
Treatment Patterns, Effectiveness, and Safety of Originator Insulin Glargine versus Insulin Glargine-yfgn within the Veterans Health Administration

Abstract
:1. Introduction
2. Results
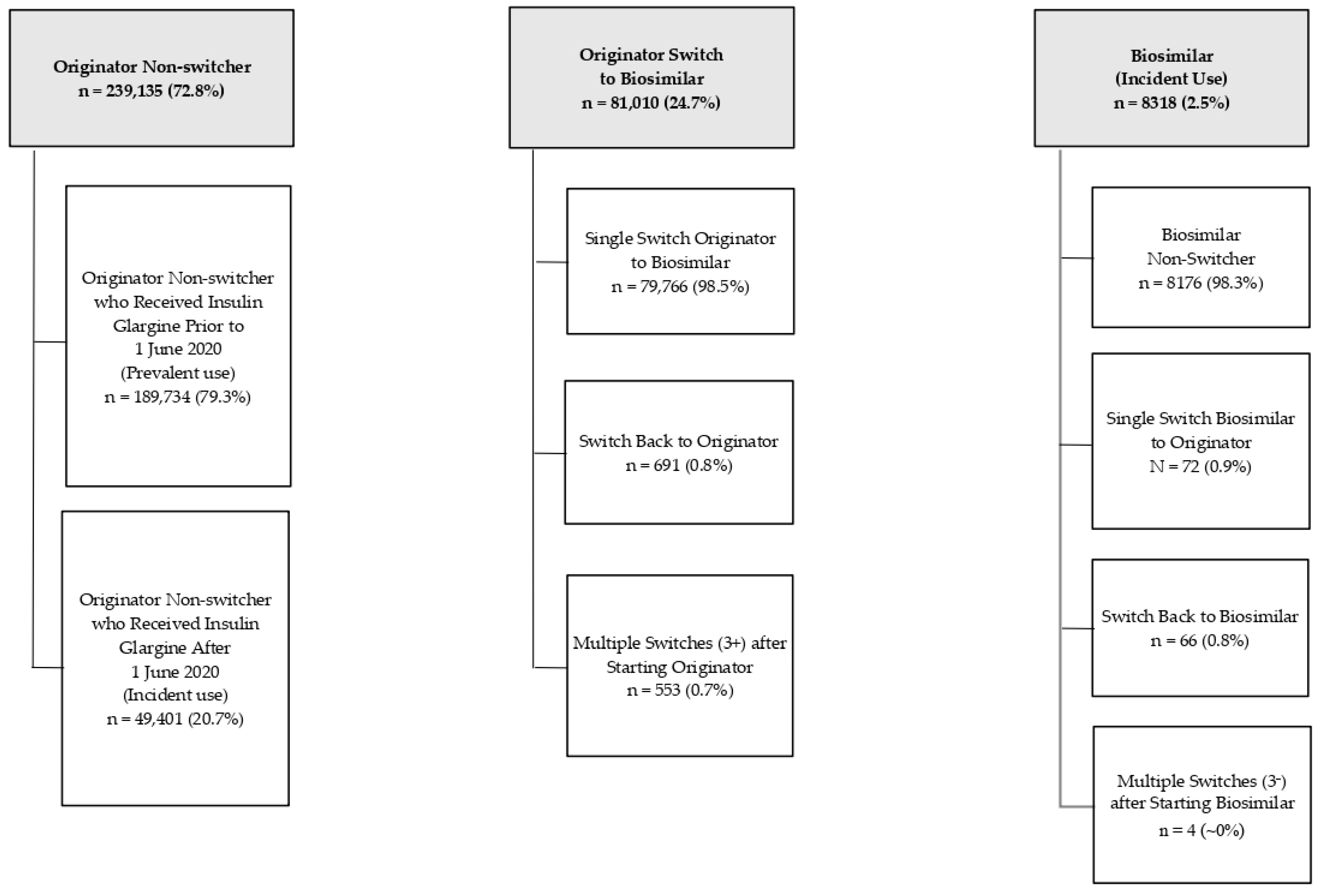
2.1. Patient Cohort
2.2. Prescribing Patterns
2.3. Baseline Patient Characteristics
2.4. Effectiveness Outcomes
2.5. Safety Outcomes
2.6. Adjusted Regression Analyses
2.7. Switching Back to Originator Insulin Glargine
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design and Participants
5.2. Data Sources and Data Collection
5.3. Creation of Subgroups
5.4. Outcomes
5.4.1. Prescribing Patterns
5.4.2. Effectiveness and Safety
5.4.3. Reasons for Switching Back to Originator from Biosimilar
5.5. Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amgen 2022 Biosimilar Trends Report. Available online: https://www.amgenbiosimilars.com/commitment/-/media/Themes/Amgen/amgenbiosimilars-com/Amgenbiosimilars-com/pdf/USACBU81422-2022-Amgen-Biosimilars-Trend-Report-Oct-2022.pdf?#page=4 (accessed on 18 May 2023).
- US Food & Drug Administration. Biosimilar and Interchangeable Biologics: More Treatment Choices. Available online: https://www.fda.gov/consumers/consumer-updates/biosimilar-and-interchangeable-biologics-more-treatment-choices (accessed on 18 May 2023).
- Triplitt, C.; Hinnen, D.; Valentine, V. How similar are biosimilars? What do clinicians need to know about biosimilar and follow-on insulins? Clin. Diabetes 2017, 35, 209–216. [Google Scholar] [CrossRef]
- Cunningham, A.M.; Freeman, A.M. Glargine Insulin; StatPearls: Treasure Island, FL, USA, 2022. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK557756/ (accessed on 18 May 2023).
- Blevins, T.C.; Barve, A.; Sun, B.; Ankersen, M. Efficacy and safety of MYL-1501D vs insulin glargine in patients with type 1 diabetes after 52 weeks: Results of the INSTRIDE 1 phase III study. Diabetes Obes. Metab. 2018, 20, 1944–1950. [Google Scholar] [CrossRef]
- Blevins, T.C.; Barve, A.; Sun, B.; Raiter, Y.; Aubonnet, P.; Muniz, R.; Athalye, S.; Ankersen, M. Efficacy and safety of MYL-1501D versus insulin glargine in patients with type 2 diabetes after 24 weeks: Results of the phase III INSTRIDE 2 study. Diabetes Obes. Metab. 2019, 21, 129–135. [Google Scholar] [CrossRef]
- Blevins, T.C.; Barve, A.; Raiter, Y.; Aubonnet, P.; Athalye, S.; Sun, B.; Muniz, R. Efficacy and safety of MYL-1501D versus insulin glargine in people with type 1 diabetes mellitus: Results of the INSTRIDE 3 phase 3 switch study. Diabetes Obes. Metab. 2020, 22, 365–372. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 13. Older Adults: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47, S244–S257. [Google Scholar] [CrossRef] [PubMed]
- Vaidyanathan, J.; Wang, Y.C.; Tran, D.; Seo, S.K. Leveraging Clinical Pharmacology Data to Assess Biosimilarity and Interchangeability of Insulin Products. Clin. Pharmacol. Ther. 2023, 113, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.; Kim, J.D.; Dormuth, C. The impact of mandatory nonmedical switching from originator to biosimilar insulin glargine. Clin. Ther. 2022, 4, 957–970. [Google Scholar] [CrossRef] [PubMed]
- Pitlick, J.M.; Bryant, G.A.; Daly, M.W.; Koenigsfeld, C.F.; Lehman, N.; Brueggen, K.; McCormick, A.; Wellington, K. Real-World Evaluation of Dosing in Patients Converted from Insulin Glargine (Lantus) to Insulin Glargine (Basaglar). Ann. Pharmacother. 2020, 54, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Taki, K.; Koyanagi, M.; Nagaoka, S.; Shingaki, T. Treatment satisfaction, safety, and effectiveness of biosimilar insulin glargine is comparable in patients with type 2 diabetes mellitus after switching from insulin glargine or insulin degludec: A post-marketing safety study. Curr. Med. Res. Opin. 2020, 36, 1975–1983. [Google Scholar] [CrossRef]
- Shingaki, T.; Taki, K.; Koyanagi, M.; Nagaoka, S.; Yoshizawa, K.; Oki, N.; Yoshikawa, A.; Imaoka, T. Long-term safety and effectiveness of biosimilar insulin glargine in Japanese patients with diabetes mellitus in routine clinical practice: Results of a post-marketing safety study. Curr. Med. Res. Opin. 2020, 36, 947–958. [Google Scholar] [CrossRef] [PubMed]
- Eli Lilly and Company. Rezvoglar (Insulin Glargine-Aglr) Injection [Package Insert]. Available online: https://pi.lilly.com/us/rezvoglar-uspi.pdf (accessed on 20 December 2023).
- Dugan, J.; Shubrook, J. International Classification of Diseases, 10th Revision, Coding for Diabetes. Clin. Diabetes 2017, 35, 232–238. [Google Scholar] [CrossRef]
- Lipscombe, L.L.; Austin, P.C.; Alessi-Severini, S.; Blackburn, D.F.; Blais, L.; Bresee, L.; Filion, K.B.; Kawasumi, Y.; Kurdyak, P.; Platt, R.W.; et al. Atypical antipsychotics and hyperglycemic emergencies: Multicentre, retrospective cohort study of administrative data. Schizophr. Res. 2014, 154, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.H.; Ziemba, R.; Shehab, N.; Geller, A.I.; Talreja, K.; Campbell, K.N.; Budnitz, D.S. Assessment of International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code assignment validity for case finding of medication-related hypoglycemia acute care visits among Medicare beneficiaries. Med. Care. 2022, 60, 219–226. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Eyth, E.; Naik, R. Hemoglobin A1C; StatPearls: Treasure Island, FL, USA, 2023. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK549816/ (accessed on 18 May 2023).
- Mamdani, M.; Sykora, K.; Li, P.; Normand, S.L.; Streiner, D.L.; Austin, P.C.; Rochon, P.A.; Anderson, G.M. Reader’s guide to critical appraisal of cohort studies, 2: Assessing potential for confounding. BMJ 2005, 330, 960–962. [Google Scholar] [CrossRef]
- StataCorp. Multiple Imputation Reference Manual Release 13. Available online: https://www.stata.com/manuals13/mi.pdf (accessed on 20 December 2023).



{kind=link}
{kind=link}
| Characteristic (Total N = 328,463) | Prevalent Originator Non-Switcher 1 N = 189,734 (57.8%) n (%) | Originator Switch to Biosimilar 2 N = 81,010 (24.7%) n (%) | Standardized Difference 3 | Incident Originator Non-Switcher 4 N = 49,401 (15.0%) n (%) | Incident Biosimilar 5 N = 8318 (2.5%) n (%) | Standardized Difference 3 |
|---|---|---|---|---|---|---|
| Age (years), mean (SD) | 69.4 (10.8) | 69.2 (10.9) | −0.0195 | 66.2 (12.5) | 66.5 (12.5) | 0.0265 |
| 18–64 | 54,463 (28.7) | 24,490 (30.2) | 0.0335 | 20,361 (41.2) | 3432 (41.3) | 0.0009 |
| 65–74 | 83,178 (43.8) | 30,891 (38.1) | −0.1162 | 17,219 (34.9) | 2699 (32.4) | −0.051 |
| 75+ | 52,093 (27.5) | 25,629 (31.6) | 0.0917 | 11,821 (23.9) | 2187 (26.3) | 0.0545 |
| Sex, male | 180,933 (95.4) | 76,047 (94.6) | −0.0383 | 44,574 (93.9) | 7464 (92.5) | −0.0529 |
| Race/Ethnicity | ||||||
| Non-Hispanic White | 140,572 (74.3) | 56,789 (70.4) | −0.089 | 33,326 (68.1) | 5438 (66.0) | −0.0441 |
| Non-Hispanic Black | 36,263 (19.2) | 17,874 (22.2) | 0.073 | 11,191 (22.9) | 2051 (24.9) | 0.0472 |
| Hispanic | 4227 (2.2) | 2919 (3.6) | 0.0818 | 1580 (3.2) | 383 (4.6) | 0.0727 |
| Other | 2106 (1.1) | 752 (0.9) | −0.0181 | 467 (1.0) | 85 (1.0) | 0.0078 |
| Asian | 1779 (0.9) | 567 (0.7) | −0.0264 | 672 (1.4) | 68 (0.8) | −0.0523 |
| American Indian | 1276 (0.7) | 478 (0.6) | −0.0104 | 421 (0.9) | 45 (0.5) | −0.0374 |
| Unknown | 2972 (1.6) | 1302 (1.6) | 0.0118 | 1276 (2.6) | 174 (2.1) | −0.0309 |
| Marital Status | ||||||
| Married | 112,998 (59.8) | 49,491 (61.3) | 0.0314 | 27,208 (55.6) | 4852 (58.7) | 0.0657 |
| Divorced, separated, or widowed | 59,161 (31.3) | 24,317 (30.1) | −0.0253 | 16,176 (33.0) | 2563 (31.0) | −0.0415 |
| Never married | 16,750 (8.9) | 6866 (8.5) | −0.0125 | 5570 (11.4) | 855 (10.3) | −0.0321 |
| Smoking Status | ||||||
| Current smoker | 32,735 (18.0) | 13,689 (17.2) | −0.0094 | 9705 (20.7) | 1617 (20.1) | −0.0052 |
| Former smoker | 84,757 (46.5) | 34,845 (43.9) | −0.0334 | 19,519 (41.7) | 3255 (40.5) | −0.0078 |
| Never smoker | 64,615 (35.5) | 30,888 (38.9) | 0.0849 | 17,551 (37.5) | 3173 (39.4) | 0.0543 |
| Charlson Comorbidity Index (adapted), 6 mean (SD) | 3.1 (2.0) | 3.1 (2.0) | 0.02 | 2.9 (2.1) | 3.0 (2.1) | 0.0366 |
| Other Comorbidities 6 | ||||||
| Neuropathy | 64,911 (34.2) | 29,577 (36.5) | 0.0481 | 12,918 (26.1) | 2365 (28.4) | 0.0513 |
| Ischemic stroke | 5228 (2.8) | 2169 (2.7) | −0.0048 | 1021 (2.1) | 203 (2.4) | 0.0252 |
| Hypertension | 152,059 (80.1) | 66,170 (81.7) | 0.0391 | 36,151 (73.2) | 6227 (74.9) | 0.0384 |
| Retinopathy | 34,030 (17.9) | 16,412 (20.3) | 0.0591 | 6455 (13.1) | 1178 (14.2) | 0.0319 |
| Nephropathy | 51,285 (27.0) | 22,634 (27.9) | 0.0204 | 10,449 (21.2) | 1965 (23.6) | 0.0593 |
| Concomitant Therapies at Index Prescription 7 | ||||||
| Any non-insulin glargine medication for diabetes | 147,702 (77.8) | 65,850 (81.3) | 0.0854 | 37,663 (76.2) | 6396 (76.9) | 0.0154 |
| Metformin | 74,995 (39.5) | 33,264 (41.1) | 0.0313 | 20,300 (41.1) | 3443 (41.4) | 0.0061 |
| Insulin, fast-acting | 64,463 (34.0) | 26,955 (33.3) | −0.0149 | 15,389 (31.2) | 2627 (31.6) | 0.0093 |
| Sulfonylurea | 25,749 (13.6) | 9530 (11.8) | −0.0544 | 9281 (18.8) | 1565 (18.8) | 0.0007 |
| Glucagon-like peptide-1 (GLP-1) receptor agonist | 26,418 (13.9) | 15,000 (18.5) | 0.1248 | 4953 (10.0) | 798 (9.6) | −0.0145 |
| Thiazolidinedione | 5544 (2.9) | 2376 (2.9) | 0.0007 | 1623 (3.3) | 319 (3.8) | 0.0297 |
| Meglitinide | 202 (0.1) | 88 (0.1) | 0.0007 | 37 (0.1) | 6 (0.1) 8 | −0.001 |
| Sodium-glucose cotransporter 2 (SGLT2) inhibitor | 28,750 (15.2) | 21,934 (27.1) | 0.2953 | 8720 (17.7) | 1982 (23.8) | 0.1528 |
| Dipeptidyl peptidase 4 (DPP-4) inhibitor | 17,833 (9.4) | 7165 (8.8) | −0.0193 | 5369 (10.9) | 925 (11.1) | 0.0081 |
| Alpha-glucosidase inhibitor | 523 (0.3) | 173 (0.2) | −0.0126 | 140 (0.3) | 23 (0.3) | −0.0013 |
| Number of Concomitant Antidiabetic Medications, mean (SD) | 1.3 (1.0) | 1.4 (1.0) | 0.1515 | 1.3 (1.0) | 1.3 (1.0) | 0.0358 |
| Glucose Monitoring Sensor, at index date | 10,113 (5.3) | 8870 (10.9) | 0.2066 | 2888 (5.8) | 633 (7.6) | 0.0705 |
| Baseline HbA1c (%), 9 mean (SD) | 8.6 (3.0) | 8.0 (1.8) | −0.2389 | 9.4 (2.6) | 9.3 (2.5) | −0.0463 |
| Baseline HbA1c < 7% 9 | 38,487 (21.5) | 20,657 (26.0) | 0.1055 | 7035 (15.3) | 1328 (16.4) | 0.031 |
| VHA Hospitalizations and/or ER Visits 6 | ||||||
| Hypoglycemia | 104 (0.1) | 54 (0.1) | 0.0048 | 29 (0.1) | 4 (0.0) 8 | −0.0046 |
| Hyperglycemia | 4493 (2.4) | 2064 (2.5) | 0.0116 | 2981 (6.0) | 520 (6.3) | 0.009 |
| Outcomes of Interest 1,2 N = 177,122 (53.9% of Full Sample) | Prevalent Originator Non-Switcher N = 136,755 (77.2%) | Originator Switch to Biosimilar N = 14,538 (8.2%) | p Value: Originator Switch to Biosimilar vs. Prevalent Originator | Incident Originator Non-Switcher N = 23,966 (13.5%) | Incident Biosimilar N = 1863 (1.1%) | p Value: Incident Biosimilar vs. Incident Originator |
|---|---|---|---|---|---|---|
| Number of Patient-days Followed for Outcomes, mean (SD) | 348.9 (42.6) | 251.4 (60.7) | 294.0 (78.6) | 239.1 (70.2) | ||
| Most Recent HbA1c (%), mean (SD) | 7.9 (1.6) | 7.9 (1.5) | <0.0001 | 7.9 (1.7) | 7.9 (1.6) | 0.98 |
| Most Recent HbA1c < 7%, n (%) | 36,332 (26.6) | 4000 (27.5) | 0.01 | 7485 (31.2) | 535 (28.7) | 0.02 |
| Arithmetic Mean HbA1c (%), mean (SD) 3 | 8.0 (1.5) | 7.9 (1.5) | <0.0001 | 8.0 (1.7) | 7.9 (1.6) | 0.27 |
| Outcomes of Interest 1,2 (N = 328,463) | Prevalent Originator Non-Switcher N = 189,734 (57.8%) | Originator Switch to Biosimilar N = 81,010 (24.7%) | p Value: Originator Switch to Biosimilar vs. Prevalent Originator | Incident Originator Non-Switcher N = 49,401 (15.0%) | Incident Biosimilar N = 8318 (2.5%) | p Value: Incident Biosimilar vs. Incident Originator |
|---|---|---|---|---|---|---|
| Number of Patient-days Followed for Outcomes, mean (SD) | 316.8 (91.9) | 95.3 (96.0) | 210.8 (118.0) | 109.1 (95.4) | ||
| Hospitalizations/ER Visits for Hyperglycemia, n (rate per 100 patient-years) | 3552 (2.2) | 522 (2.5) | 0.09 | 1357 (4.8) | 151 (6.1) | 0.054 |
| Hospitalizations/ER Visits for Hypoglycemia, n (rate per 100 patient-years) | 99 (0.06) | 10 (0.5) 3 | 0.38 | 24 (0.08) | 3 (0.1) 3 | 0.61 |
| Outcomes of Interest (N = 177,122 for Effectiveness Outcomes; N = 328,463 for Safety Outcomes) | Originator Switch to Biosimilar vs. Prevalent Originator Non-Switcher | Incident Biosimilar vs. Incident Originator Non-Switcher |
|---|---|---|
| Mean difference (95% CI) | Mean difference (95% CI) | |
| Most Recent HbA1c (%) | 0.007 (−0.017, 0.031), p = 0.56 | 0.014 (−0.061, 0.089), p = 0.71 |
| Mean HbA1c (%) | −0.011 (−0.034, 0.012), p = 0.36 | −0.030 (−0.104, 0.044), p = 0.42 |
| Risk difference (95% CI) | Risk difference (95% CI) | |
| Most Recent HbA1c < 7% | 0.39 (−0.31, 1.09), p = 0.27 | −2.20 (−4.50, 0.10), p = 0.06 |
| Incident rate difference (95% CI) | Incident rate difference (95% CI) | |
| Number of Hospitalizations/ER Visits for Hyperglycemia | 0.14 (−0.03, 0.32), p = 0.11 | 0.67 (−0.10, 1.45), p = 0.09 |
| Reason | N (%) |
| Administrative Switch | 85 (61.2) |
| Incorrect—No Switch Back | 42 (30.2) |
| Other (i.e., adverse drug event, decreased effectiveness, preference, unknown) | 12 (8.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walczuk, S.; Cunningham, F.E.; Zhao, X.; Dong, D.; Glassman, P.A.; Miller, D.R.; Khachikian, D.; Au, A.; Salone, C.; Bryan, K.; et al. Treatment Patterns, Effectiveness, and Safety of Originator Insulin Glargine versus Insulin Glargine-yfgn within the Veterans Health Administration. Pharmacoepidemiology 2024, 3, 103-116. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma3010008
Walczuk S, Cunningham FE, Zhao X, Dong D, Glassman PA, Miller DR, Khachikian D, Au A, Salone C, Bryan K, et al. Treatment Patterns, Effectiveness, and Safety of Originator Insulin Glargine versus Insulin Glargine-yfgn within the Veterans Health Administration. Pharmacoepidemiology. 2024; 3(1):103-116. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma3010008
Chicago/Turabian StyleWalczuk, Samantha, Francesca E. Cunningham, Xinhua Zhao, Diane Dong, Peter A. Glassman, Donald R. Miller, Deborah Khachikian, Anthony Au, Cedric Salone, Kelly Bryan, and et al. 2024. "Treatment Patterns, Effectiveness, and Safety of Originator Insulin Glargine versus Insulin Glargine-yfgn within the Veterans Health Administration" Pharmacoepidemiology 3, no. 1: 103-116. https://0-doi-org.brum.beds.ac.uk/10.3390/pharma3010008