
Studying Physiological Synchrony in Couple Therapy through Partial Directed Coherence: Associations with the Therapeutic Alliance and Meaning Construction

 ,
,
Abstract
:1. Introduction
1.1. Interpersonal Physiological Synchrony
1.2. The therapeutic Alliance in Couple Therapy
2. Materials and Methods
2.1. The Case
2.2. Procedure
2.3. Measures
2.3.1. Autonomic Nervous System Responses
2.3.2. Clinical Outcomes in Routine Evaluation–Outcome Measure (CORE-OM)
2.3.3. Session Rating Scale (SRS)
2.3.4. System for Observing Family Therapy Alliances (SOFTA-o)
2.4. Data Analysis
Interpersonal Physiological Synchrony
2.5. Partial Directed Coherence within Sessions
2.6. Partial Directed Coherence between Sessions
2.7. Qualitative Analysis of the Therapy Process
2.7.1. Topical Episodes
2.7.2. Therapeutic Alliance
3. Findings and Discussion
3.1. Interpersonal Physiological Synchrony
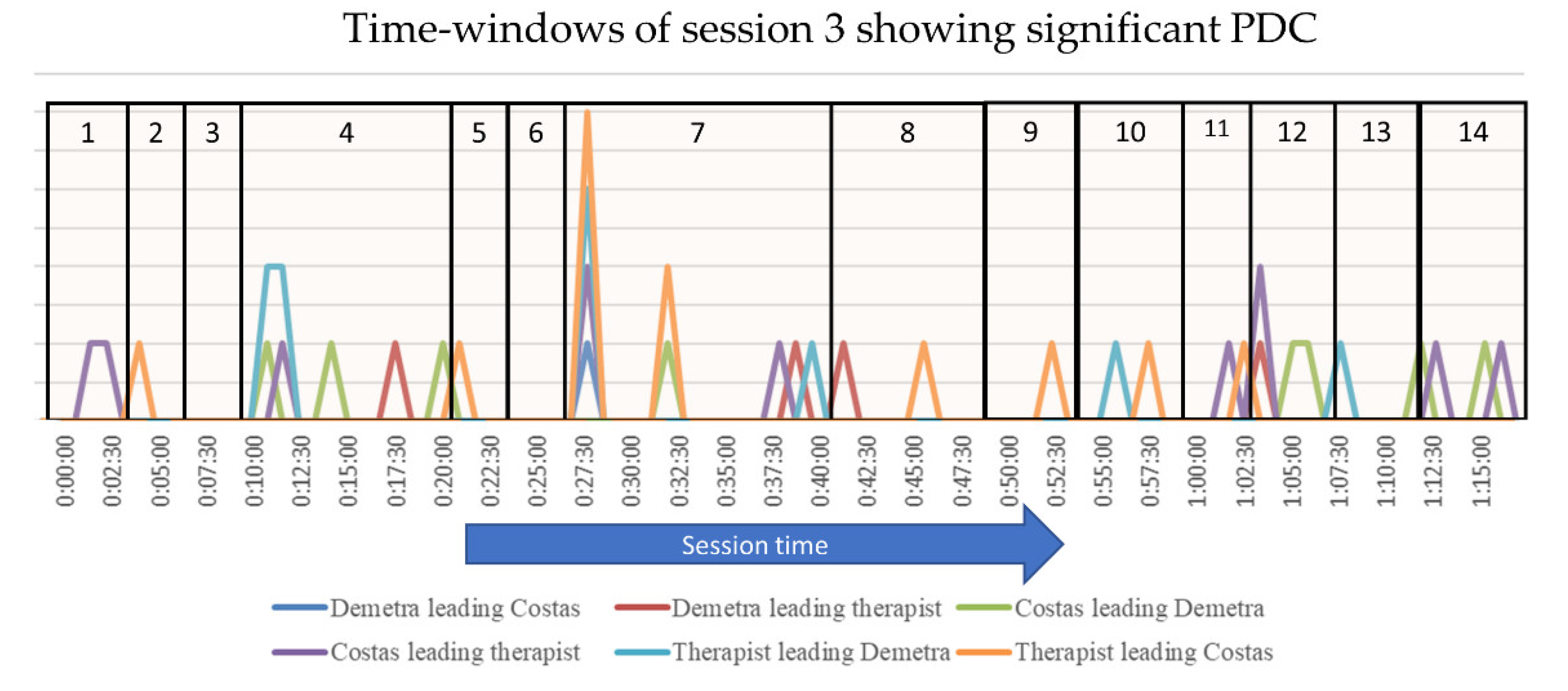
3.1.1. IPS in Session 3
3.1.2. IPS in Session 14
3.1.3. IPS between Sessions
3.2. Physiological Synchrony and Clinical Process
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stern, D.N.; Sander, L.W.; Nahum, J.P.; Harrison, A.M.; Lyons-Ruth, K.; Morgan, A.C.; Bruschweiler-Stern, N.; Tronick, E.Z. Non-interpretive mechanisms in psychoanalytic therapy. The ‘something more’ than interpretation. The Process of Change Study Group. Int. J. Psychoanal. 1998, 79, 903–921. [Google Scholar] [PubMed]
- Boston Change Process Study Group. Explicating the implicit: The local level and the microprocesses of change in the analytic situation. Int. J. Psychoanal. 2002, 83, 1051–1062. [Google Scholar] [CrossRef]
- Tschacher, W.; Meier, D. Physiological synchrony in psychotherapy sessions. Psychother. Res. 2020, 30, 558–573. [Google Scholar] [CrossRef] [PubMed]
- Bernieri, F.J.; Rosenthal, R. Interpersonal coordination: Behavior matching and interactional synchrony. In Fundamentals of Nonverbal Behavior; Rime, B., Feldman, R.S., Eds.; Cambridge University Press: Cambridge, UK, 1991; pp. 401–432. [Google Scholar]
- Chartrand, T.L.; van Baaren, R. Human mimicry. Adv. Exp. Soc. Psychol. 2009, 41, 219–274. [Google Scholar]
- Lakin, J.L.; Chartrand, T.L. Using nonconscious behavioral mimicry to create affiliation and rapport. Psychol. Sci. 2003, 14, 334–339. [Google Scholar] [CrossRef]
- Koole, S.L.; Tschacher, W. Synchrony in psychotherapy: A review and an integrative framework for the therapeutic alliance. Front. Psychol. 2016, 7, 862. [Google Scholar] [CrossRef] [Green Version]
- Raingruber, B.J. Three perspectives regarding what works and does not work in therapy: A comparison of judgments of clients, nurse-therapists, and uninvolved evaluators. J. Am. Psychiatr. Nurses Assoc. 2001, 7, 13–21. [Google Scholar] [CrossRef]
- Ramseyer, F.; Tschacher, W. Synchrony: A core concept for a constructivist approach to psychotherapy. Constr. Hum. Sci. 2006, 11, 150–171. [Google Scholar]
- Ramseyer, F.; Tschacher, W. Nonverbal synchrony in psychotherapy: Coordinated body movement reflects relationship quality and outcome. J. Consult. Clin. Psychol. 2011, 79, 284–295. [Google Scholar] [CrossRef] [Green Version]
- Wiltshire, T.J.; Philipsen, J.S.; Trasmundi, S.B.; Jensen, T.W.; Steffensen, S.V. Interpersonal coordination dynamics in psychotherapy: A systematic review. Cogn. Ther. Res. 2020, 44, 752–773. [Google Scholar] [CrossRef]
- Jaffe, J.; Beebe, B.; Feldstein, S.; Crown, C.L.; Jasnow, M.D.; Rochat, P.; Stern, D. Rhythms of dialogue in infancy: Coordinated timing in development. Monogr. Soc. Res. Child Dev. 2001, 66, i–viii, 1–132. [Google Scholar] [PubMed]
- Palmieri, A.; Kleinbub, J.R.; Calvo, V.; Benelli, E.; Messina, I.; Sambin, M.; Voci, A. Attachment-security prime effect on skin-conductance synchronization in psychotherapists: An empirical study. J. Couns. Psychol. 2018, 65, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Kleinbub, J.R.; Talia, A.; Palmieri, A. Physiological synchronization in the clinical process: A research primer. J. Couns. Psychol. 2020, 67, 420–437. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R. Child development parent—Infant synchrony: A biobehavioral model of mutual influences in the formation of affiliative bonds. Monogr. Soc. Res. Child Dev. 2005, 77, 42–51. [Google Scholar] [CrossRef]
- Ham, J.; Tronick, E. Relational psychophysiology: Lessons from mother-infant physiology research on dyadically expanded states of consciousness. Psychother. Res. 2009, 19, 619–632. [Google Scholar] [CrossRef]
- Beebe, B.; Lachmann, F.M. Infant Research and Adult Treatment; The Analytic Press: London, UK, 2002. [Google Scholar]
- Beebe, B.; Lachmann, F.M. The Origins of Attachment: Infant Research and Adult Treatment; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Butler, E.A.; Randall, A.K. Emotional coregulation in close relationships. Emot. Rev. 2013, 5, 202–210. [Google Scholar] [CrossRef]
- Timmons, A.C.; Margolin, G.; Saxbe, D.E. Physiological linkage in couples and its implications for individual and interpersonal functioning: A literature review. J. Fam. Psychol. 2015, 29, 720–731. [Google Scholar] [CrossRef]
- Cromby, J. Feeling the way: Qualitative clinical research and the affective turn. Qual. Res. Psychol. Spec. Issue Qual. Clin. Res. 2012, 9, 88–98. [Google Scholar] [CrossRef]
- Fuchs, T.; Koch, S.C. Embodied affectivity: On moving and being moved. Front. Psychol. 2014, 5, 508. [Google Scholar] [CrossRef] [Green Version]
- Avdi, E.; Evans, C. Exploring conversational and physiological aspects of psychotherapy talk. Front. Psychol. 2020, 11, 3001. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Berntson, G.G.; Andersen, B.L. Psychophysiological approaches to the evaluation of psychotherapeutic process and outcome, 1991: Contributions from social psychophysiology. Psychol. Assess. 1991, 3, 321–336. [Google Scholar] [CrossRef]
- Kreibig, S.D. Autonomic nervous system activity in emotion: A review. Biol. Psychol. 2010, 84, 394–421. [Google Scholar] [CrossRef] [PubMed]
- Soma, C.S.; Baucom, B.R.W.; Xiao, B.; Butner, J.E.; Hilpert, P.; Narayanan, S.; Atkins, D.C.; Imel, Z.E. Coregulation of therapist and client emotion during psychotherapy. Psychother. Res. 2020, 30, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A. A circumplex model of affect. J. Personal. Soc. Psychol. 1980, 39, 1161–1178. [Google Scholar] [CrossRef]
- Gennaro, A.; Carola, V.; Ottaviani, C.; Pesca, C.; Palmieri, A.; Salvatore, S. Affective saturation index: A lexical measure of affect. Entropy 2021, 23, 1421. [Google Scholar] [CrossRef]
- Deits-Lebehn, C.; Baucom, K.J.W.; Crenshaw, A.O.; Smith, T.W.; Baucom, B.R.W. Incorporating physiology into the study of psychotherapy process. J. Couns. Psychol. 2020, 67, 488–499. [Google Scholar] [CrossRef]
- Avdi, E.; Seikkula, J. Studying the process of psychoanalytic psychotherapy: Discursive and embodied aspects. Br. J. Psychother. 2019, 35, 217–232. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Friston, K.J. Functional and effective connectivity: A review. Brain Connect. 2011, 1, 13–36. [Google Scholar] [CrossRef]
- Mc Craty, R. New frontiers in heart rate variability and social coherence research: Techniques, technologies, and implications for improving group dynamics and outcomes. Front. Public Health 2017, 5, 267. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, R.V.; Marraccini, M.E.; Weyandt, L.L.; Wilder-Smith, O.; McGee, H.A.; Liu, S.; Goodwin, M.S. Interpersonal autonomic physiology: A systematic review of the literature. Personal. Soc. Psychol. Rev. 2017, 21, 99–141. [Google Scholar] [CrossRef] [PubMed]
- Dimascio, A.; Boyd, R.W.; Greenblatt, M. Physiological correlates of tension and antagonism during psychotherapy; a study of interpersonal physiology. Psychosom. Med. 1957, 19, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kykyri, V.-L.; Karvonen, A.; Wahlström, J.; Kaartinen, J.; Penttonen, M.; Seikkula, J. Soft prosody and embodied attunement in therapeutic interaction: A multimethod case study of a moment of change. J. Constr. Psychol. 2017, 30, 211–234. [Google Scholar] [CrossRef]
- Kodama, K.; Tanaka, S.; Shimizu, D.; Hori, K.; Matsui, H. Heart Rate Synchrony in Psychological Counseling: A Case Study. Psychology 2018, 9, 1858–1874. [Google Scholar] [CrossRef] [Green Version]
- Marci, C.D.; Orr, S.P. The effect of emotional distance on psychophysiologic concordance and perceived empathy between patient and interviewer. Appl. Psychophysiol. Biofeedback 2006, 31, 115–128. [Google Scholar] [CrossRef]
- Seikkula, J.; Karvonen, A.; Kykyri, V.L.; Penttonen, M.; Nyman-Salonen, P. The relational mind in couple therapy: A bateson-inspired view of human life as an embodied stream. Fam. Process 2018, 57, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Villmann, T.; Liebers, C.; Bergmann, B.; Gumz, A.; Geyer, M. Investigation of psycho-physiological interactions between patient and therapist during a psychodynamic therapy and their relation to speech using in terms of entropy analysis using a neural network approach. New Ideas Psychol. 2008, 26, 309–325. [Google Scholar] [CrossRef]
- Messina, I.; Palmieri, A.; Sambin, M.; Kleinbub, J.R.; Voci, A.; Calvo, V. Somatic underpinnings of perceived empathy: The importance of psychotherapy training. Psychother. Res. 2013, 23, 169–177. [Google Scholar] [CrossRef]
- Gennaro, A.; Kleinbub, J.R.; Mannarini, S.; Salvatore, S.; Palmieri, A. Training in psychotherapy: A call for embodied and psychophysiological approaches. Res. Psychother. Psychopathol. Process Outcome 2019, 22, 395. [Google Scholar] [CrossRef]
- Palmieri, A.; Pick, E.; Grossman-Giron, A.; Tzur Bitan, D. Oxytocin as the neurobiological basis of synchronization: A research proposal in psychotherapy settings. Front. Psychol. 2021, 12, 628011. [Google Scholar] [CrossRef]
- Levenson, R.W.; Ruef, A.M. Empathy: A physiological substrate. J. Personal. Soc. Psychol. 1992, 63, 234–246. [Google Scholar] [CrossRef]
- Creaven, A.M.; Skowron, E.A.; Hughes, B.M.; Howard, S.; Loken, E. Dyadic concordance in mother and preschooler resting cardiovascular function varies by risk status. Dev. Psychobiol. 2014, 56, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dale, R.; Fusaroli, R.; Duran, N.D.; Richardson, D.C. The Self-Organization of human interaction. Psychol. Learn. Motiv. 2013, 59, 43–95. [Google Scholar] [CrossRef] [Green Version]
- Reed, R.G.; Barnard, K.; Butler, E.A. Distinguishing emotional coregulation from codysregulation: An investigation of emotional dynamics and body weight in romantic couples. Emotion 2015, 15, 45–60. [Google Scholar] [CrossRef]
- Peräkylä, A.; Henttonen, P.; Voutilainen, L.; Kahri, M.; Stevanovic, M.; Sams, M.; Ravaja, N. Sharing the emotional load: Recipient affiliation calms down the storyteller. Soc. Psychol. Q. 2015, 78, 301–323. [Google Scholar] [CrossRef]
- Voutilainen, L.; Henttonen, P.; Kahri, M.; Ravaja, N.; Sams, M.; Peräkylä, A. Empathy, challenge, and psychophysiological activation in therapist–client interaction. Front. Psychol. 2018, 9, 530. [Google Scholar] [CrossRef]
- Baccalá, L.A.; Sameshima, K. Partial directed coherence: A new concept in neural structure determination. Biol. Cybern. 2001, 84, 463–474. [Google Scholar] [CrossRef]
- Safran, J.D.; Muran, J.C. Negotiating the Therapeutic Alliance: A Relational Treatment Guide; Guilford Press: New York, NY, USA, 2000. [Google Scholar]
- Tronick, E.Z. Emotions and emotional communication in infants. Am. Psychol. 1989, 44, 112–119. [Google Scholar] [CrossRef]
- Tronick, E.Z.; Bruschweiler-Stern, N.; Harrison, A.M.; Lyons-Ruth, K.; Morgan, A.C.; Nahum, J.P.; Sander, L.; Stern, D.N. Dyadically expanded states of consciousness and the process of therapeutic change. Infant Ment. Health J. 1998, 19, 290–299. [Google Scholar] [CrossRef]
- Kleinbub, J.R. State of the art of interpersonal physiology in psychotherapy: A systematic review. Front. Psychol. 2017, 8, 2053. [Google Scholar] [CrossRef] [Green Version]
- Laitila, A.; Vall, B.; Penttonen, M.; Karvonen, A.; Kykyri, V.L.; Tsatsishvili, V.; Kaartinen, J.; Seikkula, J. The added value of studying embodied responses in couple therapy research: A case study. Fam. Process 2019, 58, 685–697. [Google Scholar] [CrossRef] [PubMed]
- Mylona, A.; Avdi, E. Alliance ruptures and embodied arousal in psychodynamic psychotherapy: An exploratory study. Hell. J. Psychol. 2021, 18, 226–248. [Google Scholar] [CrossRef]
- Tschacher, W.; Haken, H. Causation and chance: Detection of deterministic and stochastic ingredients in psychotherapy processes. Psychother. Res. 2020, 30, 1075–1087. [Google Scholar] [CrossRef] [PubMed]
- Smoliak, O.; Strong, T. Therapy as Discourse: Practice and Research; Springer International Publishing: London, UK, 2018; ISBN 978-3-319-93066-4. [Google Scholar]
- Avdi, E.; Georgaca, E. Discourse analysis and psychotherapy: A critical review. Eur. J. Psychother. Couns. 2007, 9, 157–176. [Google Scholar] [CrossRef]
- Avdi, E.; Georgaca, E. Researching the discursive construction of subjectivity. In Therapy as Discourse: Practice and Research; Smoliak, O., Strong, T., Eds.; Palgrave: London, UK, 2018; pp. 45–70. [Google Scholar]
- Norcross, J.C.; Lambert, M.J. Psychotherapy Relationships That Work: Evidence-Based Therapist Contributions; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Bordin, E.S. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy 1979, 16, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Horvath, A.O.; Bedi, R.P. The alliance. In Psychotherapy Relationships that Work: Therapist Contributions and Responsiveness to Patients; Norcross, J.C., Ed.; Oxford University Press: Oxford, UK, 2002; pp. 37–69. [Google Scholar]
- Larner, G. Towards a common ground in psychoanalysis and family therapy: On knowing not to know. J. Fam. Ther. 2000, 22, 61–82. [Google Scholar] [CrossRef]
- Anderson, H. Postmodern collaborative and person-centred therapies: What would Carl Rogers say? J. Fam. Ther. 2001, 23, 339–360. [Google Scholar] [CrossRef]
- Friedlander, M.L.; Escudero, V.; Heatherington, L.; Diamond, G.M. Alliance in couple and family therapy. Psychotherapy 2011, 48, 25–33. [Google Scholar] [CrossRef]
- Kuhlman, I.; Tolvanen, A.; Seikkula, J. The therapeutic alliance in couple therapy for depression: Predicting therapy progress and outcome from assessments of the alliance by the patient, the spouse, and the therapists. Contemp. Fam. Ther. 2013, 35, 1–13. [Google Scholar] [CrossRef]
- Speed, B. All aboard in the NHS: Collaborating with colleagues who use different approaches. J. Fam. Ther. 2004, 26, 260–279. [Google Scholar] [CrossRef]
- Tilden, T.; Johnson, S.U.; Hoffart, A.; Zahl-Olsen, R.; Wampold, B.E.; Ulvenes, P.; Håland, Å.T. Alliance predicting progress in couple therapy. Psychotherapy 2021, 58, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Glebova, T.; Bartle-Haring, S.; Gangamma, R.; Knerr, M.; Delaney, R.O.; Meyer, K.; McDowell, T.; Adkins, K.; Grafsky, E. Therapeutic alliance and progress in couple therapy: Multiple perspectives. J. Fam. Ther. 2011, 33, 42–65. [Google Scholar] [CrossRef]
- Halford, T.C.; Owen, J.; Duncan, B.L.; Anker, M.G.; Sparks, J.A. Pre-therapy relationship adjustment, gender and the alliance in couple therapy. J. Fam. Ther. 2016, 38, 18–35. [Google Scholar] [CrossRef]
- Seikkula, J.; Karvonen, A.; Kykyri, V.-L.; Kaartinen, J.; Penttonen, M. The embodied attunement of therapists and a couple within dialogical psychotherapy: An introduction to the relational mind research project. Fam. Process 2015, 54, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T. The Reflecting Team: Dialogues and Dialogues about the Dialogues; Norton: New York, NY, USA, 1991. [Google Scholar]
- Kagan, N.; Krathwohl, D.R.; Miller, R. Stimulated recall in therapy using video tape: A case study. J. Couns. Psychol. 1963, 10, 237–243. [Google Scholar] [CrossRef]
- Larsen, D.; Flesaker, K.; Stege, R. Qualitative interviewing using interpersonal process recall: Investigating internal experiences during professional-client conversations. Int. J. Qual. Methods 2008, 7, 18–37. [Google Scholar] [CrossRef] [Green Version]
- Firstbeat Technologies, Oy. Available online: https://www.firstbeat.com/en/ (accessed on 28 March 2022).
- Evans, C.; Connell, J.; Barkham, M.; Margison, F.; McGrath, G.; Mellor-Clark, J.; Audin, K. Towards a standardised brief outcome measure: Psychometric properties and utility of the CORE-OM. Br. J. Psychiatry 2002, 180, 51–60. [Google Scholar] [CrossRef]
- Miller, S.D.; Duncan, B.L.; Brown, J.; Sparks, J.; Claud, D. The outcome rating scale: A preliminary study of the reliability, validity, and feasibility of a brief visual analog measure. J. Br. Ther. 2003, 2, 91–100. [Google Scholar]
- Friedlander, M.L.; Escudero, V.; Horvath, A.O.; Heatherington, L.; Cabero, A.; Martens, M.P. System for observing family therapy alliances: A tool for research and practice. J. Couns. Psychol. 2006, 53, 214–225. [Google Scholar] [CrossRef]
- Kettunen, J.; Saalasti, S. Procedure for Detection of Stress by Segmentation and Analyzing A Heart Beat Signal. US Patent 7,330,752, 12 February 2008. [Google Scholar]
- Leite, A.; Silva, M.E.; Rocha, A.P. Modeling volatility in heat rate variability. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3582–3585. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Nollo, G. Assessing frequency domain causality in cardiovascular time series with instantaneous interactions. Methods Inf. Med. 2010, 49, 453–457. [Google Scholar] [CrossRef]
- Seikkula, J.; Laitila, A.; Rober, P. Making sense of multi—Actor dialogues in family therapy and network meetings. J. Marital Fam. Ther. 2012, 38, 667–687. [Google Scholar] [CrossRef] [PubMed]
- Codrons, E.; Bernardi, N.F.; Vandoni, M.; Bernardi, L. Spontaneous group synchronization of movements and respiratory rhythms. PLoS ONE 2014, 9, e107538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Päivinen, H.; Holma, J.; Karvonen, A.; Kykyri, V.L.; Tsatsishvili, V.; Kaartinen, J.; Penttonen, M.; Seikkula, J. Affective arousal during blaming in couple therapy: Combining analyses of verbal discourse and physiological responses in two case studies. Contemp. Fam. Ther. 2016, 38, 373–384. [Google Scholar] [CrossRef]
- Tourunen, A.; Kykyri, V.-L.; Seikkula, J.; Kaartinen, J.; Tolvanen, A.; Penttonen, M. Sympathetic nervous system synchrony: An exploratory study of its relationship with the therapeutic alliance and outcome in couple therapy. Psychotherapy 2020, 57, 160–173. [Google Scholar] [CrossRef]
- Haken, H.; Portugali, J. Information and selforganization: A unifying approach and applications. Entropy 2016, 18, 197. [Google Scholar] [CrossRef] [Green Version]
- Orsucci, F. Human synchronization maps—The hybrid consciousness of the embodied mind. Entropy 2021, 23, 1569. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CORE-OM | CORE-OM RISK | SRS | ||||
|---|---|---|---|---|---|---|
| Session 1 | Session 15 | Session 1 | Session 15 | Session 3 | Session 14 | |
| Demetra | 12 | 10 | 0 | 1.6 | 5.6 | 8.0 |
| Costas | 19 | 11 | 5 | 0 | 8.9 | 9.8 |
| Leading Role | ||||
|---|---|---|---|---|
| Demetra | Costas | Therapist | ||
| Pacing role | Demetra | 8 | 6 | |
| Costas | 1 | 8 | ||
| Therapist | 4 | 9 | ||
| Leading Role | ||||
|---|---|---|---|---|
| Demetra | Costas | Therapist | ||
| Pacing role | Demetra | 1 | 4 | |
| Costas | 4 | 1 | ||
| Therapist | 1 | 2 | ||
| TE | SOFTA Scores | Time-Windows with PDC | % Episode Time in PDC | ||||
|---|---|---|---|---|---|---|---|
| Costas | Demetra | Therapist | SSP | Composite Score | |||
| 1 | 2 | 1 | 0 | 0 | 3 | 2 | 47.6 |
| 2 | 1 | 1 | 2 | 0 | 4 | 1 | 26.3 |
| 3 | −1 | 0 | 1 | 2 | 3-1 | 0 | 0 |
| 4 | 1 | 2 | 1 | 2 | 6 | 5 | 39 |
| 5 | 0 | 0 | 0 | 1 | 1 | 1 | 15.4 |
| 6 | 1 | 0 | 0 | 0 | 1 | 0 | 0 |
| 7 | −1 | 2 | 2 | 0 | 4-1 | 5 | 28 |
| 8 | 0 | 1 | 1 | 2 | 4 | 2 | 19.2 |
| 9 | 1 | 0 | 1 | 2 | 4 | 1 | 17.9 |
| 10 | 0 | 1 | 1 | 1 | 3 | 2 | 28.6 |
| 11 | 0 | 0 | 0 | 1 | 1 | 1 | 31.2 |
| 12 | 0 | 1 | 1 | 0 | 2 | 5 | 66 |
| 13 | 1 | 2 | 1 | 2 | 6 | 1 | 34.5 |
| 14 | 1 | 0 | 1 | 1 | 3 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avdi, E.; Paraskevopoulos, E.; Lagogianni, C.; Kartsidis, P.; Plaskasovitis, F. Studying Physiological Synchrony in Couple Therapy through Partial Directed Coherence: Associations with the Therapeutic Alliance and Meaning Construction. Entropy 2022, 24, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/e24040517
Avdi E, Paraskevopoulos E, Lagogianni C, Kartsidis P, Plaskasovitis F. Studying Physiological Synchrony in Couple Therapy through Partial Directed Coherence: Associations with the Therapeutic Alliance and Meaning Construction. Entropy. 2022; 24(4):517. https://0-doi-org.brum.beds.ac.uk/10.3390/e24040517
Chicago/Turabian StyleAvdi, Evrinomy, Evangelos Paraskevopoulos, Christina Lagogianni, Panagiotis Kartsidis, and Fotis Plaskasovitis. 2022. "Studying Physiological Synchrony in Couple Therapy through Partial Directed Coherence: Associations with the Therapeutic Alliance and Meaning Construction" Entropy 24, no. 4: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/e24040517