Novel Nanoparticulate and Ionic Titanium Antigens for Hypersensitivity Testing


Abstract
:1. Introduction
2. Results
2.1. Endotoxin Levels
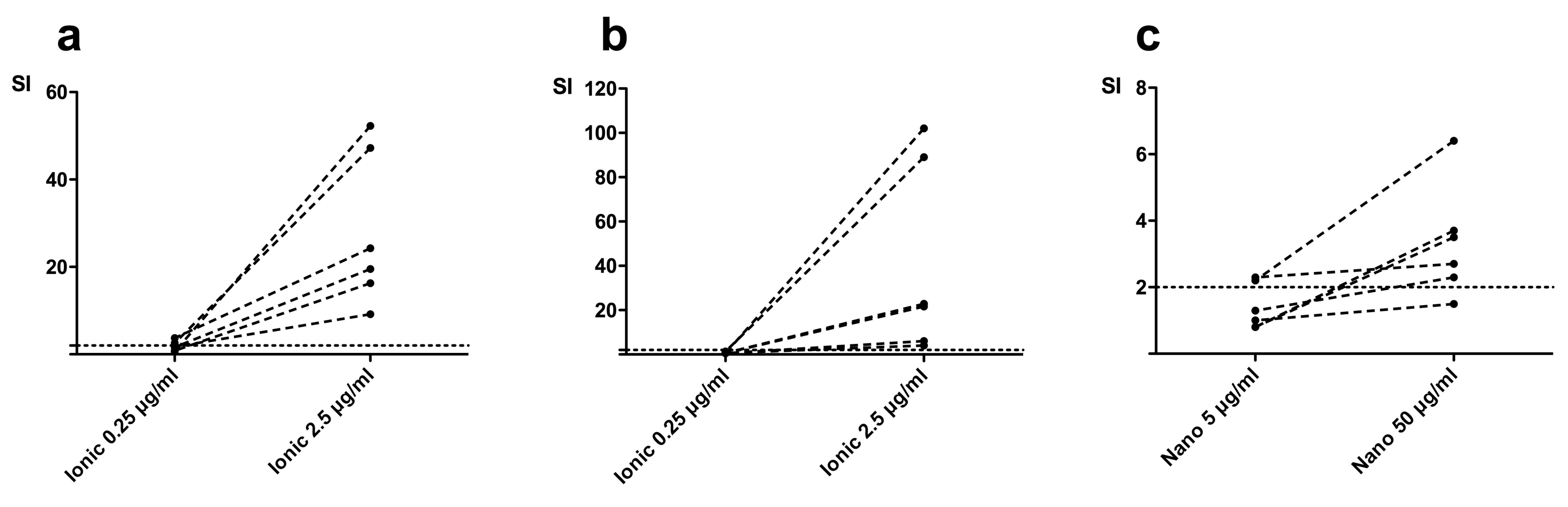
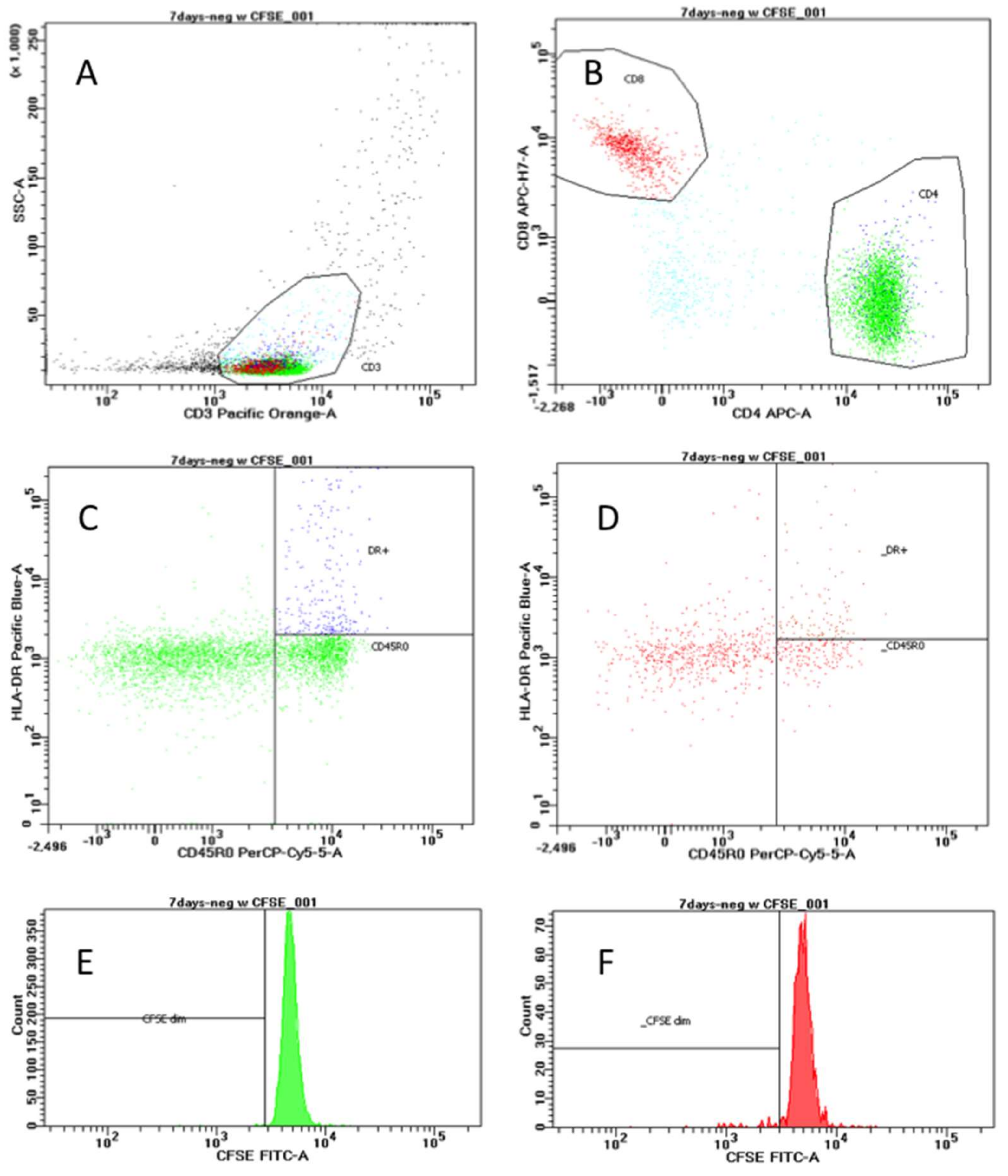
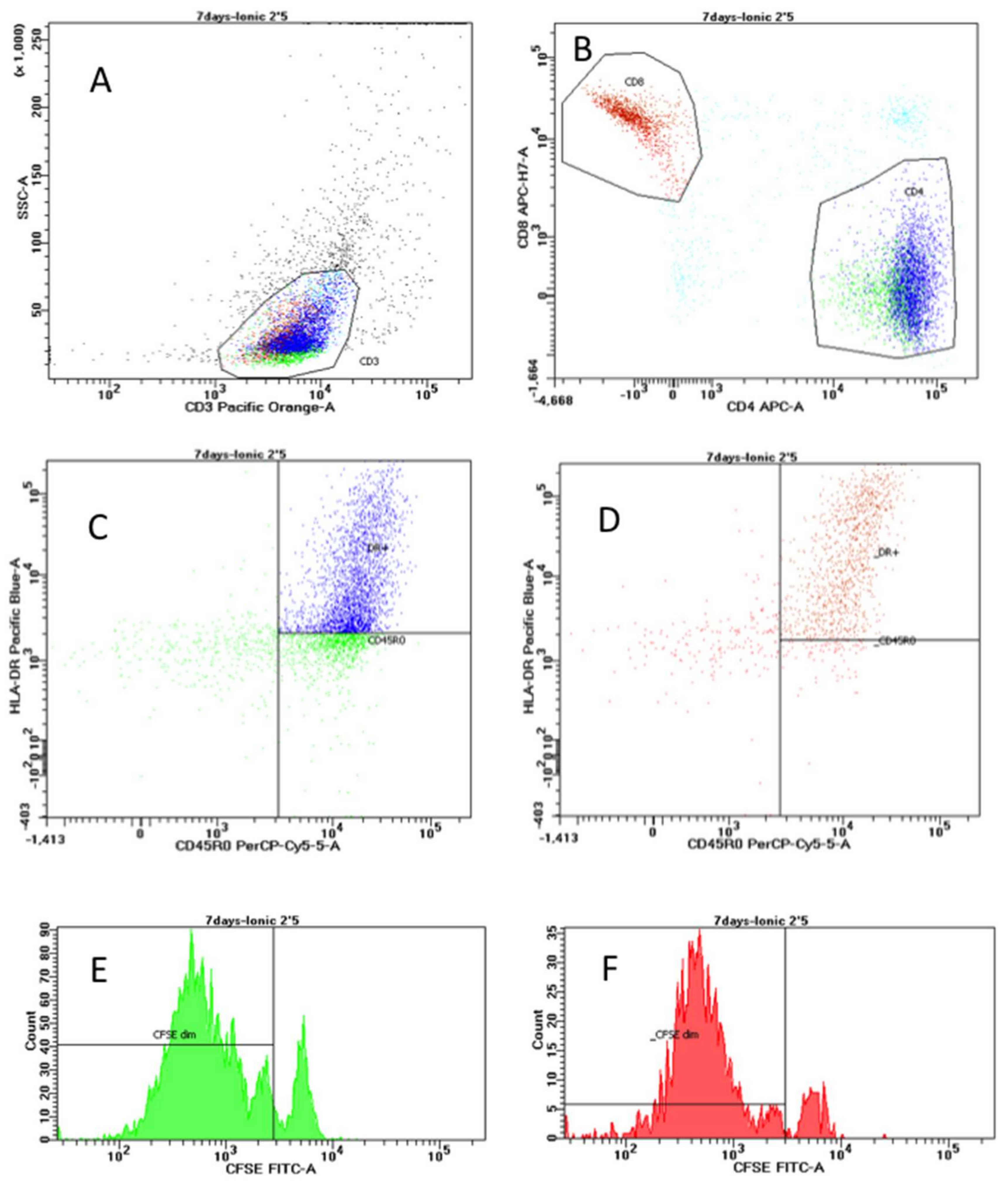
2.2. Lymphocyte Proliferation Responses to Titanium Antigens
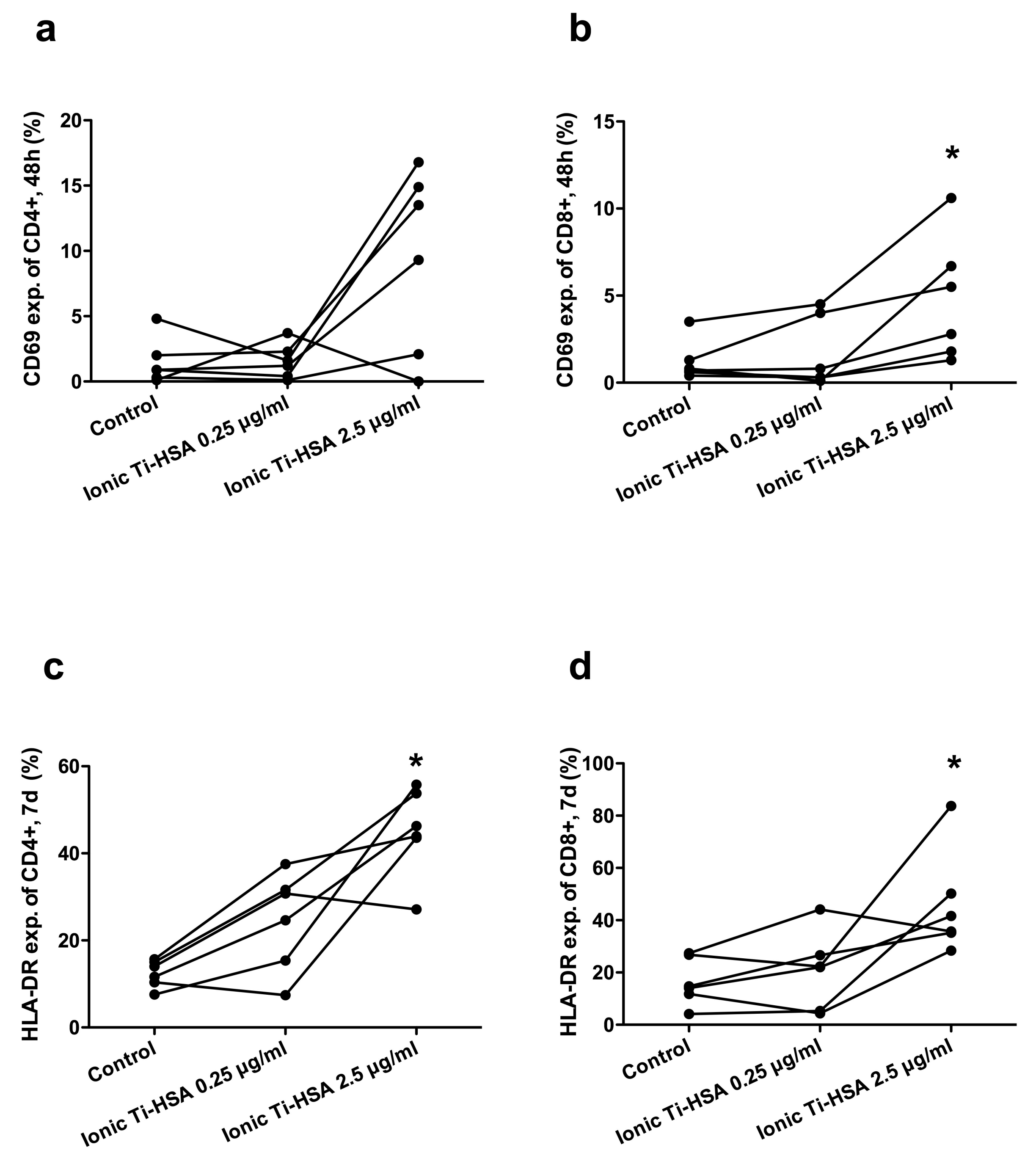
2.3. Activation Marker Expression
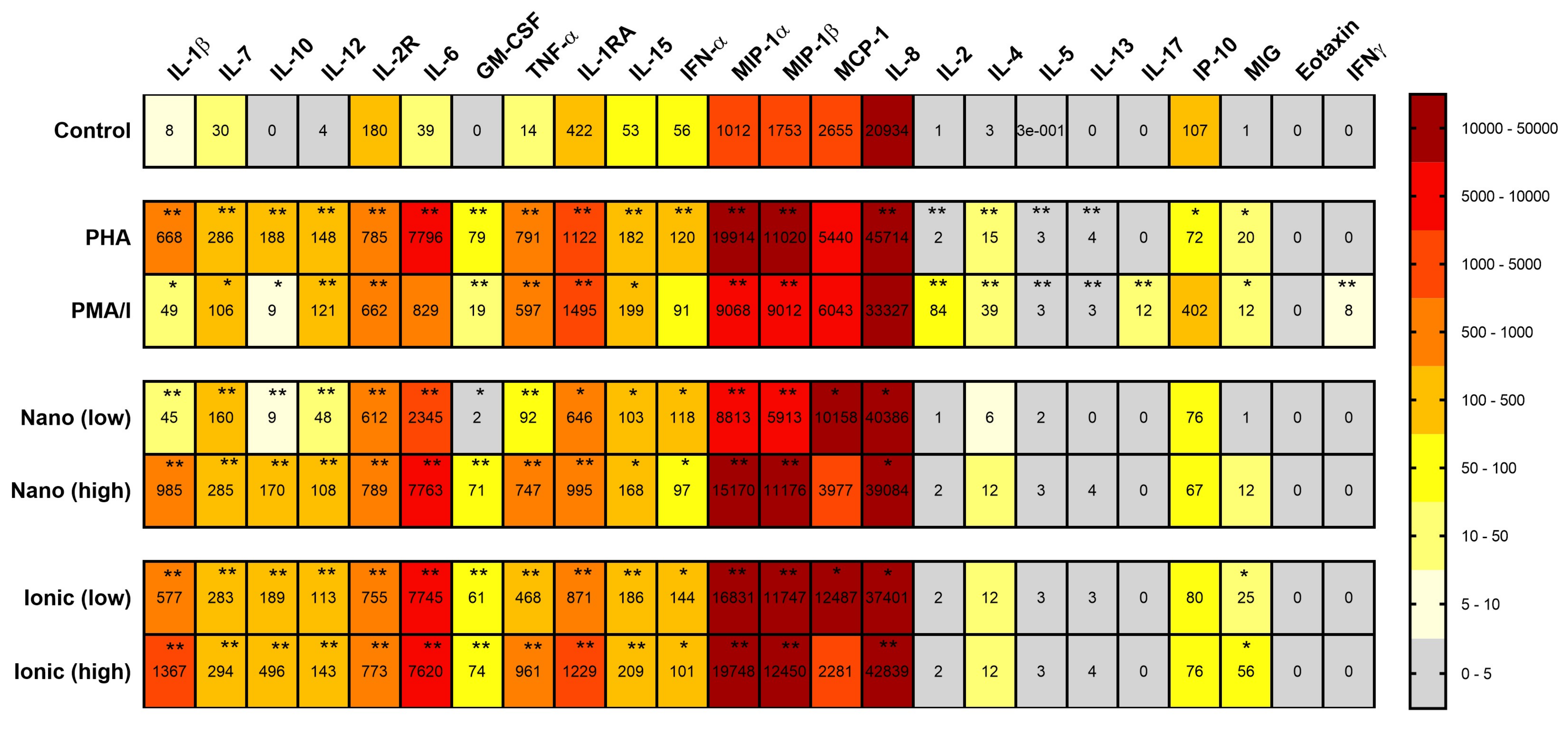
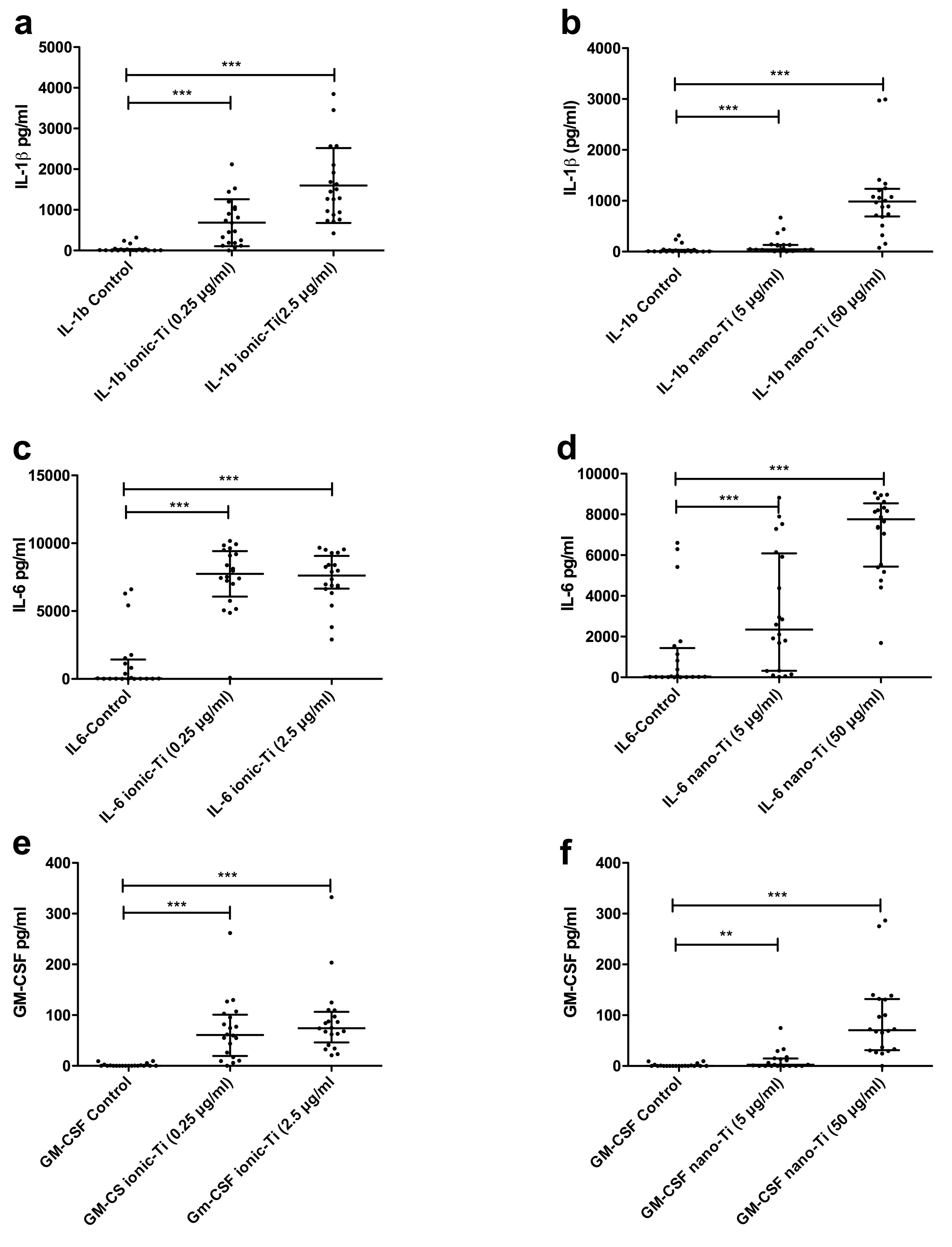
2.4. Cytokine Release in Response to Titanium Antigens
3. Discussion
3.1. Antigens
3.2. Flow Cytometry
3.3. Cytokines
3.4. Possible Mechanism
3.5. Limitations
4. Materials and Methods
4.1. Test Subjects
4.2. Ethics
4.3. Blood Sample Collection and Processing
4.4. Titanium Antigens Used for In Vitro Assays
4.4.1. Ionic Titanium(IV) Albumin Antigens (Ionic-Ti)
4.4.2. Nano-TiO2 Antigens
4.5. Endotoxin Testing
4.6. Flow Cytometry Analyses
4.7. Cytokine Analyses
4.8. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A


References
- NIOSH (National Institute for Occupational Safety and Health). Occupational Exposure to Titanium Dioxide; DHHS (NIOSH) Publication No. 2011–160; US Department of Health and Human Services, Public Health Service, Centers for Disease Control: Atlanta, GA, USA, 2011.
- Cuddy, M.F.; Poda, A.R.; Moser, R.D.; Weiss, C.A.; Cairns, C.; Steevens, J.A. A weight-of-evidence approach to identify nanomaterials in consumer products: A case study of nanoparticles in commercial sunscreens. J. Expo. Sci. Env. Epid. 2016, 26, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.F.; Du, L.J.; Song, Z.M.; Chen, X.X. Progress in the characterization and safety evaluation of engineered inorganic nanomaterials in food. Nanomedicine 2013, 8, 2007–2025. [Google Scholar] [CrossRef] [PubMed]
- Debia, M.; Bakhiyi, B.; Ostiguy, C.; Verbeek, J.H.; Brouwer, D.H.; Murashov, V. A Systematic Review of Reported Exposure to Engineered Nanomaterials. Ann. Occup. Hyg. 2016, 60, 916–935. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, H.; Beyer, M.; Fissan, H.; Asbach, C.; Kuhlbusch, T.A.J. Measurements of Nanoscale TiO2 and Al2O3 in Industrial Workplace Environments—Methodology and Results. Aerosol Air Qual. Res. 2015, 15, 129–141. [Google Scholar] [CrossRef]
- Warheit, D.B.; Sayes, C.M.; Reed, K.L.; Swain, K.A. Health effects related to nanoparticle exposures: Environmental, health and safety considerations for assessing hazards and risks. Pharmacol. Ther. 2008, 120, 35–42. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). IARC Monograph on the Evaluation of Carcinogenic Risks to Humans. Volume 93. Carbon Black, Titanium Dioxide, and Talc; World Health Organization: Lyon, France, 2010. [Google Scholar]
- Iavicoli, I.; Leso, V.; Bergamaschi, A. Toxicological Effects of Titanium Dioxide Nanoparticles: A Review of In Vivo Studies. J. Nanomater. 2012. [Google Scholar] [CrossRef]
- Sun, D.H.; Trindade, M.C.; Nakashima, Y.; Maloney, W.J.; Goodman, S.B.; Schurman, D.J.; Smith, R.L. Human serum opsonization of orthopedic biomaterial particles: Protein-binding and monocyte/macrophage activation in vitro. J. Biomed. Mater. Res. A 2003, 65, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Mahendra, G.; Pandit, H.; Kliskey, K.; Murray, D.; Gill, H.S.; Athanasou, N. Necrotic and inflammatory changes in metal-on-metal resurfacing hip arthroplasties. Acta Orthop. 2009, 80, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Muller, K.; Valentine-Thon, E. Hypersensitivity to titanium: Clinical and laboratory evidence. Neuro Endocrinol. Lett. 2006, 27, 31–35. [Google Scholar] [PubMed]
- Acero, J.; Calderon, J.; Salmeron, J.I.; Verdaguer, J.J.; Concejo, C.; Somacarrera, M.L. The behaviour of titanium as a biomaterial: Microscopy study of plates and surrounding tissues in facial osteosynthesis. J. Craniomaxillofac. Surg. 1999, 27, 117–123. [Google Scholar] [CrossRef]
- Grosse, S.; Haugland, H.K.; Lilleng, P.; Ellison, P.; Hallan, G.; Hol, P.J. Wear particles and ions from cemented and uncemented titanium-based hip prostheses—A histological and chemical analysis of retrieval material. J. Biomed. Mater. Res. B Appl. Biomater. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, N.; Naya, M.; Endoh, S.; Maru, J.; Yamamoto, K.; Nakanishi, J. Comparative pulmonary toxicity study of nano-TiO(2) particles of different sizes and agglomerations in rats: Different short- and long-term post-instillation results. Toxicology 2009, 264, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Willert, H.G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Koster, G.; Lohmann, C.H. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints—A clinical and histomorphological study. J. Bone Joint Surg. Am. Vol. 2005, 87A, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Takano, H.; Yanagisawa, R.; Ichinose, T.; Sakurai, M.; Yoshikawa, T. Effects of nano particles on cytokine expression in murine lung in the absence or presence of allergen. Arch. Toxicol. 2006, 80, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Messori, L.; Orioli, P.; Banholzer, V.; Pais, I.; Zatta, P. Formation of titanium(IV) transferrin by reaction of human serum apotransferrin with titanium complexes. FEBS Lett. 1999, 442, 157–161. [Google Scholar] [CrossRef]
- Silwood, C.J.; Grootveld, M. Chemical nature of implant-derived titanium(IV) ions in synovial fluid. Biochem. Biophys. Res. Commun. 2005, 330, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Tinoco, A.D.; Eames, E.V.; Valentine, A.M. Reconsideration of serum Ti(IV) transport: Albumin and transferrin trafficking of Ti(IV) and its complexes. J. Am. Chem. Soc. 2008, 130, 2262–2270. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Skipor, A.; Jacobs, J.J. Interfacial kinetics of titanium- and cobalt-based implant alloys in human serum: Metal release and biofilm formation. J. Biomed. Mater. Res. 2003, 65A, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Anderson, S.; Stafford, T.; Glant, T.; Jacobs, J.J. Lymphocyte responses in patients with total hip arthroplasty. J. Orthop. Res. 2005, 23, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.B. Citrate Binding of Al-3+ and Fe-3+. J. Inorg. Biochem. 1986, 28, 181–187. [Google Scholar] [CrossRef]
- Collins, J.M.; Uppal, R.; Incarvito, C.D.; Valentine, A.M. Titanium(IV) citrate speciation and structure under environmentally and biologically relevant conditions. Inorg. Chem. 2005, 44, 3431–3440. [Google Scholar] [CrossRef] [PubMed]
- Minang, J.T.; Arestrom, I.; Troye-Blomberg, M.; Lundeberg, L.; Ahlborg, N. Nickel, cobalt, chromium, palladium and gold induce a mixed Th1- and Th2-type cytokine response in vitro in subjects with contact allergy to the respective metals. Clin. Exp. Immunol. 2006, 146, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.B.; Davis, M.D.; Nakamura, K.; Hanson, L.; Richardson, D.M. Retrospective evaluation of patch testing before or after metal device implantation. Arch. Dermatol. 2008, 144, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Summer, B.; Paul, C.; Mazoochian, F.; Rau, C.; Thomsen, M.; Banke, I.; Gollwitzer, H.; Dietrich, K.A.; Mayer-Wagner, S.; Ruzicka, T.; Thomas, P. Nickel (Ni) allergic patients with complications to Ni containing joint replacement show preferential IL-17 type reactivity to Ni. Contact Dermat. 2010, 63, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Allouni, Z.E.; Cimpan, M.R.; Høl, P.J.; Skodvin, T.; Gjerdet, N.R. Agglomeration and sedimentation of TiO2 nanoparticles in cell culture medium. Colloids Surf. B Biointerfaces 2009, 68, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Vamanu, C.; Høl, P.; Allouni, Z.; Elsayed, S.; Gjerdet, N. Formation of potential antigens based on protein binding to titanium dioxide nanoparticles. Int. J. Nanomed. 2008, 3, 69–74. [Google Scholar] [CrossRef]
- Jacobs, J.J.; Hallab, N.J. Loosening and osteolysis associated with metal-on-metal bearings: A local effect of metal hypersensitivity? J. Bone Joint Surg. Am. 2006, 88, 1171–1172. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, E.; Pigatto, P.D.; Guzzi, G.; Altomare, G. Metal sensitivity in patients with orthopaedic implants: A prospective study. Contact Dermatitis 2011, 64, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Beeler, A.; Zaccaria, L.; Kawabata, T.; Gerber, B.O.; Pichler, W.J. CD69 upregulation on T cells as an in vitro marker for delayed-type drug hypersensitivity. Allergy 2008, 63, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, C.; Cumberbatch, M.; Dearman, R.J.; Daniel, R.J.; Kimber, I.; Groves, R.W. Functional caspase-1 is required for Langerhans cell migration and optimal contact sensitization in mice. J. Immunol. 2001, 166, 3672–3677. [Google Scholar] [CrossRef] [PubMed]
- Ashwood, P.; Thompson, R.P.; Powell, J.J. Fine particles that adsorb lipopolysaccharide via bridging calcium cations may mimic bacterial pathogenicity towards cells. Exp. Biol. Med. (Maywood) 2007, 232, 107–117. [Google Scholar] [PubMed]
- Caicedo, M.S.; Desai, R.; McAllister, K.; Reddy, A.; Jacobs, J.J.; Hallab, N.J. Soluble and particulate Co-Cr-Mo alloy implant metals activate the inflammasome danger signaling pathway in human macrophages: A novel mechanism for implant debris reactivity. J. Orthop. Res. 2009, 27, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Enk, A.H.; Katz, S.I. Early molecular events in the induction phase of contact sensitivity. Proc. Natl. Acad. Sci. USA 1992, 89, 1398–1402. [Google Scholar] [CrossRef] [PubMed]
- Trindade, M.C.; Lind, M.; Goodman, S.B.; Maloney, W.J.; Schurman, D.J.; Smith, R.L. Interferon-gamma exacerbates polymethylmethacrylate particle-induced interleukin-6 release by human monocyte/macrophages in vitro. J. Biomed. Mater. Res. 1999, 47, 1–7. [Google Scholar] [CrossRef]
- Nakashima, Y.; Sun, D.H.; Trindade, M.C.; Maloney, W.J.; Goodman, S.B.; Schurman, D.J.; Smith, R.L. Signaling pathways for tumor necrosis factor-alpha and interleukin-6 expression in human macrophages exposed to titanium-alloy particulate debris in vitro. J. Bone Joint Surg. Am. 1999, 81, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.F.; Esser, P.R.; Weber, F.C.; Jakob, T.; Freudenberg, M.A.; Schmidt, M.; Goebeler, M. Mechanisms of chemical-induced innate immunity in allergic contact dermatitis. Allergy 2011, 66, 1152–1163. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Raghavan, B.; Muller, V.; Vogl, T.; Fejer, G.; Tchaptchet, S.; Keck, S.; Kalis, C.; Nielsen, P.J.; Galanos, C.; et al. Crucial role for human Toll-like receptor 4 in the development of contact allergy to nickel. Nature Immunol. 2010, 11, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, Y.; Sasaki, K.; Sasaki, A.; Takakubo, Y.; Hasegawa, H.; Ogino, T.; Konttinen, Y.T.; Salo, J.; Takagi, M. Enhanced osteolytic potential of monocytes/macrophages derived from bone marrow after particle stimulation. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Trindade, M.C.; Lind, M.; Sun, D.; Schurman, D.J.; Goodman, S.B.; Smith, R.L. In vitro reaction to orthopaedic biomaterials by macrophages and lymphocytes isolated from patients undergoing revision surgery. Biomaterials 2001, 22, 253–259. [Google Scholar] [CrossRef]
- Perren, S.M.; Mathys, R.; Pohler, O. Implants and materials in fracture fixation. In AO Principles of Fracture Management; Colton, C.L., Fernandez Dell’Oca, A., Kellam, J.F., Holz, U., Ochsner, P.E., Eds.; AO Foundation: Dübendorf, Switzerland, 2004; pp. 36–40. [Google Scholar]
- Tomizawa, Y.; Hanawa, T. Corrosion of pure titanium sternal wire. Ann. Thorac. Surg. 2007, 84, 1012–1014. [Google Scholar] [CrossRef] [PubMed]
- Mu, Y.; Kobayashi, T.; Sumita, M.; Yamamoto, A.; Hanawa, T. Metal ion release from titanium with active oxygen species generated by rat macrophages in vitro. J. Biomed. Mater. Res. 2000, 49, 238–243. [Google Scholar] [CrossRef]
- Kwon, Y.M.; Thomas, P.; Summer, B.; Pandit, H.; Taylor, A.; Beard, D.; Murray, D.W.; Gill, H.S. Lymphocyte proliferation responses in patients with pseudotumors following metal-on-metal hip resurfacing arthroplasty. J. Orthop. Res. 2010, 28, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Kwon, Y.M.; Mehmood, S.; Downing, C.; Jurkschat, K.; Murray, D.W. Characterization of metal-wear nanoparticles in pseudotumor following metal-on-metal hip resurfacing. Nanomedicine 2011, 7, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.J.; Gilbert, J.L.; Urban, R.M. Corrosion of metal orthopaedic implants. J. Bone Joint Surg. Am. 1998, 80, 268–282. [Google Scholar] [CrossRef] [PubMed]
- Leso, V.; Fontana, L.; Mauriello, M.C.; Iavicoli, I. Occupational Risk Assessment of Engineered Nanomaterials: Limits, Challenges and Opportunities. Curr. Nanosci. 2017, 13, 55–78. [Google Scholar] [CrossRef]
- Warheit, D.B.; Hansen, J.F.; Yuen, I.S.; Kelly, D.P.; Snajdr, S.I.; Hartsky, M.A. Inhalation of high concentrations of low toxicity dusts in rats results in impaired pulmonary clearance mechanisms and persistent inflammation. Toxicol. Appl. Pharmacol. 1997, 145, 10–22. [Google Scholar] [CrossRef] [PubMed]
- St Pierre, C.A.; Chan, M.; Iwakura, Y.; Ayers, D.C.; Kurt-Jones, E.A.; Finberg, R.W. Periprosthetic osteolysis: Characterizing the innate immune response to titanium wear-particles. J. Orthop. Res. 2010, 28, 1418–1424. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.B. Wear particles, periprosthetic osteolysis and the immune system. Biomaterials 2007, 28, 5044–5048. [Google Scholar] [CrossRef] [PubMed]
- Kohilas, K.; Lyons, M.; Lofthouse, R.; Frondoza, C.G.; Jinnah, R.; Hungerford, D.S. Effect of prosthetic titanium wear debris on mitogen-induced monocyte and lymphoid activation. J. Biomed. Mater. Res. 1999, 47, 95–103. [Google Scholar] [CrossRef]
- Hallab, N.J.; Anderson, S.; Caicedo, M.; Brasher, A.; Mikecz, K.; Jacobs, J.J. Effects of soluble metals on human peri-implant cells. J. Biomed. Mater. Res. A 2005, 74, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Fulcher, D.; Wong, S. Carboxyfluorescein succinimidyl ester-based proliferative assays for assessment of T cell function in the diagnostic laboratory. Immunol. Cell Biol. 1999, 77, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Milovanova, T.N.; Popma, S.H.; Cherian, S.; Moore, J.S.; Rossman, M.D. Flow cytometric test for beryllium sensitivity. Cytometry Part B Clin. Cytometry 2004, 60, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Milovanova, T.N. Comparative analysis between CFSE flow cytometric and tritiated thymidine incorporation tests for beryllium sensitivity. Cytometry Part B Clin. Cytometry 2007, 72, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Caicedo, M.; McAllister, K.; Skipor, A.; Amstutz, H.; Jacobs, J.J. Asymptomatic prospective and retrospective cohorts with metal-on-metal hip arthroplasty indicate acquired lymphocyte reactivity varies with metal ion levels on a group basis. J. Orthop. Res. 2013, 31, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Schanen, B.C.; Das, S.; Reilly, C.M.; Warren, W.L.; Self, W.T.; Seal, S.; Drake, D.R., 3rd. Immunomodulation and T helper TH(1)/TH(2) response polarization by CeO(2) and TiO(2) nanoparticles. PLoS ONE 2013, 8, e62816. [Google Scholar] [CrossRef] [PubMed]
- Cadosch, D.; Sutanto, M.; Chan, E.; Mhawi, A.; Gautschi, O.P.; von Katterfeld, B.; Simmen, H.P.; Filgueira, L. Titanium uptake, induction of RANK-L expression, and enhanced proliferation of human T-lymphocytes. J. Orthop. Res. 2010, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.P.; Mhawi, A.; Clode, P.; Saunders, M.; Filgueira, L. Effects of titanium(iv) ions on human monocyte-derived dendritic cells. Met. Integr. Biomet. Sci. 2009, 1, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Goodman, S.B.; Konttinen, Y.T.; Raska, M. Particle disease: Biologic mechanisms of periprosthetic osteolysis in total hip arthroplasty. Innate Immun. 2013, 19, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, S.; Dornhofertakenaka, H.; Muhle, H. Alveolar Distribution of Fly-Ash and of Titanium-Dioxide after Long-Term Inhalation by Wistar Rats. J. Aerosol Sci. 1986, 17, 361–364. [Google Scholar] [CrossRef]
- Warheit, D.B.; Webb, T.R.; Sayes, C.M.; Colvin, V.L.; Reed, K.L. Pulmonary instillation studies with nanoscale TiO2 rods and dots in rats: Toxicity is not dependent upon particle size and surface area. Toxicol. Sci. 2006, 91, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Iavicoli, I.; Fontana, L.; Leso, V.; Corbi, M.; Marinaccio, A.; Leopold, K.; Schindl, R.; Lucchetti, D.; Calapa, F.; Sgambato, A. Subchronic exposure to palladium nanoparticles affects serum levels of cytokines in female Wistar rats. Hum. Exp. Toxicol. 2018, 37, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.F.; Wu, N.; Porter, D.; Buford, M.; Wolfarth, M.; Holian, A. Particle length-dependent titanium dioxide nanomaterials toxicity and bioactivity. Part. Fibre Toxicol. 2009, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Moon, C.; Park, H.J.; Choi, Y.H.; Park, E.M.; Castranova, V.; Kang, J.L. Pulmonary inflammation after intraperitoneal administration of ultrafine titanium dioxide (TiO2) at rest or in lungs primed with lipopolysaccharide. J. Toxicol. Environ. Health A 2010, 73, 396–409. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.M.; Pylkkanen, L.; Koivisto, A.J.; Nykasenoja, H.; Wolff, H.; Savolainen, K.; Alenius, H. Inhalation exposure to nanosized and fine TiO2 particles inhibits features of allergic asthma in a murine model. Part. Fibre Toxicol. 2010, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Sager, T.M.; Kommineni, C.; Castranova, V. Pulmonary response to intratracheal instillation of ultrafine versus fine titanium dioxide: Role of particle surface area. Part. Fibre Toxicol. 2008, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granchi, D.; Ciapetti, G.; Savarino, L.; Stea, S.; Filippini, F.; Sudanese, A.; Rotini, R.; Giunti, A. Expression of the CD69 activation antigen on lymphocytes of patients with hip prosthesis. Biomaterials 2000, 21, 2059–2065. [Google Scholar] [CrossRef]
- Schanen, B.C.; Karakoti, A.S.; Seal, S.; Drake, D.R., 3rd; Warren, W.L.; Self, W.T. Exposure to titanium dioxide nanomaterials provokes inflammation of an in vitro human immune construct. ACS Nano 2009, 3, 2523–2532. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Lauridsen, H.M.; Amezquita, R.A.; Pierce, R.W.; Jane-Wit, D.; Fang, C.; Pellowe, A.S.; Kirkiles-Smith, N.C.; Gonzalez, A.L.; Pober, J.S. IL-17 Promotes Neutrophil-Mediated Immunity by Activating Microvascular Pericytes and Not Endothelium. J. Immunol. 2016, 197, 2400–2408. [Google Scholar] [CrossRef] [PubMed]
- Jacobi-Gresser, E.; Huesker, K.; Schutt, S. Genetic and immunological markers predict titanium implant failure: A retrospective study. Int. J. Oral Maxillofac. Surg. 2013, 42, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Wang, N.; Zhu, M.; Lu, J.; Zhong, H.; Xue, X.; Guo, S.; Li, M.; Wei, X.; Tao, Y.; Yin, H. TiO2 nanoparticles cause mitochondrial dysfunction, activate inflammatory responses, and attenuate phagocytosis in macrophages: A proteomic and metabolomic insight. Redox Biol. 2018, 15, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Vamanu, C.I.; Cimpan, M.R.; Høl, P.J.; Sornes, S.; Lie, S.A.; Gjerdet, N.R. Induction of cell death by TiO(2) nanoparticles: Studies on a human monoblastoid cell line. Toxicol. In Vitro 2008, 22, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Kongseng, S.; Yoovathaworn, K.; Wongprasert, K.; Chunhabundit, R.; Sukwong, P.; Pissuwan, D. Cytotoxic and inflammatory responses of TiO nanoparticles on human peripheral blood mononuclear cells. J. Appl. Toxicol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Iavicoli, I.; Fontana, L.; Corbi, M.; Leso, V.; Marinaccio, A.; Leopold, K.; Schindl, R.; Sgambato, A. Exposure to Palladium Nanoparticles Affects Serum Levels of Cytokines in Female Wistar Rats. PLoS ONE 2015, 10, e0143801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantrell, D.A.; Collins, M.K.; Crumpton, M.J. Autocrine regulation of T-lymphocyte proliferation: Differential induction of IL-2 and IL-2 receptor. Immunology 1988, 65, 343–349. [Google Scholar] [PubMed]
- Tinoco, A.D.; Valentine, A.M. Ti(IV) Binds to Human Serum Transferrin More Tightly Than Does Fe(III). J. Am. Chem. Soc. 2005, 127, 11218–11219. [Google Scholar] [CrossRef] [PubMed]
- Allouni, Z.E.; Høl, P.J.; Cauqui, M.A.; Gjerdet, N.R.; Cimpan, M.R. Role of physicochemical characteristics in the uptake of TiO(2) nanoparticles by fibroblasts. Toxicol. In Vitro 2012. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | Metal Implants | General Health |
|---|---|---|---|---|
| 1 | F | 1965 | - | Healthy. Ni allergic |
| 2 | F | 1968 | - | Healthy. Ni allergic |
| 3 | F | 1993 | - | Healthy. Ni allergic |
| 4 | M | 1968 | - | Healthy. Ni allergic |
| 5 | F | 1964 | - | Healthy. Ni allergic |
| 6 | M | 1964 | - | Healthy. Ni allergic and hand eczema. |
| 7 | M | 1991 | - | Healthy. Hand eczema. |
| 8 | M | 1973 | - | Healthy. Skin allergy. Hand eczema. |
| 9 | F | 1963 | THA 1 (1y) | Diabetes, Joint/muscle disease |
| 10 | M | 1968 | THA | Stroke (8 years ago) |
| 11 | M | 1949 | Plates/screws (22 y) | Good |
| 12 | M | 1943 | Bilateral THA (1 y, 3 y) | Good |
| 13 | F | 1947 | Bilateral THA (20 y) | Osteoarthritis. Hip pain. |
| 14 | F | 1974 | Bilateral THA (11 y). Ti heart valve (15 y) | Heart disease, Joint/Muscle disease or rheumatism |
| 15 | M | 1934 | Peripheral stent (2 y). Pacemaker (2 y) | Diabetes, heart disease, Parkinson’s |
| 16 | M | 1942 | Two peripheral stents (12 y, 14 y) | Parkinson’s and heart disease |
| 17 | F | 1940 | Aorta stent, re-stented twice due to restenosis | Heart disease |
| 18 | M | 1943 | Stent graft (10 days) | N/A 3 |
| 19 | F | N/A | Nails/Screws right knee (11 y). TKA 2 left (6 y) | High blood pressure, osteoarthritis, rhinitis and eczema |
| 20 | F | 1984 | Dental implants (6 y) | Gastric/ Intestinal disease (IBS) and eczema |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Høl, P.J.; Kristoffersen, E.K.; Gjerdet, N.R.; Pellowe, A.S. Novel Nanoparticulate and Ionic Titanium Antigens for Hypersensitivity Testing. Int. J. Mol. Sci. 2018, 19, 1101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041101
Høl PJ, Kristoffersen EK, Gjerdet NR, Pellowe AS. Novel Nanoparticulate and Ionic Titanium Antigens for Hypersensitivity Testing. International Journal of Molecular Sciences. 2018; 19(4):1101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041101
Chicago/Turabian StyleHøl, Paul Johan, Einar K. Kristoffersen, Nils Roar Gjerdet, and Amanda S. Pellowe. 2018. "Novel Nanoparticulate and Ionic Titanium Antigens for Hypersensitivity Testing" International Journal of Molecular Sciences 19, no. 4: 1101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041101