
Multimedication in Family Doctor Practices: The German Evidence-Based Guidelines on Multimedication

 ,
,
Abstract
:1. Introduction
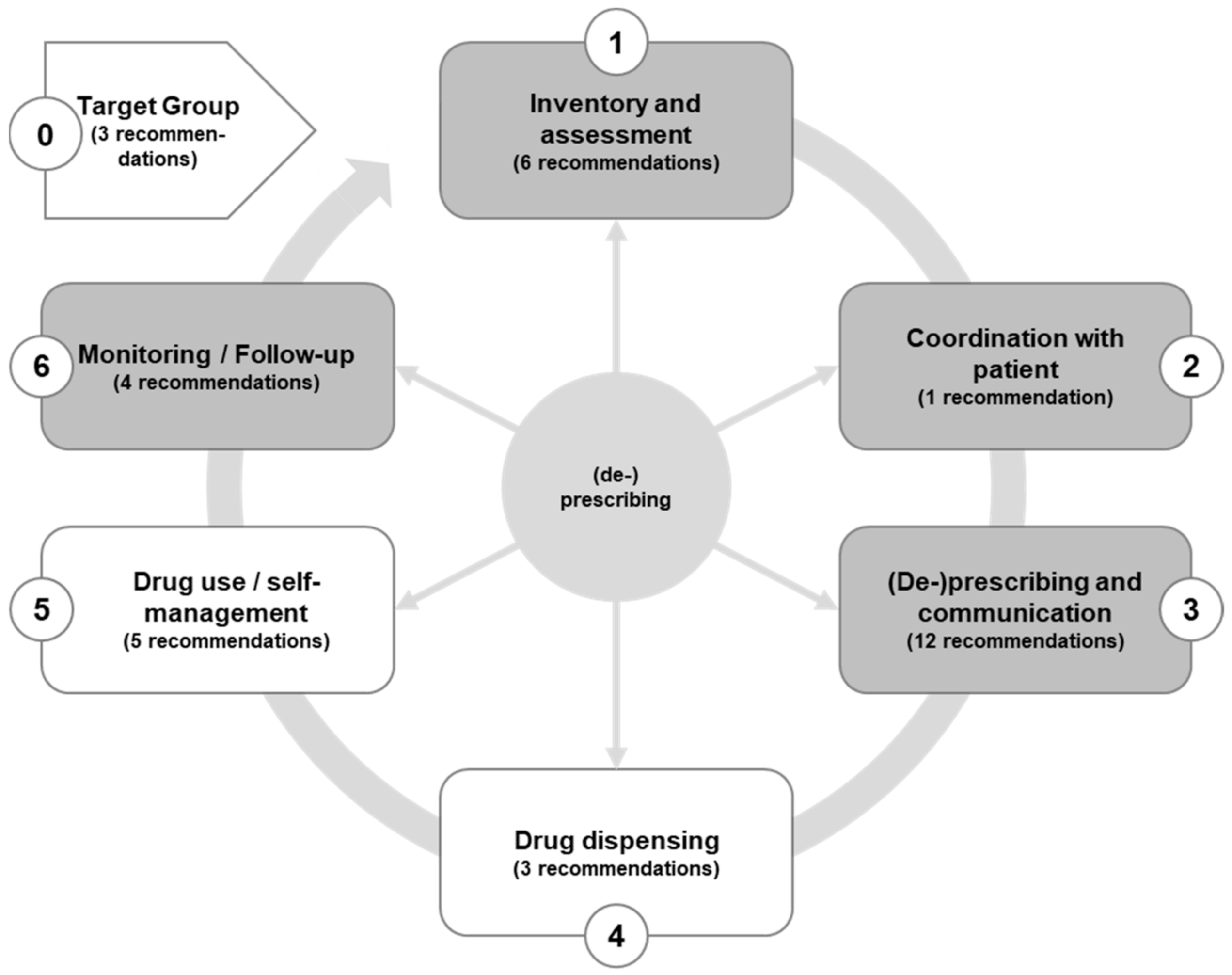
2. Results

2.1. Target Groups for a Medication Review
- Implement a practice routine to record patients who meet the criteria for a medication review. Set up the call to the patient record so that an alert window automatically appears, indicating if and when the medication check is required.
2.2. Inventory and Assessment (Step 1)
- Record the current medication including over-the-counter drugs (OTC)—if necessary, by means of a medication plan and brown bag. In practice, this can be done very easily, using a commercially available scanner. This makes it possible to record the medicines in the patient’s file, to carry out interaction checks, and to update the medication plan;
- Arrange a separate appointment in the practice, to which the patient (or a caregiver) brings all medicines (including self-medication) and package inserts from home;
- Home visits are also a good opportunity to gain an overview of the drugs available, the handling of the medication (use of daily or weekly dosettes, blisters), and any application problems;
- Ask the patient about their medication regime, and whether they understand the information. Ask or check whether the medication plan is also filled in by other specialists or a pharmacy;
- Ask the patient about application problems, e.g., whether they have been able to cope with their previous medication, and whether there are problems with the application of such medicines, such as opening packages, counting drops, and dividing and taking tablets (e.g., swallowing). Ask the patient whether they have changed the dosage on their own, or whether they have tried to stop taking the medicine (questions to assess adherence can be found in the guidelines);
- Ask the patient whether they have been in contact with other doctors or other health professionals since the last consultation, and, if so, what the results were.
- It is advisable for all patients to regularly check the drug dosage according to the instructions in the Summary of Product Characteristics (SPC);
- Do you have up-to-date information on the patient’s renal function in your patient records?
- Is the patient receiving a medicine for which a dose adjustment is necessary?
- Is the maximum permissible dosage being adhered to?
2.3. Coordination with the Patient (Step 2)
- To recognize situations in which patients with multimorbidity have to make a preference-sensitive decision, i.e., have to weigh between different options;
- Ensuring that patients are adequately informed about the benefits and harms of treatment options;
- Preferences should be asked only after sufficient information has been provided;
- The level of involvement in decision making should be asked for, not guessed.
- What complaints do you have?
- What is the significance of the complaints for you? Can you live with it? How much are you affected?
- What is your strongest complaint?
- Which complaints restrict you in your everyday life or contact?
- What do you no longer dare to do? What do you feel strongly limited in? What would you like to be able to do again?
- Have you often felt down or hopeless in the past month? Have you often found little joy in the things you do in the past month?
- What do you need help with? Do you miss people whom you can trust and whose help you can count on?
- This medicine can prolong your life or can prevent the following complications..... Question for patients: What side effects are you willing to accept in return? What risks are you willing to accept?
- Check if necessary: Is there reliable information for the age or target group whether the drug prolongs life or prevents complications?
2.4. Prescription Proposal and Communication (Step 3)
- Contraindications or intolerable adverse drug reactions (e.g., interactions) occur;
- The reason for the prescription (indication) no longer exists;
- Non-therapeutically indicated duplicate prescriptions occur in an indication group;
- A recommended duration of treatment has been exceeded.
- Actively ask the patient for the medication plan;
- Talk to them about the importance of recording other doctors’ medication as well as self-medication;
- Many patients neither know the names of their medications nor do they have their medication schedule with them regularly. Digital solutions are being considered, but have not yet been implemented. These patients can be advised to take pictures of the medication plan or medication boxes with their mobile. Prescriptions from other doctors or OTC preparations can also be recorded in this way.
2.5. Drug Dispensing, Drug Use, and Self-Management (Step 4, 5 and 6)
- Use the advantages of simplified therapy. Reduce the number of drugs (e.g., through combination preparations, prioritization). Simplify dosage and offer aids for taking medication—as far as pharmaceutically possible and suitable for the patient (e.g., dosettes). To improve adherence, preference should be given, where possible, to medicines that can be administered once;
- Pass on information verbally and in writing, e.g., medication plan, patient information;
- Point out possibilities for useful self-monitoring (e.g., weight control, blood glucose measurements) and show how to use inhalers or pens;
- Individualize measures for taking medication or doing exercises, e.g., special reminder tricks. Form habits (ritualization), e.g., always take tablets before dessert or going to bed (if no other instructions);
- Patients should be reminded of the importance of their therapy at every visit;
- Explain risk factors and antismoking measures;
- Explain side effects that experience has shown often lead to non-adherence (e.g., impotence, weight gain, ankle edema). It is helpful to point out key symptoms for which the patient should report promptly to the practice (e.g., cough, muscle pain, tarry stools, etc.);
- Anticipate that the patient may change the therapy on their own. Give advice on which medicines should not be discontinued, paused, or changed in dosage;
- Enquire about the patient’s own activities (as an expression of participation in the therapy), such as alternative, anthroposophical, and homoeopathic therapy. Explain that this information is necessary for the treating doctor, as drugs may be discontinued or others taken in addition.
2.6. Monitoring and Follow-Up (Step 7)
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Ia:
- Systematic review +/− meta-analyses of several randomized controlled trials (RCT)
- IIa:
- Systematic review +/− meta-analyses of multiple cohort studies
- IV:
- Observational studies—also systematic reviews of these studies
- V:
- Expert consensus
- 0-1
- Patients with multiple medications (≥5 medications used continuously) and multimorbidity (≥3 chronic diseases) should undergo a medication review at least once a year. (B, V)
- 0-2
- Patients with multimedication and multimorbidity with additional risks or events (e.g., falls, hospitalization) should have an ad hoc medication review (with inventory and assessment of medication). (B, V)
- 0-3
- You should define for your practice (e.g., in your quality management system) how to identify patients with these criteria (see recommendations 0-1 and 0-2) for a medication review and where you document when the next medication review should take place at the latest. (B, V)
- 1-1
- The following information should be available and collected for the medication review (B, V):
- Pre-existing conditions and current medical conditions (including severity, impairment of quality of life, functionality);
- Clinical status and current relevant laboratory values;
- Prescriptions or self-medication, e.g., using the brown bag method;
- Information on lifestyle factors (diet, smoking, alcohol, etc.);
- Psychosocial context;
- Therapy goals of the patient.
- 1-2
- Relatives and professional groups involved in the therapy should be included in the assessment if the patient has agreed. (B, V)
- 1-3
- The patient’s treatment burden should be assessed with a screening question (if necessary, with the inclusion of caring relatives). (B, IIIa)
- 1-4
- If the patient confirms a treatment burden, more targeted questions should be used with patients, and, if necessary, with caring relatives. (A, IIa)
- 1-5
- If in consultation with the patient, and, if applicable, the patient’s relatives and caregivers, there is a desire to reduce the burden of therapy, suitable options should be explored and implemented (A, IV), with particular consideration of the following:
- Number of drugs and complexity of the medication regime;
- Effort and extent of the necessary therapy controls (laboratory tests, control appointments with doctors, self-controls);
- Effort and extent of other types of self-management;
- Coordination of doctor visits and follow-up prescriptions.
- 1-6
- Medication should be assessed in a structured way (A, V), e.g., by means of an instrument such as the Medication Appropriateness Index, with particular reference to the following:
- PIM lists/anticholinergic loads, QTc-time-prolonging drugs;
- Underuse;
- Adherence.
- 2-1
- Patients should be asked about their preferred therapy goals. The aim is to identify their personal priorities with regard to the following aspects (A, IIa):
- Improvement or maintenance of quality of life;
- Independent living/independence;
- Improvement or preservation of functional capacity;
- Survival/prognosis improvement;
- Pain relief;
- Further symptom improvement (nausea, shortness of breath, dizziness, etc.);
- Importance of the burden of therapy.
- 3-1
- The primary goal of drug therapy should be to use as few drugs as possible, and only as many as necessary. Underuse and overuse must be prevented. (B, Ib)
- 3-2
- Non-pharmacological measures should be considered, taking into account the patient’s therapeutic goals and the burden of therapy. (B, V)
- 3-3
- The medication regime should be kept as simple as possible to avoid burden and errors. (B, Ia)
- 3-4
- The prescribing doctor should explain the therapy and, also, ask whether the patient knows the indication of each drug and how it should be used. (A, V)
- 3-5
- At every medication review, it should be clarified whether medication is missing, can be discontinued, or whether the dose has to be adjusted. (A, V)
- 3-6
- When selecting a drug for long-term therapy, an individual risk/benefit assessment should be made. (A, V)
- 3-7
- The initiation and discontinuation of each medication should be planned and carried out as a structured process with the involvement of the patient. (A, Ia)
- 3-8
- If discontinuation of a medication is being considered, the patient should be made to understand the reasons for discontinuation, especially in the case of a medication that has been prescribed for many years. (A, Ia)
- 3-9
- When discontinuing a medication, attention should be paid to discontinuation symptoms. (A, Ia)
- 3-10
- The patient should be actively asked about their experiences and concerns regarding their medication. (B, Ia)
- 3-11
- Documentation should be made in the patient’s record and on the medication plan in case of confirmed or probable incompatibilities or interactions leading to discontinuation of medication. (A, V)
- 3-12
- The medication plan should always be complete and up to date; the national medication plan (BMP) is the preferred format. Coordination lies with the general practitioner/primary care physician. The medication plan is to be presented at every consultation and at the pharmacy. (A, V)
- 4-1
- GPs should agree on a communication channel with pharmacists to address issues with dispensing medications. (A, Ia)
- 4-2
- GPs should recommend that patients taking multiple medications select a regular pharmacy that provides personalized advice on medication use, documents all medication, checks interactions, and supports the doctor and patient in keeping track of the patient’s medication. (A, Ia)
- 4-3
- The patient should be made aware that it may be beneficial for them to contact the regular pharmacy for all prescriptions, OTC needs, and questions or problems regarding the use of medicines. (A, Ia)
- 5-1
- The coordinating doctor should ensure that every patient with multiple medication has an up-to-date medication plan. (B, V)
- 5-2
- In the patient’s medication plan, there should be a note in plain language for each medicine stating the condition(s) for which it is used. (A, V)
- 5-3
- The patient should be informed about and motivated to self-monitor and support the use of medicines. (A, Ia)
- 5-4
- The patient should be instructed on what to do if certain symptoms or self-measured values occur, especially after stopping medication. (B, V)
- 5-5
- The patient should be offered explanations and help on the use of medicines (e.g., weekly dosettes). They should be asked about their ideas. (B, V)
- 6-1
- Each practice should draw up an individual schedule for patients with multimedication, as to when and which laboratory parameters are checked. (B, V)
- 6-2
- Whenever the therapy is changed, the relevance of the medication schedule should be checked, and an appointment should be made with the patient to check the treatment results. (B, V)
- 6-3
- Treatment results, clinical parameters, and any side effects (including observed non-specific symptoms), as well as the timeliness of the medication plan, should be checked at follow-up appointments. (B, V)
- 6-4
- Problems with the management of the therapy and need for support should be addressed at the follow-up appointment. (B, V)
References
- Cascorbi, I. Drug interactions—Principles, examples and clinical consequences. Dtsch. Arztebl. Int. 2012, 109, 546–555. [Google Scholar] [PubMed]
- National Institute for Health and Clinical Excellence (NICE). Medicines Adherence. Involving Patients in Decisions about Prescribed Medicines and Supporting Adherence. [Clinical Guideline]. 2009. Available online: Nice.org.uk/guidance/cg76 (accessed on 22 February 2022).
- Beardon, P.H.; McGilchrist, M.M.; McKendrick, A.D.; McDevitt, D.G.; MacDonald, T.M. Primary non-compliance with prescribed medication in primary care. BMJ 1993, 307, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuijpers, M.A.; van Marum, R.J.; Egberts, A.C.; Jansen, P.A. Relationship between polypharmacy and underprescribing. Br. J. Clin. Pharmacol. 2008, 65, 130–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandt, D.; Lappe, V.; Schubert, I. Arzneimittelreport 2018; Barmer: Berlin, Germany, 2018. [Google Scholar]
- Thürmann, P.A.; Holt-Noreiks, S.; Nink, K.; Zawinell, A. Arzneimittelversorgung älterer Patienten. In Versorgungsreport; Günter, C., Klose, J., Schmacke, N., Eds.; Schattauer GmbH: Stuttgart, Germany, 2012; pp. 111–130. [Google Scholar]
- Nguyen, T.N.; Ngangue, P.; Haggerty, J.; Bouhali, T.; Fortin, M. Multimorbidity, polypharmacy and primary prevention in community-dwelling adults in Quebec: A cross-sectional study. Fam. Pract. 2019, 36, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Bergert, F.W.; Braun, M.; Ehrenthal, K.; Fessler, J.; Gross, J.; Hüttner, U.; Kluthe, B.; Liesenfeld, A.; Seffrin, J.; Vetter, G.; et al. Recommendations for treating adult and geriatric patients on multimedication. Int. J. Clin. Pharmacol. Ther. 2014, 52, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Dinh, T.S.; Brueckle, M.-S.; González-González, A.I.; Fessler, J.; Marschall, U.; Schubert-Zsilavesz, M.; Gerlach, F.M.; Harder, S.; van den Akker, M.; Schubert, I.; et al. Evidence-Based Decision Support for a Structured Care Program on Polypharmacy in Multimorbidity: A Guideline Upgrade Based on a Realist Synthesis. J. Pers. Med. 2022, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Muth, C.; Blom, J.W.; Smith, S.M.; Johnell, K.; Gonzalez-Gonzalez, A.I.; Nguyen, T.S.; Brueckle, M.-S.; Cesari, M.; Tinetti, M.E.; Valderas, J.M. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. J. Intern. Med. 2019, 285, 272–288. [Google Scholar] [CrossRef] [Green Version]
- Muth, C.; van den Akker, M.; Blom, J.W.; Mallen, C.D.; Rochon, J.; Schellevis, F.G.; Becker, A.; Beyer, M.; Gensichen, J.; Kirchner, H.; et al. The Ariadne principles: How to handle multimorbidity in primary care consultations. BMC Med. 2014, 12, 223. [Google Scholar] [CrossRef]
- Prados-Torres, A.; del Cura-González, I.; Prados-Torres, J.D.; Muth, C.; Leiva-Fernández, F.; Lopez-Rodriguez, J.A.; González-Rubio, F. MULTIPAP Study: Improving healthcare for patients with multimorbidity. Br. J. Gen. Pract. 2020, 70 (Suppl. 1). [Google Scholar] [CrossRef]
- Leitliniengruppe Hessen, DEGAM. S3-Leitlinie Multimedikation (AWMF-Reg-Nr. 053–04). 2021. Available online: https://www.awmf.org/uploads/tx_szleitlinien/053-043l_S3_Multimedikation_2021-08.pdf (accessed on 5 May 2022).
- Lappe, V.; Dinh, T.S.; Harder, S.; Brueckle, M.S.; Fessler, J.; Marschall, U.; Muth, C.; Schubert, I.; EVITA Study Group. Polypharmacy guideline: Estimating the percentage of patients eligible for medication review and assessment of their potential drug safety problems with routine data. Pharmacoepidemiology 2022, 1, 12–25. [Google Scholar] [CrossRef]
- Lindblad, C.I.; Hanlon, J.T.; Gross, C.R.; Sloane, R.J.; Pieper, C.F.; Hajjar, E.R.; Ruby, C.M.; Schmader, K.E.; Panel, M.C. Clinically important drug-disease interactions and their prevalence in older adults. Clin. Ther. 2006, 28, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.-T.; Harrington, M.; Montori, V.M.; Barnes, C.; Wicks, P.; Ravaud, P. Adaptation and validation of the Treatment Burden Questionnaire (TBQ) in English using an internet platform. BMC Med. 2014, 12, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pazan, F.; Kather, J.; Wehling, M. A systematic review and novel classification of listing tools to improve medication in older people. Eur. J. Clin. Pharmacol. 2019, 75, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.; Schmiedl, S.; Thürmann, P.A. Potentially Inappropriate Medications in the Elderly. Dtsch. Arztebl. Int. 2010, 107, 543–551. [Google Scholar] [CrossRef]
- Kuhn-Thiel, A.M.; Weiss, C.; Wehling, M. Consensus validation of the FORTA (Fit fOR The Aged) List: A clinical tool for increasing the appropriateness of pharmacotherapy in the elderly. Drugs Aging 2014, 31, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, J.T.; Schmader, K.E.; Samsa, G.P.; Weinberger, M.; Uttech, K.M.; Lewis, I.K.; Cohen, H.J.; Feussner, J.R. A method for assessing drug therapy appropriateness. J. Clin. Epidemiol. 1992, 45, 1045–1051. [Google Scholar] [CrossRef]
- Hanlon, J.T.; Schmader, K.E. The Medication Appropriateness Index: A Clinimetric Measure. Psychother. Psychosom. 2022, 91, 78–83. [Google Scholar] [CrossRef]
- Meid, A.D.; Quinzler, R.; Groll, A.; Wild, B.; Saum, K.U.; Schöttker, B.; Heider, D.; König, H.-H.; Brenner, H.H.; Haefeli, W.E. Longitudinal evaluation of medication underuse in older outpatients and its association with quality of life. Eur. J. Clin. Pharmacol. 2016, 72, 877–885. [Google Scholar] [CrossRef]
- Bertsche, T.; Fleischer, M.; Pfaff, J.; Encke, J.; Czock, D.; Haefeli, W.E. Pro-active provision of drug information as a technique to address overdosing in intensive-care patients with renal insufficiency. Eur. J. Clin. Pharmacol. 2009, 65, 823–829. [Google Scholar] [CrossRef] [Green Version]
- Erler, A.; Beyer, M.; Petersen, J.J.; Saal, K.; Rath, T.; Rochon, J.; Haefeli, W.E.; Gerlach, F.M. How to improve drug dosing for patients with renal impairment in primary care—A cluster-randomized controlled trial. BMC Fam. Pract. 2012, 13, 91. [Google Scholar] [CrossRef] [Green Version]
- Jonville-Béra, A.P.; Paroux, L.; Autret-Leca, E. Assessing general practitioners’ prescribing behaviour in elderly patients with concealed renal failure. Br. J. Clin. Pharmacol. 2008, 65, 961–963. [Google Scholar] [CrossRef] [Green Version]
- Nishtala, P.S.; Salahudeen, M.S.; Hilmer, S.N. Anticholinergics: Theoretical and clinical overview. Expert Opin. Drug Saf. 2016, 15, 753–768. [Google Scholar] [CrossRef]
- Wouters, H.; Hilmer, S.N.; Gnjidic, D.; Van Campen, J.P.; Teichert, M.; van der Meer, H.G.; Schaap, L.A.; Huisman, M.; Comijs, H.C.; Denig, P.; et al. Long-Term Exposure to Anticholinergic and Sedative Medications and Cognitive and Physical Function in Later Life. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 75, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Dinh, T.S.; González-González, A.I.; Meid, A.D.; Snell, K.I.; Rudolf, H.; Brueckle, M.S.; Blom, J.W.; Thiem, U.; Trampisch, H.-J.; Elders, P.J.M.; et al. Are Anticholinergic Symptoms a Risk Factor for Falls in Older General Practice Patients With Polypharmacy? Study Protocol for the Development and Validation of a Prognostic Model. Front. Pharmacol. 2021, 11, 577747. [Google Scholar] [CrossRef]
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and Fall-Related Injuries among Community-Dwelling Adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef] [Green Version]
- Drug and Therapeutic Bulletin: QT interval and drug therapy. BMJ 2016, 353, i2732.
- Arizona Center for Education and Research on Therapeutics (AZCERT). Drugs that Prolong QT & Induce Torsades de Pointes (TdP): CredibleMeds® Resources. 2018. Available online: https://crediblemeds.org/healthcare-providers/ (accessed on 5 May 2022).
- de Vries, M.; Seppala, L.J.; Daams, J.G.; van de Glind, E.M.; Masud, T.; van der Velde, N. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: I. Cardiovascular Drugs. J. Am. Med. Dir. Assoc. 2018, 19, 371.E1–371.E9. [Google Scholar] [CrossRef] [Green Version]
- Seppala, L.J.; Wermelink, A.M.; de Vries, M.; Ploegmakers, K.J.; van de Glind, E.M.; Daams, J.; van der Velde, N.; Blain, H.; Bousquet, J.; Bucht, G.; et al. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: II. Psychotropics. J. Am. Med. Dir. Assoc. 2018, 19, 371.E11–371.E17. [Google Scholar] [CrossRef] [Green Version]
- Seppala, L.J.; van de Glind, E.M.M.; Daams, J.G.; Ploegmakers, K.J.; de Vries, M.; Wermelink, A.M.; van der Velde, N.; Blain, H.; Bousquet, J.; Bucht, G.; et al. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-analysis: III. Others. J. Am. Med. Dir. Assoc. 2018, 19, 372.E1–372.E8. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health Care Excellence (NICE). Medicines Optimisation: The Safe and Effective Use of Medicines to Enable the Best Possible Outcomes. 2015. Available online: https://www.nice.org.uk/guidance/ng5/evidence/full-guideline-pdf-6775454 (accessed on 22 February 2022).
- Woodward, M.C. Deprescribing: Achieving Better Health Outcomes for Older People through Reducing Medications. J. Pharm. Pract. Res. 2003, 33, 323–328. [Google Scholar] [CrossRef]
- Reeve, E.; Shakib, S.; Hendrix, I.; Roberts, M.S.; Wiese, M.D. Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. Br. J. Clin. Pharmacol. 2014, 78, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Seidling, H.M.; Send AF, J.; Bittmann, J.; Renner, K.; Dewald, B.; Lange, D.; Bruckner, T.; Haefeli, W.E. Medication review in German community pharmacies—Post-hoc analysis of documented drug-related problems and subsequent interventions in the ATHINA-project. Res. Soc. Adm. Pharm. RSAP 2017, 13, 1127–1134. [Google Scholar] [CrossRef]
- Köberlein-Neu, J.; Mennemann, H.; Hamacher, S.; Waltering, I.; Jaehde, U.; Schaffert, C.; Rose, O. Interprofessional Medication Management in Patients with Multiple Morbidities. Dtsch. Arztebl. Int. 2016, 113, 741–748. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Assessment Dimension | Key Questions | MAI Item No. |
|---|---|---|
| Is there an indication for the drug? | 1 |
| Is the drug effective for the indication and the patient group? | 2 | |
| Is the duration of drug therapy adequate? (Since when was it prescribed? *) | 9 | |
| Is the dosage correct? Is there any relevant restriction of kidney or liver function? | 3 |
| Are there clinically relevant interactions with other medicines? | 6 | |
| Are there clinically relevant interactions with other diseases/conditions? Is there any previous cardiac damage with regard to QT syndrome? Are there age restrictions (PIM, FRID, ACh)? | 7 | |
| Is there an up-to-date and written intake plan? Are the intake instructions correct? (Mode of administration, frequency of administration, time of administration, relation to meals). | 4 |
| Are handling and application instructions practicable? | 5 | |
| Are there duplicate prescriptions? | 8 | |
| Is adherence to the therapy given? | - | |
| Is every indication requiring treatment treated? | - |
| Has the most cost-effective alternative of comparable preparations been selected | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schubert, I.; Fessler, J.; Harder, S.; Dinh, T.S.; Brueckle, M.-S.; Muth, C.; on behalf of the EVITA Study Group. Multimedication in Family Doctor Practices: The German Evidence-Based Guidelines on Multimedication. Pharmacoepidemiology 2022, 1, 35-48. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010005
Schubert I, Fessler J, Harder S, Dinh TS, Brueckle M-S, Muth C, on behalf of the EVITA Study Group. Multimedication in Family Doctor Practices: The German Evidence-Based Guidelines on Multimedication. Pharmacoepidemiology. 2022; 1(1):35-48. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010005
Chicago/Turabian StyleSchubert, Ingrid, Joachim Fessler, Sebastian Harder, Truc Sophia Dinh, Maria-Sophie Brueckle, Christiane Muth, and on behalf of the EVITA Study Group. 2022. "Multimedication in Family Doctor Practices: The German Evidence-Based Guidelines on Multimedication" Pharmacoepidemiology 1, no. 1: 35-48. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma1010005