
Multimedication Guidelines: Assessment of the Size of the Target Group for Medication Review and Description of the Frequency of Their Potential Drug Safety Problems with Routine Data

 ,
,
Abstract
:1. Introduction
2. Results
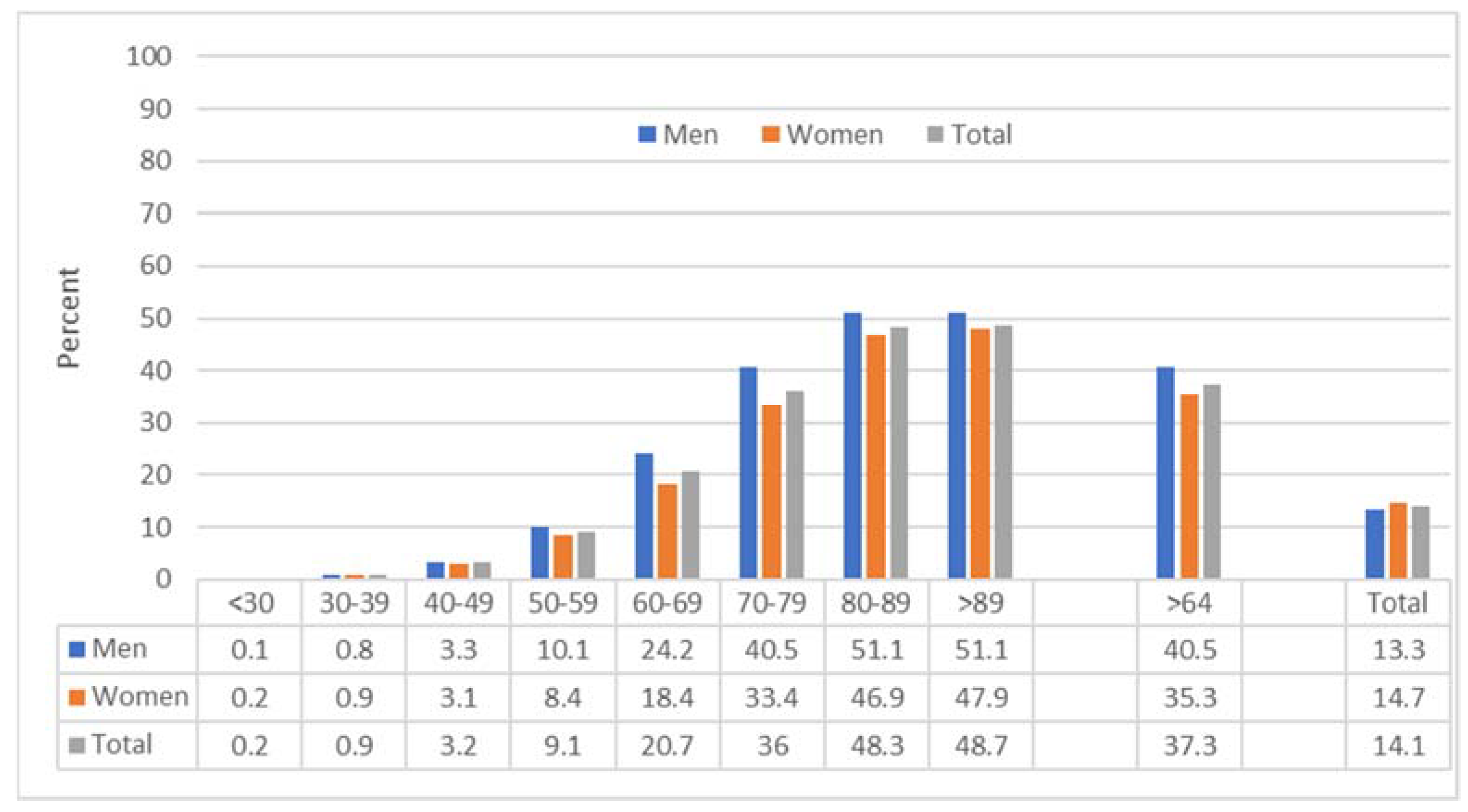
2.1. Prevalence of Polypharmacy and Multimorbidity
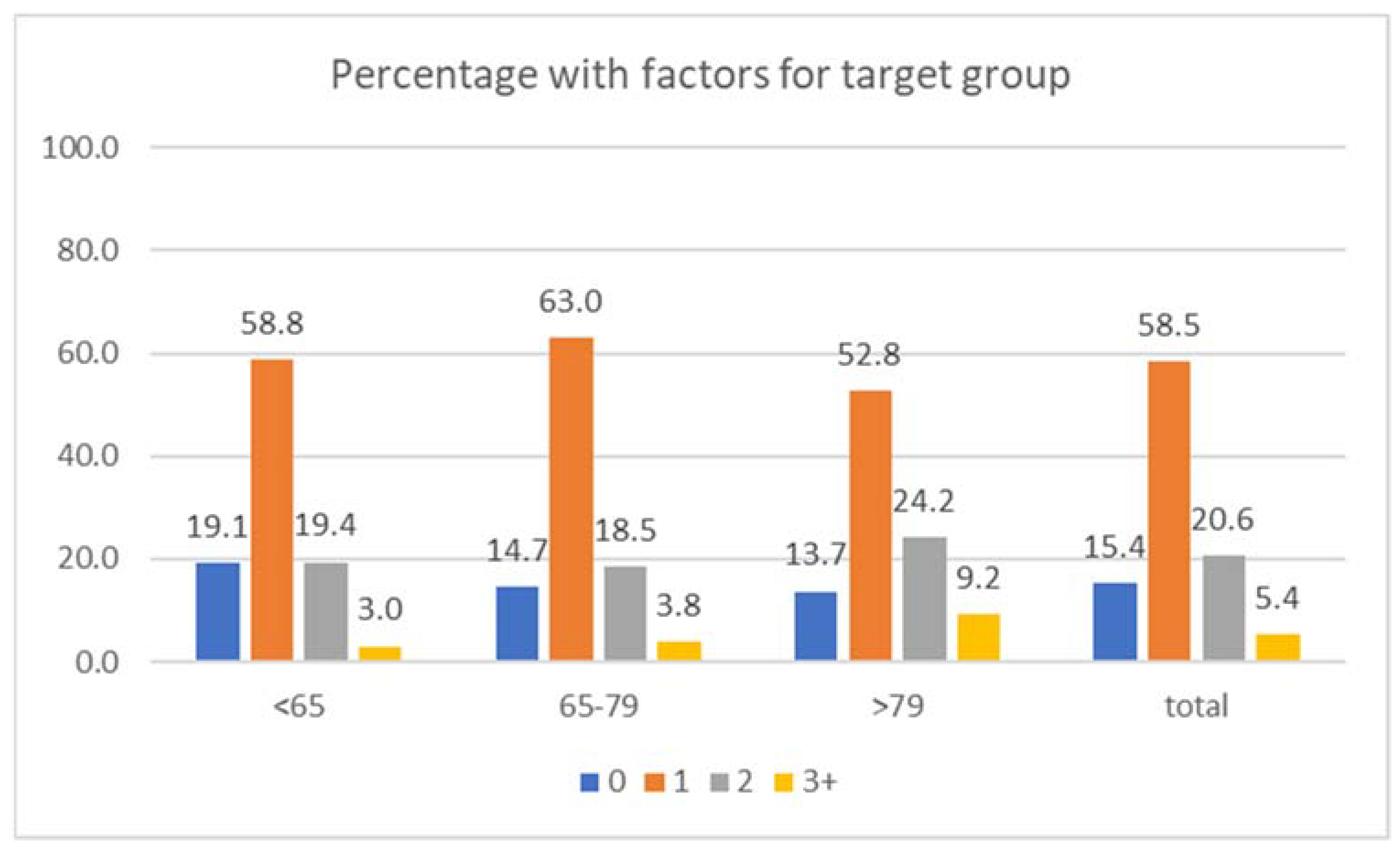
2.2. Target Group for Medication Review
- Almost 80% of the patients had contact with three or more different physician groups;
- In total, 17.4% had two or more hospitalizations;
- In total, 2.5% had inpatient nursing care for the first time;
- In total, 9.1% received at least one prescription for a psychotropic drug (men: 6.6%; women 10.8%);
- In total, 10% of the study population had a diagnosis of dementia or a corresponding prescription.
2.3. Aspects of Medication Safety
- About 30% of the population with multimorbidity and polypharmacy aged 65 years and older received at least one prescription with a drug classified as potentially inadequate for the elderly according to the PRISCUS list [17], the German PIM list. Better alternatives or special monitoring are recommended for these drugs.
- Overall, 29% (men: 25.7%, women: 31.1%) of the analyzed population with multimorbidity and polypharmacy received a drug with known drug-induced prolongation of the QT interval as a feared adverse and potentially life-threatening effect.
- Benzodiazepines, but also the so-called Z-drugs (zopiclone, zolpidem, and zaleplon), have a risk of drug dependence and should therefore only be prescribed for a short time. About 11% of the study population received at least one prescription of these agents (benzodiazepines: 7.7%; Z-drugs 4.5%).
- Across all age groups, treatment prevalence with PPI in the study population was around 52% in 2019; the mean daily dose was 442 DDD (around 8% received the therapy rather short-term, i.e., up to one quarter; around 18% of the insured persons received a prescription quantity that allowed for treatment with at least two DDD daily over the whole year (data not presented)).
3. Discussion
3.1. Polypharmacy Prevalence
3.2. Risk Situations and Occasions for Medication Review
3.3. Medication Safety Issues in Patients with Polypharmacy
- The prescription of PIM is analyzed in many countries [29,30], though changes in everyday practice seem to be difficult [31,32]. Overall, 30% of the study population had at least one prescription classified as PIM, with a higher percentage of women compared to men, among other reasons due to the higher prescribing of psychotropics in women [33].
- The risk of QT interval prolongation increases in the presence of multimedication [34]. The frequency of prescribing drugs that prolong the QT interval might be underestimated by practitioners due to lack of information. In the population under study, almost 29% received least one non-cardiac drug with this potential adverse drug effect. The prevalence estimate is influenced by the population studied and the drugs included. Comparison with other studies is hampered by differences in the study population and numbers of drugs included. Schaechtele et al. report for a cohort of 130,434 geriatric patients (mean age 81 years, 67% women) a treatment prevalence of 58.7% for drugs associated with any QT risk (ALL-QT) and 17.2% for drugs classified as a high-QT-risk drug [35]. Our analysis was restricted to non-cardiac drugs. The German guidelines for “multimedication” urges having an ECG performed in patients with QT-time-prolonging drugs.
- Benzodiazepine or Z-drugs with their risk of increasing falls and drug dependence are often prescribed for too-long periods. Prevalence estimates are not only influenced by the characteristics of the population studied, but also by reimbursement schemes or prescribing recommendations. A recently published study analyzed the use of benzodiazepines and other hypnotics in multimorbid older people (≥2 chronic diseases) in the province of Quebec (Canada) with routine data [36]. Despite a decline since 2000, almost 31% still received at least one prescription in 2016. A study from Spain [37] reports a prevalence of 28.4% for patients with polypharmacy—a joint prescription of five or more drugs—in 2015. The prevalence in our study is much lower (7.7%), which could partly be due to private prescribing not included in routine data or a more restrained prescription.
- Potential for deprescribing is not only seen for benzodiazepine or Z-drugs, but also for proton pump inhibitors. Internationally, this problem of overprescribing has been also addressed [38,39,40,41]. The above-cited study from Spain identified PPI as the most prescribed drug with 63.3% (2015) [37]. PPIs were also prescribed most frequently in our study: 52% received at least one prescription. Medication review helps to detect the correctness of indication.
- Drug combinations such as renin inhibitors together with diuretics and NSAIDs increase the risk of renal failure [18] and should be avoided. In the presented analysis, 16% of the study population received this combination, which demonstrates, among other measures, the necessity for medication reviews. The percentage of patients at risk is underestimated in our analysis, as NSAIDs in self-medication could not be included.
- Anticholinergic drugs are an important issue for the medication review, as they can lead to a variety of health problems and adverse drug effects, especially in the elderly [42]. During medication review, physicians should discuss alternatives with the patients. According to the risk scale of Rudolph et al. (2008) [19], 25% of the study population received at least one drug, and about 6% received a drug with strong anticholinergic effects. Comparable to the analysis of QT drugs, prevalence estimates are influenced by the characteristics of the population under study and the drugs or risk scale included. Krueger et al. (2021) reported a prevalence of anticholinergic drug use according to the list of Carnahan et al. (2006) [43] of 38.4%, and 53.7% applying the German list of Kiesel et al. (2018) [44] for a patients with at least three diagnosed chronic diseases and aged between 65 and 85 years [45]. The authors point out the need to be aware of the cumulative effects of the use of several lower potential anticholinergic drugs, which in turn leads to high anticholinergic burden.
3.4. Strength and Limitation
4. Materials and Methods
- Contact with different physician groups: Physician groups are identified by the lifetime doctor’s number (8th and 9th position of the 9-digit code). Diagnosing physicians such as microbiologists and radiologists, as well as pathologists and unknown specialty were omitted. Different subgroups of a specialty were combined into a group.
- Number of hospital stays: Hospital stays with at least one overnight stay in the observation year 2019 were included. Overlapping or immediately following hospital stays were counted as one hospital stay.
- First time of inpatient nursing care: First-time inpatient care was assumed if patients with multimorbidity and polypharmacy had only outpatient care or no care in the 92-day quarter prior to their first day of inpatient care in the observation year.
- Prescribing of psychotropic drugs: prescriptions with ATC Code N05 and N06, excluding N05BP, N05CP, N05H, N06AH, N06AP (= herbal or homoeopathic drugs) and N06D (= antidementia drugs).
- Patients with dementia: Documentation of the ICD-10 diagnoses G30 (Alzheimer’s disease) or F00 to F03 (dementia) or at least one prescription of an antidementia drug (ATC code N06D)
- Frequency of drug utilization: Potentially inadequate medication according to PRISCUS list [12], QT-drugs (Table A1), benzodiazepines and Z-drugs (ATC codes: N05BA, N05CF), proton pump inhibitors (ATC codes A02BC), “triple whammy” combination: prescribing of agents acting on the renin–angiotensin system (ATC-code: C09A or C09C, or C09XA and diuretics (ATC codes: C03 or C02L or C07B/-C/-D or C08G) and antiphlogistics (ATC codes: M01A und NSAID in other groups).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Indication | Active Substances (Examples) |
|---|---|
| Antibiotics | azithromycin, clarithromycin, erythromycin, ciprofloxacin, levofloxacin, moxifloxacin, ofloxacin, trimethoprim-sulfamethoxazole |
| Antidepressants | amitriptyline, citalopram, escitalopram, doxepin, fluoxetine, imipramine |
| Antiemetics | granisetron, ondansetron |
| Antihistamines | terfenadine |
| Antimycotics | fluconazole, ketoconazole |
| Antipsychotics | chlorpromazine, clozapine, droperidol, fluphenazine, haloperidol, olanzapine, pimozide, paliperidone, quetiapine, risperidone |
| Antiasthmatic agents | salbutamol, salmeterol, terbutaline |
| Antiprotozoals | quinine, chloroquine, mefloquine, pentamidine |
| other | amantadine, amiodaron, alfuzosin, octreotide, tacrolimus, tamoxifen, vardenafil |
| Number and Percentage (%) of Study Population 1 with Prescription | ||
|---|---|---|
| Drug Group | n | % |
| ACE inhibitor/sartan/renin inhibitor | 1,028,867 | 80.9 |
| plus diuretic * | 730,253 | 57.4 |
| plus diuretic and NSAID * | 199,992 | 15.7 |
References
- Bergert, F.W.; Braun, M.; Ehrenthal, K.; Feßler, J.; Gross, J.; Hüttner, U.; Kluthe, B.; Liesenfeld, A.; Seffrin, J.; Vetter, G.; et al. Recommendations for treating adult and geriatric patients on multimedication. Int. J. Clin. Pharmacol. Ther. 2014, 52 (Suppl. S1), 1–64. [Google Scholar] [CrossRef] [PubMed]
- Leitliniengruppe Hessen; DEGAM. S3-Leitlinie Multimedikation (AWMF-Reg-Nr. 053-04). 2021. Available online: https://www.awmf.org/uploads/tx_szleitlinien/053-043l_S3_Multimedikation_2021-08.pdf (accessed on 2 February 2022).
- Nederlands Huisartsen Genootschap. Multidisciplinaire Richtlijn Polyfarmacie bij Ouderen. 2012, p. 199. Available online: https://www.nhg.org/themas/publicaties/multidisciplinaire-richtlijn-polyfarmacie-bij-ouderen (accessed on 2 February 2022).
- National Institute for Health Care Excellence (NICE). Medicines Optimisation: The Safe and Effective Use of Medicines to Enable the Best Possible Outcomes 2015. Available online: https://www.nice.org.uk/guidance/ng5/evidence/full-guideline-pdf-6775454 (accessed on 22 February 2022).
- National Institute for Health and Care Excellence (NICE). Multimorbidity: Clinical Assessment and Management. Multimorbidity: Assessment, Prioritisation and Management of Care for People with Commonly Occurring Multimorbidity. NICE Guideline NG56. 2016. Available online: https://www.nice.org.uk/guidance/ng56/evidence (accessed on 22 February 2022).
- National Institute for Health Care Excellence (NICE). Older People with Social Care Needs and Multiple Long-Term Conditions. 2015. Available online: https://www.nice.org.uk/guidance/ng22/evidence/full-guideline-pdf-552742669 (accessed on 22 February 2022).
- AGS. Guiding principles for the care of older adults with multimorbidity: An approach for clinicians: American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. J. Am. Geriatr. Soc. 2012, 60, E1–E25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, C.M.; Darer, J.; Boult, C.; Fried, L.P.; Boult, L.; Wu, A.W. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: Implications for pay for performance. JAMA 2005, 294, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, D.; Mangin, D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: Addressing polypharmacy. Arch. Intern. Med. 2010, 170, 1648–1654. [Google Scholar] [CrossRef] [Green Version]
- Woodward, M.C. Deprescribing: Achieving Better Health Outcomes for Older People through Reducing Medications. J. Pharm. Pract. Res. 2003, 33, 323–328. [Google Scholar] [CrossRef]
- Amelung, S.; Bender, B.; Meid, A.; Walk-Fritz, S.; Hoppe-Tichy, T.; Haefeli, W.E.; Seidling, H.M. Wie vollständig ist der Bundeseinheitliche Medikationsplan? Eine Analyse bei Krankenhausaufnahme. DMW 2020, 145, e116–e122. [Google Scholar] [CrossRef]
- Peralta-Pedrero, M.L.; Valdivia-Ibarra, F.J.; Hernández-Manzano, M.; Medina-Beltrán, G.R.; Cordero-Guillén, M.A.; Baca-Zúñiga, J.; Cruz-Avelar, A.; Aguilar-Salas, I.; Avalos-Mejía, A.M. Clinical practice guideline. Drug prescription in elderly. Rev. Med. Inst. Mex. Seguro Soc. 2013, 51, 228–239. [Google Scholar]
- Schubert, I.; Fessler, J.; Harder, S.; Dhin, T.S.; Brueckle, M.-S.; Muth, C.; The EVITA Study Group. Multimedication in Family Doctor Practice: The German Evidence-based Guideline “Multimedication”. Pharmacoepidemiology 2022, in press. [Google Scholar]
- Anderson, K.; Stowasser, D.; Freeman, C.; Scott, I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: A systematic review and thematic synthesis. BMJ Open 2014, 4, e006544. [Google Scholar] [CrossRef]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef] [Green Version]
- Khezrian, M.; McNeil, C.J.; Murray, A.; Myint, P.K. An overview of prevalence, determinants and health outcomes of polypharmacy. Ther. Adv. Drug Saf. 2020, 11, 2042098620933741. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.; Schmiedl, S.; Thürmann, P.A. Potenziell inadäquate Medikation für ältere Menschen: Die PRISCUS-Liste. Dtsch. Arztebl. Int. 2010, 107, 543–551. [Google Scholar] [PubMed]
- Lapi, F.; Azoulay, L.; Yin, H.; Nessim, S.J.; Suissa, S. Concurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: Nested case-control study. BMJ 2013, 346, e8525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The Anticholinergic Risk Scale and Anticholinergic Adverse Effects in Older Persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midão, L.; Giardini, A.; Menditto, E.; Kardas, P.; Costa, E. Polypharmacy prevalence among older adults based on the survey of health, ageing and retirement in Europe. Arch. Gerontol. Geriatr. 2018, 78, 213–220. [Google Scholar] [CrossRef]
- Scottish Government Polypharmacy Model of Care Group. Polypharmacy Guidance, Realistic Prescribing, 3rd ed.; Scottish Government: Edinburgh, Scotland, 2018; Available online: https://www.therapeutics.scot.nhs.uk/wp-content/¬uploads/2018/04/-Polypharmacy-Guidance-2018.pdf (accessed on 2 March 2022).
- Guillot, J.; Maumus-Robert, S.; Pariente, A.; Bezin, J. Chronic polypharmacy at all age: A population-based drug utilization study. Fundam. Clin. Pharmacol. 2021, 36, 405–413. [Google Scholar] [CrossRef]
- Guillot, J.; Maumus-Robert, S.; Bezin, J. Polypharmacy: A general review of definitions, descriptions and determinants. Therapie 2019, 75, 407–416. [Google Scholar] [CrossRef]
- Sirois, C.; Domingues, N.S.; Laroche, M.-L.; Zongo, A.; Lunghi, C.; Guénette, L.; Kröger, E.; Émond, V. Polypharmacy Definitions for Multimorbid Older Adults Need Stronger Foundations to Guide Research, Clinical Practice and Public Health. Pharmacy 2019, 7, 126. [Google Scholar] [CrossRef] [Green Version]
- Lappe, V.; Ihle, P.; Schubert, I. Multimedikation im Alter: Versorgungsrealität und Leitlinienempfehlungen. Gesundheitswesen 2016, 78, A82. [Google Scholar] [CrossRef]
- Jokanovic, N.; Tan, E.C.K.; Dooley, M.J.; Kirkpatrick, C.M.; Bell, J.S. Prevalence and factors associated with polypharmacy in long-term care facilities: A systematic review. J. Am. Med. Dir. Assoc. 2015, 16, 535.e1–535.e12. [Google Scholar] [CrossRef]
- Johnell, K.; Jonasdottir Bergman, G.; Fastbom, J.; Danielsson, B.; Borg, N.; Salmi, P. Psychotropic drugs and the risk of fall injuries, hospitalisations and mortality among older adults. Int. J. Geriatr. Psychiatry 2017, 32, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huisartsen, N.; Genootschap Namens de Werkgroep van de Module Medicatiebeoordeling. Budget Impact Analysis: Impact en Kosten van Aanbevelingen van de Module Medicatiebeoordeling in de Eerste lijn bij de Multidisciplinaire Richtlijn Polyfarmacie bij Ouderen. Utrecht. 2020. Available online: https://richtlijnendatabase.nl/gerelateerde_documenten/f/20117/-Rapportage%20BIA.pdf (accessed on 23 February 2022).
- Renom-Guiteras, A.; Meyer, G.; Thürmann, P.A. The EU(7)-PIM list: A list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur. J. Clin. Pharmacol. 2015, 71, 861–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Geriatric Society Beers Criteria Update Expert Panel. American Geriatric Society 2019 Updated AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- Schmiedl, S.; Rottenkolber, M.; Szymanski, J.; Drewelow, B.; Siegmund, W.; Hippius, M.; Farker, K.; Guenther, I.R.; Hasford, J.; Thuermann, P.A.; et al. Preventable ADRs leading to hospitalization—Results of a long-term prospective safety study with 6,427 ADR cases focusing on elderly patients. Expert Opin. Drug Saf. 2018, 17, 125–137. [Google Scholar] [CrossRef]
- Rantsi, M.; Hyttinen, V.; Jyrkkä, J.; Vartiainen, A.-K.; Kankaanpää, E. Process evaluation of implementation strategies to reduce potentially inappropriate medication prescribing in older population: A scoping review. Res. Soc. Adm. Pharm. 2022, 18, 2367–2391. [Google Scholar] [CrossRef] [PubMed]
- Schubert, I.; Küpper-Nybelen, J.; Ihle, P.; Thürmann, P. Prescribing potentially inappropriate medication (PIM) in Germany’s elderly as indicated by the PRISCUS list. An analysis based on regional claims data. Pharmacoepidemiol. Drug Saf. 2013, 22, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Khan, Q.; Ismail, M.; Haider, I.; Khan, F. Prevalence of QT interval prolonging drug–drug interactions (QT-DDIs) in psychiatry wards of tertiary care hospitals in Pakistan: A multicenter cross-sectional study. Int. J. Clin. Pharm. 2017, 39, 1256–1264. [Google Scholar] [CrossRef] [PubMed]
- Schächtele, S.; Tümena, T.; Gaßmann, K.-G.; Fromm, M.F.; Maas, R. Co-Prescription of QT-Interval Prolonging Drugs: An Analysis in a Large Cohort of Geriatric Patients. PLoS ONE 2016, 11, e0155649. [Google Scholar] [CrossRef]
- Gosselin, E.; Simard, M.; Lunghi, C.; Sirois, C. Trends in benzodiazepine and alternative hypnotic use in relation with multimorbidity among older adults in Quebec, Canada. Pharmacoepidemiol. Drug Saf. 2022, 31, 322–333. [Google Scholar] [CrossRef]
- Hernández-Rodríguez, M.; Sempere-Verdú, E.; Vicens-Caldentey, C.; González-Rubio, F.; Miguel-García, F.; Palop-Larrea, V.; Orueta-Sánchez, R.; Esteban-Jiménez, Ó.; Sempere-Manuel, M.; Arroyo-Aniés, M.; et al. Drug Prescription Profiles in Patients with Polypharmacy in Spain: A Large-Scale Pharmacoepidemiologic Study Using Real-World Data. Int. J. Environ. Res. Public Health 2021, 18, 4754. [Google Scholar] [CrossRef]
- Rane, P.P.; Guha, S.; Chatterjee, S.; Aparasu, R.R. Prevalence and predictors of non-evidence based proton pump inhibitor use among elderly nursing home residents in the US. Res. Soc. Adm. Pharm. 2017, 13, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Forgacs, I.; Loganayagam, A. Overprescribing proton pump inhibitors. BMJ 2008, 336, 2–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Othman, F.; Card, T.R.; Crooks, C.J. Proton pump inhibitor prescribing patterns in the UK: A primary care database study. Pharmacoepidemiol. Drug Saf. 2016, 25, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Heidelbaugh, J.J.; Kim, A.H.; Chang, R.; Walker, P.C. Overutilization of proton-pump inhibitors: What the clinician needs to know. Ther. Adv. Gastroenterol. 2012, 5, 219–232. [Google Scholar] [CrossRef] [Green Version]
- Nishtala, P.S.; Salahudeen, M.S.; Hilmer, S.N. Anticholinergics: Theoretical and clinical overview. Expert Opin. Drug Saf. 2016, 15, 753–768. [Google Scholar] [CrossRef]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Culp, K.R. The Anticholinergic Drug Scale as a Measure of Drug-Related Anticholinergic Burden: Associations with Serum Anticholinergic Activity. J. Clin. Pharmacol. 2006, 46, 1481–1486. [Google Scholar] [CrossRef]
- Kiesel, E.K.; Hopf, Y.M.; Drey, M. An anticholinergic burden score for German prescribers: Score development. BMC Geriatr. 2018, 18, 239. [Google Scholar] [CrossRef] [Green Version]
- Krüger, C.; Schäfer, I.; van den Bussche, H.; Bickel, H.; Fuchs, A.; Gensichen, J.; König, H.-H.; Maier, W.; Mergenthal, K.; Riedel-Heller, S.G.; et al. Anticholinergic drug burden according to the anticholinergic drug scale and the German anticholinergic burden and their impact on cognitive function in multimorbid elderly German people: A multicentre observational study. BMJ Open 2021, 11, e044230. [Google Scholar] [CrossRef]
- Hoffmann, F.; Icks, A. Structural differences between health insurance funds and their impact on health services research: Results from the Bertelsmann Health-Care Monitor. Gesundheitswesen 2012, 74, 291–297. [Google Scholar] [CrossRef]
- Busse, R.; Blümel, M.; Knieps, F.; Bärnighausen, T. Statutory health insurance in Germany: A health system shaped by 135 years of solidarity, self-governance, and competition. Lancet 2017, 390, 882–897. [Google Scholar] [CrossRef] [Green Version]
- Deutsches Institut für medizinische Dokumentation und Information (DIMDI) im Auftrag des Bundesministeriums für Gesundheit. 10. Revision. ICD 10-GM 2019. Internationale Statistische Klassifikation der Krankheiten und Verwandter Gesundheitsprobleme. 2019. Contract No.: 02.11. Available online: https://www.dimdi.de/static/de/klassifikationen/icd/icd-10-gm/kode-suche/htmlgm2019/ (accessed on 8 February 2022).
- Swart, E.; Ihle, P.; Gothe, H. Gute Praxis Sekundärdatenanalyse (GPS). Die 2. Revision. Das. Gesundh. 2005, 67, P38. [Google Scholar] [CrossRef] [PubMed]
- Drug and Therapeutics Bulletin. QT interval and drug therapy. BMJ 2016, 353, i2732, Erratum in BMJ 2016, 354, i4331. [Google Scholar]


| Percentage (%) of Insured Persons with Multimorbidity and Polypharmacy 1 | ||||||
|---|---|---|---|---|---|---|
| Five or More Active Substances Over at Least | 10 or More Active Substances Over at Least… | |||||
| Age group | 91 days | 182 days | 273 days | 91 days | 182 days | 273 days |
| <50 | 1.0 | 0.6 | 0.3 | 0.1 | 0.0 | 0.0 |
| 50–59 | 9.1 | 6.0 | 3.7 | 0.7 | 0.4 | 0.2 |
| 60–69 | 20.7 | 14.7 | 9.7 | 2.2 | 1.1 | 0.5 |
| 70–79 | 36.0 | 26.6 | 17.8 | 4.1 | 2.0 | 0.8 |
| 80–89 | 48.3 | 36.1 | 23.8 | 5.0 | 2.1 | 0.8 |
| >89 | 48.7 | 34.3 | 21.0 | 3.3 | 1.1 | 0.3 |
| <65 | 4.7 | 3.1 | 1.9 | 0.4 | 0.2 | 0.1 |
| >64 | 37.3 | 27.5 | 18.2 | 4.0 | 1.8 | 0.7 |
| 65–79 | 31.7 | 23.3 | 15.6 | 3.6 | 1.7 | 0.8 |
| >79 | 48.4 | 35.8 | 23.3 | 4.7 | 1.9 | 0.7 |
| Total | 14.1 | 10.2 | 6.6 | 1.4 | 0.7 | 0.3 |
| Percentage (%) of Insured Persons with Multimorbidity and Polypharmacy 1 and Utilization/Documentation of… | ||||||
|---|---|---|---|---|---|---|
| Sex | Age Group | at Least Three Different Physician Groups | Two or More Hospitalizations | First time Inpatient Nursing Care | Psychotropics | Dementia |
| Men | <65 | 69.7 | 13.8 | 0.4 | 11.8 | 1.2 |
| 65–79 | 79.8 | 18.1 | 1.1 | 4.9 | 6.2 | |
| >79 | 81.2 | 23.6 | 4.5 | 4.6 | 19.5 | |
| total | 77.5 | 18.5 | 1.9 | 6.6 | 8.6 | |
| Women | <65 | 82.5 | 12.8 | 0.4 | 18.0 | 1.0 |
| 65–79 | 82.2 | 15.2 | 1.4 | 8.8 | 5.9 | |
| >79 | 72.4 | 20.4 | 6.0 | 8.9 | 22.3 | |
| total | 78.7 | 16.6 | 2.9 | 10.8 | 10.9 | |
| Total | <65 | 76.6 | 13.2 | 0.4 | 15.1 | 1.1 |
| 65–79 | 81.2 | 16.4 | 1.2 | 7.1 | 6.1 | |
| >79 | 75.4 | 21.5 | 5.5 | 7.4 | 21.4 | |
| total | 78.2 | 17.4 | 2.5 | 9.1 | 10.0 | |
| Percentage (%) of the Insured Patients with Multimorbidity and Polypharmacy 1 and at Least One Prescription of… | |||||
|---|---|---|---|---|---|
| Sex | Age Group | PIM * | QT-Drug ** | Benzodiazepine/Z-Drug *** | PPI **** |
| Men | <65 | n.a. | 27.5 | 8.5 | 48.5 |
| 65–79 | 23.7 | 24.0 | 7.3 | 47.0 | |
| >79 | 26.5 | 26.9 | 10.2 | 49.7 | |
| total | 24.8 | 25.7 | 8.4 | 48.2 | |
| Women | <65 | n.a. | 37.5 | 12.6 | 55.1 |
| 65–79 | 32.8 | 28.5 | 11.3 | 53.6 | |
| >79 | 35.5 | 30.4 | 14.9 | 57.5 | |
| total | 34.0 | 31.1 | 12.9 | 55.3 | |
| Total | <65 | n.a. | 32.9 | 10.7 | 52.0 |
| 65–79 | 28.9 | 26.6 | 9.6 | 50.8 | |
| >79 | 32.4 | 29.2 | 13.2 | 54.8 | |
| total | 30.4 | 28.9 | 11.1 | 52.4 | |
| Percentage (%) of the Insured Patients with Multimorbidity and Polypharmacy 1 with Anticholinergic Prescription * According to Degree of Anticholinergic Effects | |||||||
|---|---|---|---|---|---|---|---|
| <65 Years | 65–79 Years | >79 Years | Total | ||||
| Degree of | men | women | men | women | men | women | |
| anticholinergic effects | % | ||||||
| 1 | 17.7 | 24.8 | 13.7 | 19.0 | 17.5 | 24.7 | 19.7 |
| 2 | 4.7 | 5.4 | 3.3 | 3.5 | 3.0 | 3.0 | 3.7 |
| 3 | 6.1 | 10.9 | 3.7 | 6.8 | 3.9 | 6.5 | 6.3 |
| Total ** | 24.0 | 34.1 | 18.0 | 25.4 | 21.8 | 30.5 | 25.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lappe, V.; Dinh, T.S.; Harder, S.; Brueckle, M.-S.; Fessler, J.; Marschall, U.; Muth, C.; Schubert, I.; on behalf of the EVITA Study Group. Multimedication Guidelines: Assessment of the Size of the Target Group for Medication Review and Description of the Frequency of Their Potential Drug Safety Problems with Routine Data. Pharmacoepidemiology 2022, 1, 12-25. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010002
Lappe V, Dinh TS, Harder S, Brueckle M-S, Fessler J, Marschall U, Muth C, Schubert I, on behalf of the EVITA Study Group. Multimedication Guidelines: Assessment of the Size of the Target Group for Medication Review and Description of the Frequency of Their Potential Drug Safety Problems with Routine Data. Pharmacoepidemiology. 2022; 1(1):12-25. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010002
Chicago/Turabian StyleLappe, Veronika, Truc Sophia Dinh, Sebastian Harder, Maria-Sophie Brueckle, Joachim Fessler, Ursula Marschall, Christiane Muth, Ingrid Schubert, and on behalf of the EVITA Study Group. 2022. "Multimedication Guidelines: Assessment of the Size of the Target Group for Medication Review and Description of the Frequency of Their Potential Drug Safety Problems with Routine Data" Pharmacoepidemiology 1, no. 1: 12-25. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010002