
Discrimination of Patients with Varying Degrees of Coronary Artery Stenosis by ECG and PCG Signals Based on Entropy

 ,
,  ,
,
Abstract
:1. Introduction
- (1)
- Patients with varying degrees of coronary artery stenosis are given different treatment programs clinically. At present, other than coronary angiography, there is no effective noninvasive technique for the identification of patients with varying degrees of coronary artery stenosis. Therefore, it is very necessary to accurately identify patients with varying degrees of coronary artery stenosis in clinical practice. In this study, 191 patients with varying degrees of coronary artery stenosis were studied. The classification accuracy for a severe CAD–mild-to-moderate CAD group, severe CAD–chest pain and normal coronary angiography group, and mild-to-moderate CAD–chest pain and normal coronary angiography group was 0.80, 0.77, and 0.75, respectively. The results show that this study can provide a valuable reference for clinicians to diagnose CAD.
- (2)
- Multitype coupling feature sets were constructed. It was verified that the entropy-based coupling feature set was more suitable for the discrimination of patients with varying degrees of coronary artery stenosis.
- (3)
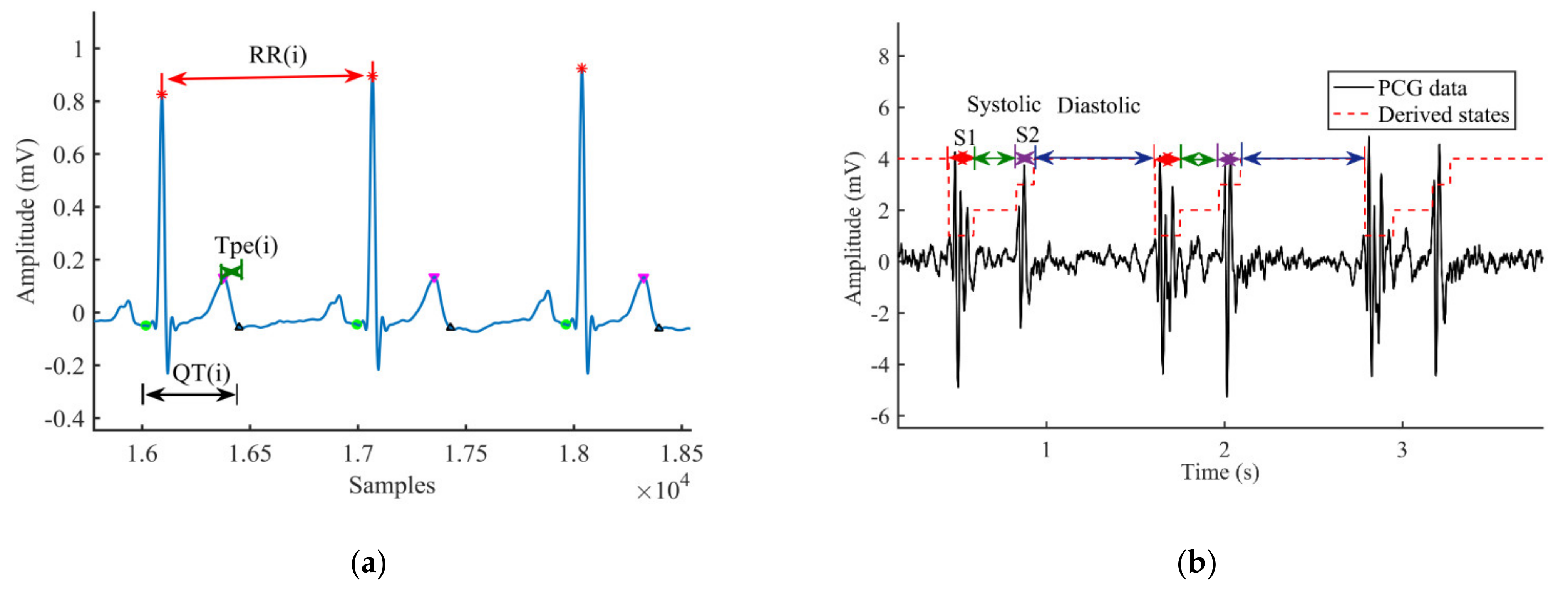
- Dysfunction of the cardiovascular system may result in abnormal electromechanical activity of the heart. In this study, ECG and PCG signals of patients were collected synchronously, and different types of time series intervals related to CAD were extracted. The results confirmed that the coupling series composed of TpeI, Tpe/QTI, DTI, and STI contributed the most to the identification of patients with varying degrees of coronary artery stenosis, which has a guiding significance for the clinical identification of CAD.
2. Materials and Methods
2.1. Data Acquisition
2.2. Preprocessing
2.3. The Localization of Fiducial Points
2.3.1. ECG Signals
2.3.2. PCG Signals
2.4. Feature Extraction
2.4.1. XSampEn
- (1)
- For the two normalized time series and , , state space reconstruction is carried out to obtain and , respectively.
- (2)
- is calculated.
- (3)
- The XsampEn is defined as follows:
2.4.2. XfuzzyEn
2.4.3. JdistEn
- (1)
- For the normalized time series , the state space is reconstructed:where , , , is the embedding dimension, and is the time delay. The input parameters m and were set at 2 and 3, respectively.
- (2)
- A joint distance matrix is constructed:where J is the all-ones matrix, and and are the distance matrix.
- (3)
- Probability density is estimated.
- (4)
- The JdistEn is defined as follows:where is the probability of each histogram.
2.4.4. MSCF
2.4.5. CPSD
2.4.6. MI
- (1)
- For given the series X, Y, N data pairs (xi, yj) are formed, I = j = 1,…, N.
- (2)
- For I = 1,…,N, the probabilities Px(xi) and Py(yj) are estimated at the sample point using Equations (14)—(17), respectively. Px,y (xi,yj) is calculated using the same formula:where Px,y (xi,yj) is the joint probability density of x and y evaluated at (xi,yj), and Px(xi) and Py(yj) are the marginal probability densities of x and y evaluated at xi and yj, respectively. d was set to 2. N is the length of the series. h is the kernel bandwidth, and S(y) is the covariance matrix on the y. K(u) is the multivariate Gaussian probability density function.
- (3)
- Where the overall dependence between the two series is of interest, one can define the average mutual information , as:
2.5. Feature Selection
2.6. Classification
3. Results
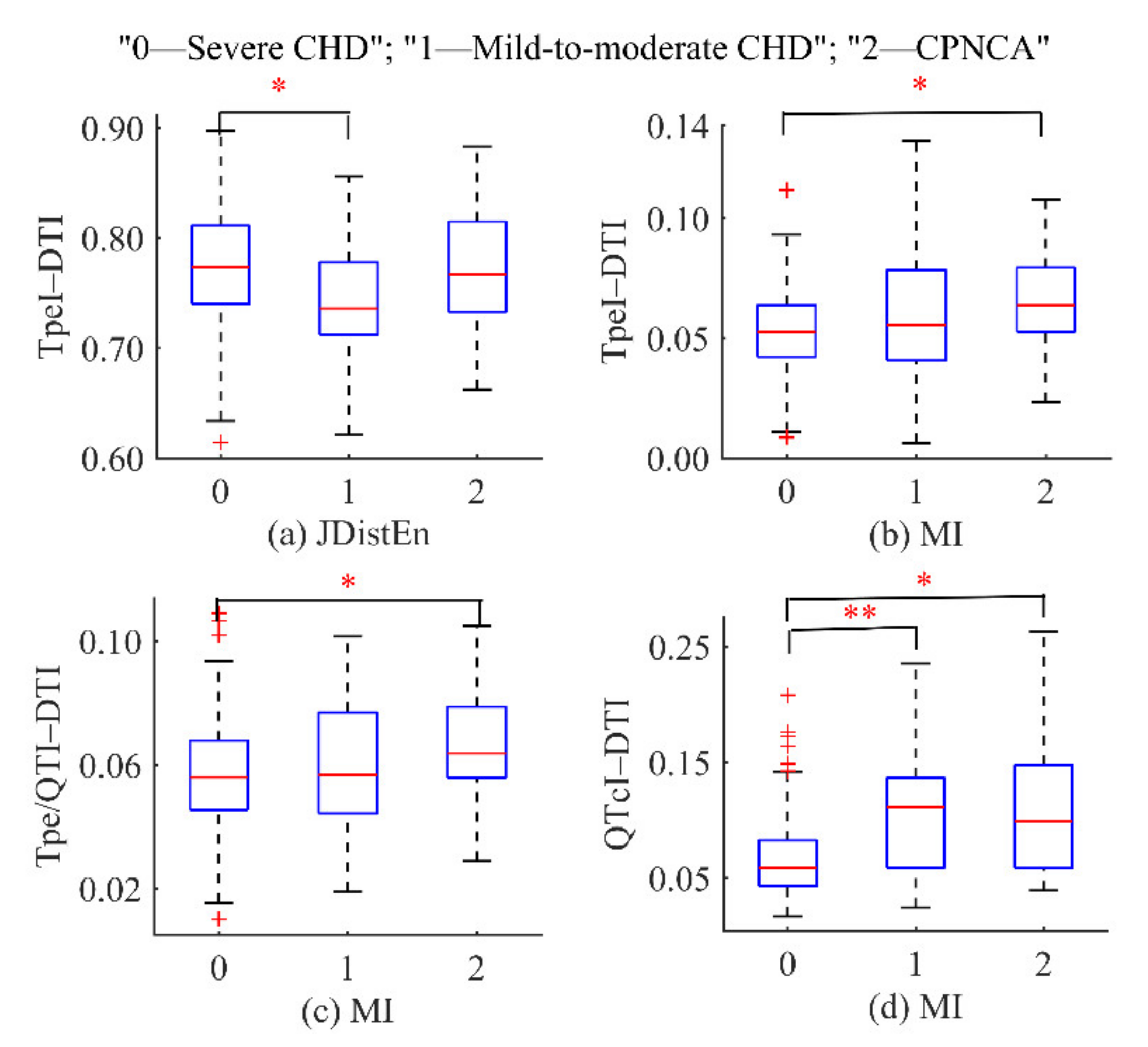
3.1. Statistical Analysis
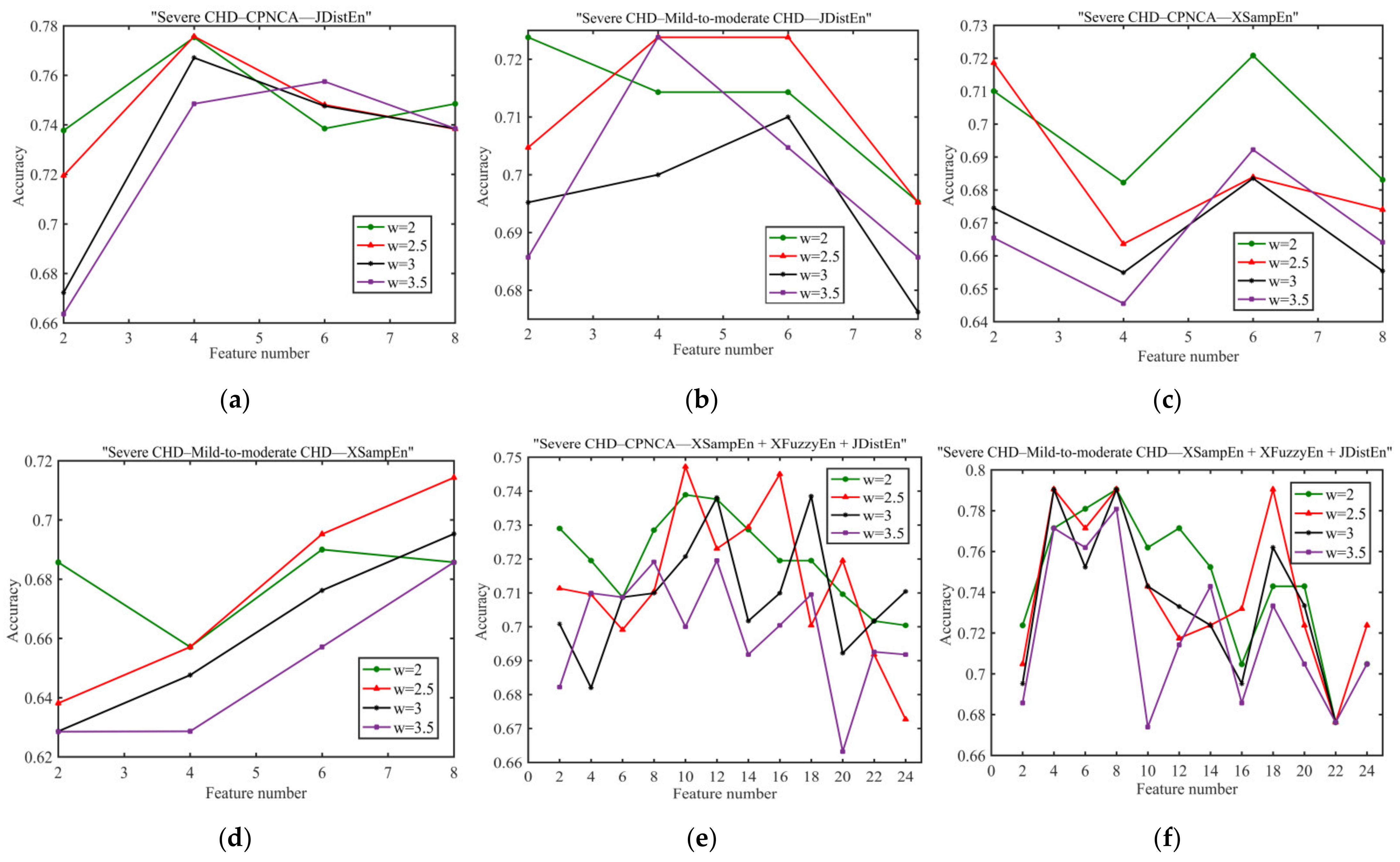
3.2. Parameter Selection
3.3. Feature Selection Results
3.4. Classification Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fox, K.A.A.; Metra, M.; Morais, J.; Atar, D. The myth of ‘stable’ coronary artery disease. Nat. Rev. Cardiol. 2020, 17, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Bonow, R.O. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, Single Volume, 9th ed; Elsevier/Saunders: Philadelphia, PA, USA, 2012; pp. 1076–1086. [Google Scholar]
- Al’Aref, S.J.; Anchouche, K.; Singh, G.; Slomka, P.J.; Kolli, K.K.; Kumar, A.; Pandey, M.; Maliakal, G.; Van Rosendael, A.R.; Beecy, A.N.; et al. Clinical applications of machine learning in cardiovascular disease and its relevance to cardiac imaging. Eur. Heart J. 2019, 40, 1975–1986. [Google Scholar] [CrossRef]
- Lab, M.J. Mechanoelectric Transduction/Feedback: Physiology and Pathophysiology. In Cardiac Mechanotransduction; Weck-ström, M., Tavi, P., Eds.; Springer: New York, NY, USA, 2007; pp. 48–77. [Google Scholar]
- Quinn, T.A.; Kohl, P. Cardiac Mechano-Electric Coupling: Acute Effects of Mechanical Stimulation on Heart Rate and Rhythm. Physiol. Rev. 2021, 101, 37–92. [Google Scholar] [CrossRef] [PubMed]
- Lab, M.J. Mechanoelectric feedback (transduction) in heart: Concepts and implications. Cardiovasc. Res. 1996, 32, 3–14. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Liu, C.; Li, L.; Yan, C.; Yao, L.; Li, P. Variability of Cardiac Electromechanical Delay with Application to the Noninvasive Detection of Coronary Artery Disease. IEEE Access 2019, 7, 53115–53124. [Google Scholar] [CrossRef]
- Ansari-Asl, K.; Senhadji, L.; Bellanger, J.-J.; Wendling, F. Quantitative evaluation of linear and nonlinear methods charac-terizing interdependencies between brain signals. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2006, 74, 031916. [Google Scholar]
- Ruiz-Blais, S.; Orini, M.; Chew, E. Heart Rate Variability Synchronizes When Non-experts Vocalize Together. Front. Physiol. 2020, 11, 762. [Google Scholar] [CrossRef]
- Pathak, A.; Samanta, P.; Mandana, K.; Saha, G. An improved method to detect coronary artery disease using phonocardio-gram signals in noisy environment. Appl. Acoust. 2020, 164, 107242. [Google Scholar] [CrossRef]
- Martínez-Cancino, R.; Heng, J.; Delorme, A.; Kreutz-Delgado, K.; Sotero, R.C.; Makeig, S. Measuring transient phase-amplitude coupling using local mutual information. NeuroImage 2019, 185, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Paluš, M.; Stefanovska, A. Direction of coupling from phases of interacting oscillators: An information-theoretic approach. Phys. Rev. E 2003, 67, 055201. [Google Scholar] [CrossRef]
- Xiao, M.-X.; Wei, H.-C.; Xu, Y.-J.; Wu, H.-T.; Sun, C.-K. Combination of R-R Interval and Crest Time in Assessing Complexity Using Multiscale Cross-Approximate Entropy in Normal and Diabetic Subjects. Entropy 2018, 20, 497. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Yang, L.; Su, Z.; Liu, C. Cardiorespiratory Coupling Analysis Based on Entropy and Cross-Entropy in Distinguishing Different Depression Stages. Front. Physiol. 2019, 10, 359. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.; Bär, K.-J.; Voss, A. Analyses of Heart Rate, Respiration and Cardiorespiratory Coupling in Patients with Schizo-phrenia. Entropy 2015, 17, 483–501. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Sun, Z. Characterization of QT and RR interval series during acute myocardial ischemia by means of recurrence quantification analysis. Med Biol. Eng. Comput. 2010, 49, 25–31. [Google Scholar] [CrossRef]
- Nasario-Junior, O.; Benchimol-Barbosa, P.R.; Nadal, J. IEEE, Beat-to-beat T-peak T-end Interval Duration Variability Assessed by RR-Interval Histogram Analysis in Health Sedentary and Athlete. In Proceedings of the 2017 Computing in Cardiology, Rennes, France, 24–27 September 2017; Volume 44. [Google Scholar]
- Li, P.; Li, K.; Liu, C.; Zheng, D.; Li, Z.; Liu, C. Detection of Coupling in Short Physiological Series by a Joint Distribution Entropy Method. IEEE Trans. Biomed. Eng. 2016, 63, 2231–2242. [Google Scholar] [CrossRef]
- Zhao, L.; Wei, S.; Tang, H.; Liu, C. Multivariable Fuzzy Measure Entropy Analysis for Heart Rate Variability and Heart Sound Amplitude Variability. Entropy 2016, 18, 430. [Google Scholar] [CrossRef] [Green Version]
- Ji, L.; Li, P.; Liu, C.; Wang, X.; Yang, J.; Liu, C. Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects. Entropy 2016, 18, 153. [Google Scholar] [CrossRef] [Green Version]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Schafer, R.W. What Is a Savitzky-Golay Filter? [Lecture Notes]. IEEE Signal Process. Mag. 2011, 28, 111–117. [Google Scholar] [CrossRef]
- Maheshwari, S.; Acharyya, A.; Puddu, P.E.; Mazomenos, E.B.; Leekha, G.; Maharatna, K.; Schiariti, M. An automated al-gorithm for online detection of fragmented QRS and identification of its various morphologies. J. R. Soc. Interface 2013, 10, 20130761. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, J.; Johannesen, L.; Grove, U.; Lundhus, K.; Couderc, J.-P.; Graff, C. A Comparison of IIR and Wavelet Filtering for Noise Reduction of the ECG. Comput. Cardiol. 2010, 37, 489–492. [Google Scholar]
- Afonso, V.; Tompkins, W.; Nguyen, T.; Luo, S. ECG beat detection using filter banks. IEEE Trans. Biomed. Eng. 1999, 46, 192–202. [Google Scholar] [CrossRef]
- Hu, X.; Liu, J.; Wang, J.; Xiao, Z.; Yao, J. Automatic detection of onset and offset of QRS complexes independent of isoelectric segments. Measurement 2014, 51, 53–62. [Google Scholar] [CrossRef]
- Zhang, Q.; Manriquez, A.I.; Medigue, C.; Papelier, Y.; Sorine, M. An Algorithm for Robust and Efficient Location of T-Wave Ends in Electrocardiograms. IEEE Trans. Biomed. Eng. 2006, 53, 2544–2552. [Google Scholar] [CrossRef]
- Xue, Q.; Reddy, S. Algorithms for computerized QT analysis. J. Electrocardiol. 1998, 30, 181–186. [Google Scholar] [CrossRef]
- Springer, D.B.; Tarassenko, L.; Clifford, G.D. Logistic Regression-HSMM-based Heart Sound Segmentation. IEEE Trans. Biomed. Eng. 2015, 63, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Michler, K.; Johnston, P.; Macfarlane, P.W. A comparison of commonly used QT correction formulae: The effect of heart rate on the QTc of normal ECGs. J. Electrocardiol. 2004, 37, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Perkiomaki, J.S.; Koistinen, M.J.; Ylimayry, S.; Huikuri, H.V. Dispersion of QT interval in patients with and without sus-ceptibility to ventricular tachyarrhythmias after previous myocardial infarction. J. Am. Coll. Cardiol. 1995, 26, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Panikkath, R.; Reinier, K.; Uy-Evanado, A.; Teodorescu, C.; Hattenhauer, J.; Mariani, R.; Gunson, K.; Jui, J.; Chugh, S.S. Prolonged Tpeak-to-Tend Interval on the Resting ECG Is Associated with Increased Risk of Sudden Cardiac Death. Circ. Arrhythmia Electrophysiol. 2011, 4, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.-B.; Zheng, Y.-P.; Guo, J.-Y.; Chen, X. Cross-fuzzy entropy: A new method to test pattern synchrony of bivariate time series. Inf. Sci. 2010, 180, 1715–1724. [Google Scholar] [CrossRef]
- Doane, D.P. Aesthetic frequency classifications. Am. Stat. 1976, 30, 181–183. [Google Scholar]
- Moon, Y.I.; Rajagopalan, B.; Lall, U. Estimation of mutual information using kernel density estima-tors. Phys. Rev. E 1995, 52, 2318–2321. [Google Scholar] [CrossRef] [PubMed]
- Guyon, I.; Weston, J.; Barnhill, S.; Vapnik, V. Gene Selection for Cancer Classification using Support Vector Machines. Mach. Learn. 2002, 46, 389–422. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Li, P.; Liu, C.; Wang, X.; Li, L.; Yang, L.; Chen, Y.; Liu, C. Testing pattern synchronization in coupled systems through different entropy-based measures. Med. Biol. Eng. Comput. 2013, 51, 581–591. [Google Scholar] [CrossRef]
- Semmlow, J.; Akay, M.; Welkowitz, W. Noninvasive detection of coronary artery disease using parametric spectral analysis methods. IEEE Eng. Med. Boil. Mag. 1990, 9, 33–36. [Google Scholar] [CrossRef]
- Wang, J.-Z.; Tie, B.; Welkowitz, W.; Semmlow, J.; Kostis, J. Modeling sound generation in stenosed coronary arteries. IEEE Trans. Biomed. Eng. 1990, 37, 1087–1094. [Google Scholar] [CrossRef]
- Li, P.; Ji, L.; Yan, C.; Li, K.; Liu, C.; Liu, C. Coupling between Short-Term Heart Rate and Diastolic Period is Reduced in Heart Failure Patients as Indicated by Multivariate Entropy Analysis. In Proceedings of the 2014 Computing in Cardiology Conference, Cambridge, MA, USA, 7–10 September 2014; pp. 97–100. [Google Scholar]
- Porta, A.; Bari, V.; Badilini, F.; Tobaldini, E.; Gnecchi-Ruscone, T.; Montano, N. Frequency domain assessment of the coupling strength between ventricular repolarization duration and heart period during graded head-up tilt. J. Electrocardiol. 2011, 44, 662–668. [Google Scholar] [CrossRef] [Green Version]
- Baumert, M.; Czippelova, B.; Porta, A.; Javorka, M. Decoupling of QT interval variability from heart rate variability with ageing. Physiol. Meas. 2013, 34, 1435–1448. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Liu, C.; Sun, X.; Ren, Y.; Yan, C.; Yu, Z.; Liu, C. IEEE, Age Related Changes in Variability of Short-Term Heart Rate and Diastolic Period. In Proceedings of the 2013 Computing in Cardiology Conference, Zaragoza, Spain, 22–25 September 2013; pp. 995–998. [Google Scholar]
- Collet, A.; Desaive, T.; Dauby, P.C. One-dimensional time-dependent model of the cardiac pacemaker activity induced by the mechanoelectric feedback in a thermo-electro-mechanical background. Ann. Cardiol. Angeiol. 2012, 61, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Fossa, A.A.; Zhou, M.; Robinson, A.; Purkayastha, J.; Martin, P. Use of ECG Restitution (Beat-to-Beat QT-TQ Interval Analysis) to Assess Arrhythmogenic Risk of QTc Prolongation with Guanfacine. Ann. Noninvasive Electrocardiol. 2014, 19, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-C.; Liu, X.-H.; Liu, L.-B.; Li, S.-M.; Wang, Y.-Q.; Mead, R.H. Evaluation of left ventricular systolic function using syn-chronized analysis of heart sounds and the electrocardiogram. Heart Rhythm 2020, 17, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Dobson, C.P.; Kim, A.; Haigney, M. QT Variability Index. Prog. Cardiovasc. Dis. 2013, 56, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E.; et al. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar]
- Zhao, X.; Xie, Z.; Chu, Y.; Yang, L.; Xu, W.; Yang, X.; Liu, X.; Tian, L. Association Between Tp-e/QT Ratio and Prognosis in Patients Undergoing Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. Clin. Cardiol. 2012, 35, 559–564. [Google Scholar] [CrossRef]
- Castro Hevia, J.; Antzelevitch, C.; Tornés Bárzaga, F.; Dorantes Sánchez, M.; Dorticós Balea, F.; Zayas Molina, R.; Quiñones Pérez, M.A.; Fayad Rodríguez, Y. Tpeak-Tend and Tpeak-Tend Dispersion as Risk Factors for Ventricular Tachycar-dia/Ventricular Fibrillation in Patients with the Brugada Syndrome. J. Am. Coll. Cardiol. 2006, 47, 1828–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jukic, A.; Carevic, V.; Zekanovic, D.; Stojanović-Stipić, S.; Runjic, F.; Ljubkovic, M.; Fabijanić, D. Impact of Percutaneous Coronary Intervention on Exercise-Induced Repolarization Changes in Patients with Stable Coronary Artery Disease. Am. J. Cardiol. 2015, 116, 853–857. [Google Scholar] [CrossRef]
- Tang, H.; Dai, Z.; Jiang, Y.; Li, T.; Liu, C. PCG Classification Using Multidomain Features and SVM Classifier. BioMed Res. Int. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Semmlow, J.; Rahalkar, K. Acoustic Detection of Coronary Artery Disease. Annu. Rev. Biomed. Eng. 2007, 9, 449–469. [Google Scholar] [CrossRef]
- Schmidt, S.E.; Holst-Hansen, C.; Hansen, J.; Toft, E.; Struijk, J.J. Acoustic Features for the Identification of Coronary Artery Disease. IEEE Trans. Biomed. Eng. 2015, 62, 2611–2619. [Google Scholar] [CrossRef]
- Hnatkova, K.; Kowalski, D.; Keirns, J.J.; Van Gelderen, E.M.; Malik, M. Relationship of QT interval variability to heart rate and RR interval variability. J. Electrocardiol. 2013, 46, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Mozos, I.; Filimon, L. QT and Tpeak-Tend intervals in shift workers. J. Electrocardiol. 2013, 46, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Magagnin, V.; Bassani, T.; Bari, V.; Turiel, M.; Maestri, R.; Pinna, G.D.; Porta, A. Non-stationarities significantly distort short-term spectral, symbolic and entropy heart rate variability indices. Physiol. Meas. 2011, 32, 1775–1786. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | CPNCA Group | Mild-to-Moderate CHD Group | Severe CHD Group |
|---|---|---|---|
| Male/female | 20/20 | 20/17 | 71/43 |
| Age (year) | 60 ± 11 | 63 ± 7 | 65 ± 9 |
| Height (cm) | 163 ± 7 | 165 ± 7 | 166 ± 7 |
| Weight (kg) | 69 ± 13 | 68 ± 9 | 69 ± 11 |
| Body mass index (kg/m2) | 26 ± 3 | 26 ± 3 | 25 ± 3 |
| Systolic blood pressure (mmHg) | 128 ± 16 | 133 ± 16 | 137 ± 18 |
| Diastolic blood pressure (mmHg) | 81 ± 11 | 81 ± 9 | 85 ± 16 |
| Severe CHD–CPNCA | Severe CHD– Mild-to-Moderate CHD | Mild-to-Moderate CHD–CPNCA |
|---|---|---|
| RRI–STI–XS | RRI–STI–XF | RRI–STI–XS |
| RRI–STI–JD | RRI–STI–JD | RRI–STI–XF |
| RRI–DTI–JD | RRI–DTI–XF | QTcI–STI–XS |
| QTcI–STI–XS | RRI–DTI–JD | QTcI–DTI–XF |
| TpeI–STI–XF | QTcI–STI–XF | QTcI–DTI–JD |
| TpeI–STI–JD | QTcI–DTI–XF | TpeI–STI–XS |
| TpeI–DTI–XF | QTcI–DTI–JD | TpeI–DTI–XS |
| Tpe/QTI–STI–XS | TpeI–STI–XS | TpeI–DTI–JD |
| Tpe/QTI–STI–XF | TpeI–STI–XF | Tpe/QTI–STI–XS |
| Tpe/QTI–STI–JD | TpeI–STI–JD | Tpe/QTI–STI–JD |
| TpeI–DTI–XS | Tpe/QTI–DTI–XS | |
| TpeI–DTI–XF | Tpe/QTI–DTI–JD | |
| TpeI–DTI–JD | ||
| Tpe/QTI–STI–XF | ||
| Tpe/QTI–STI–JD | ||
| Tpe/QTI–DTI–XS | ||
| Tpe/QTI–DTI–XF | ||
| Tpe/QTI–DTI–JD |
| Groups | Methods | Accuracy | F1-Score | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|---|
| Severe CHD– Mild-to-moderate CHD | MI | 0.6522 | 0.7714 | 0.7714 | 0.2727 | 0.5792 |
| XFuzzyEn | 0.7174 | 0.8267 | 0.8857 | 0.1818 | 0.5636 | |
| JDistEn | 0.7391 | 0.8286 | 0.8286 | 0.4545 | 0.6195 | |
| MSCF | 0.7391 | 0.8286 | 0.8286 | 0.4545 | 0.6468 | |
| CPSD | 0.7608 | 0.8571 | 0.9429 | 0.1818 | 0.6415 | |
| XSampEn | 0.7826 | 0.8718 | 0.9714 | 0.1818 | 0.5156 | |
| Severe CHD–CPNCA | XSampEn | 0.6383 | 0.7536 | 0.7429 | 0.3333 | 0.5667 |
| XFuzzyEn | 0.6596 | 0.7714 | 0.7714 | 0.3333 | 0.5845 | |
| MSCF | 0.6808 | 0.7945 | 0.8286 | 0.2500 | 0.5976 | |
| CPSD | 0.7021 | 0.8108 | 0.8571 | 0.2500 | 0.4476 | |
| MI | 0.7021 | 0.8000 | 0.8571 | 0.1667 | 0.6619 | |
| JDistEn | 0.7021 | 0.8158 | 0.8857 | 0.1667 | 0.4238 | |
| Mild-to-moderate CHD–CPNCA | MI | 0.5000 | 0.5714 | 0.6667 | 0.3333 | 0.5000 |
| XFuzzyEn | 0.5833 | 0.6154 | 0.6667 | 0.5000 | 0.5417 | |
| XSampEn | 0.6667 | 0.6364 | 0.5833 | 0.7500 | 0.7049 | |
| CPSD | 0.7083 | 0.6667 | 0.5833 | 0.8333 | 0.7638 | |
| MSCF | 0.7083 | 0.6957 | 0.6667 | 0.7500 | 0.7743 | |
| JDistEn | 0.7083 | 0.7200 | 0.7500 | 0.6667 | 0.7222 |
| Groups | Methods | Accuracy | F1-Score | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|---|
| Severe CHD– mild-to-moderate CHD | MI–CPSD–MSCF | 0.7826 | 0.8650 | 0.9143 | 0.3636 | 0.6182 |
| XSampEn–XFuzzyEn–JDistEn | 0.8043 | 0.8831 | 0.9714 | 0.2727 | 0.6078 | |
| Severe CHD–CPNCA | MI–CPSD–MSCF | 0.7447 | 0.8333 | 0.8571 | 0.4167 | 0.6500 |
| XSampEn–XFuzzyEn–JDistEn | 0.7659 | 0.8571 | 0.9428 | 0.2500 | 0.5047 | |
| Mild-to-moderate CHD–CPNCA | MI–CPSD–MSCF | 0.6667 | 0.6923 | 0.7500 | 0.5833 | 0.5694 |
| XSampEn–XFuzzyEn–JDistEn | 0.7500 | 0.7000 | 0.5833 | 0.8299 | 0.8290 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Wang, X.; Liu, C.; Li, Y.; Liu, Y.; Jiao, Y.; Liu, T.; Dong, H.; Wang, J. Discrimination of Patients with Varying Degrees of Coronary Artery Stenosis by ECG and PCG Signals Based on Entropy. Entropy 2021, 23, 823. https://0-doi-org.brum.beds.ac.uk/10.3390/e23070823
Zhang H, Wang X, Liu C, Li Y, Liu Y, Jiao Y, Liu T, Dong H, Wang J. Discrimination of Patients with Varying Degrees of Coronary Artery Stenosis by ECG and PCG Signals Based on Entropy. Entropy. 2021; 23(7):823. https://0-doi-org.brum.beds.ac.uk/10.3390/e23070823
Chicago/Turabian StyleZhang, Huan, Xinpei Wang, Changchun Liu, Yuanyang Li, Yuanyuan Liu, Yu Jiao, Tongtong Liu, Huiwen Dong, and Jikuo Wang. 2021. "Discrimination of Patients with Varying Degrees of Coronary Artery Stenosis by ECG and PCG Signals Based on Entropy" Entropy 23, no. 7: 823. https://0-doi-org.brum.beds.ac.uk/10.3390/e23070823