

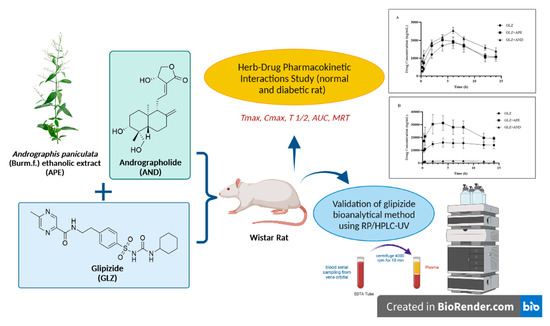
Pharmacokinetic Herb-Drug Interactions of Glipizide with Andrographis paniculata (Burm. f.) and Andrographolide in Normal and Diabetic Rats by Validated HPLC Method

 ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. HPLC Condition
2.3. Preparation of Standard Stock and Working Solutions
2.4. Preparation of Spiked Plasma
2.5. System Suitability Test (SST)
2.6. Method Validation
2.6.1. Selectivity and Carryover
2.6.2. Calibration Curve and LLOQ
2.6.3. Accuracy and Precision
2.6.4. Dilution Integrity
2.6.5. Stability
2.7. Experimental Design for In Vivo Studies
2.7.1. Animals Used in the Study
2.7.2. Sample Preparation
2.7.3. Pharmacokinetic Interaction Study in Normal and Diabetic Rats
2.8. Data Analysis
3. Results
3.1. SST
3.2. Validation Method
3.2.1. Selectivity
3.2.2. Calibration Curve and LLOQ
3.2.3. Accuracy and Precision
3.2.4. Dilution Integrity
3.2.5. Stability
3.3. Study of Pharmacokinetic Interaction in Normal and Diabetic Rats
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and Alternative Medicine Use Among Adults and Children: United States, 2007. Natl. Health Stat. Rep. 2008, 12, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Fjær, E.L.; Landet, E.R.; McNamara, C.L.; Eikemo, T.A. The use of complementary and alternative medicine (CAM) in Europe. BMC Complement. Med. Ther. 2020, 20, 108. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Hu, H.; Harnett, J.; Zheng, X.; Liang, Z.; Wang, Y.-T.; Ung, C.O.L. An evaluation of randomized controlled trials on nutraceuticals containing traditional Chinese medicines for diabetes management: A systematic review. Chin. Med. 2019, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- Manya, K.; Champion, B.; Dunning, T. The use of complementary and alternative medicine among people living with diabetes in Sydney. BMC Complement. Altern. Med. 2012, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.-Y.; Wallis, M.; Tiralongo, E. Use of complementary and alternative medicine among people living with diabetes: Literature review. J. Adv. Nurs. 2007, 58, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Phutrakool, P.; Pongpirul, K. Acceptance and use of complementary and alternative medicine among medical specialists: A 15-year systematic review and data synthesis. Syst. Rev. 2022, 11, 10. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Bo, L.; Baosheng, Z.; Yang, L.; Mingmin, T.; Beiran, L.; Zhiqiang, L.; Huaqiang, Z. Herb-drug enzyme-mediated interactions and the associated experimental methods: A review. J. Tradit. Chin. Med. 2016, 36, 392–408. [Google Scholar] [CrossRef] [Green Version]
- Babos, M.; Heinan, M.; Redmond, L.; Moiz, F.; Souza-Peres, J.; Samuels, V.; Masimukku, T.; Hamilton, D.; Khalid, M.; Herscu, P. Herb–Drug Interactions: Worlds Intersect with the Patient at the Center. Medicines 2021, 8, 44. [Google Scholar] [CrossRef]
- Brantley, S.J.; Argikar, A.A.; Lin, Y.S.; Nagar, S.; Paine, M.F. Herb–Drug Interactions: Challenges and Opportunities for Improved Predictions. Drug Metab. Dispos. 2014, 42, 301–317. [Google Scholar] [CrossRef]
- Fasinu, P.S.; Bouic, P.J.; Rosenkranz, B. An Overview of the Evidence and Mechanisms of Herb–Drug Interactions. Front. Pharmacol. 2012, 3, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tornio, A.; Niemi, M.; Neuvonen, P.J.; Backman, J.T. Drug interactions with oral antidiabetic agents: Pharmacokinetic mechanisms and clinical implications. Trends Pharmacol. Sci. 2012, 33, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.K.; Rettie, A.E.; Fowler, D.M.; Miners, J.O. Pharmacogenomics of CYP2C9: Functional and Clinical Considerations. J. Pers Med. 2017, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Booven, D.; Marsh, S.; McLeod, H.; Whirl-Carrillo, M.; Sangkuhl, K.; Klein, T.E.; Altman, R.B. Cytochrome P450 2C9-CYP2C9. Pharm. Genom. 2010, 20, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Desta, Z.; Zhao, X.; Shin, J.G.; Flockhart, D.A. Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin. Pharmacokinet. 2002, 41, 913–958. [Google Scholar] [CrossRef] [PubMed]
- Holstein, A.; Beil, W. Oral antidiabetic drug metabolism: Pharmacogenomics and drug interactions. Expert Opin. Drug Metab. Toxicol. 2009, 5, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Tirkkonen, T.; Heikkilä, P.; Huupponen, R.; Laine, K. Potential CYP2C9-mediated drug–drug interactions in hospitalized type 2 diabetes mellitus patients treated with the sulphonylureas glibenclamide, glimepiride or glipizide. J. Intern. Med. 2010, 268, 359–366. [Google Scholar] [CrossRef]
- Tan, B.; Zhang, Y.F.; Chen, X.Y.; Zhao, X.H.; Li, G.X.; Zhong, D.F. The effects of CYP2C9 and CYP2C19 genetic polymorphisms on the pharmacokinetics and pharmacodynamics of glipizide in Chinese subjects. Eur. J. Clin. Pharmacol. 2010, 66, 145–151. [Google Scholar] [CrossRef]
- Arifullah, M.; Namsa, N.D.; Mandal, M.; Chiruvella, K.K.; Vikrama, P.; Gopal, G.R. Evaluation of anti–bacterial and anti–oxidant potential of andrographolide and echiodinin isolated from callus culture of Andrographis paniculata Nees. Asian Pac. J. Trop. Biomed. 2013, 3, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.; Chen, S.R.; Chai, L.; Zhao, J.; Wang, Y.; Wang, Y. Overview of pharmacological activities of Andrographis paniculata and its major compound andrographolide. Crit. Rev. Food Sci. Nutr. 2019, 59 (Suppl. S1), S17–S29. [Google Scholar] [CrossRef]
- Edwin, E.-S.; Vasantha-Srinivasan, P.; Senthil-Nathan, S.; Thanigaivel, A.; Ponsankar, A.; Pradeepa, V.; Selin-Rani, S.; Kalaivani, K.; Hunter, W.B.; Abdel-Megeed, A.; et al. Anti-dengue efficacy of bioactive andrographolide from Andrographis paniculata (Lamiales: Acanthaceae) against the primary dengue vector Aedes aegypti (Diptera: Culicidae). Acta Trop. 2016, 163, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Fitrawan, L.; Ariastuti, R.; Tjandrawinata, R.R.; Nugroho, A.E.; Pramono, S. Antidiabetic effect of combination of fractionated-extracts of Andrographis paniculata and Centella asiatica: In vitro study. Asian Pac. J. Trop. Biomed. 2018, 8, 527. [Google Scholar] [CrossRef]
- Sundhani, E.; Nugroho, A.E.; Nurrochmad, A.; Lukitaningsih, E. Molecular interactions of Andrographis paniculata Burm. f. Active Compound with Nuclear Receptor (CAR and PXR): An In Silico Assessment Approach. Indones J. Chem. 2022, 22, 126. [Google Scholar] [CrossRef]
- Pan, Y.; Abd-Rashid, B.A.; Ismail, Z.; Ismail, R.; Mak, J.W.; Pook, P.C.K.; Er, H.M.; Ong, C.E. In vitro determination of the effect of Andrographis paniculata extracts and andrographolide on human hepatic cytochrome P450 activities. J. Nat. Med. 2011, 65, 440–447. [Google Scholar] [CrossRef]
- Pekthong, D.; Blanchard, N.; Abadie, C.; Bonet, A.; Heyd, B.; Mantion, G.; Berthelot, A.; Richert, L.; Martin, H. Effects of Andrographis paniculata extract and Andrographolide on hepatic cytochrome P450 mRNA expression and monooxygenase activities after in vivo administration to rats and in vitro in rat and human hepatocyte cultures. Chem. Biol. Interact. 2009, 179, 247–255. [Google Scholar] [CrossRef]
- Pekthong, D.; Martin, H.; Abadie, C.; Bonet, A.; Heyd, B.; Mantion, G.; Richert, L. Differential inhibition of rat and human hepatic cytochrome P450 by Andrographis paniculata extract and andrographolide. J. Ethnopharmacol. 2008, 115, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Qiu, F.; Hou, X.L.; Takahashi, K.; Chen, L.X.; Azuma, J.; Kang, N. Andrographolide inhibits the expression and metabolic activity of cytochrome P450 3A4 in the modified Caco-2 cells. J. Ethnopharmacol. 2012, 141, 709–713. [Google Scholar] [CrossRef]
- Balap, A.; Lohidasan, S.; Sinnathambi, A.; Mahadik, K. Pharmacokinetic and Pharmacodynamic Interaction of Andrographolide and Standardized Extract of Andrographis paniculata (Nees) with Nabumetone in Wistar Rats. Phytother. Res. PTR 2017, 31, 75–80. [Google Scholar] [CrossRef]
- Balap, A.; Lohidasan, S.; Sinnathambi, A.; Mahadik, K. Herb-drug interaction of Andrographis paniculata (Nees) extract and andrographolide on pharmacokinetic and pharmacodynamic of naproxen in rats. J. Ethnopharmacol. 2017, 195, 214–221. [Google Scholar] [CrossRef]
- Balap, A.; Atre, B.; Lohidasan, S.; Sinnathambi, A.; Mahadik, K. Pharmacokinetic and pharmacodynamic herb–drug interaction of Andrographis paniculata (Nees) extract and andrographolide with etoricoxib after oral administration in rats. J. Ethnopharmacol. 2016, 183, 9–17. [Google Scholar] [CrossRef]
- Chien, C.F.; Wu, Y.T.; Lee, W.C.; Lin, L.C.; Tsai, T.H. Herb–drug interaction of Andrographis paniculata extract and andrographolide on the pharmacokinetics of theophylline in rats. Chem. Biol. Interact. 2010, 184, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Mouid, M.G. Effect of Ethanolic Extract of Aerial Parts of Andrographis paniculata on the Pharmacokinetics of Gliclazide in Rats. Asian J. Biomed. Pharm. Sci. 2015, 5, 21–24. [Google Scholar] [CrossRef]
- Wongnawa, M.; Soontaro, P.; Riditid, W.; Wongpoowarak, P.; Ruengkittisaku, S. The effects of Andrographis paniculata (Burm. f.) Nees on the pharmacokinetics and pharmacodynamics of midazolam in healthy volunteers. Songklanakarin J. Sci. Technol. 2012, 34, 533–539. [Google Scholar]
- Vaishali, V.G.; Patel, J.; Varia, R.; Bhavsar, S.; Priti, P.V.; Falguni, F.M.; Tamanna, T.S. Effect of Andrographolide Co-Administration on Pharmacokinetics of Meloxicam in Rats. Int. J. Curr. Microbiol. Appl. Sci. 2017, 6, 2147–2153. [Google Scholar] [CrossRef]
- Li, X.P.; Zhang, C.L.; Gao, P.; Gao, J.; Liu, D. Effects of andrographolide on the pharmacokinetics of aminophylline and doxofylline in rats. Drug Res. 2013, 63, 258–262. [Google Scholar] [CrossRef]
- Samala, S.; Veeresham, C. Pharmacokinetic and Pharmacodynamic Interaction of Boswellic Acids and Andrographolide with Glyburide in Diabetic Rats: Including Its PK/PD Modeling: PK/PD Interactions with Glyburide. Phytother. Res. 2016, 30, 496–502. [Google Scholar] [CrossRef]
- Samala, S.; Veeresham, C. Andrographolide Pretreatment Enhances the Bioavailability and Hypoglycemic Action of Glimepiride and Metformin. Int. J. Phytomedicine. 2015, 7, 254–264. [Google Scholar]
- Zhang, X.; Zhang, X.; Wang, X.; Zhao, M. Influence of andrographolide on the pharmacokinetics of warfarin in rats. Pharm. Biol. 2018, 56, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Kirthi, A.; Shanmugam, R.; Prathyusha, M.S.; Basha, D.J. A Review on Bioanalytical Method Development and Validation by RP-HPLC. J. Glob. Trends Pharm. Sci. 2014, 5, 2265–2271. [Google Scholar]
- Anusha, A.; Narendar, D.; Krishna Murthy, B.; Goverdhan, P. Influence of Single and Multi Dose Treatment of Glipizide on Pharmacokinetics and Pharmacodynamics of Irbesartan in Normal and Hypertensive Rats. High Blood Press Cardiovasc. Prev. Off J. Ital. Soc. Hypertens. 2017, 24, 179–185. [Google Scholar] [CrossRef]
- Chaudhari, S.; Zambad, S.; Ali, M. Effect of Aqueous Extract of Azadirachta indica Leaves on Pharmacokineics and Pharmacodynamics of Glipizide. Drug Metab. Lett. 2019, 13, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Nikolin, B.; Imamović, B.; Medanhodzić-Vuk, S.; Sober, M. High perfomance liquid chromatography in pharmaceutical analyses. Bosn. J. Basic Med. Sci. 2004, 4, 5–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezazadeh, M.; Emami, J. A simple and sensitive HPLC method for analysis of imipramine in human plasma with UV detection and liquid-liquid extraction: Application in bioequivalence studies. Res. Pharm. Sci. 2016, 11, 168–176. [Google Scholar] [PubMed]
- Deshpande, M.M.; Kasture, V.S.; Mohan, M.; Chavan, M.M.A.M.J. Bioanalytical Method Development and Validation: A Review; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Sebaiy, M.M.; Abdellatef, H.E.; Elmosallamy, M.A.; Alshuwaili, M.K. Identification of Antioxidative Ingredients from Feverfew (Tanacetum Parthenium) Extract Substantially free of Parthenolide and other Alpha-Unsaturated Gamma-Lactones. Open J. Anal. Bioanal. Chem. 2020, 4, 001–006. [Google Scholar] [CrossRef]
- Atif, M.; Khalid, S.H.; Onn Kit, G.L.; Sulaiman, S.A.S.; Asif, M.; Chandersekaran, A. Development and validation of RP-HPLC-UV method for the determination of Glipizide in human plasma. J. Young Pharm. JYP 2013, 5, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Thippani, R.; Pothuraju, N.R.; Ramisetti, N.R.; Shaik, S. Optimization and validation of a fast RP–HPLC method for the determination of dobutamine in rat plasma: Pharmacokinetic studies in healthy rat subjects. J. Pharm. Anal. 2013, 3, 434–439. [Google Scholar] [CrossRef]
- Gedawy, A.; Al-Salami, H.; Dass, C.R. Advanced and multifaceted stability profiling of the first-line antidiabetic drugs metformin, gliclazide and glipizide under various controlled stress conditions. Saudi Pharm. J. 2020, 28, 362–368. [Google Scholar] [CrossRef]
- Gupta, S.; Bansal, G. Validated Stability-Indicating HPLC-UV Method for Simultaneous Determination of Glipizide and Four Impurities. J. AOAC Int. 2011, 94, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Jarrar, Y.B.; Al-Essa, L.; Kilani, A.; Hasan, M.; Al-Qerem, W. Alterations in the gene expression of drug and arachidonic acid-metabolizing Cyp450 in the livers of controlled and uncontrolled insulin-dependent diabetic mice. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Neyshaburinezhad, N.; Rouini, M.; Shirzad, N.; Esteghamati, A.; Nakhjavani, M.; Namazi, S.; Ardakani, Y.H. Evaluating the effect of type 2 diabetes mellitus on CYP450 enzymes and P-gp activities, before and after glycemic control: A protocol for a case–control pharmacokinetic study. MethodsX 2020, 7, 100853. [Google Scholar] [CrossRef]
- Palatini, P.; De Martin, S. Pharmacokinetic drug interactions in liver disease: An update. World J. Gastroenterol. 2016, 22, 1260–1278. [Google Scholar] [CrossRef] [PubMed]
- Dostalek, M.; Akhlaghi, F.; Puzanovova, M. Effect of diabetes mellitus on pharmacokinetic and pharmacodynamic properties of drugs. Clin. Pharmacokinet. 2012, 51, 481–499. [Google Scholar] [CrossRef] [PubMed]
- Furman, B.L. Streptozotocin-Induced Diabetic Models in Mice and Rats. Curr. Protoc. Pharmacol. 2015, 70, 5–47. [Google Scholar] [CrossRef]
- Price, G.; Patel, D.A. Drug Bioavailability; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Nugroho, A.E.; Rais, I.R.; Setiawan, I.; Pratiwi, P.Y.; Hadibarata, T.; Tegar, M.; Pramono, S. Pancreatic effect of andrographolide isolated from Andrographis paniculata (Burm. f.) Nees. Pak. J. Biol. Sci. PJBS 2014, 17, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Nugroho, A.E.; Lindawati, N.Y.; Herlyanti, K.; Widyastuti, L.; Pramono, S. Anti-diabetic effect of a combination of andrographolide-enriched extract of Andrographis paniculata (Burm. f.) Nees and asiaticoside-enriched extract of Centella asiatica L. in high fructose-fat fed rats. Indian J. Exp. Biol. 2013, 51, 1101–1108. [Google Scholar] [PubMed]
- Sundhani, E.; Lukitaningsih, E.; Nurrochmad, A.; Nugroho, A.E. Potential pharmacokinetic and pharmacodynamic herb-drug interactions of Andrographis paniculata (Burm. f.) and andrographolide: A systematic review. J. Herbmed. Pharmacol. 2022, 11, 154–165. [Google Scholar] [CrossRef]
- Chen, H.-W.; Huang, C.-S.; Liu, P.-F.; Li, C.-C.; Chen, C.-T.; Liu, C.-T.; Chiang, J.-R.; Yao, H.-T.; Lii, C.-K. Andrographis paniculata Extract and Andrographolide Modulate the Hepatic Drug Metabolism System and Plasma Tolbutamide Concentrations in Rats. Evid. Based Complement. Altern. Med. 2013, 2013, 982689. [Google Scholar] [CrossRef] [Green Version]
- Niu, J.; Straubinger, R.M.; Mager, D.E. Pharmacodynamic Drug-Drug Interactions. Clin. Pharmacol. Ther. 2019, 105, 1395–1406. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Result | Acceptance Criteria |
|---|---|---|
| Retention time | 0.30 | RSD ≤ 2.0% |
| Area | 0.36 | RSD ≤ 2.0% |
| Tailing factor (asymmetry) | 1.23 | ≤2.0 |
| Number of theoretical plates | 11,336 | ≥2000 |
| Concentration (ng/mL) | % Error | % CV | ||||||
|---|---|---|---|---|---|---|---|---|
| Within (n = 6) | Between (n = 18) | Within (n = 6) | Between (n = 18) | |||||
| Day 1 | Day 2 | Day 3 | Day 1 | Day 2 | Day 3 | |||
| 25 | −2.89 | 0.54 | 10.64 | 2.76 | 10.82 | 5.69 | 3.89 | 7.36 |
| 75 | −1.53 | 3.95 | 8.84 | 3.75 | 6.43 | 5.08 | 3.84 | 5.12 |
| 700 | −1.65 | 9.56 | −4.17 | 1.25 | 5.55 | 3.92 | 3.82 | 4.43 |
| 1250 | 9.20 | 13.30 | 5.34 | 9.28 | 5.13 | 0.34 | 6.08 | 3.85 |
| Concentration (ng/mL) | Measured Concentration (ng/mL) (Mean ± SD) | % Recovery (±CV) |
|---|---|---|
| 25 | 25.69 ± 1.76 | 102.76 ± 0.07 |
| 75 | 77.81 ± 3.89 | 103.42 ± 0.05 |
| 700 | 708.72 ± 5.14 | 101.29 ± 0.07 |
| 1250 | 1366 ± 49.75 | 109.28 ± 0.04 |
| Dilution Factor | Mean ± SD Measurable Conc. (ng/mL) | Accuracy (% Error) | Precision (% CV) |
|---|---|---|---|
| 2× | 199.04 ± 10.94 | −0.48 | 5.50 |
| 5× | 423.20 ± 24.54 | 5.80 | 5.80 |
| 10× | 1054.29 ± 74.57 | 5.43 | 7.07 |
| Stability Study | Mean ± SD Measurable Conc. (ng/mL) | Accuracy (% Error) | Precision (% CV) | |
|---|---|---|---|---|
| Short-Term Stability | ||||
| T0 | Low QC 75 µ/mL High QC 1250 µ/mL | 81.10 ± 2.06 | 8.13 | 2.54 |
| 1239.79 ± 68.22 | −0.82 | 5.50 | ||
| T4 | 69.99 ± 1.61 | −6.68 | 2.30 | |
| 1285.25 ± 10.84 | 2.82 | 0.84 | ||
| T24 | 70.30 ± 2.90 | −6.27 | 4.12 | |
| 1311.63 ± 30.52 | 4.93 | 2.33 | ||
| Freeze–thaw stability | 78.65 ± 4.84 | 4.86 | 6.15 | |
| 1230.17 ± 112.55 | −1.59 | 9.15 | ||
| Autosampler | 76.37 ± 2.27 | 1.83 | 2.98 | |
| 1233.47 ± 71.06 | −1.32 | 5.76 | ||
| Parameters | Unit | Value (±SEM) | |||||
|---|---|---|---|---|---|---|---|
| Normal Rats | Diabetic Rats | ||||||
| GLZ | GLZ + APE | GLZ + AND | GLZ | GLZ + APE | GLZ + AND | ||
| T 1/2 | h | 11.7 ± 4.19 | 7.07 ± 0.49 | 6.8 ± 0.6 | 39.06 ± 12.4 | 13.5 ± 3.9 | 23.59 ± 8.3 |
| Tmax | h | 5.6 ± 0.7 | 4.4 ± 0.4 | 6 ± 0 | 5.2 ± 1.3 | 3.7 ± 1.2 | 6.4 ± 0.75 |
| Cmax | ng/mL | 2038.3 ± 359.4 | 2134 ± 233.2 | 2545.6 ± 165 | 17,049.6 ± 3407 | 44,634.7 ± 5.471 ** | 1876.4 ± 133.2 * |
| AUC0–t | ng/mL·h | 25,130.3 ± 5.228 | 28,231.4 ± 2978 | 35,893 ± 3048 | 204,126.9 ± 41,879 | 356,362.8 ± 37.946 * | 21,052.9 ± 1.292 ** |
| AUC0–∞ | ng/mL·h | 34.266 ± 3379 | 31,729.2 ± 3120 | 41,127.7 ± 4339 | 978,757.3 ± 279,871 | 734,414.7 ± 123.596 * | 71.719 ± 22.203 ** |
| AUMC0–∞ | ng/mL·h2 | 637,882.6 ± 162,429 | 378,090.9 ± 29,818 | 522,329 ± 89,356 | 74,019,560 ± 3,708,6791 | 17,673,567.5 ± 7,373,051 | 3,632,224 ± 2,286,205 |
| MRT0–∞ | h | 19.3 ± 6.1 | 12 ± 0.4 | 12.4 ± 0.89 | 57.8 ± 17.8 | 20.9 ± 5 | 35.8 ± 12.04 |
| Cl/F | (ng)/(ng/mL) | 2.662 ± 1.1381 | 1.713 ± 0.30 | 1.22 ± 0.09 | 0.3067 ± 0.059 | 0.1263 ± 0.02006 | 2.272 ± 0.179 |
| Vd/F | (ng)/(ng/mL)/h | 0.152 ± 0.0159 | 0.165 ± 0.02 | 0.13 ± 0.02 | 0.0075 ± 0.002 | 0.0076 ± 0.00118 | 0.094 ± 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sundhani, E.; Nugroho, A.E.; Nurrochmad, A.; Puspitasari, I.; Amalia Prihati, D.; Lukitaningsih, E. Pharmacokinetic Herb-Drug Interactions of Glipizide with Andrographis paniculata (Burm. f.) and Andrographolide in Normal and Diabetic Rats by Validated HPLC Method. Molecules 2022, 27, 6901. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27206901
Sundhani E, Nugroho AE, Nurrochmad A, Puspitasari I, Amalia Prihati D, Lukitaningsih E. Pharmacokinetic Herb-Drug Interactions of Glipizide with Andrographis paniculata (Burm. f.) and Andrographolide in Normal and Diabetic Rats by Validated HPLC Method. Molecules. 2022; 27(20):6901. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27206901
Chicago/Turabian StyleSundhani, Elza, Agung Endro Nugroho, Arief Nurrochmad, Ika Puspitasari, Dita Amalia Prihati, and Endang Lukitaningsih. 2022. "Pharmacokinetic Herb-Drug Interactions of Glipizide with Andrographis paniculata (Burm. f.) and Andrographolide in Normal and Diabetic Rats by Validated HPLC Method" Molecules 27, no. 20: 6901. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules27206901