
The Impact of Visual Input and Support Area Manipulation on Postural Control in Subjects after Osteoporotic Vertebral Fracture


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Data Analysis
2.2.1. Stationarity of CoP data
2.2.2. Sample Entropy (SampEn)
- (1)
- From a vector two sequences of m consecutive points: and were selected to compute the maximum distance and compared to tolerance r for repeated sequence counting, according to:where the tolerance r is equal to 0.1∼0.2∗SD and SD is the standard deviation of XN [19].
- (2)
- is the average amount of for and is the average of m + 1 consecutive points. Thus, sample entropy can be computed as follows:
2.2.3. Fractal Dimension (FD)
- (1)
- For one dimensional time series: , a new k time series can be formed as follows:where k and m are integers, is the integral part of , k indicates the discrete time interval between points, whereas m = 1, 2, …, k.
- (2)
- The length of each new time series can be defined as follows:where N is length of the original time series X.
- (3)
- The length of the curve for the time interval k is defined as the average of the k values L(m, k), for m = 1, 2, …, k:Finally, when L(k) is plotted against 1/k on a double logarithmic scale, with k = 1, 2, …, kmax, the data should fall on a straight line, with a slope equal to the FD of X. Thus, Higuchi’s FD is defined as the slope of the line that fits the pairs in a least-squares sense. In order to choose an appropriate value of the parameter kmax, Higuchi’s FD values were plotted against a range of kmax. The point at which the FD plateaus was considered a saturation point, and that kmax value should be selected [29]. A value of kmax = 100 was chosen for our study.
2.2.4. ANOVA Skillings–Mack (Missing Data)
3. Results
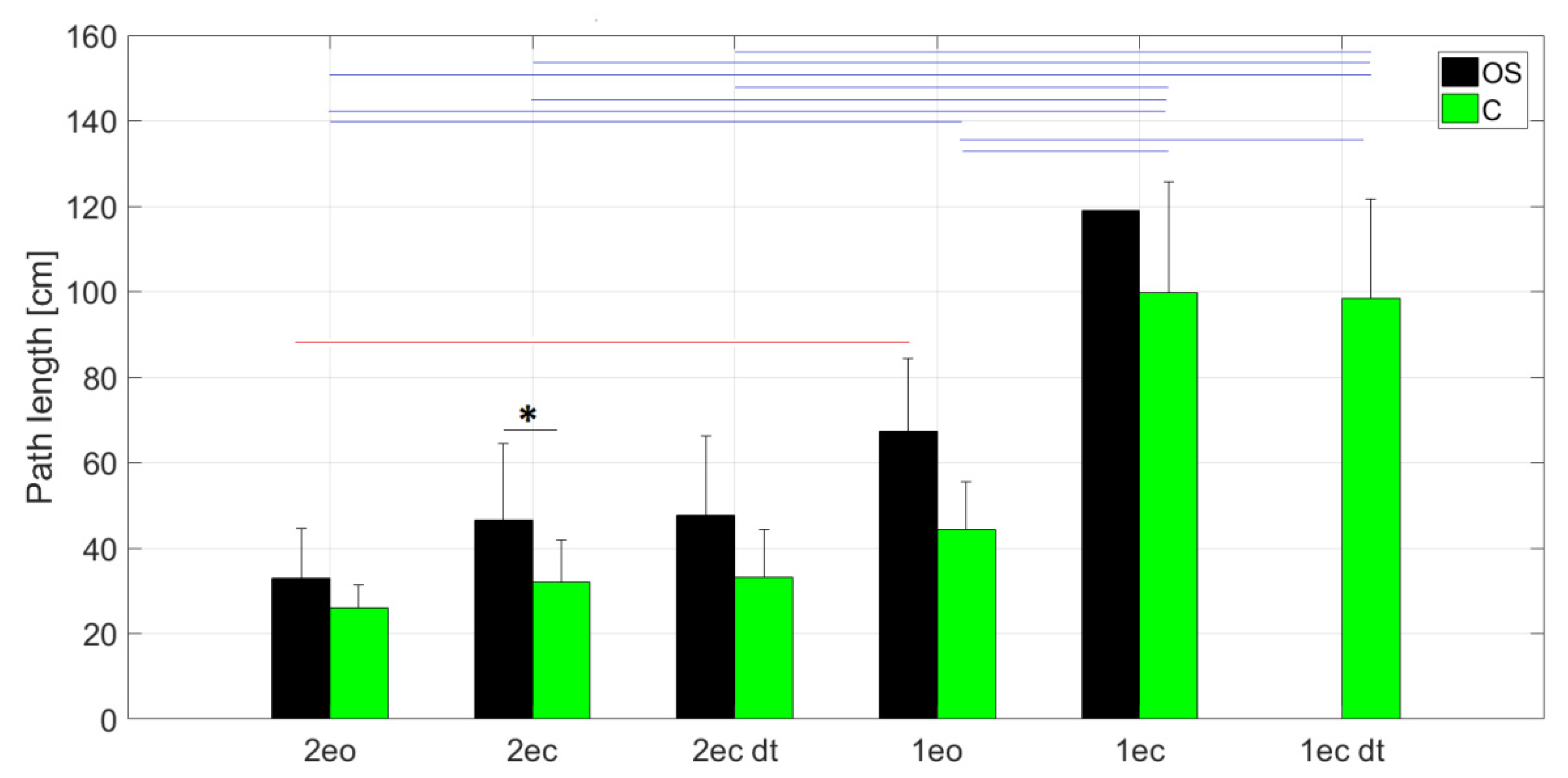
3.1. Increasing Task Difficulty
3.2. Nonlinear Dynamics Indicators
3.2.1. Analysis between Groups
3.2.2. Analysis within Groups
3.3. Fall Risk Test and Summary of Balance Test Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dionyssiotis, Y. Management of osteoporotic vertebral fractures. Int. J. Gen. Med. 2010, 3, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caracchini, G.; Cavalli, L. Severe osteoporosis: Diagnosis of femoral fractures. Clin. Cases Min. Bone Metab. 2010, 7, 97–101. [Google Scholar]
- Dobbs, M.B.; Buckwalter, J.; Saltzman, C. Osteoporosis: The increasing role of the orthopaedist. Iowa Orthop. J. 1999, 19, 43–52. [Google Scholar] [PubMed]
- World Health Organization. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group [Meeting Held in Rome from 22 to 25 June 1992]; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Miyakoshi, N.; Itoi, E.; Kobayashi, M.; Kodama, H. Impact of postural deformities and spinal mobility on quality of life in postmenopausal osteoporosis. Osteoporos. Int. 2003, 14, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Burke, T.N.; Franca, F.J.; Ferreira de Meneses, S.R.; Cardoso, V.I.; Marques, A.P. Postural control in elderly persons with osteoporosis: Efficacy of an intervention program to improve balance and muscle strength: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2010, 89, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Sinaki, M.; Brey, R.H.; Hughes, C.A.; Larson, D.R.; Kaufman, K.R. Balance disorder and increased risk of falls in osteoporosis and kyphosis: Significance of kyphotic posture and muscle strength. Osteoporos. Int. 2005, 16, 1004–1010. [Google Scholar] [CrossRef]
- Balzini, L.; Vannucchi, L.; Benvenuti, F.; Benucci, M.; Monni, M.; Cappozzo, A.; Stanhope, S.J. Clinical characteristics of flexed posture in elderly women. J. Am. Geriatr. Soc. 2003, 51, 1419–1426. [Google Scholar] [CrossRef]
- Halvarsson, A.; Franzen, E.; Stahle, A. Balance training with multi-task exercises improves fall-related self-efficacy, gait, balance performance and physical function in older adults with osteoporosis: A randomized controlled trial. Clin. Rehabil. 2015, 29, 365–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynn, S.G.; Sinaki, M.; Westerlind, K.C. Balance characteristics of persons with osteoporosis. Arch. Phys. Med. Rehabil. 1997, 78, 273–277. [Google Scholar] [CrossRef]
- Nguyen, T.; Sambrook, P.; Kelly, P.; Jones, G.; Lord, S.; Freund, J.; Eisman, J. Prediction of osteoporotic fractures by postural instability and bone density. BMJ 1993, 307, 1111–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.Y.; Liaw, M.Y.; Huang, Y.C.; Lau, Y.C.; Leong, C.P.; Pong, Y.P.; Chen, C.L. Static and dynamic balance performance in patients with osteoporotic vertebral compression fracture. J. Back Musculoskelet. Rehabil. 2013, 26, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Eng, J.J.; Khan, K.M.; Carter, N.D.; McKay, H.A. Older Women with Osteoporosis Have Increased Postural Sway and Weaker Quadriceps Strength Than Counterparts with Normal Bone Mass: Overlooked Determinants of Fracture Risk? J. Gerontol. Ser. A 2003, 58, M862–M866. [Google Scholar] [CrossRef] [PubMed]
- Donker, S.F.; Roerdink, M.; Greven, A.J.; Beek, P.J. Regularity of center-of-pressure trajectories depends on the amount of attention invested in postural control. Exp. Brain Res. 2007, 181, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roerdink, M.; Hlavackova, P.; Vuillerme, N. Center-of-pressure regularity as a marker for attentional investment in postural control: A comparison between sitting and standing postures. Hum. Mov. Sci. 2011, 30, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmit, J.M.; Regis, D.I.; Riley, M.A. Dynamic patterns of postural sway in ballet dancers and track athletes. Exp. Brain Res. 2005, 163, 370–378. [Google Scholar] [CrossRef]
- Ramdani, S.; Tallon, G.; Bernard, P.L.; Blain, H. Recurrence quantification analysis of human postural fluctuations in older fallers and non-fallers. Ann. Biomed. Eng. 2013, 41, 1713–1725. [Google Scholar] [CrossRef] [PubMed]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The appropriate use of approximate entropy and sample entropy with short data sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Higuchi, T. Approach to an irregular time series on the basis of the fractal theory. Phys. D Nonlinear Phenom. 1988, 31, 277–283. [Google Scholar] [CrossRef]
- Kedziorek, J.; Blazkiewicz, M. Nonlinear Measures to Evaluate Upright Postural Stability: A Systematic Review. Entropy 2020, 22, 1357. [Google Scholar] [CrossRef]
- Potvin-Desrochers, A.; Richer, N.; Lajoie, Y. Cognitive tasks promote automatization of postural control in young and older adults. Gait Posture 2017, 57, 40–45. [Google Scholar] [CrossRef]
- Georgoulis, A.D.; Moraiti, C.; Ristanis, S.; Stergiou, N. A novel approach to measure variability in the anterior cruciate ligament deficient knee during walking: The use of the approximate entropy in orthopaedics. J. Clin. Monit. Comput. 2006, 20, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Doyle, T.L.; Newton, R.U.; Burnett, A.F. Reliability of traditional and fractal dimension measures of quiet stance center of pressure in young, healthy people. Arch. Phys. Med. Rehabil. 2005, 86, 2034–2040. [Google Scholar] [CrossRef]
- Zhivomirov, H. Stationarity Estimation of a Signal with Matlab. Available online: https://www.mathworks.com/matlabcentral/fileexchange/75118-stationarity-estimation-of-a-signal-with-matlab (accessed on 10 March 2021).
- Stergiou, N. Nonlinear Analysis for Human Movement Variability; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Lubetzky, A.V.; Harel, D.; Lubetzky, E. On the effects of signal processing on sample entropy for postural control. PLoS ONE 2018, 13, e0193460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [Green Version]
- Doyle, T.L.A.; Dugan, E.L.; Humphries, B.; Newton, R.U. Discriminating between elderly and young using a fractal dimension analysis of centre of pressure. Int. J. Med. Sci. 2004, 1, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatfield, M.; Mander, A. The Skillings-Mack test (Friedman test when there are missing data). Stata J. 2009, 9, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Skillings, J.H.; Mack, G.A. On the use of a Friedman-type statistic in balanced and unbalanced block designs. Technometrics 1981, 23, 171–177. [Google Scholar] [CrossRef]
- Ghahramani, M. Fall Risk Assessment in Older People. Int. J. Eng. Sci. 2016, 5, 1–14. [Google Scholar] [CrossRef]
- Zijlstra, A.; Ufkes, T.; Skelton, D.A.; Lundin-Olsson, L.; Zijlstra, W. Do dual tasks have an added value over single tasks for balance assessment in fall prevention programs? A mini-review. Gerontology 2008, 54, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.; Gu, M.O.; Yim, J. Comparison of Walking, Muscle Strength, Balance, and Fear of Falling between Repeated Fall Group, One-time Fall Group, and Nonfall Group of the Elderly Receiving Home Care Service. Asian Nurs. Res. 2017, 11, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha-Henriques, S.; Costa-Paiva, L.; Pinto-Neto, A.M.; Fonsechi-Carvesan, G.; Nanni, L.; Morais, S.S. Postmenopausal women with osteoporosis and musculoskeletal status: A comparative cross-sectional study. J. Clin. Med. Res. 2011, 3, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Kinsner, W. System Complexity and Its Measures: How Complex Is Complex. In Advances in Cognitive Informatics and Cognitive Computing. Studies in Computational Intelligence; Wang, Y., Zhang, D., Kinsner, W., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; Volume 323. [Google Scholar]
- Radaei, F.; Shirazi, S.Y.; Gharibzadeh, S.; Khashayar, P.; Ramezani, M.; Fatouraee, N. Evaluation of Relationship between Balance Parameters and Bone Mineral Density. In Proceedings of the 2015 22nd Iranian Conference on Biomedical Engineering (ICBME), Tehran, Iran, 25–27 November 2015. [Google Scholar] [CrossRef]
- Abreu, D.C.; Trevisan, D.C.; Costa, G.C.; Vasconcelos, F.M.; Gomes, M.M.; Carneiro, A.A. The association between osteoporosis and static balance in elderly women. Osteoporos. Int. 2010, 21, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- da Costa, C.S.; Batistao, M.V.; Rocha, N.A. Quality and structure of variability in children during motor development: A systematic review. Res. Dev. Disabil. 2013, 34, 2810–2830. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, N.; Decker, L.M. Human movement variability, nonlinear dynamics, and pathology: Is there a connection? Hum. Mov. Sci. 2011, 30, 869–888. [Google Scholar] [CrossRef] [Green Version]
- Lipsitz, L.A.; Goldberger, A.L. Loss of ‘complexity’ and aging. Potential applications of fractals and chaos theory to senescence. JAMA 1992, 267, 1806–1809. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, N.; Harbourne, R.; Cavanaugh, J. Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J. Neurol. Phys. 2006, 30, 120–129. [Google Scholar] [CrossRef] [Green Version]
- Ramdani, S.; Seigle, B.; Lagarde, J.; Bouchara, F.; Bernard, P.L. On the use of sample entropy to analyze human postural sway data. Med. Eng. Phys. 2009, 31, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.P.; Seigle, B.; Frère, J.; Parietti-Winkler, C. Dynamical analysis of balance in vestibular schwannoma patients. Gait Posture 2017, 54, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Da Costa Barbosa, R.; Vieira, M.F. Postural Control of Elderly Adults on Inclined Surfaces. Ann. Biomed. Eng. 2017, 45, 726–738. [Google Scholar] [CrossRef]
- Rhea, C.K.; Kiefer, A.W.; Wright, W.G.; Raisbeck, L.D.; Haran, F.J. Interpretation of postural control may change due to data processing techniques. Gait Posture 2015, 41, 731–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, L.; Li, Y.; Ye, J.; Yang, X.; Wang, J. Emotion-induced higher wavelet entropy in the EEG with depression during a cognitive task. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2009, 2009, 5018–5021. [Google Scholar] [CrossRef]
- Borg, F.G.; Laxaback, G. Entropy of balance—Some recent results. J. Neuroeng. Rehabil. 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, C.; Wei, Q.; Shieh, J.S.; Fourcade, P.; Isableu, B.; Majed, L. Sample Entropy, Univariate, and Multivariate Multi-Scale Entropy in Comparison with Classical Postural Sway Parameters in Young Healthy Adults. Front. Hum. Neurosci. 2017, 11, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjuya, N.; Melzer, I.; Kaplanski, J. Aging-induced shifts from a reliance on sensory input to muscle cocontraction during balanced standing. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Hsu, W.L.; Lin, K.H.; Yang, R.S.; Cheng, C.H. Use of motor abundance in old adults in the regulation of a narrow-based stance. Eur. J. Appl. Physiol. 2014, 114, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Madeleine, P.; Nielsen, M.; Arendt-Nielsen, L. Characterization of postural control deficit in whiplash patients by means of linear and nonlinear analyses—A pilot study. J. Electromyogr. Kinesiol. 2011, 21, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Raffalt, P.C.; Spedden, M.E.; Geertsen, S.S. Dynamics of postural control during bilateral stance—Effect of support area, visual input and age. Hum. Mov. Sci. 2019, 67, 102462. [Google Scholar] [CrossRef] [PubMed]
- Sempere-Rubio, N.; Lopez-Pascual, J.; Aguilar-Rodriguez, M.; Cortes-Amador, S.; Espi-Lopez, G.; Villarrasa-Sapina, I.; Serra-Ano, P. Characterization of postural control impairment in women with fibromyalgia. PLoS ONE 2018, 13, e0196575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaszczyk, J.W.; Klonowski, W. Postural stability and fractal dynamics. Acta Neurobiol. Exp. (Wars) 2001, 61, 105–112. [Google Scholar]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Balance failure in single limb stance due to ankle sprain injury: An analysis of center of pressure using the fractal dimension method. Gait Posture 2014, 40, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.H.; Lin, R.M.; Chang, R.I.; Lin, Y.W.; Chang, G.L. Radiographic and balance characteristics for patient with osteoporotic vertebral fracture. J. Chin. Inst. Eng. 2004, 27, 377–383. [Google Scholar] [CrossRef]
- Greig, A.M.; Bennell, K.L.; Briggs, A.M.; Wark, J.D.; Hodges, P.W. Balance impairment is related to vertebral fracture rather than thoracic kyphosis in individuals with osteoporosis. Osteoporos. Int. 2007, 18, 543–551. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Task | Symbol | Number of Subjects Who Completed the OS/C Tasks |
|---|---|---|
| Standing on both legs with eyes open | 2eo | 17/17 |
| Standing on both legs with eyes closed | 2ec | 16/17 |
| Standing on both legs with eyes closed and with dual-task | 2ec_dt | 15/17 |
| Standing on one leg with eyes open | 1eo | 8/17 |
| Standing on one leg with eyes closed | 1ec | 1/17 |
| Standing on one leg with eyes closed and with dual-task | 1ec_dt | 0/17 |
| Number of Subjects Who Completed the FRT | Norm Level for the FRT Test | 2eo | 2ec | 2ec_dt | 1eo | 1ec | 1ec_dt |
|---|---|---|---|---|---|---|---|
| 3 | Fall | X | X | X | - | - | - |
| 1 | Fall | X | X | - | - | - | - |
| 1 | Fall | X | - | - | - | - | - |
| 2 | Fall | X | X | X | X | - | - |
| 3 | Norm | X | X | X | - | - | - |
| 3 | Norm | X | X | X | X | - | - |
| 1 | Below | X | X | X | X | X | - |
| 2 | Below | X | X | X | X | - | - |
| 1 | Below | X | X | X | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błażkiewicz, M.; Kędziorek, J.; Hadamus, A. The Impact of Visual Input and Support Area Manipulation on Postural Control in Subjects after Osteoporotic Vertebral Fracture. Entropy 2021, 23, 375. https://0-doi-org.brum.beds.ac.uk/10.3390/e23030375
Błażkiewicz M, Kędziorek J, Hadamus A. The Impact of Visual Input and Support Area Manipulation on Postural Control in Subjects after Osteoporotic Vertebral Fracture. Entropy. 2021; 23(3):375. https://0-doi-org.brum.beds.ac.uk/10.3390/e23030375
Chicago/Turabian StyleBłażkiewicz, Michalina, Justyna Kędziorek, and Anna Hadamus. 2021. "The Impact of Visual Input and Support Area Manipulation on Postural Control in Subjects after Osteoporotic Vertebral Fracture" Entropy 23, no. 3: 375. https://0-doi-org.brum.beds.ac.uk/10.3390/e23030375