Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis

 and
and 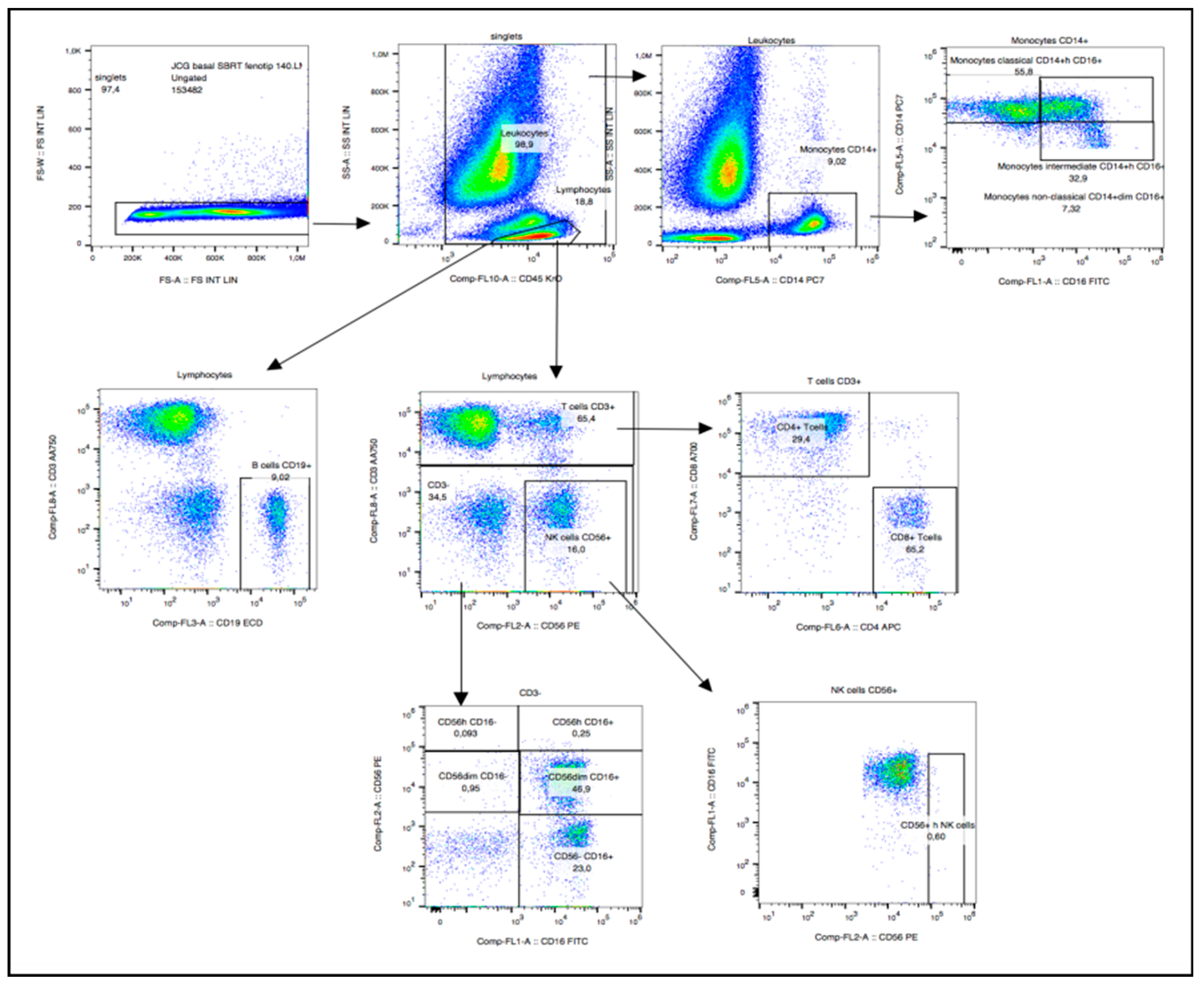{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of Patients
2.2. Immunophenotyping Panel
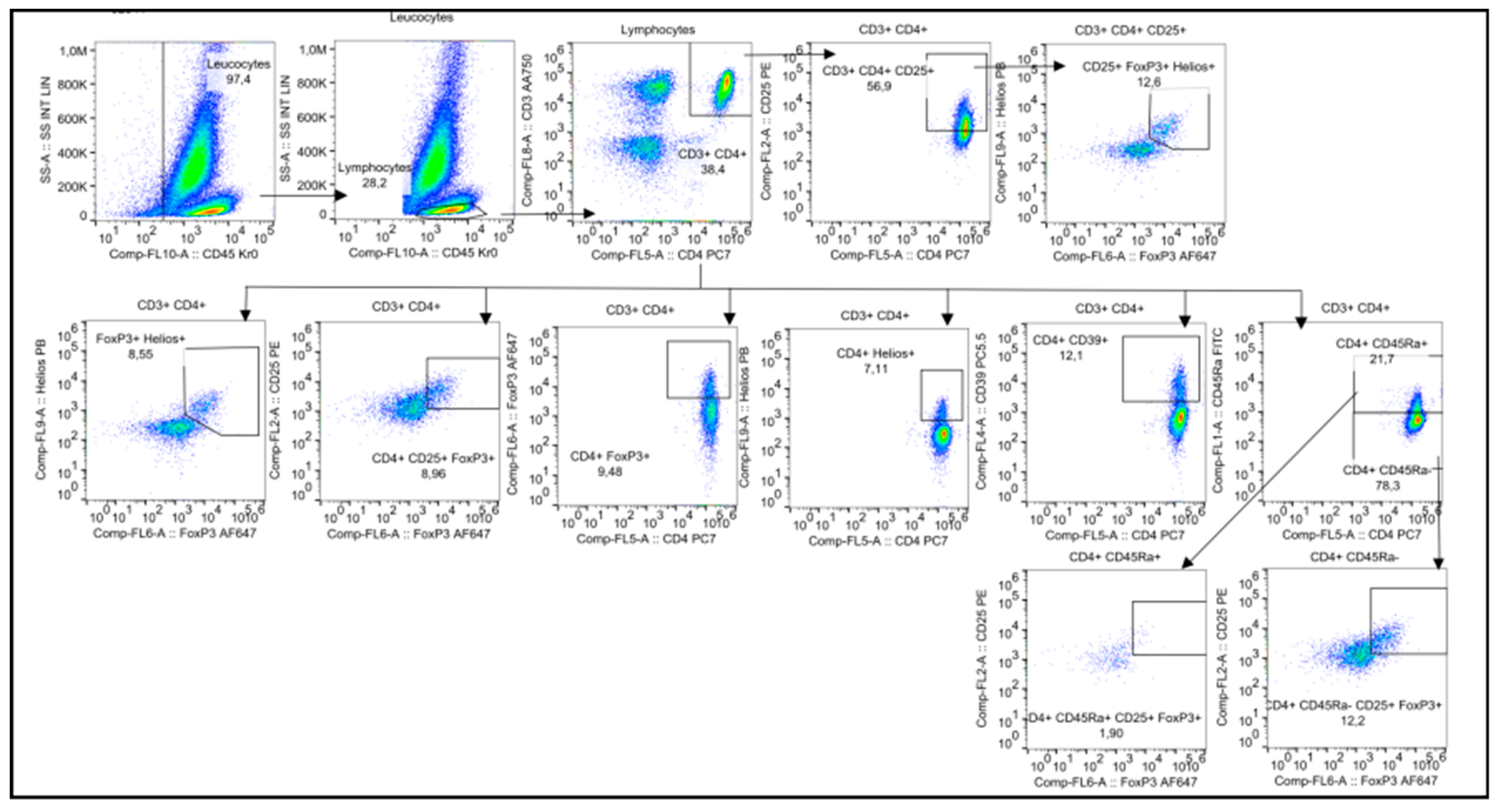
2.3. Regulatory T Cells (Treg cells)
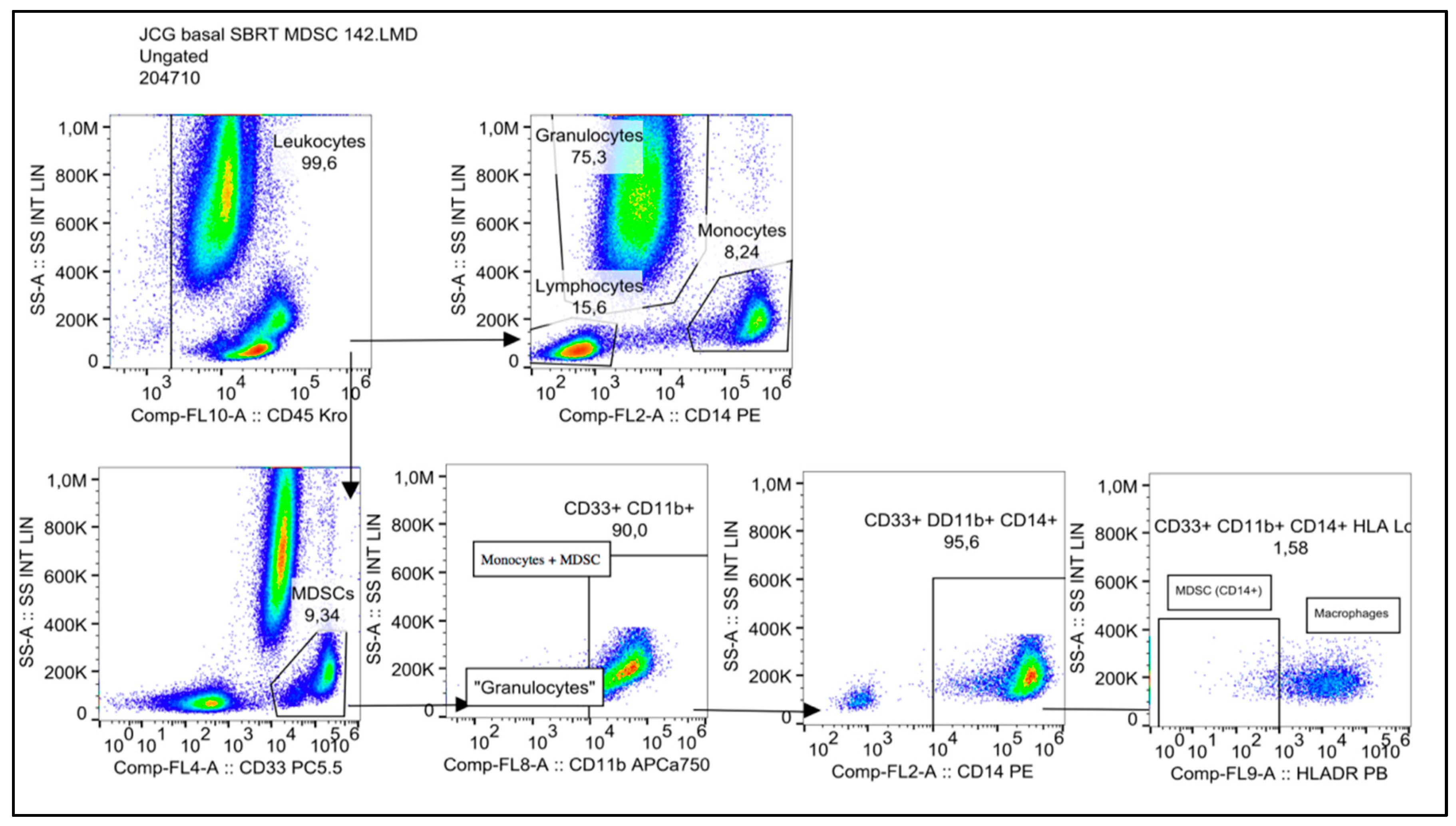
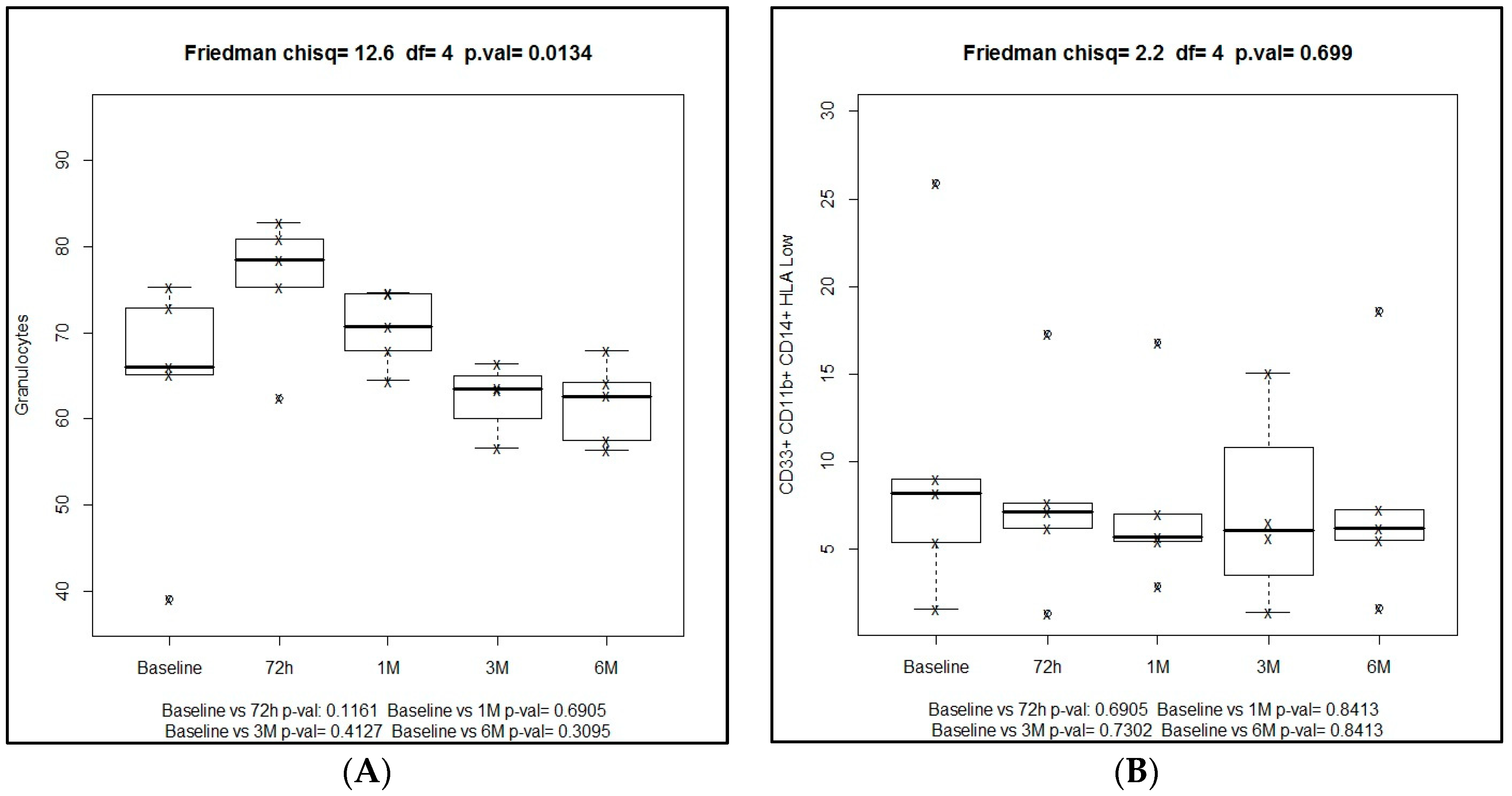
2.4. Myeloid-Derived Supressor Cells (MDSCs)
3. Discussion
Limitations of the Study
4. Materials and Methods
4.1. Design and Patients
4.2. Eligibility
4.3. SBRT Treatment
4.4. Blood Samples
4.5. Flow Cytometry
- -
- Lymphocyte Phenotyping DuraCloneTM, Beckman Coulter Life Sciences (Indianapolis, IN, USA): CD16 antibody (Ab), CD56 Ab, CD19 Ab, CD14 Ab, CD4 Ab, CD8 Ab, CD3 Ab, and CD45 Ab.
- -
- Regulatory T Cells DuraCloneTM, Beckman Coulter Life Sciences: CD45RA Ab, CD25 Ab, CD39 Ab, CD4 Ab, intracellular Foxp3 Ab, CD3 Ab, and CD45 Ab.
- -
- Myeloid-derived Suppressor Cells (MDSC) DuraCloneTM, Beckman Coulter Life Sciences: CD45, HLA-DR, CD14, CD33, and CD11b.
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SBRT | Stereotactive body radiotherapy |
| SABR | Stereotactic body radiotherapy |
| NSCLC | Non-small cell lung cancer |
| ANOVA | Analysis of variance |
| NK | Natural killer |
| MDSC | Myeloid-derived suppressor cells |
| G-MDSC | Granulocytic myeloid-derived suppressor cells |
| MHC | Major histocompatibility |
| Mo-MDSC | Monocytic myeloid-derived suppressor cells |
| TGF | Tumor growth factor |
| GM-CSF | Granulocyte-macrophage colony-stimulating factor |
| KPS | Karnofsky performance status |
| FEV1 | Forced expiratory volume in one second |
| DLCO | Diffusing capacity for carbon monoxide |
| PET | Positron-emission tomography |
| RECIST | Response Evaluation Criteria for Solid Tumors |
| PBMCs | Peripheral blood mononuclear cells |
References
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; on behalf of the ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv1–iv21. [Google Scholar]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.M.; McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet 2015, 16, 630–637. [Google Scholar] [CrossRef]
- Mole, R.H. Whole body irradiation-radiobiology or medicine. Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Demaria, S.; Ng, B.; Devitt, M.L.; Babb, J.S.; Kawashima, N.; Liebes, L.; Formenti, S.C. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Yang, G.; Pan, Z.; Zhao, Y.; Liang, X.; Li, W.; Cai, L. Hormetic response to low-dose radiation: Focus on the immune system and its clinical implications. Int. J. Mol. Sci. 2017, 18, 280. [Google Scholar] [CrossRef]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Golden, E.B.; Demaria, S.; Schiff, P.B.; Chachoua, A.; Formenti, S.C. An abscopal response to radiation and ipilimumab in a patient with metastatic non-small cell lung cancer. Cancer Immunol. Res. 2013, 1, 365–372. [Google Scholar] [CrossRef]
- Robin, H.I.; AuBuchon, J.; Varanasi, V.R.; Weinstein, A.B. The abscopal effect: Demonstration in lymphomatous involvement of kidneys. Med. Pediatr. Oncol. 1981, 9, 473–476. [Google Scholar] [CrossRef]
- Wersäll, P.J.; Blomgren, H.; Pisa, P.; Lax, I.; Kälkner, K.M.; Svedman, C. Regression of non-irradiated metastases after extracranial stereotactic radiotherapy in metastatic renal cell carcinoma. Acta Oncol. 2006, 45, 493–497. [Google Scholar] [CrossRef] [Green Version]
- Silva, S.; MacManus, M.P.; Martin, R.F.; Martin, O.A. Abscopal effects of radiation therapy: A clinical review for the radiobiologist. Cancer Lett. 2015, 356, 82–90. [Google Scholar]
- Finkelstein, S.E.; Timmerman, R.; McBride, W.H.; Schaue, D.; Hoffe, S.E.; Mantz, C.A.; Wilson, G.D. The confluence of stereotactic ablative radiotherapy and tumor immunology. Clin. Dev. Immunol. 2011, 2011, 439752. [Google Scholar] [CrossRef] [PubMed]
- Sharabi, A.B.; Lim, M.; DeWeese, T.; Drake, C.G. Radiation and checkpoint blockade immunotherapy radiosensitization and potential mechanisms for synergy. Lancet Oncol. 2015, 16, e498–e509. [Google Scholar] [CrossRef]
- Park, B.; Yee, C.; Lee, K.M. The effect of radiation on the immune response to cancers. Int. J. Mol. Sci. 2014, 15, 927–943. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Formenti, S.C. Role of T lymphocytes in tumor response to radiotherapy. Front. Oncol. 2012, 2, 95. [Google Scholar] [CrossRef]
- Venkatesulu, B.P.; Mallick, S.; Lin, S.H.; Krishnan, S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit. Rev. Oncol. Hematol. 2018, 123, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Burnette, B.; Weichselbaum, R.R. Radiation as an immune modulator. Semin. Radiat. Oncol. 2013, 23, 273–280. [Google Scholar] [CrossRef]
- Tang, C.; Liao, Z.; Gomez, D.; Levy, L.; Zhuang, Y.; Gebremichael, R.A.; Hong, D.S.; Komaki, R.; Welsh, J.W. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Schauer, D.; Ratikan, J.A.; Iwamoto, K.S.; McBride, W.H. Maximizing tumor immunity with fractionated radiation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1306–1310. [Google Scholar] [CrossRef]
- Vivier, E.; Ugolini, E.; Blaise, D.; Chabannon, C.; Brossay, L. Targeting natural killer cells and natural killer T cells in cancer. Nat. Rev. Immunol. 2012, 12, 239–252. [Google Scholar] [CrossRef] [Green Version]
- Childs, R.; Chernoff, A.; Contentin, N.; Bahceci, E.; Schrump, D.; Leitman, S.; Read, J.; Tisdale, J.; Dunbar, C.; Linehan, S.; et al. Regression of metastatic renal-cell carcinoma after nonmyeloablative allogenic peripheral-blood stem-cell transplantation. N. Engl. J. Med. 2000, 343, 750–758. [Google Scholar] [CrossRef]
- Iyengar, P.; Timmerman, R.D. Stereotactic ablative radiotherapy for non-small cell lung cancer: Rationale and outcomes. J. Natl. Compr. Cancer Netw. 2012, 10, 1514–1520. [Google Scholar] [CrossRef]
- Garnett, C.T.; Palena, C.; Chakarborty, M.; Tsang, K.Y.; Schlom, J.; Hodge, J.W. Sublethal irradiation of human tumor cells modulates phenotype resulting in enhanced killing by cytotoxic T lymphocytes. Cancer Res. 2014, 64, 7985–7994. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Miyara, M.; Yoshioka, Y.; Kitoh, A.; Shima, T.; Wing, K.; Niwa, A.; Parizot, P.; Taflin, C.; Heike, T.; Valeyre, D.; et al. Functional delineation and differentiation dynamics of human CD4+ T cells expressing the FoxP3 transcription factor. Immunity 2009, 30, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Ward-Hartstonge, K.A.; Kemp, R.A. Regulatory T-cell heterogeneity and the cancer immune response. Clin. Transl. Immunol. 2017, 6, e154. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Jayaraman, P.; Parikh, F.; Newton, J.M.; Hanoteau, A.; Rivas, C.; Krupar, R.; Rajapakshe, K.; Pathak, R.; Kanthaswamy, K.; McLaren, C.; et al. TGF-β1 programmed myeloid-derived suppressor cells (MDSC) acquire immune-stimulating and tumor killing activity capable of rejecting established tumors in combination with radiotherapy. Oncoimmunology 2018, 7, e1490853. [Google Scholar] [CrossRef]
- Carvajal, C.; Navarro-Martin, A.; Cacicedo, J.; Ramos, R.; Guedea, F. Stereotactic body radiotherapy for colorectal lung oligometastases: Preliminary single-institution results. J. BUON 2015, 20, 158–165. [Google Scholar]
- Vilalta, M.; Rafat, M.; Giaccia, A.J.; Graves, E.E. Recruitment of circulating breast cancer cells is stimulated by radiotherapy. Cell Rep. 2014, 8, 402–409. [Google Scholar] [CrossRef]
- Vilalta, M.; Brune, J.; Rafat, M.; Soto, L.; Graves, E.E. The role of granulocyte macrophage stimulating factor (GM-CSF) in radiation-induced tumor cell migration. Clin. Exp. Metastasis 2018, 35, 247–254. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumors: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Hedley, B.D.; Keeney, M.; Popma, J.; Chin-Yee, I. Novel lymphocyte screening tube using dried monoclonal antibody reagents. Cytom. Part B 2015, 88B, 361–370. [Google Scholar] [CrossRef] [PubMed]









© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Martín, A.; Galiana, I.L.; Berenguer Frances, M.A.; Cacicedo, J.; Cañas Cortés, R.; Comas Anton, S.; Padrones Sánchez, S.; Bolívar Cuevas, S.; Parry, R.; Guedea Edo, F. Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis. Int. J. Mol. Sci. 2018, 19, 3963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123963
Navarro-Martín A, Galiana IL, Berenguer Frances MA, Cacicedo J, Cañas Cortés R, Comas Anton S, Padrones Sánchez S, Bolívar Cuevas S, Parry R, Guedea Edo F. Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis. International Journal of Molecular Sciences. 2018; 19(12):3963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123963
Chicago/Turabian StyleNavarro-Martín, Arturo, Isabel Linares Galiana, Miguel A. Berenguer Frances, Jon Cacicedo, Rut Cañas Cortés, Silvia Comas Anton, Susana Padrones Sánchez, Santiago Bolívar Cuevas, Renate Parry, and Ferran Guedea Edo. 2018. "Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis" International Journal of Molecular Sciences 19, no. 12: 3963. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123963