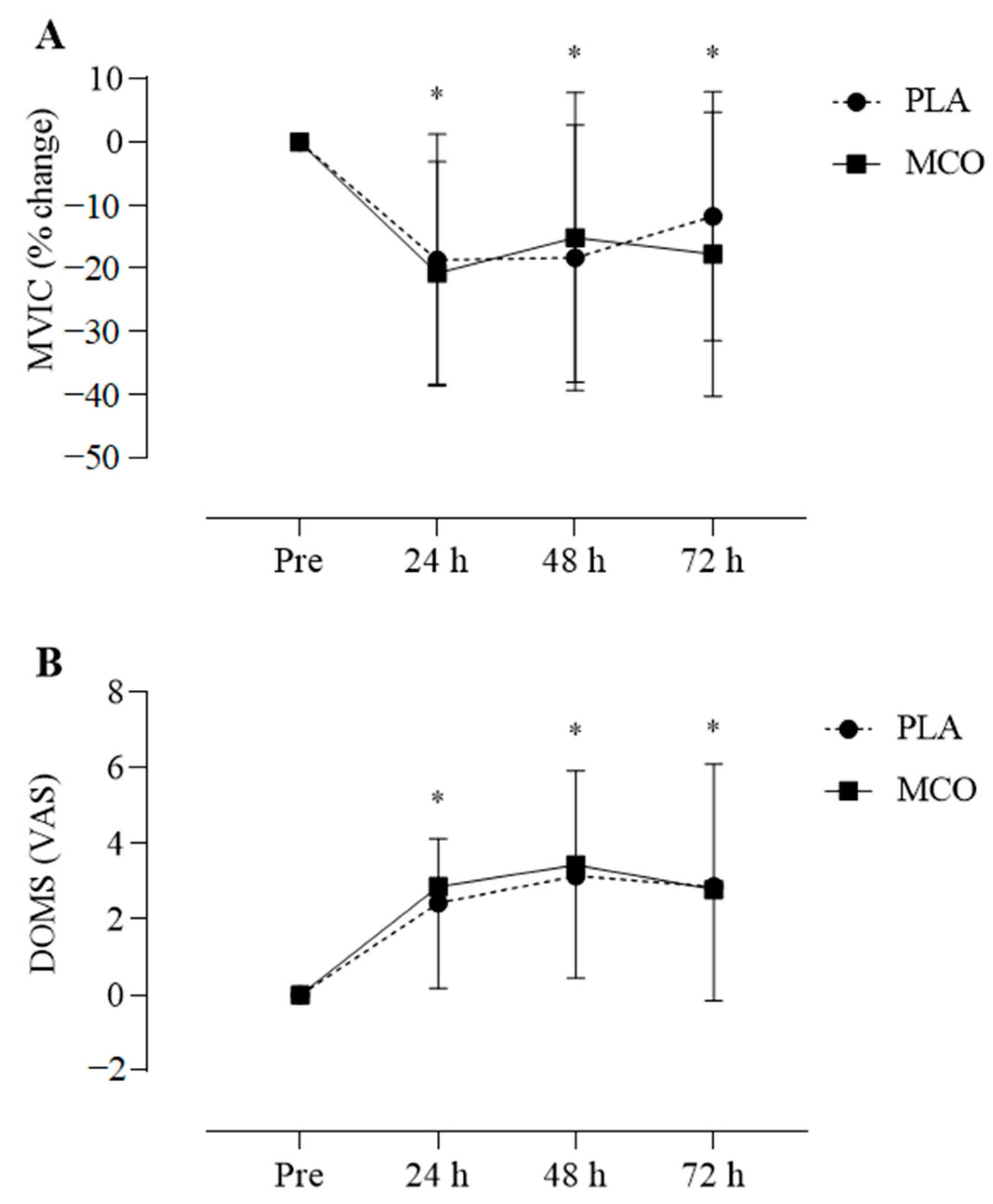
3.1. Isometric Muscle Performance
3.2. Blood Markers
3.3. Muscle Soreness
4. Discussion
Experimental Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CF | Cocoa Flavanol |
| CRP | C-reactive protein |
| DOMS | Delayed onset muscle soreness |
| EIMD | Exercise-induced muscle damage |
| GSH | Reduced glutathione |
| HPLC | High-performance liquid chromatography |
| Mb | Myoglobin |
| MCO | Microencapsulated cocoa |
| MDA | Malondialdehyde |
| MVIC | Maximal voluntary isometric contractions |
| PLA | Placebo |
| ROS | Reactive oxygen species |
| TBA | 2-Thiobarbituric |
| VAS | Visual analogic scale |
References
- Clarkson, P.M.; Hubal, M.J. Exercise-induced muscle damage in humans. Am. J. Phys. Med. Rehabil. 2002, 81 (Suppl. 11), S52–S69. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.J.; Twist, C.; Cobley, J.N.; Howatson, G.; Close, G.L. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? Eur. J. Sport Sci. 2019, 2, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Stožer, A.; Vodopivc, P.; Bombek, L.K. Pathophysiology of exercise-induced muscle damage and its structural, functional, metabolic, and clinical consequences. Physiol. Res. 2020, 26, 565–598. [Google Scholar] [CrossRef] [PubMed]
- Carey, C.C.; Lucey, A.; Doyle, L. Flavonoid Containing Polyphenol Consumption and Recovery from Exercise-Induced Muscle Damage: A Systematic Review and Meta-Analysis. Sports Med. 2021, 9, 1293–1316. [Google Scholar] [CrossRef] [PubMed]
- Sorrenti, V.; Fortinguerra, S.; Caudullo, G.; Buriani, A. Deciphering the role of polyphenols in sports performance: From nutritional genomics to the gut microbiota toward phytonutritional epigenomics. Nutrients 2020, 29, 1265. [Google Scholar] [CrossRef] [PubMed]
- Bowtell, J.; Kelly, V. Fruit-Derived Polyphenol Supplementation for Athlete Recovery and Performance. Sports Med. 2019, 22, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Marika, M.; Scoditti, E.; Carluccio, M.A.; Kaltsatou, A.; Cicchella, A. Effect of cocoa products and its polyphenolic constituents on exercise performance and exercise-induced muscle damage and inflammation: A review of clinical trials. Nutrients 2019, 28, 1471. [Google Scholar]
- Corr, L.D.; Field, A.; Pufal, D.; Clifford, T.; Harper, L.D.; Naughton, R.J. The effects of cocoa flavanols on indices of muscle recovery and exercise performance: A narrative review. BMC Sports Sci. Med. Rehabilitation. 2021, 14, 90. [Google Scholar] [CrossRef]
- Steinbacher, P.; Eckl, P. Impact of oxidative stress on exercising skeletal muscle. Biomolecules 2015, 5, 356–377. [Google Scholar] [CrossRef]
- Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Rémésy, C. Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies. Am. J. Clin. Nutr. 2005, 81 (Suppl. 1), 230S–242S. [Google Scholar] [CrossRef]
- D’Archivio, M.; Filesi, C.; Varì, R.; Scazzocchio, B.; Masella, R. Bioavailability of the polyphenols: Status and controversies. Int. J. Mol. Sci. 2010, 31, 1321–1342. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Mcdougall, G.J.; Alegría, A.; Alminger, M.; Arrigoni, E.; Aura, A.M.; Brito, C.; Cilla, A.; El, S.; Karakaya, S.; et al. Mind the gap-deficits in our knowledge of aspects impacting the bioavailability of phytochemicals and their metabolites-a position paper focusing on carotenoids and polyphenols. Mol. Nutr. Food Res. 2015, 3, 1307–1323. [Google Scholar] [CrossRef] [PubMed]
- Bento-Silva, A.; Koistinen, V.M.; Mena, P.; Bronze, M.R.; Hanhineva, K.; Sahlstrøm, S.; Sahlstrøm, S.; Kitrytė, V.; Moco, S.; Aura, A.-M.; et al. Factors affecting intake, metabolism and health benefits of phenolic acids: Do we understand individual variability? Eur. J. Nutr. 2020, 21, 1275–1293. [Google Scholar] [CrossRef]
- Landberg, R.; Manach, C.; Kerckhof, F.M.; Minihane, A.M.; Saleh, R.N.M.; De Roos, B.; Tomas-Barberan, F.; Morand, C.; Van de Wiele, T. Future prospects for dissecting inter-individual variability in the absorption, distribution and elimination of plant bioactives of relevance for cardiometabolic endpoints. Eur. J. Nutr. 2019, 23, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Mena, P.; Bresciani, L.; Brindani, N.; Ludwig, I.A.; Pereira-Caro, G.; Angelino, D.; Llorach, R.; Calani, L.; Brighenti, F.; Clifford, M.N.; et al. Phenyl-γ-valerolactones and phenylvaleric acids, the main colonic metabolites of flavan-3-ols: Synthesis, analysis, bioavailability, and bioactivity. Nat. Prod. Rep. 2019, 36, 714–752. [Google Scholar] [CrossRef] [PubMed]
- Polia, F.; Pastor-Belda, M.; Martínez-Blázquez, A.; Horcajada, M.N.; Tomás-Barberán, F.A.; García-Villalba, R. Technological and Biotechnological Processes To Enhance the Bioavailability of Dietary (Poly)phenols in Humans. J. Agric. Food Chem. 2022, 23, 2092–2107. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Oliver, M.; Ponce-Alquicira, E. The Role of Microencapsulation in Food Application. Molecules 2022, 23, 1499. [Google Scholar] [CrossRef]
- Fang, Z.; Bhandari, B. Encapsulation of polyphenols—A review. Trends Food Sci. Technol. 2010, 21, 510–523. [Google Scholar] [CrossRef]
- Vitaglione, P.; Barone Lumaga, R.; Ferracane, R.; Sellitto, S.; Morelló, J.R.; Reguant Miranda, J.; Shimoni, E.; Fogliano, V. Human bioavailability of flavanols and phenolic acids from cocoa-nut creams enriched with free or microencapsulated cocoa polyphenols. Br. J. Nutr. 2013, 28, 1832–1843. [Google Scholar] [CrossRef]
- Chen, T.C. Variability in muscle damage after eccentric exercise and the repeated bout effect. Res. Q. Exerc. Sport 2006, 77, 362–371. [Google Scholar] [CrossRef]
- Sansone, R.; Ottaviani, J.I.; Rodriguez-Mateos, A.; Heinen, Y.; Noske, D.; Spencer, J.P.; Crozier, A.; Merx, M.W.; Kelm, M.; Schroeter, H.; et al. Methylxanthines enhance the effects of cocoa flavanols on cardiovascular function: Randomized, double-masked controlled studies. Am. J. Clin. Nutr. 2017, 105, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.T.; Wollman, P.M.; Jackman, S.R.; Bowtell, J.L. Flavanol-rich cacao mucilage juice enhances recovery of power but not strength from intensive exercise in healthy, young men. Sports 2018, 6, 159. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rangel, J.C.; Benavides, J.; Heredia, J.B.; Cisneros-Zevallos, L.; Jacobo-Velázquez, D.A. The Folin-Ciocalteu assay revisited: Improvement of its specificity for total phenolic content determination. Anal. Methods 2013, 5, 5990–5999. [Google Scholar] [CrossRef]
- Wabaidur, S.M.; Obbed, M.S.; Alothman, Z.A.; Alfaris, N.A.; Badjah-Hadj-ahmed, A.Y.; Siddiqui, M.R.; Altamimi, J.Z.; Aldayel, T.S. Total phenolic acids and flavonoid contents determination in yemeni honey of various floral sources: Folin-ciocalteu and spectrophotometric approach. Food Sci. Technol. 2020, 40, 647–652. [Google Scholar] [CrossRef]
- Giustarini, D.; Dalle-Donne, I.; Milzani, A.; Fanti, P.; Rossi, R. Analysis of GSH and GSSG after derivatization with N-ethylmaleimide. Nat. Protoc. 2013, 1, 1660–1669. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.; Mikkelsen, B.B.; Nielsen, J.B.; Andersen, H.R.; Grandjean, P. Plasma malondialdehyde as biomarker for oxidative stress: Reference interval and effects of life-style factors. Clin. Chem. 1997, 43, 1209–1214. [Google Scholar] [CrossRef]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Gomez-Cabrera, M.C.; Carretero, A.; Millan-Domingo, F.; Garcia-Dominguez, E.; Correas, A.G.; Olaso-Gonzalez, G.; Vina, J. Redox-related biomarkers in physical exercise. Redox Biol. 2021, 42, 101956. [Google Scholar] [CrossRef]
- Morillas-Ruiz, J.M.; Villegas García, J.A.; López, F.J.; Vidal-Guevara, M.L.; Zafrilla, P. Effects of polyphenolic antioxidants on exercise-induced oxidative stress. Clin. Nutr. 2006, 25, 444–453. [Google Scholar] [CrossRef]
- Reid, M.B. Redox interventions to increase exercise performance. J. Physiol. 2016, 15, 5125–5133. [Google Scholar] [CrossRef]
- Moopanar, T.R.; Allen, D.G. Reactive oxygen species reduce myofibrillar Ca2+ sensitivity in fatiguing mouse skeletal muscle at 37 °C. J. Physiol. 2005, 564, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Jackson, M.J. Exercise-induced oxidative stress: Cellular mechanisms and impact on muscle force production. Physiol. Rev. 2008, 88, 1243–1276. [Google Scholar] [CrossRef] [PubMed]
- Schramm, D.D.; Wang, J.F.; Holt, R.R.; Ensunsa, J.L.; Gonsalves, J.L.; Lazarus, S.A.; Schmitz, H.H.; German, J.B.; Keen, C.L. Chocolate procyanidins decrease the leukotriene-prostacyclin ratio in humans and human aortic endothelial cells. Am. J. Clin. Nutr. 2001, 1, 36–40. [Google Scholar] [CrossRef]
- Vázquez-Agell, M.; Urpi-Sarda, M.; Sacanella, E.; Camino-López, S.; Chiva-Blanch, G.; Llorente-Cortés, V.; Tobias, E.; Roura, E.; Andres-Lacueva, C.; Lamuela-Raventos, R.M.; et al. Cocoa consumption reduces NF-κB activation in peripheral blood mononuclear cells in humans. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Decroix, L.; Soares, D.D.; Meeusen, R.; Heyman, E.; Tonoli, C. Cocoa Flavanol Supplementation and Exercise: A Systematic Review. Sports Med. 2018, 3, 867–892. [Google Scholar] [CrossRef] [PubMed]
- Vlachojannis, J.; Erne, P.; Zimmermann, B.; Chrubasik-Hausmann, S. The Impact of Cocoa Flavanols on Cardiovascular Health. Phytother. Res. 2016, 30, 1641–1657. [Google Scholar] [CrossRef] [PubMed]
- Decroix, L.; Tonoli, C.; Soares, D.D.; Descat, A.; Drittij-Reijnders, M.J.; Weseler, A.R.; Bast, A.; Stahl, W.; Heyman, E.; Meeusen, R. Acute cocoa Flavanols intake has minimal effects on exercise-induced oxidative stress and nitric oxide production in healthy cyclists: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2017, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- Wiswedel, I.; Hirsch, D.; Kropf, S.; Gruening, M.; Pfister, E.; Schewe, T.; Sies, H. Flavanol-rich cocoa drink lowers plasma F2-isoprostane concentrations in humans. Free Radic. Biol. Med. 2004, 37, 411–421. [Google Scholar] [CrossRef]
- Fraga, C.G.; Actis-Goretta, L.; Ottaviani, J.I.; Carrasquedo, F.; Lotito, S.B.; Lazarus, S.; Schmitz, H.H.; Keen, C.L. Regular consumption of a flavanol-rich chocolate can improve oxidant stress in young soccer players. Clin. Dev. Immunol. 2005, 12, 11–17. [Google Scholar] [CrossRef]
- Taub, P.R.; Ramirez-Sanchez, I.; Patel, M.; Higginbotham, E.; Moreno-Ulloa, A.; Román-Pintos, L.M.; Phillips, P.; Perkins, G.; Ceballos, G.; Villarreal, F. Beneficial effects of dark chocolate on exercise capacity in sedentary subjects: Underlying mechanisms. A double blind, randomized, placebo controlled trial. Food Funct. 2016, 7, 3686–3693. [Google Scholar] [CrossRef]
- Allgrove, J.; Farrell, E.; Gleeson, M.; Williamson, G.; Cooper, K. Regular dark chocolate consumption’s reduction of oxidative stress and increase of free-fatty-acid mobilization in response to prolonged cycling. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Davison, G.; Callister, R.; Williamson, G.; Cooper, K.A.; Gleeson, M. The effect of acute pre-exercise dark chocolate consumption on plasma antioxidant status, oxidative stress and immunoendocrine responses to prolonged exercise. Eur. J. Nutr. 2012, 5, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Decroix, L.; Tonoli, C.; Lespagnol, E.; Balestra, C.; Descat, A.; Drittij-Reijnders, M.J.; Blackwell, J.R.; Stahl, W.; Jones, A.M.; Weseler, A.R.; et al. One-week cocoa flavanol intake increases prefrontal cortex oxygenation at rest and during moderate-intensity exercise in normoxia and hypoxia. J. Appl. Physiol. 2018, 1, 8–18. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, F.G.; Fisher, M.G.; Thornley, T.T.; Roemer, K.; Pritchett, R.; de Freitas, E.C.; Pritchett, K. Cocoa flavanol effects on markers of oxidative stress and recovery after muscle damage protocol in elite rugby players. Nutrition 2019, 62, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Donia, T.; Khamis, A. Management of oxidative stress and inflammation in cardiovascular diseases: Mechanisms and challenges. Environ. Sci. Pollut. Res. 2021, 8, 34121–34153. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, L.; Hill, J.A.; Jehnali, A.; Dunbar, J.; Brouner, J.; McHugh, M.P.; Howatson, G. Influence of a montmorency cherry juice blend on indices of exercise-induced stress and upper respiratory tract symptoms following marathon running—A pilot investigation. J. Int. Soc. Sports Nutr. 2015, 12, 22. [Google Scholar] [CrossRef]
- Phillips, T.; Childs, A.C.; Dreon, D.M.; Phinney, S.; Leeuwenburgh, C. A Dietary Supplement Attenuates IL-6 and CRP after Eccentric Exercise in Untrained Males. Med. Sci. Sports Exerc. 2003, 35, 2032–2037. [Google Scholar] [CrossRef]
- Peschek, K.; Pritchett, R.; Bergman, E.; Pritchett, K. The effects of acute post exercise consumption of two cocoa-based beverages with varying flavanol content on indices of muscle recovery following downhill treadmill running. Nutrients 2013, 20, 50–62. [Google Scholar] [CrossRef]
- Corr, L.D.; Field, A.; Pufal, D.; Killey, J.; Clifford, T.; Harper, L.D.; Naughton, R.J. Acute Consumption of Varied Doses of Cocoa Flavanols Does Not Influence Exercise-Induced Muscle Damage. Int. J. Sport Nutr. Exerc. Metab. 2020, 1, 338–344. [Google Scholar] [CrossRef]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 1, 757–767. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Male | Female |
|---|---|---|
| N Age (years) | 7 28 ± 5 | 7 27 ± 4 |
| Body mass (kg) | 75.7 ± 8.3 | 58.6 ± 7.5 |
| Height (m) | 1.72 ± 0.06 | 1.60 ± 0.06 |
| Body Mass Index (kg/m2) | 24.7 ± 2.8 | 22.6 ± 1.8 |
| Resistance training experience (years) | 6 ± 2 | 3 ± 1 |
| Nutrient | Value | %DR * | ||
|---|---|---|---|---|
| PLA | MCO | PLA | MCO | |
| Energy content (Kcal/kJ) | 93/387 | 49/205 | 4.6 | 2.5 |
| Carbohydrates (g) | 21 | 11 | 7.1 | 3.7 |
| Proteins (g) | 1.0 | 2.5 | 1.3 | 3.3 |
| Total fat (g) | 0 | 1.2 | 0 | 2.2 |
| Dietary fiber (g) | 0.9 | 3.4 | 3.5 | 14 |
| Sodium (mg) | 35 | 3.8 | 1.5 | 0.2 |
| Total flavonoids | 8 | 75 | - | - |
| Total polyphenols | 9 | 240 | - | - |
| PLA | MCO | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-EIMD | 2 h | 24 h | 48 h | 72 h | Pre-EIMD | 2 h | 24 h | 48 h | 72 h | |
| Blood markers | ||||||||||
| C-reactive protein (mg·L−1) | 0.9 ± 0.4 | 2.1 ± 1.3 * | 1.6 ± 1.4 | 1.4 ± 1.2 | 1.2 ± 1.1 | 1.0 ± 0.6 | 2.3 ± 1.6 * | 1.5 ± 1.2 | 1.4 ± 1.5 | 1.2 ± 1.3 |
| Malondialdehyde (µmol·L−1) | 23.1 ± 9.8 | 24.3 ± 16.9 | 19.5 ± 10.4 | 24.6 ± 17.0 | 26.1 ± 11.1 | 26.5 ± 12.8 | 27.2 ± 11.1 | 28.0 ± 19.1 | 20.4 ± 8.1 | 20.8 ± 7.9 |
| Myoglobin (ng·mL−1) | 18.6 ± 3.3 | 36.4 ± 25.8 * | 28.6 ± 20.8 | 84.9 ± 119.1 * | 97.8 ± 130.8 * | 19.4 ± 5.2 | 32.0 ± 17.1 * | 29.1 ± 29.6 | 108.1 ± 129.1 * | 120.6 ± 156.7 * |
| Reduced glutathione (µmol·L−1) | 0.7 ± 0.4 | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.8 ± 0.4 | 0.8 ± 0.3 | 0.8 ± 0.4 | 0.8 ± 0.3 | 0.7 ± 0.3 | 0.8 ± 0.4 | 0.8 ± 0.3 |
| Isometric muscle performance | ||||||||||
| MVIC (Nm) | 54.4 ± 24.7 | - | 45.9 ± 27.0 * | 45.9 ± 26.6 * | 48.6 ± 26.1 * | 53.4 ± 22.0 | - | 44.9 ± 24.8 * | 48.4 ± 28.5 * | 47.6 ± 29.0 * |
| MVIC (% change) | 100 ± 0.0 | - | 82.2 ± 20.5 * | 80.3 ± 22.5 * | 87.9 ± 21.4 * | 100 ± 0.0 | - | 79.3 ± 17.7 * | 82.9 ± 23.9 * | 80.7 ± 22.7 * |
| Muscle soreness | ||||||||||
| DOMS (VAS) | 0 ± 0 | - | 2 ± 2 * | 3 ± 3 * | 3 ± 3 * | 0 ± 0 | - | 3 ± 2 * | 3 ± 3 * | 3 ± 3 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Junior, O.J.F.R.; dos Santos, K.S.; Tavares, I.R.G.; de Oliveira, G.V.; Alvares, T.S. A Single Dose of Microencapsulated Cocoa Supplementation Does Not Speed up Muscle Force Recovery after Eccentric Exercise-Induced Muscle Damage: A Placebo-Controlled, Double-Blind, Crossover Study. Appl. Biosci. 2024, 3, 1-13. https://0-doi-org.brum.beds.ac.uk/10.3390/applbiosci3010001
Junior OJFR, dos Santos KS, Tavares IRG, de Oliveira GV, Alvares TS. A Single Dose of Microencapsulated Cocoa Supplementation Does Not Speed up Muscle Force Recovery after Eccentric Exercise-Induced Muscle Damage: A Placebo-Controlled, Double-Blind, Crossover Study. Applied Biosciences. 2024; 3(1):1-13. https://0-doi-org.brum.beds.ac.uk/10.3390/applbiosci3010001
Chicago/Turabian StyleJunior, Olavo João Frederico Ramos, Karen Souza dos Santos, Isabela Ribeiro Grangeira Tavares, Gustavo Vieira de Oliveira, and Thiago Silveira Alvares. 2024. "A Single Dose of Microencapsulated Cocoa Supplementation Does Not Speed up Muscle Force Recovery after Eccentric Exercise-Induced Muscle Damage: A Placebo-Controlled, Double-Blind, Crossover Study" Applied Biosciences 3, no. 1: 1-13. https://0-doi-org.brum.beds.ac.uk/10.3390/applbiosci3010001