



Cancers 2023, 15(21), 5226; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15215226 - 31 Oct 2023
Viewed by 864
Abstract
►
Show Figures
Despite advances in cancer screening, late-stage cancer diagnosis is still a major cause of morbidity and mortality in the United States. In this study, we aim to understand demographic and geographic factors associated with receiving a late-stage diagnosis (LSD) of lung, colorectal, breast,
[...] Read more.
Despite advances in cancer screening, late-stage cancer diagnosis is still a major cause of morbidity and mortality in the United States. In this study, we aim to understand demographic and geographic factors associated with receiving a late-stage diagnosis (LSD) of lung, colorectal, breast, or cervical cancer. (1) Methods: We analyzed data of patients with a cancer diagnosis between 2016 and 2020 from the Florida Cancer Data System (FCDS), a statewide population-based registry. To investigate correlates of LSD, we estimated multi-variable logistic regression models for each cancer while controlling for age, sex, race, insurance, and census tract rurality and poverty. (2) Results: Patients from high-poverty rural areas had higher odds for LSD of lung (OR = 1.23, 95% CI (1.10, 1.37)) and breast cancer (OR = 1.31, 95% CI (1.17,1.47)) than patients from low-poverty urban areas. Patients in high-poverty urban areas saw higher odds of LSD for lung (OR = 1.05 95% CI (1.00, 1.09)), breast (OR = 1.10, 95% CI (1.06, 1.14)), and cervical cancer (OR = 1.19, 95% CI (1.03, 1.37)). (3) Conclusions: Financial barriers contributing to decreased access to care likely drive LSD for cancer in rural and urban communities of Florida.
Full article
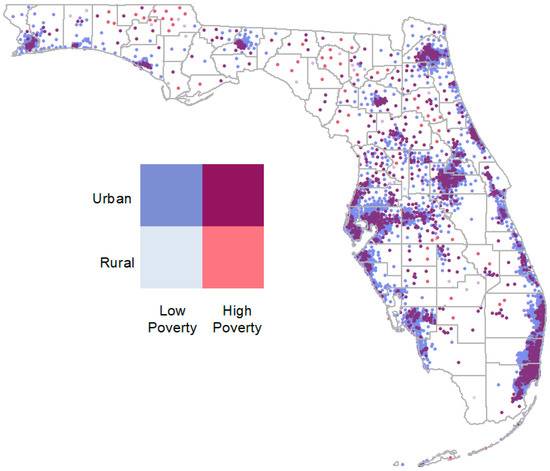
Figure 1


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}