Current Approaches Including Novel Nano/Microtechniques to Reduce Silicone Implant-Induced Contracture with Adverse Immune Responses

 , , ,
, , , 
Abstract
:1. Introduction
2. Anaplastic Large Cell Lymphoma (ALCL)
3. Approaches to Reducing Adverse Immune Responses
3.1. Drugs
3.1.1. Systemic Drugs
3.1.2. Topical Application
3.2. Materials
3.2.1. Combined with Autologous Tissues (Fat Grafts)
3.2.2. Combined with Acellular Dermal Matrix
3.3. Surface Type
3.3.1. Smooth and Textured Surfaces
3.3.2. Surface Modification Using Nano/Microtechnology
4. Future Directions
5. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| ALCL | Anaplastic large cell lymphoma |
| IL-17 | Interleukin-17 |
| IL-6 | Interleukin-6 |
| IL-8 | Interleukin-8 |
| TGF-β1 | Transforming growth factor-β1 |
| IFN-γ | Interferon-gamma |
| LTAs | Leukotriene antagonists |
| Cys-LT1 | Cysteinyl leukotrienes receptors type 1 |
| PFD | Pirfenidone |
| ADM | Acellular dermal matrix |
| ECM | Extracellular matrix |
| FCs | Human fibroblasts |
| ECs | Human endothelial cells |
| SMCs | Human smooth muscle cells |
| PDMS | Polydimethylsiloxane |
| SEM | Scanning electron microscopy |
| ADM PDMS F | Acellular dermal matrix polydimethylsiloxane fabricated surface |
| ADM PDMS C | Acellular dermal matrix polydimethylsiloxane cast surface |
| BDFs | Breast-derived fibroblasts |
| TNF-α | Tumor necrosis factor-alpha |
References
- Pearse, H.E. Results from using Vitallium tubes in biliary surgery. Ann. Surg. 1946, 124, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B.; McCue, J. Safety and effectiveness of Mentor’s Memorygel implants at 6 years. Aesthet. Plast. Surg. 2009, 33, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Spear, S.L.; Murphy, D.K.; Slicton, A.; Walker, P.S. Inamed silicone breast implant, U.S.S.G. Inamed silicone breast implant core study results at 6 years. Plast. Reconstr. Surg. 2007, 120, 8S–16S. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B. The Mentor study on contour profile gel silicone MemoryGel breast implants. Plast. Reconstr. Surg. 2007, 120, 33S–39S. [Google Scholar] [CrossRef] [PubMed]
- Araco, A.; Gravante, G.; Araco, F.; Delogu, D.; Cervelli, V. Capsular contracture: Results of 3002 patients with aesthetic breast augmentation. Plast. Reconstr. Surg. 2006, 118, 1499–1500. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.S.; Walls, B.; Murphy, D.K. Natrelle saline-filled breast implants: A prospective 10-year study. Aesthet. Surg. J. 2009, 29, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Spear, S.L.; Baker, J.L., Jr. Classification of capsular contracture after prosthetic breast reconstruction. Plast. Reconstr. Surg. 1995, 96, 1119–1123. [Google Scholar] [CrossRef] [PubMed]
- Forster, N.A.; Kunzi, W.; Giovanoli, P. The reoperation cascade after breast augmentation with implants: What the patient needs to know. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Handel, N.; Cordray, T.; Gutierrez, J.; Jensen, J.A. A long-term study of outcomes, complications, and patient satisfaction with breast implants. Plast. Reconstr. Surg. 2006, 117, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Kamel, M.; Protzner, K.; Fornasier, V.; Peters, W.; Smith, D.; Ibanez, D. The PERI-implant breast capsule: An immunophenotypic study of capsules taken at explantation surgery. J. Biomed. Mater. Res. 2001, 58, 88–96. [Google Scholar] [CrossRef]
- Adams, W.P., Jr.; Haydon, M.S.; Raniere, J., Jr.; Trott, S.; Marques, M.; Feliciano, M.; Robinson, J.B., Jr.; Tang, L.; Brown, S.A. A rabbit model for capsular contracture: Development and clinical implications. Plast. Reconstr. Surg. 2006, 117, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- De Jong, D.; Vasmel, W.L.; de Boer, J.P.; Verhave, G.; Casparie, M.K.; van Leeuwen, F.E. Anaplastic large-cell lymphoma in women with breast implants. JAMA 2008, 300, 2030–2035. [Google Scholar] [CrossRef] [PubMed]
- Duvic, M.; Moore, D.; Menter, A.; Vonderheid, E.C. Cutaneous T-cell lymphoma in association with silicone breast implants. J. Am. Acad. Dermatol. 1995, 32, 939–942. [Google Scholar] [CrossRef]
- Roden, A.C.; Macon, W.R.; Keeney, G.L.; Myers, J.L.; Feldman, A.L.; Dogan, A. Seroma-associated primary anaplastic large-cell lymphoma adjacent to breast implants: An indolent T-cell lymphoproliferative disorder. Mod. Pathol. 2008, 21, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Roth, C.; Chung, K.C.; Young, V.L.; van Busum, K.; Schnyer, C.; Mattke, S. Anaplastic large cell lymphoma and breast implants: A systematic review. Plast. Reconstr. Surg. 2011, 127, 2141–2150. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.A.; Gruss, H.J.; Davis, T.; Anderson, D.; Farrah, T.; Baker, E.; Sutherland, G.R.; Brannan, C.I.; Copeland, N.G.; Jenkins, N.A.; et al. Cd30 antigen, a marker for Hodgkin’s lymphoma, is a receptor whose ligand defines an emerging family of cytokines with homology to TNF. Cell 1993, 73, 1349–1360. [Google Scholar] [CrossRef]
- Falini, B.; Martelli, M.P. Anaplastic large cell lymphoma: Changes in the world health organization classification and perspectives for targeted therapy. Haematologica 2009, 94, 897–900. [Google Scholar] [CrossRef] [PubMed]
- Brody, G.S. Anaplastic large cell lymphoma occurring in women with breast implants: Analysis of 173 cases. Plast. Reconstr. Surg. 2015, 136, 553e–554e. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Roth, C.; Young, V.L.; Chung, K.C.; van Busum, K.; Schnyer, C.; Mattke, S. Anaplastic large cell lymphoma and breast implants: Results from a structured expert consultation process. Plast. Reconstr. Surg. 2011, 128, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Jewell, M.; Spear, S.L.; Largent, J.; Oefelein, M.G.; Adams, W.P., Jr. Anaplastic large T-cell lymphoma and breast implants: A review of the literature. Plast. Reconstr. Surg. 2011, 128, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Lade, S.; Webster, H.; Ryan, G.; Prince, H.M. Effusion-associated anaplastic large cell lymphoma of the breast: Time for it to be defined as a distinct clinico-pathological entity. Haematologica 2010, 95, 1977–1979. [Google Scholar] [CrossRef] [PubMed]
- Antonella, C.; Rosaria, B.; Marcella, M. 22 cases of BIA-ALCL: Awareness and outcome tracking from the Italian ministry of health. Plast. Reconstr. Surg. 2018, 141, 11e–19e. [Google Scholar]
- Loch-Wilkinson, A.; Beath, K.J.; Knight, R.J.W.; Wessels, W.L.F.; Magnusson, M.; Papadopoulos, T.; Connell, T.; Lofts, J.; Locke, M.; Hopper, I.; et al. Breast implant-associated anaplastic large cell lymphoma in Australia and New Zealand: High-surface-area textured implants are associated with increased risk. Plast. Reconstr. Surg. 2017, 140, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Johani, K.; Almatroudi, A.; Vickery, K.; van Natta, B.; Kadin, M.E.; Brody, G.; Clemens, M.; Cheah, C.Y.; Lade, S.; et al. Bacterial biofilm infection detected in breast implant-associated anaplastic large-cell lymphoma. Plast. Reconstr. Surg. 2016, 137, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Kadin, M.E.; Deva, A.; Xu, H.; Morgan, J.; Khare, P.; MacLeod, R.A.; van Natta, B.W.; Adams, W.P., Jr.; Brody, G.S.; Epstein, A.L. Biomarkers provide clues to early events in the pathogenesis of breast implant-associated anaplastic large cell lymphoma. Aesthet Surg. J. 2016, 36, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Aladily, T.N.; Medeiros, L.J.; Amin, M.B.; Haideri, N.; Ye, D.; Azevedo, S.J.; Jorgensen, J.L.; de Peralta-Venturina, M.; Mustafa, E.B.; Young, K.H.; et al. Anaplastic large cell lymphoma associated with breast implants: A report of 13 cases. Am. J. Surg. Pathol. 2012, 36, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Gidengil, C.A.; Predmore, Z.; Mattke, S.; van Busum, K.; Kim, B. Breast implant-associated anaplastic large cell lymphoma: A systematic review. Plast. Reconstr. Surg. 2015, 135, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Prince, H.M. Breast implant-associated anaplastic large cell lymphoma: A systematic review of the literature and mini-meta analysis. Curr. Hematol. Malig. Rep. 2013, 8, 196–210. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa, D.R.; Miranda, R.N.; Kaura, A.; Francis, A.M.; Campanale, A.; Boldrini, R.; Alexander, J.; Deva, A.K.; Gravina, P.R.; Medeiros, L.J.; et al. Global adverse event reports of breast implant-associated ALCL: An international review of 40 government authority databases. Plast. Reconstr. Surg. 2017, 139, 1029–1039. [Google Scholar] [CrossRef] [PubMed]
- Wolfram, D.; Rabensteiner, E.; Grundtman, C.; Bock, G.; Mayerl, C.; Parson, W.; Almanzar, G.; Hasenohrl, C.; Piza-Katzer, H.; Wick, G. T regulatory cells and TH17 cells in peri-silicone implant capsular fibrosis. Plast. Reconstr. Surg. 2012, 129, 327e–337e. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.M.; Anderson, J.M. Human monocyte/macrophage activation and interleukin 1 generation by biomedical polymers. J. Biomed. Mater. Res. 1988, 22, 713–731. [Google Scholar] [CrossRef] [PubMed]
- O’Hanlon, T.P.; Okada, S.; Love, L.A.; Dick, G.; Young, V.L.; Miller, F.W. Immunohistopathology and T cell receptor gene expression in capsules surrounding silicone breast implants. Curr. Top. Microbiol. Immunol. 1996, 210, 237–242. [Google Scholar] [PubMed]
- Wolfram, D.; Rainer, C.; Niederegger, H.; Piza, H.; Wick, G. Cellular and molecular composition of fibrous capsules formed around silicone breast implants with special focus on local immune reactions. J. Autoimmun. 2004, 23, 81–91. [Google Scholar] [PubMed]
- Ooi, A.; Song, D.H. Reducing infection risk in implant-based breast-reconstruction surgery: Challenges and solutions. Breast Cancer 2016, 8, 161–172. [Google Scholar] [PubMed]
- Clayton, J.L.; Bazakas, A.; Lee, C.N.; Hultman, C.S.; Halvorson, E.G. Once is not enough: Withholding postoperative prophylactic antibiotics in prosthetic breast reconstruction is associated with an increased risk of infection. Plast. Reconstr. Surg. 2012, 130, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.L.; Ellenbogen, R.; Desvigne, M.N.; Svehlak, S.; Heck, R. Zafirlukast (Accolate): A new treatment for capsular contracture. Aesthet. Surg. J. 2002, 22, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.L.; Desvigne, M.N.; Ellenbogen, R.; Svehlak, S.; Heck, R. Results of using zafirlukast (Accolate) and montelukast (Singulair) for treatment of capsular contracture. Aesthet. Surg. J. 2003, 23, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.K.; Handel, N. Effects of singulair (Montelukast) treatment for capsular contracture. Aesthet. Surg. J. 2010, 30, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, N.; Mazzocchi, M.; Fioramonti, P.; Bistoni, G. The effects of Zafirlukast on capsular contracture: Preliminary report. Aesthet. Plast. Surg. 2006, 30, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Mazzocchi, M.; Dessy, L.A.; Alfano, C.; Scuderi, N. Effects of Zafirlukast on capsular contracture: Long-term results. Int. J. Immunopathol. Pharmacol. 2012, 25, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Sapountzis, S.; Kim, J.H.; Francescato Veiga, D.; Masako Ferreira, L. The effect of Zafirlukast on capsule formation in post-radiation silicone implants. Med. Hypotheses 2012, 78, 787–789. [Google Scholar] [CrossRef] [PubMed]
- Perng, D.W.; Wu, Y.C.; Chang, K.T.; Wu, M.T.; Chiou, Y.C.; Su, K.C.; Perng, R.P.; Lee, Y.C. Leukotriene C4 induces TGF-β1 production in airway epithelium via P38 kinase pathway. Am. J. Respir. Cell Mol. Biol. 2006, 34, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Shimbori, C.; Shiota, N.; Okunishi, H. Effects of montelukast, a cysteinyl-leukotriene type 1 receptor antagonist, on the pathogenesis of bleomycin-induced pulmonary fibrosis in mice. Eur. J. Pharmacol. 2011, 650, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Spano, A.; Palmieri, B.; Taidelli, T.P.; Nava, M.B. Reduction of capsular thickness around silicone breast implants by Zafirlukast in rats. Eur. Surg. Res. 2008, 41, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Zimman, O.A.; Toblli, J.; Stella, I.; Ferder, M.; Ferder, L.; Inserra, F. The effects of angiotensin-converting-enzyme inhibitors on the fibrous envelope around mammary implants. Plast. Reconstr. Surg. 2007, 120, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Gancedo, M.; Ruiz-Corro, L.; Salazar-Montes, A.; Rincon, A.R.; Armendariz-Borunda, J. Pirfenidone prevents capsular contracture after mammary implantation. Aesthet. Plast. Surg. 2008, 32, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.N.; Wild, J.S.; Schiedt, M.J.; Hyde, D.M.; Margolin, S.B.; Giri, S.N. Dietary intake of pirfenidone ameliorates bleomycin-induced lung fibrosis in hamsters. J. Lab. Clin. Med. 1995, 125, 779–785. [Google Scholar] [PubMed]
- Garcia, L.; Hernandez, I.; Sandoval, A.; Salazar, A.; Garcia, J.; Vera, J.; Grijalva, G.; Muriel, P.; Margolin, S.; Armendariz-Borunda, J. Pirfenidone effectively reverses experimental liver fibrosis. J. Hepatol. 2002, 37, 797–805. [Google Scholar] [CrossRef]
- Shimizu, T.; Kuroda, T.; Hata, S.; Fukagawa, M.; Margolin, S.B.; Kurokawa, K. Pirfenidone improves renal function and fibrosis in the post-obstructed kidney. Kidney Int. 1998, 54, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Veras-Castillo, E.R.; Cardenas-Camarena, L.; Lyra-Gonzalez, I.; Munoz-Valle, J.F.; Lucano-Landeros, S.; Guerrerosantos, J.; Gonzalez-Ulloa, B.; Mercado-Barajas, J.L.; Sanchez-Parada, M.G.; Azabache-Wennceslao, R.; et al. Controlled clinical trial with pirfenidone in the treatment of breast capsular contracture: Association of TGF-β polymorphisms. Ann. Plast. Surg. 2013, 70, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Hawtof, D.B.; Kelly, C.B. Colchicine and capsular contracture around breast prostheses. Eur. J. Plast. Surg. 1996, 19, 81–83. [Google Scholar] [CrossRef]
- Borisy, G.G.; Taylor, E.W. The mechanism of action of colchicine. Binding of colchincine-3H to cellular protein. J. Cell Biol. 1967, 34, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Cocco, G.; Chu, D.C.; Pandolfi, S. Colchicine in clinical medicine. A guide for internists. Eur. J. Intern. Med. 2010, 21, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.L., Jr. The effectiveness of α-tocopherol (vitamin E) in reducing the incidence of spherical contracture around breast implants. Plast. Reconstr. Surg. 1981, 68, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Cook-Mills, J.M. Isoforms of Vitamin E differentially regulate PKC α and inflammation: A review. J. Clin. Cell. Immunol. 2013, 4, 1000137. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Weisskopf, M.G.; O’Reilly E, J.; Jacobs, E.J.; McCullough, M.L.; Calle, E.E.; Cudkowicz, M.; Thun, M.J. Vitamin E intake and risk of amyotrophic lateral sclerosis. Ann. Neurol. 2005, 57, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Rossato, M.F.; Hoffmeister, C.; Tonello, R.; de Oliveira Ferreira, A.P.; Ferreira, J. Anti-inflammatory effects of Vitamin E on adjuvant-induced arthritis in rats. Inflammation 2015, 38, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.; Johnson, N.; Zegzula, H.D.; Schray, M.; Glissmeyer, M.; Sorenson, L. Prophylactic use of Pentoxifylline (Trental) and Vitamin E to prevent capsular contracture after implant reconstruction in patients requiring adjuvant radiation. Am. J. Surg. 2016, 211, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Jang, S.Y.; Ryou, J.H.; Kim, W.S.; Kim, H.K.; Bae, T.H.; Kim, M.K. Preventive effect of synthetic tryptophan metabolite on silicone breast implant-induced capsule formation. Ann. Plast. Surg. 2018, 80, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Chikaraishi, A.; Hirahashi, J.; Takase, O.; Marumo, T.; Hishikawa, K.; Hayashi, M.; Saruta, T. Tranilast inhibits interleukin-1β-induced monocyte chemoattractant protein-1 expression in rat mesangial cells. Eur. J. Pharmacol. 2001, 427, 151–158. [Google Scholar] [CrossRef]
- Shimizu, T.; Kanai, K.; Kyo, Y.; Asano, K.; Hisamitsu, T.; Suzaki, H. Effect of tranilast on matrix metalloproteinase production from neutrophils in-vitro. J. Pharm. Pharmacol. 2006, 58, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Frumento, G.; Rotondo, R.; Tonetti, M.; Damonte, G.; Benatti, U.; Ferrara, G.B. Tryptophan-derived catabolites are responsible for inhibition of t and natural killer cell proliferation induced by indoleamine 2,3-dioxygenase. J. Exp. Med. 2002, 196, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Inglis, J.J.; Criado, G.; Andrews, M.; Feldmann, M.; Williams, R.O.; Selley, M.L. The anti-allergic drug, N-(3′,4′-dimethoxycinnamonyl) anthranilic acid, exhibits potent anti-inflammatory and analgesic properties in arthritis. Rheumatology 2007, 46, 1428–1432. [Google Scholar] [CrossRef] [PubMed]
- Yalanis, G.C.; Liu, E.W.; Cheng, H.T. Efficacy and safety of povidone-iodine irrigation in reducing the risk of capsular contracture in aesthetic breast augmentation: A systematic review and meta-analysis. Plast. Reconstr. Surg. 2015, 136, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Wiener, T.C. The role of betadine irrigation in breast augmentation. Plast. Reconstr. Surg. 2007, 119, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Adams, W.P., Jr.; Rios, J.L.; Smith, S.J. Enhancing patient outcomes in aesthetic and reconstructive breast surgery using triple antibiotic breast irrigation: Six-year prospective clinical study. Plast. Reconstr. Surg. 2006, 118, 46S–52S. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, P.; Jorgensen, S.; Kristiansen, T.B.; Jorgensen, A.; Holmich, L.R. Protective effect of topical antibiotics in breast augmentation. Plast. Reconstr. Surg. 2009, 124, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Ahn, M.; Piao, Y.; Ha, Y.; Choi, D.K.; Yi, M.H.; Shin, N.; Kim, D.W.; Oh, S.H. Effect of botulinum toxin type a on TGF-β/SMAD pathway signaling: Implications for silicone-induced capsule formation. Plast. Reconstr. Surg. 2016, 138, 821e–829e. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.D.; Yi, M.H.; Kim, D.W.; Lee, Y.; Choi, Y.; Oh, S.H. The effect of botulinum neurotoxin type A on capsule formation around silicone implants: The in vivo and in vitro study. Int. Wound J. 2016, 13, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulou, G.A.; Papalois, A.; Batistatou, A.; Doukas, M.; Tsoutsos, D. Can the use of hyaluronidase reduce capsule formation? Aesthet. Plast. Surg. 2011, 35, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Cachay-Velasquez, H.; Ale, A. Lateral approach in mammary implants. Ann. Plast. Surg. 1990, 25, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim Canter, H.; Konas, E.; Bozdogan, O.; Vargel, I.; Ozbatir, B.; Oner, F.; Erk, Y. Effect of slow-release 5-fluorouracil on capsule formation around silicone breast implants: An experimental study with mice. Aesthet. Plast. Surg. 2007, 31, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Nava, M.B.; Rocco, N.; Catanuto, G.; Frangou, J.; Rispoli, C.; Ottolenghi, J.; Bruno, N.; Spano, A. Role of Mitomycin C in preventing capsular contracture in implant-based reconstructive breast surgery: A randomized controlled trial. Plast. Reconstr. Surg. 2017, 139, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Hirche, C.; Diehm, Y.; Nuutila, K.; Kiefer, J.; Gazyakan, E.; Bueno, E.M.; Kremer, T.; Kneser, U.; Pomahac, B. Efficacy and safety of the collagenase of the bacterium clostridium histolyticum for the treatment of capsular contracture after silicone implants: Ex-vivo study on human tissue. PLoS ONE 2016, 11, e0156428. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Diehm, Y.; Henzler, T.; Berger, M.R.; Kolbenschlag, J.; Latz, A.; Bueno, E.M.; Hirche, C.; Kneser, U.; Pomahac, B. Long-term effects of the collagenase of the bacterium clostridium histolyticum for the treatment of capsular fibrosis after silicone implants. Aesthet. Plast. Surg. 2017, 41, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Hirsch, T.; Diehm, Y.; Kiefer, J.; Bueno, E.M.; Kueckelhaus, M.; Kremer, T.; Hirche, C.; Kneser, U.; Pomahac, B. The collagenase of the bacterium clostridium histolyticum for the treatment of capsular fibrosis after silicone implants. Plast. Reconstr. Surg. 2015, 136, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.C.; Chung, K.I.; Park, B.Y.; Kim, H.K.; Kim, W.S.; Bae, T.H.; Kim, M.K. The effect of antiadhesion agent on peri-implant capsular formation in rabbits. Ann. Plast. Surg. 2013, 71, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Kwon, O.H.; Lee, J.W.; Chung, H.Y.; Cho, B.C.; Park, H.Y.; Kim, T.G. The effect of montelukast and antiadhesion barrier solution on the capsule formation after insertion of silicone implants in a white rat model. Eur. Surg. Res. 2013, 51, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Shin, K.C.; Kim, W.S.; Bae, T.H.; Kim, H.K.; Kim, M.K. The preventive effect of topical Zafirlukast instillation for peri-implant capsule formation in rabbits. Arch. Plast. Surg. 2015, 42, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, M.; Kim, B.H.; Lee, J.E.; Park, H.J.; Lee, S.H.; Park, C.G.; Kim, M.H.; Kim, R.; Kim, E.H.; et al. Acute suppression of TGF-SS with local, sustained release of Tranilast against the formation of fibrous capsules around silicone implants. J. Control. Release 2015, 200, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Moreira, M.; Fagundes, D.J.; de Jesus Simoes, M.; Taha, M.O.; Perez, L.M.; Bazotte, R.B. The effect of liposome-delivered prednisolone on collagen density, myofibroblasts, and fibrous capsule thickness around silicone breast implants in rats. Wound Repair Regener. 2010, 18, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Marques, M.; Brown, S.; Correia-Sa, I.; Rodrigues-Pereira, P.; Goncalves-Rodrigues, A.; Amarante, J. The impact of triamcinolone acetonide in early breast capsule formation in a rabbit model. Aesthet. Plast. Surg. 2012, 36, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Sconfienza, L.M.; Murolo, C.; Callegari, S.; Calabrese, M.; Savarino, E.; Santi, P.; Sardanelli, F. Ultrasound-guided percutaneous injection of triamcinolone acetonide for treating capsular contracture in patients with augmented and reconstructed breast. Eur. Radiol. 2011, 21, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Zeplin, P.H.; Larena-Avellaneda, A.; Schmidt, K. Surface modification of silicone breast implants by binding the Antifibrotic drug Halofuginone reduces capsular fibrosis. Plast. Reconstr. Surg. 2010, 126, 266–274. [Google Scholar] [CrossRef] [PubMed]
- McGaha, T.L.; Phelps, R.G.; Spiera, H.; Bona, C. Halofuginone, an inhibitor of type-I collagen synthesis and skin sclerosis, blocks transforming-growth-factor-β-mediated SMAD3 activation in fibroblasts. J. Investig. Dermatol. 2002, 118, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Spira, G.; Mawasi, N.; Paizi, M.; Anbinder, N.; Genina, O.; Alexiev, R.; Pines, M. Halofuginone, a collagen type I inhibitor improves liver regeneration in cirrhotic rats. J. Hepatol. 2002, 37, 331–339. [Google Scholar] [CrossRef]
- Pines, M.; Domb, A.; Ohana, M.; Inbar, J.; Genina, O.; Alexiev, R.; Nagler, A. Reduction in dermal fibrosis in the tight-skin (TSK) mouse after local application of Halofuginone. Biochem. Pharmacol. 2001, 62, 1221–1227. [Google Scholar] [CrossRef]
- Pines, M.; Snyder, D.; Yarkoni, S.; Nagler, A. Halofuginone to treat fibrosis in chronic graft-versus-host disease and scleroderma. Biol. Blood Marrow Transplant. 2003, 9, 417–425. [Google Scholar] [CrossRef]
- Acuner, B.; Baser, N.T.; Aslan, G.; Terzioglu, A.; Caydere, M.; Ustun, H.; Gorgu, M. The effects of colchicine-impregnated oxidized regenerated cellulose on capsular contracture. Surg. Innov. 2017, 24, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.R.; Shaw, T.E.; Raju, D.R. The influence of Vitamin E on capsule formation and contracture around silicone implants. Ann. Plast. Surg. 1980, 5, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Kenneth, K.N.; Neven, A.; Michael, A.B.; Alison, C.H.; Heather, S. Local delivery of nicotine does not mitigate fibrosis but may lead to angiogenesis. J. Biomater. Appl. 2010, 26, 349–358. [Google Scholar]
- Li, S.; Ren, L.; Xu, H.; Jia, D.; Luo, S.; Hao, L.; Yang, D. Effects of medical chitosan on capsular formation following silicone implant insertion in a rabbit model. Aesthet. Plast. Surg. 2016, 40, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Oshitani, N.; Takeda, S.; Matsumoto, H.; Minamino, H.; Hayakawa, T.; Aomatsu, K. Possible antistenotic effect of tranilast in a patient with small bowel tuberculosis to prevent intestinal obstruction due to stenosis progression by antituberculous chemotherapy. Dig. Endosc. 2013, 25, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Auclair, E.; Blondeel, P.; Del Vecchio, D.A. Composite breast augmentation: Soft-tissue planning using implants and fat. Plast. Reconstr. Surg. 2013, 132, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Salgarello, M.; Visconti, G.; Farallo, E. Autologous fat graft in radiated tissue prior to alloplastic reconstruction of the breast: Report of two cases. Aesthet. Plast. Surg. 2010, 34, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, I.; Ihrai, T.; Kaufman, G.; Nos, C.; Clough, K.B. Adipose-tissue grafting to the post-mastectomy irradiated chest wall: Preparing the ground for implant reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Roca, G.B.; Graf, R.; da Silva Freitas, R.; Salles, G., Jr.; Francisco, J.C.; Noronha, L.; Maluf, I., Jr. Autologous fat grafting for treatment of breast implant capsular contracture: A study in pigs. Aesthet. Surg. J. 2014, 34, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, M.; Bertram, M.; Kneser, U.; Keller, A.K.; Horch, R.E. Experimental total wrapping of breast implants with Acellular dermal matrix: A preventive tool against capsular contracture in breast surgery? J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Komorowska-Timek, E.; Oberg, K.C.; Timek, T.A.; Gridley, D.S.; Miles, D.A. The effect of Alloderm envelopes on Periprosthetic capsule formation with and without radiation. Plast. Reconstr. Surg. 2009, 123, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Salzberg, C.A.; Ashikari, A.Y.; Berry, C.; Hunsicker, L.M. Acellular dermal matrix-assisted direct-to-implant breast reconstruction and capsular contracture: A 13-year experience. Plast. Reconstr. Surg. 2016, 138, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Mowlds, D.S.; Salibian, A.A.; Scholz, T.; Paydar, K.Z.; Wirth, G.A. Capsular contracture in implant-based breast reconstruction: Examining the role of acellular dermal matrix fenestrations. Plast. Reconstr. Surg. 2015, 136, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Lakhiani, C.; Saint-Cyr, M. Treatment of capsular contracture using complete implant coverage by acellular dermal matrix: A novel technique. Plast. Reconstr. Surg. 2013, 132, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Embrey, M.; Adams, E.E.; Cunningham, B.; Peters, W.; Young, V.L.; Carlo, G.L. A review of the literature on the etiology of capsular contracture and a pilot study to determine the outcome of capsular contracture interventions. Aesthet. Plast. Surg. 1999, 23, 197–206. [Google Scholar] [CrossRef]
- Ersek, R.A. Molecular impact surface textured implants (MISTI) alter beneficially breast capsule formation at 36 months. J. Long Term Eff. Med. Implants 1991, 1, 155–169. [Google Scholar] [PubMed]
- Liu, X.; Zhou, L.; Pan, F.; Gao, Y.; Yuan, X.; Fan, D. Comparison of the postoperative incidence rate of capsular contracture among different breast implants: A cumulative meta-analysis. PLoS ONE 2015, 10, e0116071. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.H.; Samuel, M.; Tan, B.K.; Song, C. Capsular contracture in subglandular breast augmentation with textured versus smooth breast implants: A systematic review. Plast. Reconstr. Surg. 2006, 118, 1224–1236. [Google Scholar] [CrossRef] [PubMed]
- Barnsley, G.P.; Sigurdson, L.J.; Barnsley, S.E. Textured surface breast implants in the prevention of capsular contracture among breast augmentation patients: A meta-analysis of randomized controlled trials. Plast. Reconstr. Surg. 2006, 117, 2182–2190. [Google Scholar] [CrossRef] [PubMed]
- Minami, E.; Koh, I.H.; Ferreira, J.C.; Waitzberg, A.F.; Chifferi, V.; Rosewick, T.F.; Pereira, M.D.; Saldiva, P.H.; de Figueiredo, L.F. The composition and behavior of capsules around smooth and textured breast implants in pigs. Plast. Reconstr. Surg. 2006, 118, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Abramo, A.C.; de Oliveira, V.R.; Ledo-Silva, M.C.; de Oliveira, E.L. How texture-inducing contraction vectors affect the fibrous capsule shrinkage around breasts implants? Aesthet. Plast. Surg. 2010, 34, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Hall-Findlay, E.J. Breast implant complication review: Double capsules and late seromas. Plast. Reconstr. Surg. 2011, 127, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Danino, M.A.; Nizard, N.; Paek, L.S.; Govshievich, A.; Giot, J.P. Do bacteria and biofilm play a role in double-capsule formation around macrotextured implants? Plast. Reconstr. Surg. 2017, 140, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Pamula, E.; de Cupere, V.; Dufrene, Y.F.; Rouxhet, P.G. Nanoscale organization of adsorbed collagen: Influence of substrate hydrophobicity and adsorption time. J. Colloid Interface Sci. 2004, 271, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Bozec, L.; van der Heijden, G.; Horton, M. Collagen fibrils: Nanoscale ropes. Biophys. J. 2007, 92, 70–75. [Google Scholar] [CrossRef] [PubMed]
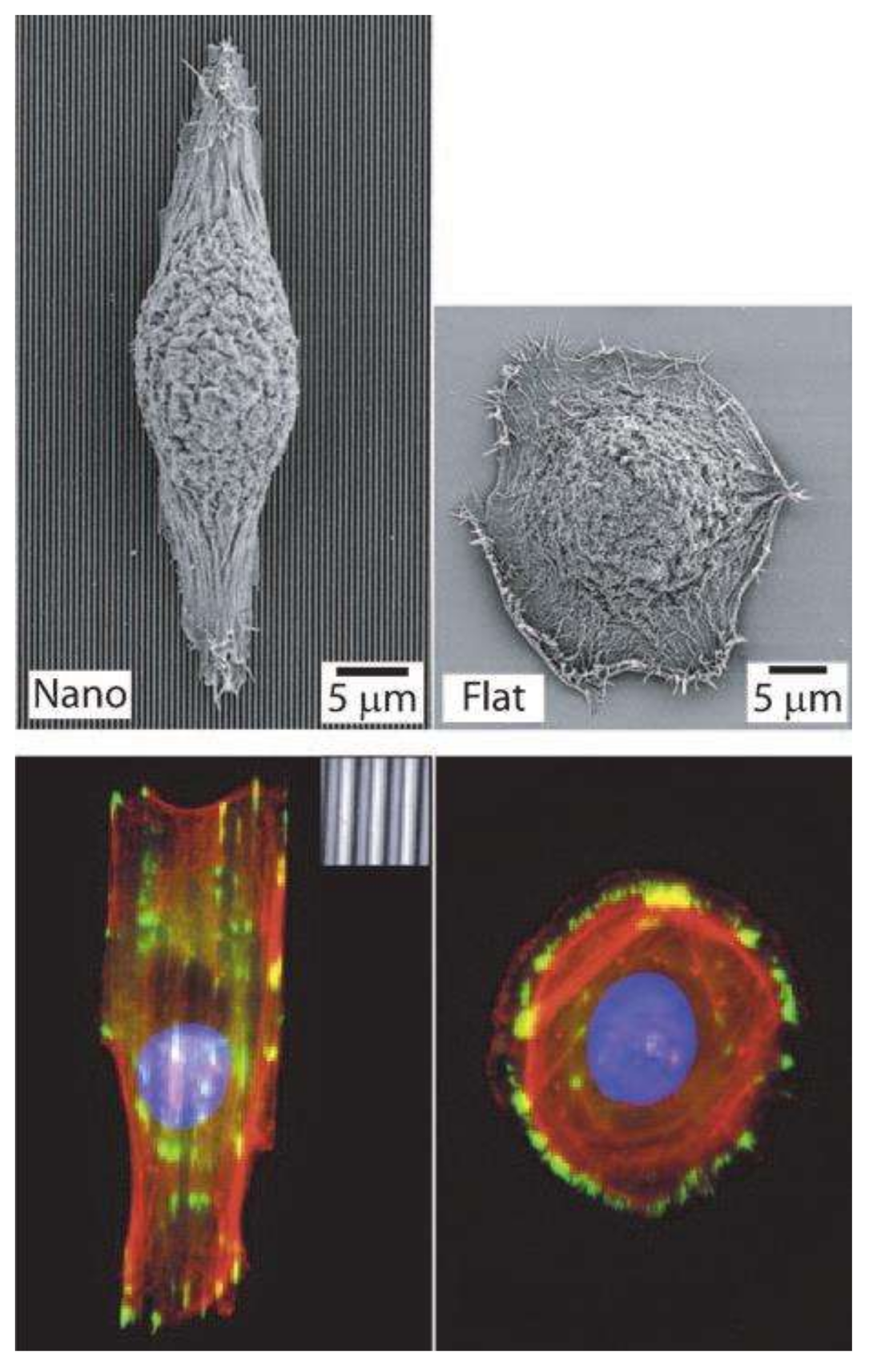
- Bettinger, C.J.; Langer, R.; Borenstein, J.T. Engineering substrate topography at the micro- and nanoscale to control cell function. Angew. Chem. 2009, 48, 5406–5415. [Google Scholar] [CrossRef] [PubMed]
- Friedl, P.; Brocker, E.B. T cell migration in three-dimensional extracellular matrix: Guidance by polarity and sensations. Dev. Immunol 2000, 7, 249–266. [Google Scholar] [CrossRef] [PubMed]
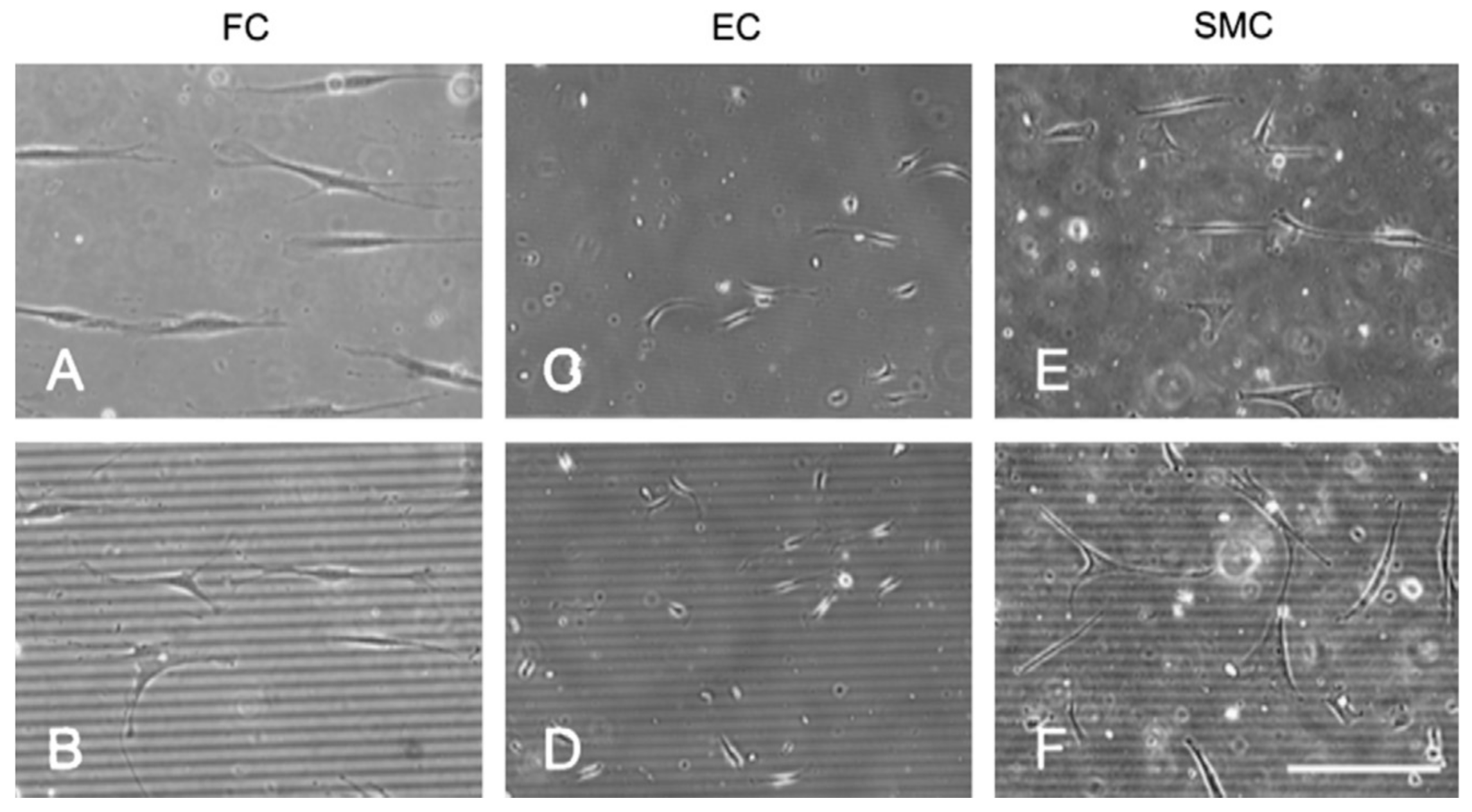
- Biela, S.A.; Su, Y.; Spatz, J.P.; Kemkemer, R. Different sensitivity of human endothelial cells, smooth muscle cells and fibroblasts to topography in the nano-micro range. Acta Biomater. 2009, 5, 2460–2466. [Google Scholar] [CrossRef] [PubMed]
- Dalby, M.J.; Riehle, M.O.; Johnstone, H.; Affrossman, S.; Curtis, A.S. Investigating the limits of filopodial sensing: A brief report using SEM to image the interaction between 10 nm high Nano-topography and fibroblast Filopodia. Cell Biol. Int. 2004, 28, 229–236. [Google Scholar] [CrossRef] [PubMed]
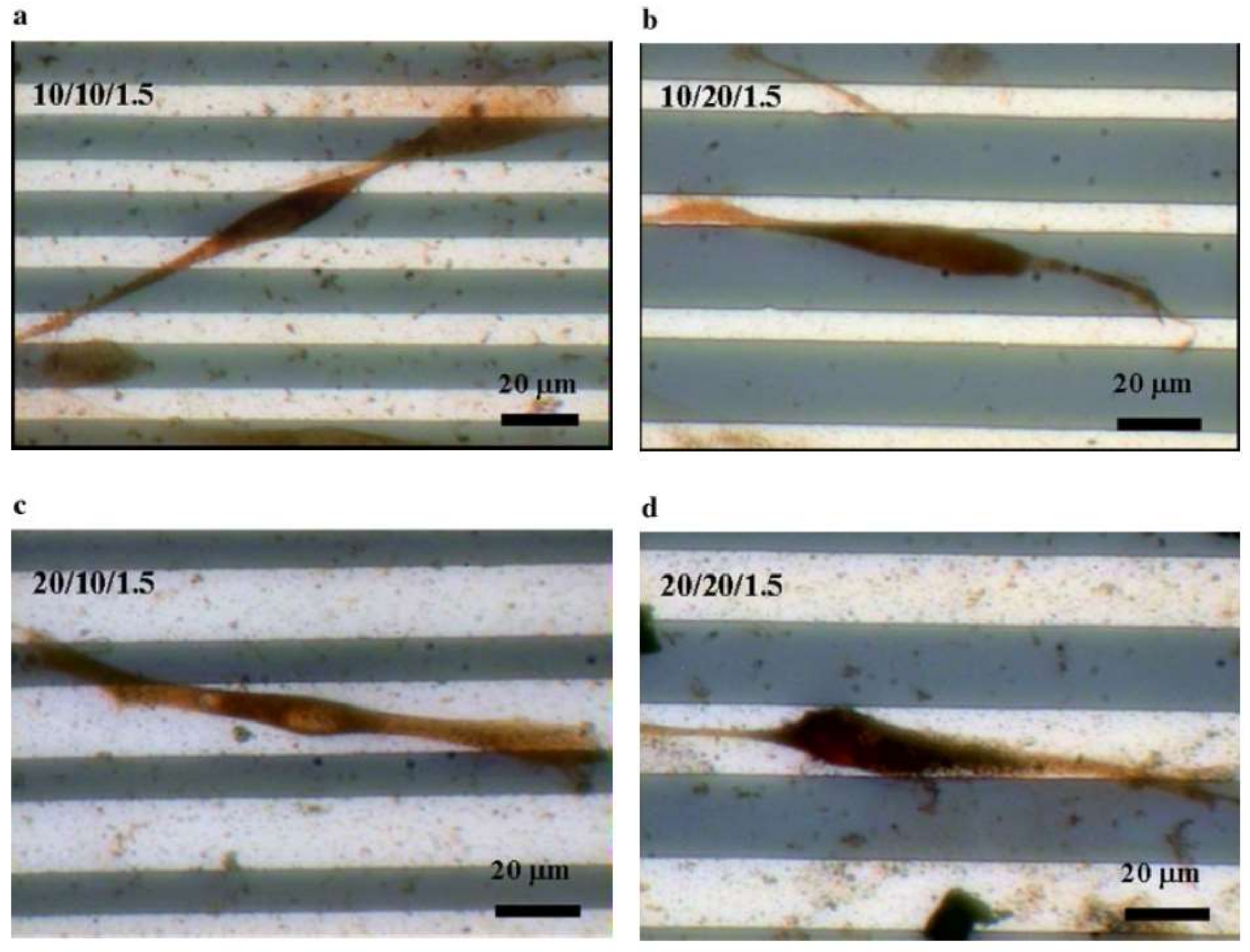
- Hsu, S.H.; Chen, C.Y.; Lu, P.S.; Lai, C.S.; Chen, C.J. Oriented Schwann cell growth on microgrooved surfaces. Biotechnol. Bioeng. 2005, 92, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Kyle, D.J.; Oikonomou, A.; Hill, E.; Bayat, A. Development and functional evaluation of biomimetic silicone surfaces with hierarchical micro/nano-topographical features demonstrates favourable in vitro foreign body response of breast-derived fibroblasts. Biomaterials 2015, 52, 88–102. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.; Hill, E.W.; Bayat, A. Development, fabrication and evaluation of a novel biomimetic human breast tissue derived breast implant surface. Acta Biomater. 2017, 49, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Sforza, M.; Zaccheddu, R.; Alleruzzo, A.; Seno, A.; Mileto, D.; Paganelli, A.; Sulaiman, H.; Payne, M.; Maurovich-Horvat, L. Preliminary 3-year evaluation of experience with Silksurface and Velvetsurface motiva silicone breast implants: A single-center experience with 5813 consecutive breast augmentation cases. Aesthet. Surg. J. 2017. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Nanotextured | Microtextured |
|---|---|---|
| Consistent surface roughness | 4000 nanometers on average (Ra) | 17 ± 3 µm |
| Median profile height (µm) | 13 ± 2 | 57 ± 15 |
| Kurtosis | 3.1 ± 0.4 | 2.6 ± 0.3 |
| Skewness | 0.4 ± 0.2 | 0.1 ± 0.2 |
| Contact angle * | 131° ± 4° | 119° ± 3° |
| Contact points per cm2 | 49,000 | 1800–2200 |
| Type of Method | Subtype | References |
|---|---|---|
| Systemic drugs | Antibiotics | [34,35] |
| Leukotriene antagonists | [36,37,38,39,40,41,42,43,44] | |
| Angiotensin-converting enzyme inhibitors | [45] | |
| Anti-fibrotics | [46,50] | |
| Colchicine | [51] | |
| Vitamin E | [54,58] | |
| Synthetic tryptophan metabolite | [59] | |
| Topical application | Anti-adhesion agents | [77,78] |
| Antibiotics | [66,67] | |
| Leukotriene antagonists | [78,79] | |
| Steroids | [81,82,83] | |
| Povidone-iodine | [64,65] | |
| 5-Fluorouracil | [72] | |
| Type A Botulinum toxin | [68,69] | |
| Hyaluronidase | [70,71] | |
| Mitomycin C | [73] | |
| Collagenase | [76] | |
| Synthetic tryptophan metabolite | [80] | |
| Halofuginone | [84] | |
| Colchicine | [89] | |
| Vitamin E | [90] | |
| Croton oil | [90] | |
| Nicotine | [91] | |
| Medical chitosan | [92] | |
| Materials | Combined with autologous tissue | [93,94,95,96,97] |
| Combined with acellular dermal matrix | [98,100,101,102] | |
| Surface types | Smooth and textured surfaces | [3,23,103,104,105,106,107,108,110,111] |
| Nano-micro modifications | [112,113,114,115,116,117,118,119,120,121] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.H.; Sutthiwanjampa, C.; Heo, C.Y.; Kim, W.S.; Lee, S.-H.; Park, H. Current Approaches Including Novel Nano/Microtechniques to Reduce Silicone Implant-Induced Contracture with Adverse Immune Responses. Int. J. Mol. Sci. 2018, 19, 1171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041171
Kang SH, Sutthiwanjampa C, Heo CY, Kim WS, Lee S-H, Park H. Current Approaches Including Novel Nano/Microtechniques to Reduce Silicone Implant-Induced Contracture with Adverse Immune Responses. International Journal of Molecular Sciences. 2018; 19(4):1171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041171
Chicago/Turabian StyleKang, Shin Hyuk, Chanutchamon Sutthiwanjampa, Chan Yeong Heo, Woo Seob Kim, Soo-Hong Lee, and Hansoo Park. 2018. "Current Approaches Including Novel Nano/Microtechniques to Reduce Silicone Implant-Induced Contracture with Adverse Immune Responses" International Journal of Molecular Sciences 19, no. 4: 1171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19041171