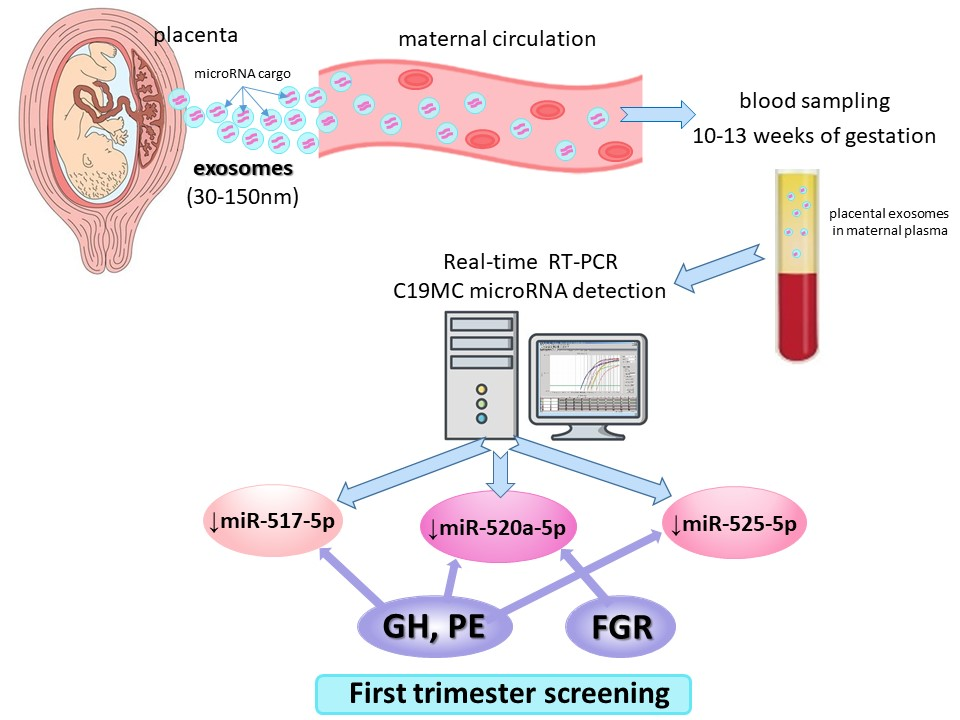
The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC microRNAs



Abstract
:
1. Introduction
2. Results
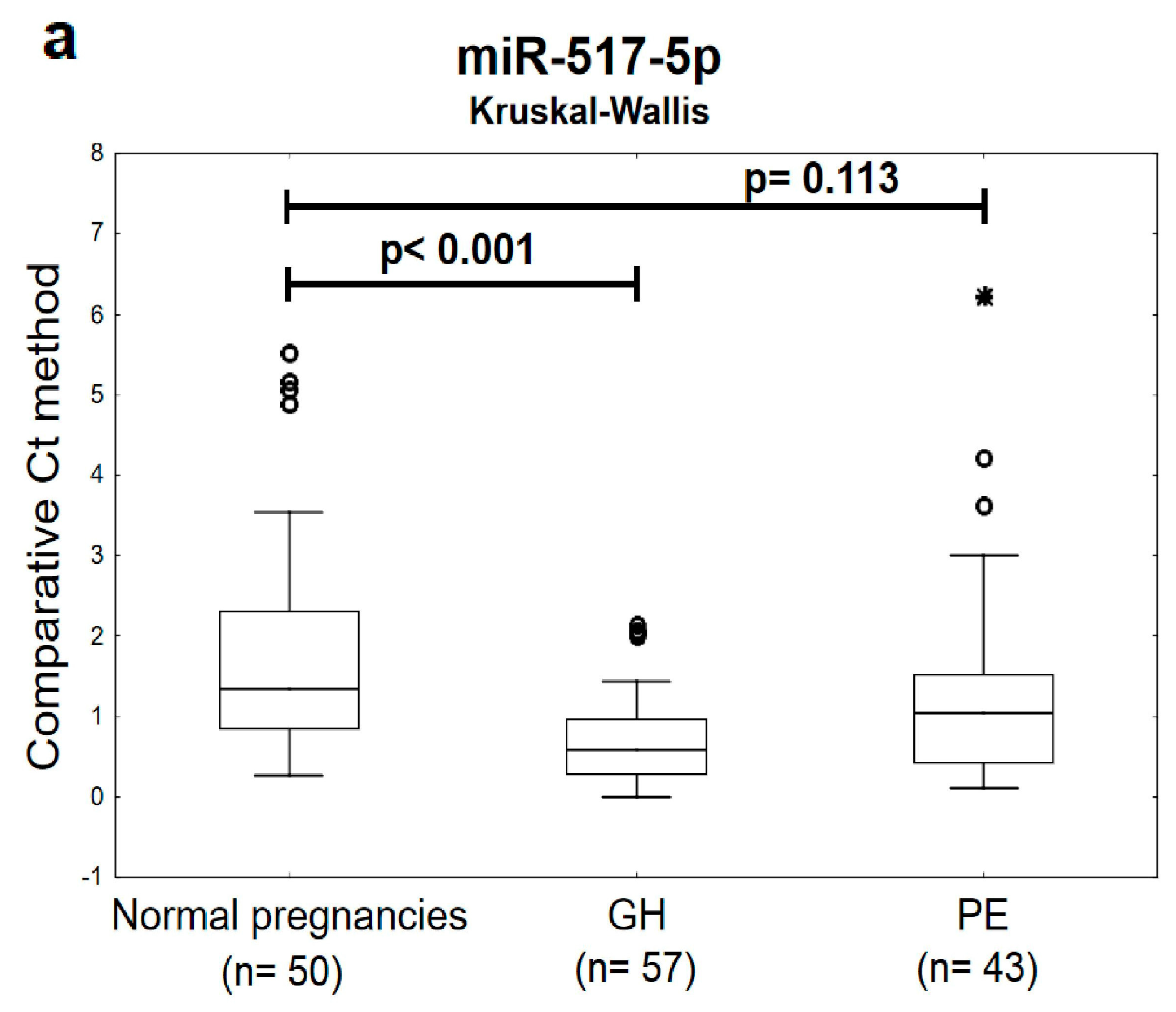
2.1. Plasma Exosomal miR-517-5p, miR-520a-5p and miR-525-5p are Down-Regulated during the First Trimester of Gestation in Women Affected with GH and PE
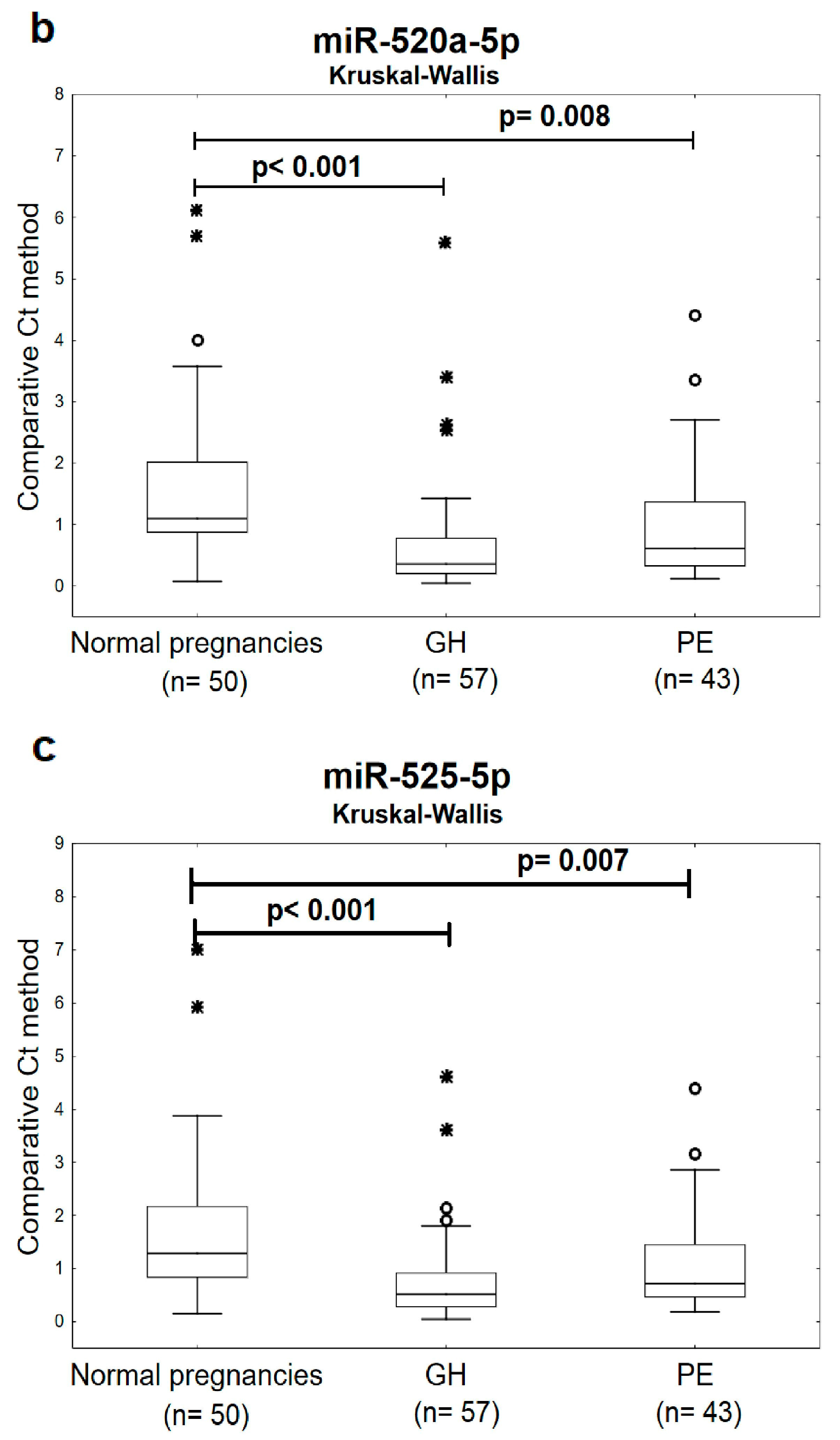
2.2. The High Accuracy of First Trimester C19MC MicroRNA Expression Profiling in Maternal Plasma Exosomes to Identify Women at a Risk of Later Development of GH or PE
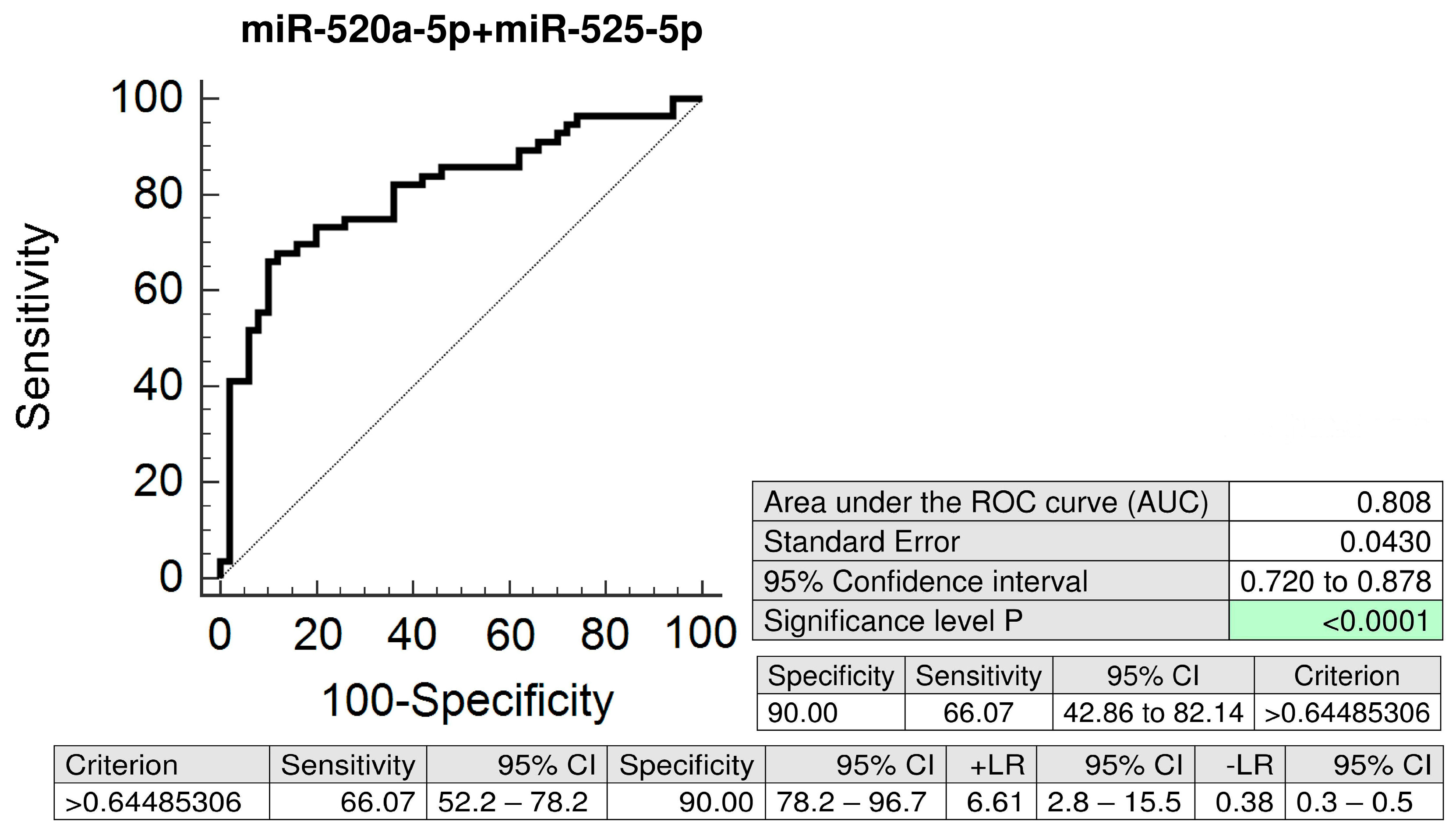
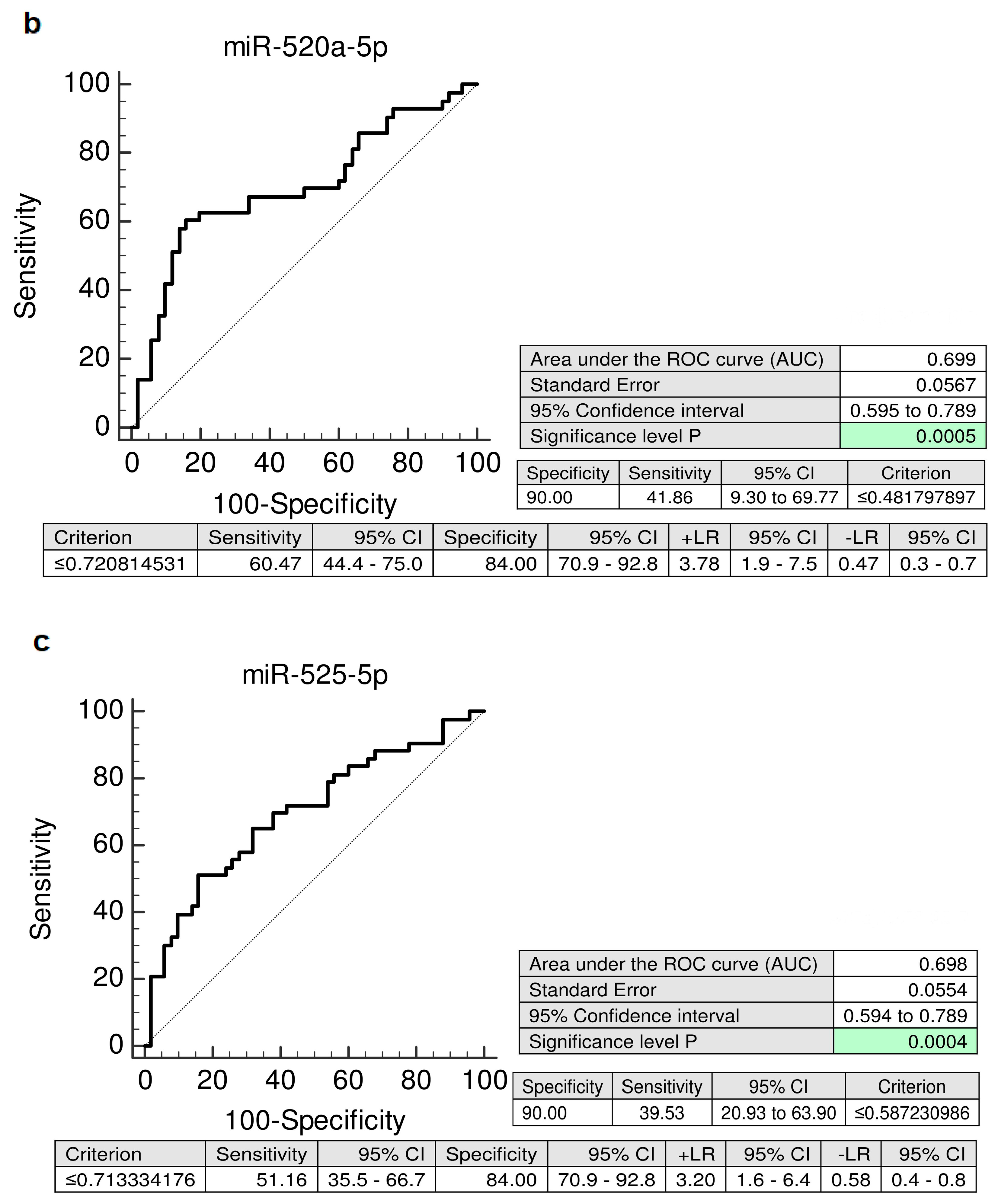
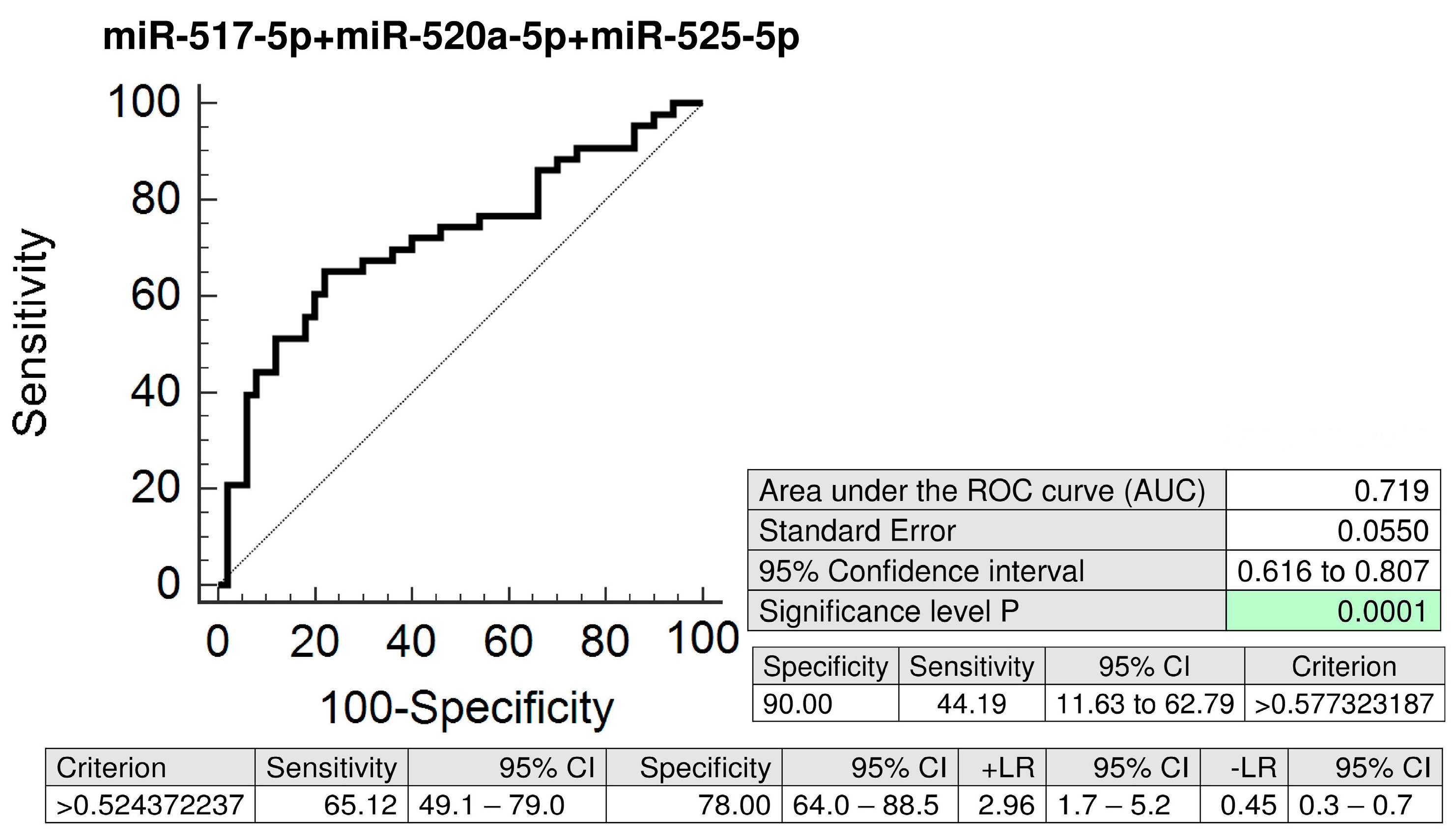
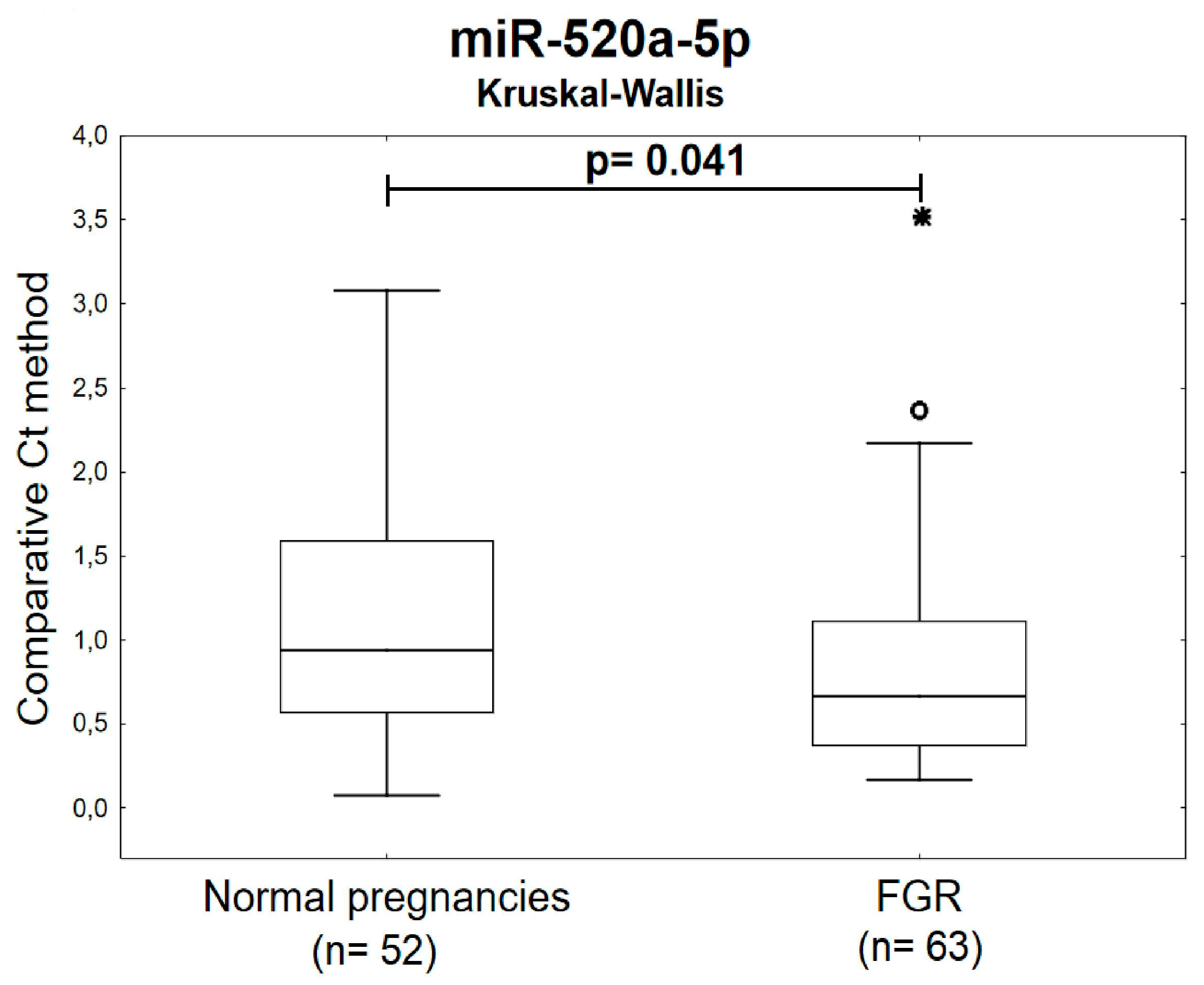
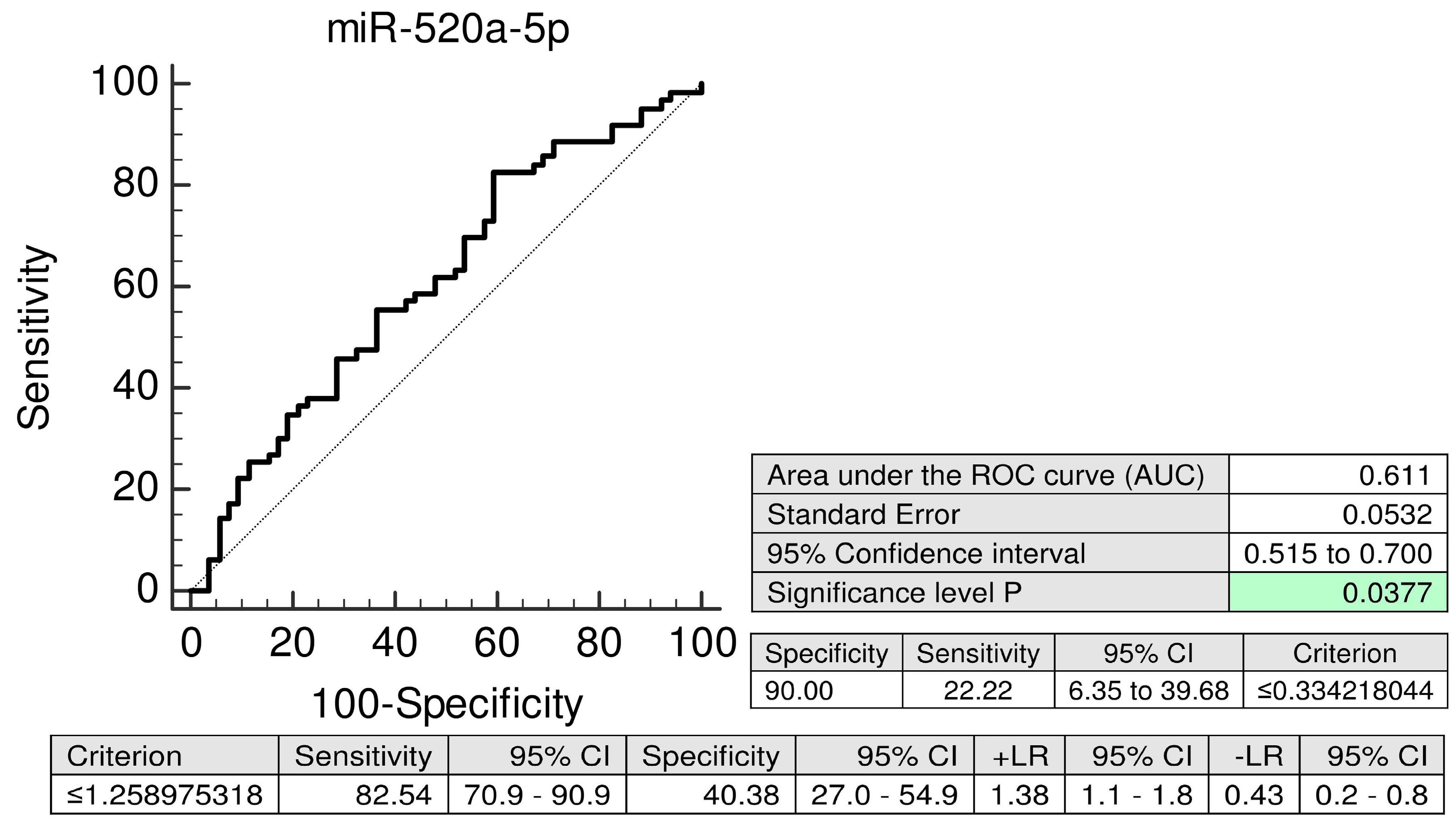
2.3. MiR-520a-5p Represents a Novel Maternal Plasma Exosome C19MC MicroRNA Biomarker for Prediction of Later Onset of FGR
3. Discussion
4. Materials and Methods
4.1. Patients Cohort
4.2. Processing of Samples
4.3. Isolation and Purification of Exosomes from Maternal Plasma Samples
4.4. Reverse Transcription Reaction
4.5. Quantification of Plasma Exosomal C19MC microRNAs by Real-Time PCR
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PE | Preeclampsia |
| FGR | Fetal growth restriction |
| GH | Gestational hypertension |
| C19MC | microRNA cluster on chromosome 19 |
| FGR | Fetal growth restriction |
| FPR | False positive rate |
| LR | Likelihood ratio |
| SE | Standard error |
| SD | Standard deviation |
| CPR | Cerebro-placental ratio |
| PI | Pulsatility index |
| EDTA | Ethylenediaminetetraacetic acid |
References
- Gunel, T.; Zeybek, Y.G.; Akçakaya, P.; Kalelioğlu, I.; Benian, A.; Ermis, H.; Aydınlı, K. Serum microRNA expression in pregnancies with preeclampsia. Genet. Mol. Res. 2011, 10, 4034–4040. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Lu, J.; Wang, S.; Li, H.; Ge, Q.; Lu, Z. Application of next-generation sequencing technology to profile the circulating microRNAs in the serum of preeclampsia versus normal pregnant women. Clin. Chim. Acta 2011, 412, 2167–2173. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Doucha, J.; Dlouha, K.; Krofta, L. Absolute and relative quantification of placenta-specific micrornas in maternal circulation with placental insufficiency-related complications. J. Mol. Diagn. 2012, 14, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhou, H.; Lin, H.; Qi, J.; Zhu, C.; Gao, Z.; Wang, H. Circulating microRNAs are elevated in plasma from severe preeclamptic pregnancies. Reproduction 2012, 143, 389–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hromadnikova, I.; Kotlabova, K.; Ondrackova, M.; Kestlerova, A.; Novotna, V.; Hympanova, L.; Doucha, J.; Krofta, L. Circulating C19MC microRNAs in preeclampsia, gestational hypertension, and fetal growth restriction. Mediat. Inflamm. 2013, 2013, 186041. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Hympanova, L.; Doucha, J.; Krofta, L. First trimester screening of circulating C19MC microRNAs can predict subsequent onset of gestational hypertension. PLoS ONE 2014, 9, e113735. [Google Scholar] [CrossRef] [PubMed]
- Ura, B.; Feriotto, G.; Monasta, L.; Bilel, S.; Zweyer, M.; Celeghini, C. Potential role of circulating microRNAs as early markers of preeclampsia. Taiwan J. Obstet. Gynecol. 2014, 53, 232–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, K.; Higashijima, A.; Murakami, Y.; Tsukamoto, O.; Hasegawa, Y.; Abe, S.; Fuchi, N.; Miura, S.; Kaneuchi, M.; Masuzaki, H. Circulating chromosome 19 miRNA cluster microRNAs in pregnant women with severe pre-eclampsia. J. Obstet. Gynaecol. Res. 2015, 41, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Ivankova, K.; Krofta, L. First trimester screening of circulating C19MC microRNAs and the evaluation of their potential to predict the onset of preeclampsia and IUGR. PLoS ONE 2017, 12, e0171756. [Google Scholar] [CrossRef]
- Wommack, J.C.; Trzeciakowski, J.P.; Miranda, R.C.; Stowe, R.P.; Ruiz, R.J. Micro RNA clusters in maternal plasma are associated with preterm birth and infant outcomes. PLoS ONE 2018, 13, e0199029. [Google Scholar] [CrossRef]
- Pillay, P.; Moodley, K.; Moodley, J.; Mackraj, I. Placenta-derived exosomes: Potential biomarkers of preeclampsia. Int. J. Nanomed. 2017, 12, 8009–8023. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Zhang, X.; Li, X. Exosomes derived from mesenchymal stem cells. Int. J. Mol. Sci. 2014, 15, 4142–4157. [Google Scholar] [CrossRef] [PubMed]
- Tomasetti, M.; Lee, W.; Santarelli, L.; Neuzil, J. Exosome-derived microRNAs in cancer metabolism: Possible implications in cancer diagnostics and therapy. Exp. Mol. Med. 2017, 49, e285. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Abdouh, M.; Arena, V.; Arena, M.; Arena, G.O. Reprogramming malignant cancer cells toward a benign phenotype following exposure to human embryonic stem cell microenvironment. PLoS ONE 2017, 12, e0169899. [Google Scholar] [CrossRef] [PubMed]
- Théry, C.; Zitvogel, L.; Amigorena, S. Exosomes: Composition, biogenesis and function. Nat. Rev. Immunol. 2002, 2, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Kalra, H.; Adda, C.G.; Liem, M.; Ang, C.S.; Mechler, A.; Simpson, R.J.; Hulett, M.D.; Mathivanan, S. Comparative proteomics evaluation of plasma exosome isolation techniques and assessment of the stability of exosomes in normal human blood plasma. Proteomics 2013, 13, 3354–3364. [Google Scholar] [CrossRef]
- Harding, C.V.; Heuser, J.E.; Stahl, P.D. Exosomes: Looking back three decades and into the future. J. Cell Biol. 2013, 200, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, M.D.; Peiris, H.N.; Kobayashi, M.; Koh, Y.Q.; Duncombe, G.; Illanes, S.E.; Rice, G.E.; Salomon, C. Placental exosomes in normal and complicated pregnancy. Am. J. Obstet. Gynecol. 2015, 213, S173–S181. [Google Scholar] [CrossRef]
- Kalluri, R. The biology and function of exosomes in cancer. J. Clin. Investig. 2016, 126, 1208–1215. [Google Scholar] [CrossRef]
- Kalluri, R.; LeBleu, V.S. Discovery of double-stranded genomic DNA in circulating exosomes. Cold Spring Harb. Symp. Quant. Biol. 2016, 81, 275–280. [Google Scholar] [CrossRef]
- Tkach, M.; Théry, C. Communication by extracellular vesicles: Where we are and where we need to go. Cell 2016, 164, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Salomon, C.; Guanzon, D.; Scholz-Romero, K.; Longo, S.; Correa, P.; Illanes, S.E.; Rice, G.E. Placental Exosomes as Early Biomarker of Preeclampsia: Potential Role of Exosomal MicroRNAs Across Gestation. J. Clin. Endocrinol. Metab. 2017, 102, 3182–3194. [Google Scholar] [CrossRef]
- Batista, I.A.; Melo, S.A. Exosomes and the Future of Immunotherapy in Pancreatic Cancer. Int. J. Mol. Sci. 2019, 20, 567. [Google Scholar] [CrossRef] [PubMed]
- Noguer-Dance, M.; Abu-Amero, S.; Al-Khtib, M.; Lefèvre, A.; Coullin, P.; Moore, G.E.; Cavaillé, J. The primate-specific microRNA gene cluster (C19MC) is imprinted in the placenta. Hum. Mol. Genet. 2010, 19, 3566–3582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augello, C.; Vaira, V.; Caruso, L.; Destro, A.; Maggioni, M.; Park, Y.N.; Montorsi, M.; Santambrogio, R.; Roncalli, M.; Bosari, S. MicroRNA profiling of hepatocarcinogenesis identifies C19MC cluster as a novel prognostic biomarker in hepatocellular carcinoma. Liver Int. 2012, 32, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Flor, I.; Bullerdiek, J. The dark side of a success story: microRNAs of the C19MC cluster in human tumours. J. Pathol. 2012, 227, 270–274. [Google Scholar] [CrossRef]
- Vaira, V.; Elli, F.; Forno, I.; Guarnieri, V.; Verdelli, C.; Ferrero, S.; Scillitani, A.; Vicentini, L.; Cetani, F.; Mantovani, G.; et al. The microRNA cluster C19MC is deregulated in parathyroid tumours. J. Mol. Endocrinol. 2012, 49, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Rippe, V.; Dittberner, L.; Lorenz, V.N.; Drieschner, N.; Nimzyk, R.; Sendt, W.; Junker, K.; Belge, G.; Bullerdiek, J. The two stem cell microRNA gene clusters C19MC and miR-371-3 are activated by specific chromosomal rearrangements in a subgroup of thyroid adenomas. PLoS ONE 2015, 5, e9485. [Google Scholar] [CrossRef]
- Kotlabova, K.; Doucha, J.; Hromadnikova, I. Placental-specific microRNA in maternal circulation—Identification of appropriate pregnancy-associated microRNAs with diagnostic potential. J. Reprod. Immunol. 2011, 89, 185–191. [Google Scholar] [CrossRef]
- Hromadnikova, I. Extracellular nucleic acids in maternal circulation as potential biomarkers for placental insufficiency. DNA Cell Biol. 2012, 31, 1221–1232. [Google Scholar] [CrossRef]
- Devor, E.; Santillan, D.; Scroggins, S.; Warrier, A.; Santillan, M. Trimester-specific plasma exosome microRNA expression profiles in preeclampsia. J. Matern. Fetal Neonatal Med. 2019, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hromadnikova, I.; Kotlabova, K.; Ondrackova, M.; Pirkova, P.; Kestlerova, A.; Novotna, V.; Hympanova, L.; Krofta, L. Expression profile of C19MC microRNAs in placental tissue in pregnancy-related complications. DNA Cell Biol. 2015, 34, 437–457. [Google Scholar] [CrossRef] [PubMed]
- Roberge, S.; Bujold, E.; Nicolaides, K.H. Aspirin for the prevention of preterm and term preeclampsia: Systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2018, 218, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Huang, R.; Zhang, J.; Ye, W.; Zhang, J. A prophylactic low-dose aspirin earlier than 12 weeks until delivery should be considered to prevent preeclampsia. Med. Hypotheses 2018, 121, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Rolnik, D.L.; Syngelaki, A.; de Paco Matallana, C.; Machuca, M.; de Alvarado, M.; Mastrodima, S.; Tan, M.Y.; Shearing, S.; Persico, N.; et al. Aspirin for Evidence-Based Preeclampsia Prevention trial: Effect of aspirin on length of stay in the neonatal intensive care unit. Am. J. Obstet. 2018, 218, 612.e1–612.e6. [Google Scholar] [CrossRef] [PubMed]
- Vayssière, C.; Sentilhes, L.; Ego, A.; Bernard, C.; Cambourieu, D.; Flamant, C.; Gascoin, G.; Gaudineau, A.; Grangé, G.; Houfflin-Debarge, V.; et al. Fetal growth restriction and intra-uterine growth restriction: Guidelines for clinical practice from the French College of Gynaecologists and Obstetricians. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 193, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Nawathe, A.; David, A.L. Prophylaxis and treatment of foetal growth restriction. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 49, 66–78. [Google Scholar] [CrossRef]
- Groom, K.M.; David, A.L. The role of aspirin, heparin, and other interventions in the prevention and treatment of fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S829–S840. [Google Scholar] [CrossRef] [Green Version]
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am. J. Obstet. Gynecol. 2000, 183, S1–S22. [CrossRef]
- Diagnosis and management of preeclampsia and eclampsia. ACOG Practice Bulletin No. 33. American College of Obstetricians and Gynecologists. Obstet. Gynecol. 2002, 99, 159–167.
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG Practice bulletin no. 134: Fetal growth restriction. Obstet. Gynecol. 2013, 121, 1122–1133. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, J.S.; Morris, R.K.; ter Riet, G.; Mol, B.W.; van der Post, J.A.; Coomarasamy, A.; Zwinderman, A.H.; Robson, S.C.; Bindels, P.J.; Kleijnen, J.; et al. Use of uterine artery Doppler ultrasonography to predict pre-eclampsia and intrauterine growth restriction: A systematic review and bivariable meta-analysis. Cmaj 2008, 178, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine Publications Committee; Berkley, E.; Chauhan, S.P.; Abuhamad, A. Doppler assessment of the fetus with intrauterine growth restriction. Am. J. Obstet. Gynecol. 2012, 206, 300–308, Erratum in Am. J. Obstet. Gynecol. 2015, 212, 246. Am. J. Obstet. Gynecol. 2012, 206, 508. [Google Scholar] [CrossRef] [PubMed]
- Gramellini, D.; Folli, M.C.; Raboni, S.; Vadora, E.; Merialdi, A. Cerebral-umbilical Doppler ratio as a predictor of adverse perinatal outcome. Obstet. Gynecol. 1992, 74, 416–420. [Google Scholar] [CrossRef]
- Arias, F. Accuracy of the middle-cerebral-to-umbilical-artery resistance index ratios in the prediction of neonatal outcome in patients at high risk for fetal and neonatal complications. Am. J. Obstet. Gynecol. 1994, 171, 1541–1545. [Google Scholar] [CrossRef]
- Arbeille, P.; Maulik, D.; Fignon, A.; Stale, H.; Berson, M.; Bodard, S.; Locatelli, A. Assessment of the fetal pO2 changes by cerebral and umbilical Doppler on lamb fetuses during acute hypoxia. Ultrasound Med. Biol. 1995, 21, 861–870. [Google Scholar] [CrossRef]
- Bahado-Singh, R.O.; Kovanci, E.; Jeffres, A.; Oz, U.; Deren, O.; Copel, J.; Mari, G. The Doppler cerebroplacental ratio and perinatal outcome in intrauterine growth restriction. Am. J. Obstet. Gynecol. 1999, 180, 750–756. [Google Scholar] [CrossRef]
- Fleischer, A.; Schulman, H.; Farmakides, G.; Bracero, L.; Blattner, P.; Randolph, G. Umbilical artery velocity waveforms and intrauterine growth retardation. Am. J. Obstet. Gynecol. 1985, 151, 502–506. [Google Scholar] [CrossRef]
- Soregaroli, M.; Bonera, R.; Danti, L.; Dinolfo, D.; Taddei, F.; Valcamonico, A.; Frusca, T. Prognostic role of umbilical artery Doppler velocimetry in growth-restricted fetuses. J. Matern. Fetal Neonatal Med. 2002, 11, 199–203. [Google Scholar] [CrossRef]
- Baschat, A.A.; Gembruch, U.; Weiner, C.P.; Harman, C.R. Qualitative venous Doppler waveform analysis improves prediction of critical perinatal outcomes in premature growth-restricted fetuses. Ultrasound Obstet. Gynecol. 2003, 22, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Seravalli, V.; Baschat, A.A. A uniform management approach to optimize outcome in fetal growth restriction. Obstet. Gynecol. Clin. N. Am. 2015, 42, 275–288. [Google Scholar] [CrossRef] [PubMed]
- Thaler, I.; Weiner, Z.; Itskovitz, J. Systolic or diastolic notch in uterine artery blood flow velocity waveforms in hypertensive pregnant patients: Relationship to outcome. Obstet. Gynecol. 1992, 80, 277–282. [Google Scholar] [PubMed]
- Park, Y.W.; Cho, J.S.; Kim, H.S.; Kim, J.S.; Song, C.H. The clinical implications of early diastolic notch in third trimester Doppler waveform analysis of the uterine artery. J. Ultrasound Med. 1996, 15, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group 1 (n = 50) | Control Group 2 (n = 52) | PE (n = 43) | FGR (n = 63) | GH (n = 57) | p-Value | |
|---|---|---|---|---|---|---|
| At sampling | ||||||
| Maternal age (years); mean ± SE | 31.88 ± 0.56 | 31.21 ± 0.56 | 32.34 ± 0.73 | 33.42 ± 0.57 | 32.15 ± 0.63 | - |
| median (range) | 32 (23–39) | 31 (23–41) | 31 (23–46) | 33 (22–44) | 32 (22–42) | - |
| Gestational age (weeks); mean ± SE | 10.69 ± 0.14 | 10.40 ± 0.08 | 10.82 ± 0.18 | 10.37 ± 0.07 | 10.84 ± 0.13 | - |
| median (range) | 10.29 (9.86–13.71) | 10.29 (10.0–13.43) | 10.29 (9.86–13.86) | 10.29 (9.86–13.29) | 10.43 (9.71–14.0) | - |
| At delivery | ||||||
| Gestational age (weeks); mean ± SE | 40.11 ± 0.11 | 39.75 ± 0.15 | 36.0 ± 0.49 | 36.68 ± 0.30 | 39.32 ± 0.16 | PE vs. Control group1; p < 0.001 FGR vs. Control group2; p < 0.001 |
| median (range) | 40.29 (37.71-42.0) | 40.0 (37.29–41.86) | 36.71 (28.0–40.71) | 37.29 (28.29–40.29) | 39.14 (36.0–41.71) | PE vs. Control group1; p < 0.001 FGR vs. Control group2; p < 0.001 |
| Blood pressure (mmHg) | ||||||
| Systolic; mean ± SE | 122.06 ± 1.58 | 122.05 ± 1.74 | 154.2 ± 2.04 | 124.91 ± 2.27 | 148.97 ± 2.42 | PE vs. Control group1; p < 0.001 GH vs. Control group1; p < 0.001 |
| median (range) | 120 (100–142) | 120 (90–148) | 150 (133–186) | 125 (86–177) | 150 (107–200) | PE vs. Control group1; p < 0.001 GH vs. Control group1; p < 0.001 |
| Diastolic; mean ± SE | 76.28 ± 0.94 | 77.64 ± 1.28 | 99.74 ± 1.38 | 79.7 ± 1.56 | 92.75 ± 1.43 | PE vs. Control group1; p < 0.001 GH vs. Control group1; p < 0.001 |
| median (range) | 76 (65–88) | 78 (58–93) | 100 (80–120) | 80 (59–109) | 95 (70–114) | PE vs. Control group1; p < 0.001 GH vs. Control group1; p < 0.001 |
| Fetal birth weight (grams); mean ± SE | 3521.02 ± 47.32 | 3476.42 ± 46.33 | 2551.90 ± 143.12 | 2179.46 ± 60.72 | 3503.87 ± 64.55 | PE vs. Control group1; p < .001 FGR vs. Control group2; p < 0.001 |
| median (range) | 3520 (2780–4240) | 3440 (2690–4290) | 2565 (930–4460) | 2260 (746–3230) | 3480 (2510–4670) | PE vs. Control group1; p < 0.001 FGR vs. Control group2; p < 0.001 |
| Mode of delivery | ||||||
| Vaginal | 36 (72.0%) | 43 (82.69%) | 7 (16.28%) | 16 (25.4%) | 36 (71.93%) | PE vs. Control group1; p < 0.001 FGR vs. Control group2; p < 0.001 |
| CS | 14 (28.0%) | 9 (17.31%) | 36 (83.72%) | 47 (74.6%) | 16 (28.07%) | PE vs. Control group1; p < 0.001 FGR vs. Control group2; p < 0.001 |
| Fetal sex | ||||||
| Boy | 20 (40.0%) | 27 (51.92%) | 19 (44.19%) | 32 (56.14%) | 30 (47.62%) | - |
| Girl | 30 (60.0%) | 25 (48.08%) | 24 (55.81%) | 25 (43.86%) | 33 (52.38%) | - |
| Primiparity | ||||||
| Yes | 21 (42.0%) | 31 (59.62%) | 33 (76.74%) | 35 (61.4%) | 38 (60.32%) | - |
| No | 20 (58.0%) | 21 (40.38%) | 10 (23.26%) | 22 (38.6%) | 25 (39.68%) | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hromadnikova, I.; Dvorakova, L.; Kotlabova, K.; Krofta, L. The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC microRNAs. Int. J. Mol. Sci. 2019, 20, 2972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20122972
Hromadnikova I, Dvorakova L, Kotlabova K, Krofta L. The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC microRNAs. International Journal of Molecular Sciences. 2019; 20(12):2972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20122972
Chicago/Turabian StyleHromadnikova, Ilona, Lenka Dvorakova, Katerina Kotlabova, and Ladislav Krofta. 2019. "The Prediction of Gestational Hypertension, Preeclampsia and Fetal Growth Restriction via the First Trimester Screening of Plasma Exosomal C19MC microRNAs" International Journal of Molecular Sciences 20, no. 12: 2972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20122972