Blood Platelet Adenosine Receptors as Potential Targets for Anti-Platelet Therapy


Department of Haemostasis and Haemostatic Disorders, Chair of Biomedical Science, Medical University of Lodz, 92-215 Lodz, Poland
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2019, 20(21), 5475; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20215475
Submission received: 30 September 2019
/
Revised: 31 October 2019
/
Accepted: 1 November 2019
/
Published: 3 November 2019
(This article belongs to the Special Issue G Protein-Coupled Adenosine Receptors: Molecular Aspects and Beyond)
Abstract
:Adenosine receptors are a subfamily of highly-conserved G-protein coupled receptors. They are found in the membranes of various human cells and play many physiological functions. Blood platelets express two (A2A and A2B) of the four known adenosine receptor subtypes (A1, A2A, A2B, and A3). Agonization of these receptors results in an enhanced intracellular cAMP and the inhibition of platelet activation and aggregation. Therefore, adenosine receptors A2A and A2B could be targets for anti-platelet therapy, especially under circumstances when classic therapy based on antagonizing the purinergic receptor P2Y12 is insufficient or problematic. Apart from adenosine, there is a group of synthetic, selective, longer-lasting agonists of A2A and A2B receptors reported in the literature. This group includes agonists with good selectivity for A2A or A2B receptors, as well as non-selective compounds that activate more than one type of adenosine receptor. Chemically, most A2A and A2B adenosine receptor agonists are adenosine analogues, with either adenine or ribose substituted by single or multiple foreign substituents. However, a group of non-adenosine derivative agonists has also been described. This review aims to systematically describe known agonists of A2A and A2B receptors and review the available literature data on their effects on platelet function.
1. Introduction
Activation of blood platelets plays a critical role in the pathogenesis of arterial thrombotic diseases, such as coronary heart disease, myocardial infarction, and stroke, which are the primary cause of mortality in developed countries. Therefore, anti-platelet therapy is one of the most important tools in the treatment of arterial thrombotic disorders [1].
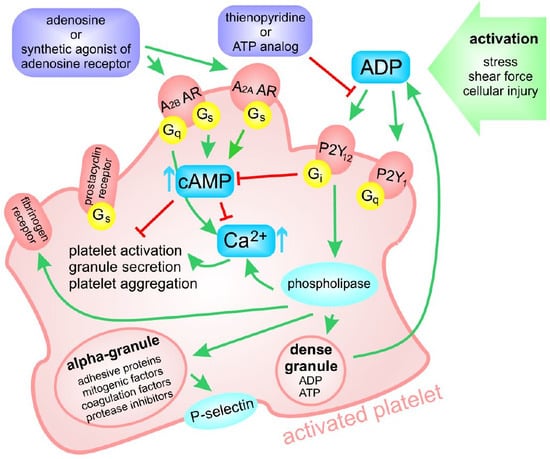
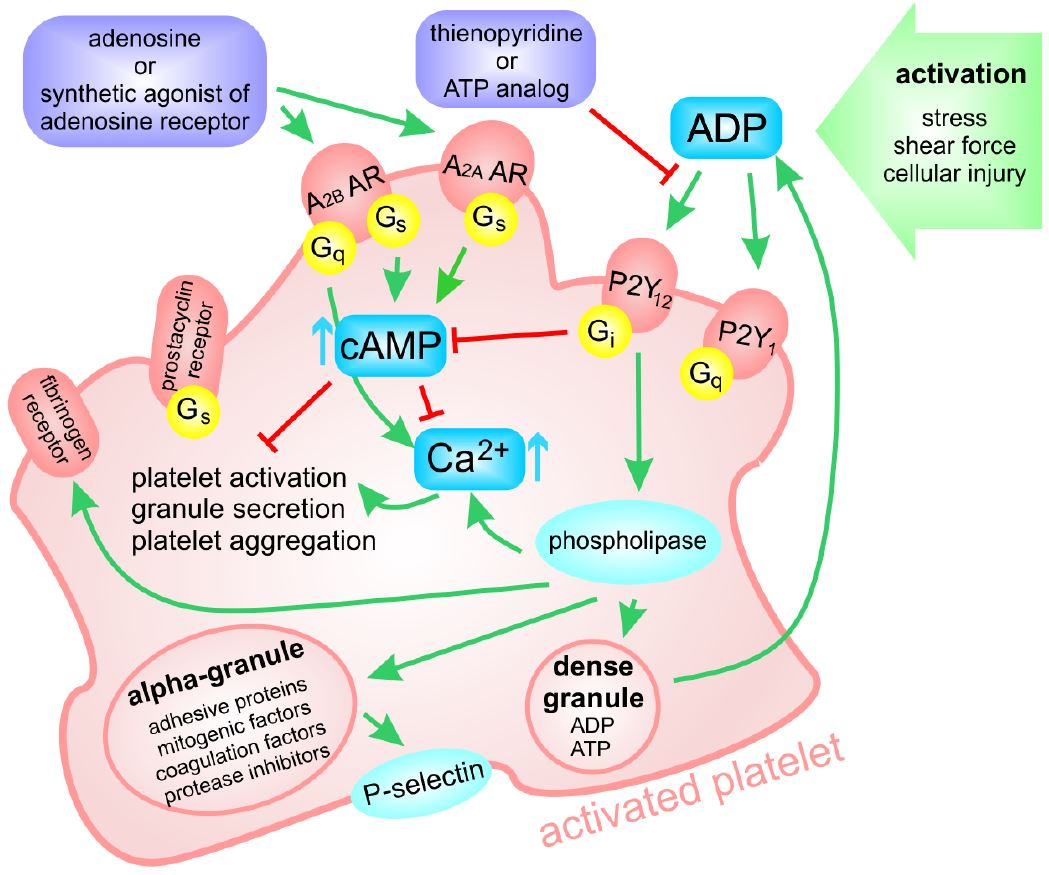
Platelets express two receptors for ADP: The P2Y1 receptor, which initiates platelet aggregation, and the P2Y12 receptor, which enhances this process, finally leading to thrombus formation. In contrast to the P2Y1 receptor, the P2Y12 receptor is almost exclusively expressed in the platelet plasma membrane. Therefore, P2Y12 has become a major therapeutic target to prevent arterial thrombotic disorders instead of adenosine receptors [2]. In general, the major clinically approved P2Y12 inhibitors include the thienopyridine-class inhibitors (ticlopidine, clopidogrel, and prasugrel), the ATP analogue—cangrelor, and the cyclo-pentyl-triazolo-pyrimidine (CPTP)—ticagrelor [2,3]. Thienopyridines are prodrugs that are converted to short-living active metabolites; these irreversibly inactivate the receptor and consequently inhibit ADP-induced platelet activation. Cangrelor is the first intravenous P2Y12 receptor inhibitor to reversibly block ADP signaling in a non-competitive manner. Ticagrelor is an allosteric antagonist of P2Y12, acting directly via reversible binding to the P2Y12 receptor, which leads to the non-competitive inhibition of ADP-induced P2Y12 activation and is used for the prevention of thromboembolic events in patients with acute coronary syndromes [2,3,4,5]. As regards current clinical practice, clopidogrel, prasugrel, and ticagrelor are the most frequently used oral platelet P2Y12 inhibitors; the use of ticlopidine has been abandoned. Clopidogrel is the only oral P2Y12 inhibitor recommended for the treatment of patients with stable coronary artery disease. Although all three agents have an indication for use in acute coronary syndromes, current guidelines suggest the preferential use of prasugrel and ticagrelor over clopidogrel because of their superior clinical benefits, i.e., the improved efficacy, lowered individual variation in response, and less frequent and severe side effects [6]. Cangrelor, in turn, as the recently approved, first P2Y12 inhibitor administered intravenously, seems to be the most promising in percutaneous coronary interventions [7].
Although these anti-platelet agents are now commonly used as clinically approved drugs, effective therapy of arterial thrombosis still presents a problem. For example, gastrointestinal bleeding is a common adverse event observed in 5 to over 10% of patients treated with oral anti-platelet drugs. Many of the patients with this complication require recurrent hospitalization [8]. Another severe and relatively common side effect of anti-platelet therapy is a higher risk of intracranial and intracerebral hemorrhage [9]. On the other hand, for some patients, the applied anti-platelet therapy appears insufficient and does not prevent excessive clotting. This can be explained by the fact that anti-platelet agents either interfere with only one out of several pathways of platelet activation or, even if they block effectively a final common step of platelet aggregation, such as fibrinogen binding (blockers of fibrinogen receptor), their use is associated with a risk of bleeding [3]. Another problem affecting the efficiency of many anti-platelet drugs stems from the individual variability of the response to these drugs resulting from both environmental and genetic factors, especially in case of prodrugs [10]. Altogether, there still is a need for the development of novel platelet inhibitors with better efficacy and safety, or using a combined therapy based on various sets of currently-available agents.
Adenosine is an important purine metabolite, serving not only as a component of nucleic acids and the most important energy carrier in the cell—ATP—but also as a signaling molecule regulating tissue function [11,12]. Adenosine receptors (AR) are present in membranes of many types of human cells and play various physiological functions. Blood platelets express two (A2A and A2B) of the four known adenosine receptor subtypes (A1, A2A, A2B, and A3). As regards platelet AR receptors, A2A is characterized by the higher affinity to adenosine in comparison with A2A; furthermore, platelets have a significantly lower density of A2B [13,14]. Activation of platelet AR results in an enhanced intracellular cAMP level and consequently leads to the inhibition of platelet activation and aggregation [15,16]. Therefore, adenosine receptors A2A and A2B could be considered as targets for anti-platelet therapy, especially under circumstances when classic therapy based on antagonizing the P2Y12 purinergic receptor is insufficient or problematic.
The aim of this review is to systematically present current knowledge of the impact of synthetic, selective, longer-lasting agonists of A2A and A2B receptors on platelet function inhibition, and evaluate their potential as anti-platelet therapeutics.
2. The Classification, Distribution, and Signaling of Adenosine Receptors
Adenosine receptors (AR) represent a subfamily of highly-conserved G-protein coupled receptors. They are found in membranes of various human cells and play a plethora of physiological functions. Four AR subtypes are known: A1, A2A, A2B, and A3. The A1 and A3 receptors preferentially couple to Gi protein to inhibit adenylate cyclase and, consequently, the production of cyclic AMP (cAMP). The A2A and A2B subtypes stimulate the production of cAMP by coupling to Gs or Go protein [17]; they are therefore classified as adenylyl cyclase inhibiting (A1 and A3) or adenylyl cyclase activating (A2A and A2B) [18].
AR subtypes are characterized by high resemblance in terms of amino acid sequence: The human A1 and A3 ARs are identical in 49%, whereas human A2A and A2B AR sequences are identical in 59%. In general, an AR molecule consists of a single polypeptide chain that transverses the membrane from the extracellular side, beginning at the N terminus and forming seven transmembrane helices [15]. AR receptors are commonly expressed in many tissues and cells types; however, the distribution of subtypes is highly tissue-specific (Table 1).
Adenosine receptors play multiple functions. A2A receptor agonization is known to cause coronary artery vasodilatation, decreased dopaminergic activity in central nervous system, and inhibition of central neuron excitation, whereas A2B receptor activation may cause bronchospasm [12,24,25,26]. Therefore, all adenosine receptor ligands should be used only with the utmost caution [11], despite some having already been approved for human use (one of them—regadenoson—is discussed further in this article). An interesting insight into adenosine receptor overstimulation may be gained from the study of adenosine deaminase deficiency—a rare, autosomal metabolic disorder that causes severe combined immunodeficiency [27]. In this syndrome, platelet dysfunction has been described, as well as severe thrombocytopenia [28,29]. It is, however, important to remember that there is no exact parallel between patients with this syndrome and an anti-platelet therapy with the use of AR agonists. The dose of synthetic adenosine agonist equivalent to adenosine would be much lower and, most importantly, it would be applied in adults.
As it has been already mentioned, blood platelets express two subtypes of AR receptors (A2A and A2B); however, the expression (the number of receptor copies in the plasma membrane) of the two receptor types has not been established. A2A receptor is believed to be expressed on platelets in higher density as compared to A2A [18]. Only one study has estimated the gene expression profile for A2A and A2B in human platelets. This report demonstrated comparable mRNA expression levels for A2A and A2B AR [22], but no further evidence exists regarding protein levels present on the platelet surface. Moreover, two studies [30,31] have not been able to quantify A2A AR in platelet proteome, while have easily identified, for example, P2Y12 receptor, expressed on healthy platelets in around 450–1000 copies [32].
A2A AR was identified as an important receptor on platelets and a mediator of adenosine inhibition of platelet aggregation [33]. This is achieved through inhibition of mobilization of internal calcium stores and influx of external calcium, both associated with activation of adenylate cyclase and increase of cAMP concentration [34]. Cyclic nucleotides are also strong inhibitors of the release of calcium ions into the cytosol, which underpins many events in platelet activation. In addition to inhibiting platelet aggregation in human blood, the activation of A2A AR by specific agonists leads to a reduction in P-selectin expression on the platelet cell surface, as a result of thromboxane A2 or ADP stimulation [15].
Phenotypically, counts of blood cell populations, including platelets, were found to be similar in A2A AR knock-out mice and with wild-type mice [20]. In this knock-out model, the rate of ADP-induced platelet aggregation differed in both the genetic variants following the treatment with nonselective AR agonist, 5′-N-ethyl-carboxamidoadenosine (NECA). NECA administration led to inhibition of platelet aggregation in wild-type mice, but demonstrated no effect in A2A AR-null mice [35].
The role of A2B AR in platelets remains disputable. It was proposed that this AR subtype activates signal transduction pathways other than adenylate cyclase [36]. It was also proposed, based on a mouse knock-out study, that A2B AR is upregulated under stress in vivo, and plays a significant role in regulating ADP receptor expression [23]. The same study also found that agonization of this receptor inhibits agonist-induced platelet aggregation, but it should be noted that no specific agonist was used: A combination of a non-selective agonist and A2A receptor inhibitor was applied.
The half-life of adenosine in circulation is extremely short (approximately 1 s), due to the action of enzymes like adenosine deaminase, which convert it to inosine, or adenosine kinase, which phosphorylates it to 5′-AMP, or due to uptake by nucleoside transporters [33]. Therefore, close study and pharmacological potential of ARs can be facilitated only by finding longer-lasting synthetic agonists and antagonists.
3. Adenosine Receptor Agonists—Structure, Chemical Properties, and Known Effects on Platelet Function
The purpose of synthesizing novel AR agonists is to achieve longer-lasting agonization and selectivity between receptor subtypes without compromising high affinity of binding to the receptor. This is accomplished, with varying success, either by introducing additional substituents to the molecule of adenosine in the hope of improving a receptor-ligand binding, or by utilizing molecules of other chemical structure. A nomenclature and the chemical structure of AR agonists is presented in Table 2.
3.1. Adenosine Derivatives
Numerous adenosine-derived compounds have been tested for their affinity and selectivity for ARs. The most prevalent strategies for obtaining novel derivatives were substitutions of adenosine at the 2-position, usually with (thio)ethers, secondary amines, and alkynes, as well as at the N6-position. The latter substitutions appear to increase affinity to the A2A receptor subtype [37]. Below, we present an overview of adenosine derivatives classified according to the position of substituents. It is, however, important to point out that the citied study was performed using various protocols and utilizing nonhomogeneous materials, hence is not possible to make a direct comparison between available data, for example for IC50 or EC50 measured for various AR agonists.
3.1.1. Adenosine Derivatives with Substituents at C1 to C8 Positions
2-chloroadanosine
2-chloroadenosine is one of the first characterized AR agonists, first described in 1964 [38,39]. Conducted studies were predominantly concentrated on its effect on platelets, from the pioneering research into activation signaling [40,41], including recognition of AR subtypes [42], through examination of platelet disorders [43,44], to investigations of 2-chloroadenosine antiaggregatory effects [45].
IC50 of 2-chloroadenosine for human platelets was established at 1.6 µM (CI95% 0.61–4.4) (by photometric method in PRP (platelet rich plasma) with ADP), while its EC50 was found to be 1.7 µM in adenylate cyclase assay using human platelet membranes (CI95% 1.5–2.0) [46]. For aggregation in whole blood, IC50 was later measured to be 2.3 µM [47]. 2-chloroadenosine is a non-selective AR agonist, with high affinity, especially to A1 and A2 AR classes [48,49]. Nowadays, it is employed in numerous research areas as a stable adenosine analogue [50,51,52,53]. Its advantage over the adenosine arises from the fact that 2-chloroadenosine has a longer half-time and exerts more potent activating effect on AR (A2A receptor biding affinity Ki = 180 nM), being only minimally different chemically [54].
Regadenoson
Regadenoson is also commonly denoted as CVT-3146 and known under its trade names Lexiscan or Rapiscan. It is a selective A2A AR agonist of low affinity (Ki = 1095 nM). It also binds to A1 receptor subtype (Ki > 16,460 nM), but has much higher affinity constants in the case of A2B and A3 receptor classes [55]. It was approved by the Food and Drug Administration (FDA) in 2008 for diagnostic purposes in radionuclide myocardial perfusion imaging, manufactured by Astellas Pharma and marketed by GE Healthcare. It is administered intravenously in bolus as a 0.08 mg/mL solution. Regadenoson rapidly increases coronary blood flow to over twice the baseline value in 30 s and decreases to below twice the baseline value in 10 min, and is removed from the human body (58% through renal excretion) within two hours [56] (clinical studies: NCT01019486 (RABIT1D) and NCT00881218). The influence of regadenoson on platelet aggregation has not been reported in literature so far. However, our unpublished results (manuscript currently under review) have confirmed that regadenoson has an anti-platelet effect—in whole blood aggregation, the obtained maximal inhibition value was of 38.1 ± 3.2%, and IC50 of 1.2 µM.
Binodenoson
Binodenoson is another AR agonist currently approved for human use. It was firstly reported in the literature in 1996 under the name WRC-0470 as a short-acting A2A agonist [57], then a year later, it was presented as a potential imaging tool [58]. Subsequently, it was tested specifically for induction of pharmacological stress as an adjunct to myocardial perfusion imaging. Its pharmacokinetics and safety profile were tested in clinical trials [59,60,61]. Binodenoson has successfully completed two phase III clinical trials (identifiers NCT00944294 and NCT00944970) and is currently used as a single bolus injection prior to myocardial perfusion imaging.
It is characterized with good selectivity for A2A AR receptor over other AR receptors, and good binding affinity (Ki = 270 nM) [62]. Despite being well characterized concerning general safety, no data concerning platelets or its potential anti-platelet effect are available.
PSB Family
PSB-0777 was developed in PharmaCenter Bonn, and described in 2011 as a potential anti-inflammatory agent for a treatment of inflammatory bowel disease [63]. Despite it being a polar and water-soluble substance, it is not absorbable when administered per os, but suitable for parenteral application only. It was determined to be a full A2A agonist, of high affinity (Ki = 44.4 nM) and high selectivity (over 225-fold) over other ARs. The compound exhibits affinity for both human and rat A2A. In cAMP accumulation assay using CHO cells expressing the A2A receptor, EC50 was established at 117 nM. PSB-0777 was successfully utilized as an A2A receptor agonist in a study concerning activation of brown adipose tissue [64]. It has yet to be investigated in the context of blood platelets.
A recent study reported the anti-platelet effects of three other recently-synthesized compounds from this family: PSB-15826, PSB-12404, and PSB-16301 [65,66,67,68]. PSB-15826 was found to be the most potent agonist out of these three compounds, characterized by IC50 values of 0.32 ± 0.05 µM for inhibition of platelet aggregation, 0.062 ± 0.2 µM for inhibition of platelet activation, and 0.24 ± 0.01 µM for cAMP production, making it a stronger anti-platelet agent than adenosine. PSB-16301 has also effectively reduced ADP-induced platelet aggregation with relatively low IC50 of 5.5 ± 0.2 µM, as well as PSB-12404, though at higher concentration: IC50 of 66.8 ± 0.07 µM [68]. Other members of this family were also described in the literature. They are either very weak AR agonists, or even AR inhibitors.
There are no data available on the cytotoxicity of this group of compounds; however, success in identifying multiple members of this family with anti-platelet properties suggests a high chance for finding an analogue with good safety profile.
MRE0094
MRE0094 is also known and marketed under names Sonedenoson and 2-[2-(4-chlorophenyl)ethoxy]adenosine. It is 39,000-fold more selective for adenosine A2 receptors than adenosine A1 receptors, with Ki for A2 AR subtype established at 490 nM [69]. It was successfully utilized as an A2A selective compound in cell signaling research focused on varying topics [70,71,72], but most promising investigations concentrated on its use in promoting wound healing [73,74]. In early 2000, it was being developed by King Pharmaceuticals with hopes of becoming a novel topical drug.
MRE0094 was tested in two Phase II clinical trials concerning wound healing in chronic, neuropathic, diabetic foot ulcers, both of them sponsored by Pfizer. The first trial (ClinicalTrials.gov Identifier: NCT00312364) was completed in 2006; however, no results are available. The second study (ClinicalTrials.gov Identifier: NCT00318214) has been terminated due to poor enrolment of participants. According to King Pharmaceuticals, MRE0094 did not show expected improvement over selected reference for the clinical endpoints. MRE0094 has not been examined for its anti-platelet activity to date.
CV1808
CV1808 is also sometimes denoted as 2-phenylaminoadenosine. It is one of the first characterized AR agonists that was utilized in studies aiming to define AR subclasses [75,76,77]. CV1808 is a non-selective agonist, with Ki values of 560–1100 nM for A1, and 190 nM for A2A [78]. It was later reported that A2B Ki is similarly low to that of A2A AR subtype [79].
AMP597
AMP597 was first described by Smits et al. in 1998 as a novel cardioprotective A1/A2 agonist [85]. It has high affinity for the A1 (Ki = 2 nM) and A2A (Ki = 56 nM) receptor subtypes [86] and was later determined to be an A2B agonist as well, based on the observation of its ability to induce phosphorylation of extracellular signal-regulated kinase and its protection against infarction in rabbit heart reperfusion studies [87]. It could be regarded, therefore, as a potent but non-selective AR agonist.
It has not been extensively studied; although it has been the subject of cardiac protection studies, a lack of publications since 2010 suggests that this line of research has been abandoned, despite the fact that it was undergoing clinical phase II studies in patients suffering acute myocardial infarction in 2000 [86]. Its effect on platelets remains unknown.
3.1.2. Adenosine Derivatives with Substituents at C1′ to C5′ Positions
NECA
5’-N-ethylcarboxamidoadenosine, commonly abbreviated as NECA, was first described in 1977 as a vasodilator, and then as a platelet function inhibitor in the 1980s [88]. NECA was employed in early radioligand studies to characterize AR platelet receptors, and was established to bind to two distinct binding sides at submicromolar concentrations [89,90].
NECA IC50 for platelet aggregation in human material was established at 0.36 µM (CI95% 0.35–0.38 µM) [91]. Ki for human AR subtypes were set at 560 nM (480–650 nM) for A1, 620 nM (300–1300 nM) for A2A, and 6.2 nM (5.1–7.5 nM) for A3, showing a lack of selectivity between A2A and A1 receptor subtypes [92]. However, it was described as a suitable A2B agonist, with IC50 of 3.1 μM (cAMP production in CHO cells) [93].
NECA has no current medical applications and has never been a subject of clinical testing. It is most commonly used in basic, platelet and vascular, and neurological research.
3.1.3. Compounds with Substituents at C1 to C8 and C1′ to C5′ Positions
CGS 21680
CGS 21,680 is one of the earliest synthesized adenosine analogue AR agonists. It was primarily used to elucidate the AR subclass division into A2A and A2B [76,94]. It is a strong, full agonist, selective towards A2A (Ki A2A = 27 nM, Ki A2B is over1000 nM) [95]. It is probably the most commonly-employed AR A2A agonist; it is used through a variety of research, especially in neurological studies. However, it has not been a subject of any clinical trials.
Its effect on platelets has been already established. Early studies reported IC50 0.82 µM (CI95% 0.6–1.1) for human platelet aggregation, as measured by turbidimetry, and EC50 0.083 ± 0.005 µM for stimulation of adenylate cyclase in human platelets [91]. Subsequently, CGS 21,680 has been used for further platelet research, including, but not limited to, studies on the association between depression and platelet signaling dysregulation [96], species-dependent platelet function [97], and neutrophil involvement and signaling in thrombosis [98].
HE-NECA
Another AR agonist extensively employed in a variety of research areas is the A2A selective agonist HE-NECA, which was derived from non-selective AR agonist NECA. It has good selectivity between A2 and A1 receptor subclasses, but only slight selectivity between A2 and A3 subclasses (Ki A2 = 130 nM; Ki A2 = 2.2 nM; Ki A3 = 24 nM) [99]. It was reported as an anti-platelet agent in 1994 [99], when its anti-aggregatory potency was estimated as three-fold stronger in comparison to NECA. The anti-platelet activity of HE-NECA was confirmed in an in vivo study in rabbits, in which the drug was administered at a dose of 10 µg/kg: Platelet accumulation in pulmonary microcirculation was found to fall by over 50% after challenge with ADP [100]. HE-NECA was also used in a Borea group study investigating the influence of caffeine (AR inhibitor) on platelet function. In this study, HE-NECA was found to increase cAMP levels with an EC50 of 59 ± 3 nM, and inhibit ADP-induced human platelet aggregation (measured by turbidimetric method) with an IC50 of 90 ± 6 nM [101,102]. Recently, HE-NECA was also used in work focused on a quantification of different imaging approaches to experiments carried out under flow conditions, where 10 µM HE-NECA was found to inhibit clot formation under flow in whole blood by 82%, based on the volumes of aggregates recorded by confocal microscopy [103].
UK-432094
This AR agonist is usually known as UK-432,094 in the literature, but notations UK-432094 or UK432094 are also in use. UK-432,094 was tested by PFIZER in a phase II clinical trial (ClinicalTrials.gov Identifier: NCT00430300) as an inhalation agent for severe chronic obstructive pulmonary disease; however, the trial was terminated due to low treatment effectiveness. UK-432094 is a selective A2A agonist (Ki of 4.75 nM) [108], with reported EC50 as low as 5.4 ±1.8 nM (cAMP level evaluation in CHO cells stably expressing human A2A and A2B receptors) [109]. Its anti-platelet effect has been recently assessed using multiple electric aggregometry in whole blood. Using this technique, IC50 was found to be below 1 µM, with an inhibition rate of 40% at this concentration. The agonist had an ability to practically abolish aggregation at higher concentrations (79% inhibition at 100 μM), while demonstrating no cytotoxic effect on platelets [110].
3.2. Non-Adenosine Compounds
Apart from compounds based on the adenosine molecule modified chemically by introducing various substituents, AR agonists could also be found among substances of different chemical structure. The examples of such the AR agonists are given below.
3.2.1 BAY 60-6583
BAY 60-6583 was patented in 2001 as a highly-selective A2B agonist (Ki A2A is over10000 nM, Ki A2B = 3–10 nM). Since then, it has been used in various research areas, including in vitro and in vivo immunological [115], cardiological [116,117], and oncological [118,119] research, lung disease and damage control studies [120,121], as well as the therapy of renal nephropathy [122]. So far, it is the only selective A2B agonist in wide use. It has been reported to be a subject of pre-clinical studies to treat coronary artery disease and atherosclerosis [123], but it has not been registered for clinical trials.
The anti-platelet effects of BAY 60-6583 have not been studied in humans; however, Bot et al. report no decrease in aggregation (as measured by turbidimetry) or any change in platelet surface activation markers after treatment with BAY 60-6583 (50 µg/day) in ApoE−/− mice [124].
3.2.2 LUF5834 and LUF5835
A series of non-adenosine compounds were synthesized in 2004 as an attempt to generate an A2B AR subtype selective agonist [125]. LUF5834—2-amino4-(4-hydroxyphenyl)-6-(1H-imidazol-2-ylmethylsulfanyl)pyridine-3,5-dicarbonitrile was described as a partial agonist (EC50 of 12 nM for A2B receptor) slightly selective between A2A and A2B (Ki of 28 ± 4 nM and 12 ± 2 nM, respectively) or A1 receptor subtypes, but selective over the A3 subtype. Its analogue, LUF5835 (2-amino4-(3-hydroxyphenyl)-6-(1H-imidazol-2-ylmethylsulfanyl)pyridine-3,5-dicarbonitrile) is a full A2B agonist with EC50 of 10 nM, with a similar selectivity profile. It was later reported that LUF5834 binds to a different receptor site of A2A AR as compared to adenosine-based agonists, suggesting a distinct binding site for this class of agonists on AR receptors [126].
4. Dual Therapy
Anti-platelet therapy is an obvious solution for the treatment and management of arterial thrombosis dependent on blood platelet hyperactivity, often resulting in cardiovascular disease and stroke—the leading causes of morbidity and mortality in developed countries. Several therapeutic options are currently available; however, the problem of efficient and safe therapy remains unsolved, and there is still a demand for novel platelet inhibitors and new therapeutic options.
In clinical practice, efficient anti-platelet treatment is often hindered by reduced sensitivity to many anti-platelet agents. High dosages of anti-platelet drugs, while preventing excessive clotting, frequently also lead to bleeding incidents and moderate to severe side effects. To avoid higher drug doses, combined therapy based on the administration of two or more drugs acting on different platelet activation pathways is often used as an alternative. An example of such an approach currently used in clinical practice is the combined administration of acetylsalicylic acid (an inhibitor of thromboxane A2 formation) and clopidogrel (an inhibitor of the P2Y12 receptor). The P2Y12 receptor is the main therapeutic target in anti-platelet therapy, targeted at the ADP-dependent activation pathway [2]. Its agonization enhances the process of platelet aggregation initiated through the P2Y1 receptor. Unfortunately, such treatment is still beset by the problem of resistance, especially among patients with type 2 diabetes, i.e., a group at higher risk of thromboembolic events [129,130,131].
Our research group has recently proposed a novel approach based on the simultaneous application of two anti-platelet agents, a P2Y12 antagonist and an AR agonist, which has been found to deepen the action of P2Y12 antagonist [110]. Based on this report, we believe that adenosine receptor agonists could significantly enhance the anti-platelet effect of P2Y12 antagonists, despite possessing different selectivity profiles and anti-platelet activities. A strategy focused on a purinergic pathway and involving low-dose inhibition of classical (P2Y12) purinergic ADP receptors with the simultaneous activation of adenosine receptors may present a novel, promising approach to prevent thrombotic events, and should be further investigated.
5. Conclusions
Adenosine receptor agonists have been shown to have anti-platelet effect; however, not all of them are of the same magnitude, with some even presenting no discernible impact on aggregation. It is difficult to unambiguously give a simple answer as to whether this group of compounds stands a fair chance of becoming anti-platelet drugs in the foreseeable future. Too few known AR agonists have been evaluated specifically for modulation of platelet function, and as this topic was studied in the 1980s, some of the data require replication and confirmation using modern methodology. However a few AR agonists, like NECA, HE-NECA, CGS 21680, 2-chloroadenosine, and recently, PSB-15826, were confirmed to have platelet inhibiting properties, and the concept of employing them in preventing thrombus formation is re-emerging. More studies of different AR agonists focused specifically on anti-platelet properties are needed, as predictions based on physicochemical properties prove to be unreliable [68]; however, currently-available data suggests that such attempts should be focused on A2A AR agonists, as agonization of A2B AR has not been reliably reported to impact platelet aggregation or activation.
The use of AR agonists as anti-platelet medication appears feasible following further research focused explicitly on this goal, especially when applied in combination with other anti-platelet agents, to identify therapies demonstrating effective antithrombotic properties without risking severe side effects.
Funding
This work was supported by the project “Dual purinoreceptor—dependent approach to prevent thromboembolic events dependent on blood platelets and endothelium—approaches based on animal and cellular models” carried out within the TEAM programme (TEAM/2016-1/8) of the Foundation for Polish Science co-financed by the European Union under the European Regional Development Fund, and by a grant from Medical University funds: 502-03/6-020-01/502-64-125-18.
Conflicts of Interest
The authors declare no conflicts of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| ADP | Adenosine Diphosphate |
| AR | Adenosine Receptor |
| cAMP | Cyclic Adenosine Monophosphate |
| CHO | Chinese Hamster Ovary Cells |
| EC50 | Half Maximal Effective Concentration |
| IC50 | Half Maximal Inhibitory Concentration |
| KO | Knock-Out |
| FDA | Food and Drug Administration |
| HE-NECA | 2-Hexynyl-5′-(N-ethylcarboxamido)adenosine |
| IUPAC | International Union of Pure and Applied Chemistry |
| NECA | 5′-(N-ethylcarboxamido)adenosine |
| PRP | Platelet-Rich Plasma |
References
- Kaplan, Z.S.; Jackson, S.P. The role of platelets in atherothrombosis. Hematology Am. Soc. Hematol. Educ. Program 2011, 2011, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Kupka, D.; Sibbing, D. P2Y12 receptor inhibitors: An evolution in drug design to prevent arterial thrombosis. Expert Opin. Drug Metab. Toxicol. 2018, 14, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; Morais, J.; Baigent, C.; Collet, J.P.; Fitzgerald, D.; Halvorsen, S.; Rocca, B.; Siegbahn, A.; Storey, R.F.; Vilahur, G. Antiplatelet Agents for the Treatment and Prevention of Coronary Atherothrombosis. J. Am. Coll. Cardiol. 2017, 70, 1760–1776. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; Andreotti, F.; Arnesen, H.; Badimon, L.; Baigent, C.; Collet, J.P.; De Caterina, R.; Gulba, D.; Huber, K.; Husted, S.; et al. Antiplatelet agents for the treatment and prevention of atherothrombosis. Eur. Heart J. 2011, 32, 2922–2932. [Google Scholar] [CrossRef] [PubMed]
- van Giezen, J.J.; Humphries, R.G. Preclinical and clinical studies with selective reversible direct P2Y12 antagonists. Semin. Thromb. Hemost. 2005, 31, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Rollini, F.; Storey, R.F.; Bhatt, D.L.; James, S.; Schneider, D.J.; Sibbing, D.; So, D.Y.F.; Trenk, D.; Alexopoulos, D.; et al. International Expert Consensus on Switching Platelet P2Y12 Receptor-Inhibiting Therapies. Circulation 2017, 136, 1955–1975. [Google Scholar] [CrossRef]
- Tyler, J.M.; Burris, R.J.; Seto, A.H. Why we need intravenous antiplatelet agents. Future Cardiology 2016, 12, 553–561. [Google Scholar] [CrossRef]
- Delaney, M.K.; Kim, K.; Estevez, B.; Xu, Z.; Stojanovic-Terpo, A.; Shen, B.; Ushio-Fukai, M.; Cho, J.; Du, X. Differential Roles of the NADPH-Oxidase 1 and 2 in Platelet Activation and Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Khan, N.I.; Siddiqui, F.M.; Goldstein, J.N.; Cox, M.; Xian, Y.; Matsouaka, R.A.; Heidenreich, P.A.; Peterson, E.D.; Bhatt, D.L.; Fonarow, G.C.; et al. Association Between Previous Use of Antiplatelet Therapy and Intracerebral Hemorrhage Outcomes. Stroke 2017, 48, 1810–1817. [Google Scholar] [CrossRef]
- Rozalski, M.; Boncler, M.; Luzak, B.; Watala, C. Genetic factors underlying differential blood platelet sensitivity to inhibitors. Pharmacol. Rep. 2005, 57, 1–13. [Google Scholar]
- Chen, J.F.; Eltzschig, H.K.; Fredholm, B.B. Adenosine receptors as drug targets--what are the challenges? Nat. Rev. Drug Discov. 2013, 12, 265–286. [Google Scholar] [CrossRef] [PubMed]
- Fredholm, B.B. Adenosine receptors as drug targets. Exp. Cell Res. 2010, 316, 1284–1288. [Google Scholar] [CrossRef] [Green Version]
- Johnston-Cox, H.A.; Ravid, K. Adenosine and blood platelets. Purinergic Signal 2011, 7, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston-Cox, H.; Koupenova, M.; Yang, D.; Corkey, B.; Gokce, N.; Farb, M.G.; LeBrasseur, N.; Ravid, K. The A2b adenosine receptor modulates glucose homeostasis and obesity. PLoS ONE 2012, 7, e40584. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.; Brito, R.; Mukherjea, D.; Rybak, L.P.; Ramkumar, V. Adenosine Receptors: Expression, Function and Regulation. Int. J. Mol. Sci. 2014, 15, 2024–2052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessi, S.; Varani, K.; Merighi, S.; Ongini, E.; Borea, P.A. A(2A) adenosine receptors in human peripheral blood cells. Br. J. Pharmacol. 2000, 129, 2–11. [Google Scholar] [CrossRef]
- Wang, J.; Miao, Y. Mechanistic Insights into Specific G Protein Interactions with Adenosine Receptors. J. Phys. Chem. B 2019, 123, 6462–6473. [Google Scholar] [CrossRef]
- Koupenova, M.; Ravid, K. Biology of Platelet Purinergic Receptors and Implications for Platelet Heterogeneity. Front. Pharmacol. 2018, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, S.A.; Quinn, R.J. Adenosine receptors: New opportunities for future drugs. Bioorg. Med. Chem. 1998, 6, 619–641. [Google Scholar] [CrossRef]
- Fredholm, B.B.; Cunha, R.A.; Svenningsson, P. Pharmacology of adenosine A2A receptors and therapeutic applications. Curr. Top. Med. Chem. 2003, 3, 413–426. [Google Scholar] [CrossRef]
- Cacciari, B.; Pastorin, G.; Bolcato, C.; Spalluto, G.; Bacilieri, M.; Moro, S. A2B adenosine receptor antagonists: Recent developments. Mini Rev. Med. Chem. 2005, 5, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Amisten, S.; Braun, O.O.; Bengtsson, A.; Erlinge, D. Gene expression profiling for the identification of G-protein coupled receptors in human platelets. Thromb. Res. 2007, 122, 47–57. [Google Scholar] [CrossRef] [PubMed]
- .Yang, D.; Chen, H.; Koupenova, M.; Carroll, S.H.; Eliades, A.; Freedman, J.E.; Toselli, P.; Ravid, K. A new role for the A2b adenosine receptor in regulating platelet function. J. Thromb. Haemost. 2010, 8, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Cristalli, G.; Lambertucci, C.; Taffi, S.; Vittori, S.; Volpini, R. Medicinal chemistry of adenosine A2A receptor agonists. Curr. Top. Med. Chem. 2003, 3, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Federico, S.; Spalluto, G. Therapeutic potential of A2 and A3 adenosine receptor: A review of novel patented ligands. Expert Opin. Ther. Pat. 2012, 22, 369–390. [Google Scholar] [CrossRef] [PubMed]
- .Ongini, E.; Fredholm, B.B. Pharmacology of adenosine A2A receptors. Trends Pharmacol. Sci. 1996, 17, 364–372. [Google Scholar] [CrossRef]
- Parkman, R.; Gelfand, E.W.; Rosen, F.S.; Sanderson, A.; Hirschhorn, R. Severe Combined Immunodeficiency and Adenosine Deaminase Deficiency. New Engl. J. Med. 1975, 292, 714–719. [Google Scholar] [CrossRef]
- Farrukh, S.; Safiah, S.; Hasan, H.; Agha, M.; Rehan, K.; Sulaiman Al, G.; Hasan, A.; Ghuzayel, A.-D.; Riad El, F.; Rand, A. Thrombocytopenia in a Patient with Severe Combined Immune Deficiency: An Unusual Cause. Int. J. Allergy Medicat. 2018, 4. [Google Scholar] [CrossRef]
- Lee, C.H.; Evans, S.P.; Rozenberg, M.C.; Bagnara, A.S.; Ziegler, J.B.; Van der Weyden, M.B. In vitro platelet abnormality in adenosine deaminase deficiency and severe combined immunodeficiency. Blood 1979, 53, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Wijten, P.; van Holten, T.; Woo, L.L.; Bleijerveld, O.B.; Roest, M.; Heck, A.J.; Scholten, A. High precision platelet releasate definition by quantitative reversed protein profiling--brief report. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1635–1638. [Google Scholar] [CrossRef]
- Burkhart, J.M.; Vaudel, M.; Gambaryan, S.; Radau, S.; Walter, U.; Martens, L.; Geiger, J.; Sickmann, A.; Zahedi, R.P. The first comprehensive and quantitative analysis of human platelet protein composition allows the comparative analysis of structural and functional pathways. Blood 2012, 120, e73–e82. [Google Scholar] [CrossRef] [Green Version]
- Ohlmann, P.; Lecchi, A.; El-Tayeb, A.; Muller, C.E.; Cattaneo, M.; Gachet, C. The platelet P2Y(12) receptor under normal and pathological conditions. Assessment with the radiolabeled selective antagonist [(3)H]PSB-0413. Purinergic Signal. 2013, 9, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.E.; Scior, T. Adenosine receptors and their modulators. Pharm. Acta Helv. 1993, 68, 77–111. [Google Scholar] [CrossRef]
- Paul, S.; Feoktistov, I.; Hollister, A.S.; Robertson, D.; Biaggioni, I. Adenosine inhibits the rise in intracellular calcium and platelet aggregation produced by thrombin: Evidence that both effects are coupled to adenylate cyclase. Mol. Pharmacol. 1990, 37, 870–875. [Google Scholar] [PubMed]
- Ledent, C.; Vaugeois, J.M.; Schiffmann, S.N.; Pedrazzini, T.; El Yacoubi, M.; Vanderhaeghen, J.J.; Costentin, J.; Heath, J.K.; Vassart, G.; Parmentier, M. Aggressiveness, hypoalgesia and high blood pressure in mice lacking the adenosine A2a receptor. Nature 1997, 388, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.; Heaney, L.G.; Ennis, M. Adenosine, inflammation and asthma—a review. Inflamm. Res. 2004, 53, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.E.; Jacobson, K.A. Recent developments in adenosine receptor ligands and their potential as novel drugs. Biochim. Biophys. Acta 2011, 1808, 1290–1308. [Google Scholar] [CrossRef] [Green Version]
- Born, G.V. Strong Inhibition by 2-Chloroadenosine of the Aggregation of Blood Platelets by Adenosine Diphosphate. Nature 1964, 202, 95–96. [Google Scholar] [CrossRef]
- Born, G.V.; Honour, A.J.; Mitchell, J.R. Inhibition by Adenosine and by 2-Chloroadenosine of the Formation and Embolization of Platelet Thrombi. Nature 1964, 202, 761–765. [Google Scholar] [CrossRef]
- Born, G.V. Observations on the change in shape of blood platelets brought about by adenosine diphosphate. J. Physiol. 1970, 209, 487–511. [Google Scholar] [CrossRef] [Green Version]
- Born, G.V.; Dearnley, R.; Foulks, J.G.; Sharp, D.E. Quantification of the morphological reaction of platelets to aggregating agents and of its reversal by aggregation inhibitors. J. Physiol. 1978, 280, 193–212. [Google Scholar] [CrossRef] [PubMed]
- Quattrin, S.; Genovese, A.; Cirillo, R.; Formisano, S.; Marone, G. Functional and biochemical evidence of a specific adenosine A2/Ra receptor on human platelets. Ric. Clin. Lab. 1988, 18, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Milton, J.G.; Frojmovic, M.M.; Tang, S.S.; White, J.G. Spontaneous platelet aggregation in a hereditary giant platelet syndrome (MPS). Am. J. Pathol. 1984, 114, 336–345. [Google Scholar] [PubMed]
- Saniabadi, A.R.; Takeich, S.; Yukawa, N.; Nakajima, Y.; Umemura, K.; Nakashima, M. Apo E4/3-rich remnant lipoproteins and platelet aggregation: A case report. Thromb. Haemost. 1998, 79, 878–879. [Google Scholar]
- Haslam, R.J.; Lynham, J.A. Activation and inhibition of blood platelet adenylate cyclase by adenosine or by 2-chloroadenosine. Life Sci. II 1972, 11, 1143–1154. [Google Scholar] [CrossRef]
- Ukena, D.; Bohme, E.; Schwabe, U. Effects of several 5’-carboxamide derivatives of adenosine on adenosine receptors of human platelets and rat fat cells. N-S Arch. Pharmacol. 1984, 327, 36–42. [Google Scholar] [CrossRef]
- Dawicki, D.D.; Agarwal, K.C.; Parks, R.E., Jr. Potentiation of the antiplatelet action of adenosine in whole blood by dipyridamole or dilazep and the cAMP phosphodiesterase inhibitor, RA 233. Thromb. Res. 1986, 43, 161–175. [Google Scholar] [CrossRef]
- Agarwal, A.K.; Tandon, N.N.; Greco, N.J.; Cusack, N.J.; Jamieson, G.A. Evaluation of the binding to fixed platelets of agonists and antagonists of ADP-induced aggregation. Thromb. Haemost. 1989, 62, 1103–1106. [Google Scholar] [CrossRef]
- Fein, T.; Schulze, E.; Bar, J.; Schwabe, U. Purification and characterization of an adenotin-like adenosine binding protein from human platelets. N-S Arch. Pharmacol. 1994, 349, 374–380. [Google Scholar] [CrossRef]
- Mares, P. Anticonvulsant action of 2-chloroadenosine against pentetrazol-induced seizures in immature rats is due to activation of A1 adenosine receptors. J. Neural Transm. (Vienna) 2010, 117, 1269–1277. [Google Scholar] [CrossRef]
- Saze, Z.; Schuler, P.J.; Hong, C.S.; Cheng, D.; Jackson, E.K.; Whiteside, T.L. Adenosine production by human B cells and B cell-mediated suppression of activated T cells. Blood 2013, 122, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Patinha, D.; Afonso, J.; Sousa, T.; Morato, M.; Albino-Teixeira, A. Activation of adenosine receptors improves renal antioxidant status in diabetic Wistar but not SHR rats. Ups. J. Med. Sci. 2014, 119, 10–18. [Google Scholar] [CrossRef] [PubMed]
- .Dubey, R.K.; Fingerle, J.; Gillespie, D.G.; Mi, Z.; Rosselli, M.; Imthurn, B.; Jackson, E.K. Adenosine Attenuates Human Coronary Artery Smooth Muscle Cell Proliferation by Inhibiting Multiple Signaling Pathways That Converge on Cyclin D. Hypertension 2015, 66, 1207–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, G.; Maguire, M.H.; Michal, F. 2-chloroadenosine 5’-phosphate and 2-chloroadenosine 5’-diphosphate, pharmacologically active nucleotide analogs. J. Med. Chem. 1969, 12, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Li, Z.; Baker, S.P.; Lasley, R.D.; Meyer, S.; Elzein, E.; Palle, V.; Zablocki, J.A.; Blackburn, B.; Belardinelli, L. Novel short-acting A2A adenosine receptor agonists for coronary vasodilation: Inverse relationship between affinity and duration of action of A2A agonists. J. Pharmacol. Exp. Ther. 2001, 298, 209–218. [Google Scholar]
- Lieu, H.D.; Shryock, J.C.; von Mering, G.O.; Gordi, T.; Blackburn, B.; Olmsted, A.W.; Belardinelli, L.; Kerensky, R.A. Regadenoson, a selective A2A adenosine receptor agonist, causes dose-dependent increases in coronary blood flow velocity in humans. J. Nucl. Cardiol. 2007, 14, 514–520. [Google Scholar] [CrossRef]
- Glover, D.K.; Ruiz, M.; Yang, J.Y.; Koplan, B.A.; Allen, T.R.; Smith, W.H.; Watson, D.D.; Barrett, R.J.; Beller, G.A. Pharmacological stress thallium scintigraphy with 2-cyclohexylmethylidenehydrazinoadenosine (WRC-0470). A novel, short-acting adenosine A2A receptor agonist. Circulation 1996, 94, 1726–1732. [Google Scholar] [CrossRef]
- Firschke, C.; Lindner, J.R.; Goodman, N.C.; Skyba, D.M.; Wei, K.; Kaul, S. Myocardial contrast echocardiography in acute myocardial infarction using aortic root injections of microbubbles in conjunction with harmonic imaging: Potential application in the cardiac catheterization laboratory. J. Am. Coll. Cardiol. 1997, 29, 207–216. [Google Scholar] [CrossRef]
- Barrett, R.J.; Lamson, M.J.; Johnson, J.; Smith, W.B. Pharmacokinetics and safety of binodenoson after intravenous dose escalation in healthy volunteers. J. Nucl. Cardiol. 2005, 12, 166–171. [Google Scholar] [CrossRef]
- Udelson, J.E.; Heller, G.V.; Wackers, F.J.; Chai, A.; Hinchman, D.; Coleman, P.S.; Dilsizian, V.; DiCarli, M.; Hachamovitch, R.; Johnson, J.R.; et al. Randomized, controlled dose-ranging study of the selective adenosine A2A receptor agonist binodenoson for pharmacological stress as an adjunct to myocardial perfusion imaging. Circulation 2004, 109, 457–464. [Google Scholar] [CrossRef]
- Murray, J.J.; Weiler, J.M.; Schwartz, L.B.; Busse, W.W.; Katial, R.K.; Lockey, R.F.; McFadden, E.R., Jr.; Pixton, G.C.; Barrett, R.J. Safety of binodenoson, a selective adenosine A2A receptor agonist vasodilator pharmacological stress agent, in healthy subjects with mild intermittent asthma. Circ. Cardiovasc. Imaging 2009, 2, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Atta-ur-Rahman; Choudhary, M.I. Advancement in Developing New Adenosine Receptors Ligands. In Frontiers in Cardiovascular Drug Discovery: Volume 4; Bentham Science Publishers: Sharjah, UAE, 2019; pp. 16–64. [Google Scholar] [CrossRef]
- El-Tayeb, A.; Michael, S.; Abdelrahman, A.; Behrenswerth, A.; Gollos, S.; Nieber, K.; Muller, C.E. Development of Polar Adenosine A2A Receptor Agonists for Inflammatory Bowel Disease: Synergism with A2B Antagonists. ACS Med. Chem. Lett. 2011, 2, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Deuther, C.; Peter, B.; Martin, E.L.; Matthias, J.B.; Sven, E.; Jürgen, S.; Gennady, G.Y.; Christa, E.M.; Alexander Pfeifer, T.G.; Saskia, S.; et al. Adenosine activates brown adipose tissue and recruits beige adipocytes via A2A receptors. Nature 2014, 516, 395–399. [Google Scholar]
- Fuentes, E.; Badimon, L.; Caballero, J.; Padro, T.; Vilahur, G.; Alarcon, M.; Perez, P.; Palomo, I. Protective mechanisms of adenosine 5’-monophosphate in platelet activation and thrombus formation. Thromb. Haemost. 2014, 111, 491–507. [Google Scholar] [CrossRef] [PubMed]
- Volpini, R.; Costanzi, S.; Lambertucci, C.; Portino, F.R.; Taffi, S.; Vittori, S.; Zablocki, J.A.; Klotz, K.N.; Cristalli, G. Adenosine receptor agonists: Synthesis and binding affinity of 2-(aryl)alkylthioadenosine derivatives. Arkivoc 2004, 2004, 301–311. [Google Scholar]
- .El-Tayeb, A.; Iqbal, J.; Behrenswerth, A.; Romio, M.; Schneider, M.; Zimmermann, H.; Schrader, J.; Muller, C.E. Nucleoside-5’-monophosphates as prodrugs of adenosine A2A receptor agonists activated by ecto-5’-nucleotidase. J. Med. Chem. 2009, 52, 7669–7677. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, E.; Fuentes, M.; Caballero, J.; Palomo, I.; Hinz, S.; El-Tayeb, A.; Muller, C.E. Adenosine A2A receptor agonists with potent antiplatelet activity. Platelets 2018, 29, 292–300. [Google Scholar] [CrossRef]
- .Ueeda, M.; Thompson, R.D.; Arroyo, L.H.; Olsson, R.A. 2-aralkoxyadenosines: Potent and selective agonists at the coronary artery A2 adenosine receptor. J. Med. Chem. 1991, 34, 1340–1344. [Google Scholar] [CrossRef]
- Nguyen, D.K.; Montesinos, M.C.; Williams, A.J.; Kelly, M.; Cronstein, B.N. Th1 cytokines regulate adenosine receptors and their downstream signaling elements in human microvascular endothelial cells. J. Immunol. 2003, 171, 3991–3998. [Google Scholar]
- Reiss, A.B.; Rahman, M.M.; Chan, E.S.; Montesinos, M.C.; Awadallah, N.W.; Cronstein, B.N. Adenosine A2A receptor occupancy stimulates expression of proteins involved in reverse cholesterol transport and inhibits foam cell formation in macrophages. J. Leukoc. Biol. 2004, 76, 727–734. [Google Scholar] [CrossRef]
- Desai, A.; Victor-Vega, C.; Gadangi, S.; Montesinos, M.C.; Chu, C.C.; Cronstein, B.N. Adenosine A2A receptor stimulation increases angiogenesis by down-regulating production of the antiangiogenic matrix protein thrombospondin 1. Mol. Pharmacol. 2005, 67, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Victor-Vega, C.; Desai, A.; Montesinos, M.C.; Cronstein, B.N. Adenosine A2A receptor agonists promote more rapid wound healing than recombinant human platelet-derived growth factor (Becaplermin gel). Inflammation 2002, 26, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Valls, M.D.; Cronstein, B.N.; Montesinos, M.C. Adenosine receptor agonists for promotion of dermal wound healing. Biochem. Pharmacol. 2009, 77, 1117–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ukena, D.; Olsson, R.A.; Daly, J.W. Definition of subclasses of adenosine receptors associated with adenylate cyclase: Interaction of adenosine analogs with inhibitory A1 receptors and stimulatory A2 receptors. Can. J. Physiol. Pharmacol. 1987, 65, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Gurden, M.F.; Coates, J.; Ellis, F.; Evans, B.; Foster, M.; Hornby, E.; Kennedy, I.; Martin, D.P.; Strong, P.; Vardey, C.J.; et al. Functional characterization of three adenosine receptor types. Br. J. Pharmacol. 1993, 109, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Brackett, L.E.; Daly, J.W. Functional characterization of the A2b adenosine receptor in NIH 3T3 fibroblasts. Biochem. Pharmacol. 1994, 47, 801–814. [Google Scholar] [CrossRef]
- Cunha, R.A.; Johansson, B.; Constantino, M.D.; Sebastiao, A.M.; Fredholm, B.B. Evidence for high-affinity binding sites for the adenosine A2A receptor agonist [3H] CGS 21680 in the rat hippocampus and cerebral cortex that are different from striatal A2A receptors. N-S Arch. Pharmacol. 1996, 353, 261–271. [Google Scholar] [CrossRef]
- Ravyn, V.; Bostwick, J.R. Functional coupling of the Galpha(olf) variant XLGalpha(olf) with the human adenosine A2A receptor. J. Recept. Signal. Transduct. Res. 2006, 26, 241–258. [Google Scholar] [CrossRef]
- White, P.J.; Rose’Meyer, R.B.; Hope, W. Functional characterization of adenosine receptors in the nucleus tractus solitarius mediating hypotensive responses in the rat. Br. J. Pharmacol. 1996, 117, 305–308. [Google Scholar] [CrossRef] [Green Version]
- Tostes, R.C.; Giachini, F.R.; Carneiro, F.S.; Leite, R.; Inscho, E.W.; Webb, R.C. Determination of adenosine effects and adenosine receptors in murine corpus cavernosum. J. Pharmacol. Exp. Ther. 2007, 322, 678–685. [Google Scholar] [CrossRef]
- Nalos, M.; Huang, S.; Sluyter, R.; Khan, A.; Santner-Nanan, B.; Nanan, R.; McLean, A.S. “Host tissue damage” signal ATP impairs IL-12 and IFNgamma secretion in LPS stimulated whole human blood. Intensive Care Med. 2008, 34, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Long, X.; Mokelke, E.A.; Neeb, Z.P.; Alloosh, M.; Edwards, J.M.; Sturek, M. Adenosine receptor regulation of coronary blood flow in Ossabaw miniature swine. J. Pharmacol. Exp. Ther. 2010, 335, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Yip, K.H.; Lau, H.Y.; Wise, H. Reciprocal modulation of anti-IgE induced histamine release from human mast cells by A(1) and A(2B) adenosine receptors. Br. J. Pharmacol. 2011, 164, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Smits, G.J.; McVey, M.; Cox, B.F.; Perrone, M.H.; Clark, K.L. Cardioprotective effects of the novel adenosine A1/A2 receptor agonist AMP 579 in a porcine model of myocardial infarction. J. Pharmacol. Exp. Ther. 1998, 286, 611–618. [Google Scholar] [PubMed]
- Clark, K.L.; Merkel, L.; Zannikos, P.; Kelley, M.F.; Boutouyrie, B.; Perrone, M.H. AMP 579, a Novel Adenosine Agonist for the Treatment of Acute Myocardial Infarction. Cardiovasc. Drug Rev. 2000, 18, 183–210. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, X.; Yang, X.M.; Walker, S.; Forster, K.; Cohen, M.V.; Krieg, T.; Downey, J.M. AMP579 is revealed to be a potent A2b-adenosine receptor agonist in human 293 cells and rabbit hearts. Basic Res. Cardiol. 2010, 105, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Cusack, N.J.; Hourani, S.M. 5’-N-ethylcarboxamidoadenosine: A potent inhibitor of human platelet aggregation. Br. J. Pharmacol. 1981, 72, 443–447. [Google Scholar] [CrossRef]
- Huttemann, E.; Ukena, D.; Lenschow, V.; Schwabe, U. Ra adenosine receptors in human platelets. Characterization by 5′-N-ethylcarboxamido[3 H]adenosine binding in relation to adenylate cyclase activity. N-S Arch. Pharmacol. 1984, 325, 226–233. [Google Scholar]
- Lohse, M.J.; Klotz, K.N.; Schwabe, U. Mechanism of A2 adenosine receptor activation. I. Blockade of A2 adenosine receptors by photoaffinity labeling. Mol. Pharmacol. 1991, 39, 517–523. [Google Scholar]
- Cristalli, G.; Vittori, S.; Thompson, R.D.; Padgett, W.L.; Shi, D.; Daly, J.W.; Olsson, R.A. Inhibition of platelet aggregation by adenosine receptor agonists. N-S Arch. Pharmacol. 1994, 349, 644–650. [Google Scholar] [CrossRef]
- Volpini, R.; Dal Ben, D.; Lambertucci, C.; Taffi, S.; Vittori, S.; Klotz, K.-N.; Cristalli, G. N 6 -Methoxy-2-alkynyladenosine Derivatives as Highly Potent and Selective Ligands at the Human A 3 Adenosine Receptor. J. Med. Chem. 2007, 50, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- de Zwart, M.; Link, R.; von Frijtag Drabbe Kunzel, J.K.; Cristalli, G.; Jacobson, K.A.; Townsend-Nicholson, A.; AP, I.J. A functional screening of adenosine analogues at the adenosine A2B receptor: A search for potent agonists. Nucleos Nucleot 1998, 17, 969–985. [Google Scholar] [CrossRef] [PubMed]
- Feoktistov, I.; Biaggioni, I. Characterization of adenosine receptors in human erythroleukemia cells and platelets: Further evidence for heterogeneity of adenosine A2 receptor subtypes. Mol. Pharmacol. 1993, 43, 909–914. [Google Scholar] [PubMed]
- van Calker, D.; Muller, M.; Hamprecht, B. Adenosine regulates via two different types of receptors, the accumulation of cyclic AMP in cultured brain cells. J. Neurochem. 1979, 33, 999–1005. [Google Scholar] [CrossRef]
- Berk, M.; Plein, H.; Ferreira, D.; Jersky, B. Blunted adenosine A2a receptor function in platelets in patients with major depression. Eur. Neuropsychopharmacol. 2001, 11, 183–186. [Google Scholar] [CrossRef]
- Linden, M.D.; Barnard, M.R.; Frelinger, A.L.; Michelson, A.D.; Przyklenk, K. Effect of adenosine A2 receptor stimulation on platelet activation-aggregation: Differences between canine and human models. Thromb. Res. 2008, 121, 689–698. [Google Scholar] [CrossRef]
- .Darbousset, R.; Delierneux, C.; Mezouar, S.; Hego, A.; Lecut, C.; Guillaumat, I.; Riederer, M.A.; Evans, R.J.; Dignat-George, F.; Panicot-Dubois, L.; et al. P2X1 expressed on polymorphonuclear neutrophils and platelets is required for thrombosis in mice. Blood 2014, 124, 2575–2585. [Google Scholar] [CrossRef] [Green Version]
- Cristalli, G.; Volpini, R.; Vittori, S.; Camaioni, E.; Monopoli, A.; Conti, A.; Dionisotti, S.; Zocchi, C.; Ongini, E. 2-Alkynyl derivatives of adenosine-5’-N-ethyluronamide: Selective A2 adenosine receptor agonists with potent inhibitory activity on platelet aggregation. J. Med. Chem. 1994, 37, 1720–1726. [Google Scholar] [CrossRef]
- Sandoli, D.; Chiu, P.J.; Chintala, M.; Dionisotti, S.; Ongini, E. In vivo and ex vivo effects of adenosine A1 and A2 receptor agonists on platelet aggregation in the rabbit. Eur. J. Pharmacol. 1994, 259, 43–49. [Google Scholar] [CrossRef]
- Varani, K.; Portaluppi, F.; Merighi, S.; Ongini, E.; Belardinelli, L.; Borea, P.A. Caffeine alters A2A adenosine receptors and their function in human platelets. Circulation 1999, 99, 2499–2502. [Google Scholar] [CrossRef]
- Varani, K.; Portaluppi, F.; Gessi, S.; Merighi, S.; Ongini, E.; Belardinelli, L.; Borea, P.A. Dose and time effects of caffeine intake on human platelet adenosine A(2A) receptors: Functional and biochemical aspects. Circulation 2000, 102, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Przygodzki, T.; Wolska, N.; Talar, M.; Polak, D.; Gapinska, M.; Watala, C. Comparison of different microscopy approaches to quantification of inhibitory effect on thrombus formation under flow conditions by the example of adenosine receptor agonist HE-NECA. J. Pharmacol. Toxicol. Methods 2018, 94, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Panzacchi, G.; Demarchi, B.; Busca, G.; Protasoni, G.; Golin, R.; Stella, A. Effects of adenosine receptor agonists on renal function in anaesthetized rats. J. Hypertens. 1997, 15, 1785–1789. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.A.; Constantino, M.D.; Ribeiro, J.A. ZM241385 is an antagonist of the facilitatory responses produced by the A2A adenosine receptor agonists CGS21680 and HENECA in the rat hippocampus. Br. J. Pharmacol. 1997, 122, 1279–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagpure, B.V.; Bian, J.S. Hydrogen sulfide inhibits A2A adenosine receptor agonist induced beta-amyloid production in SH-SY5Y neuroblastoma cells via a cAMP dependent pathway. Plos ONE 2014, 9, e88508. [Google Scholar] [CrossRef]
- Varani, K.; Gessi, S.; Merighi, S.; Iannotta, V.; Cattabriga, E.; Spisani, S.; Cadossi, R.; Borea, P.A. Effect of low frequency electromagnetic fields on A2A adenosine receptors in human neutrophils. Br. J. Pharmacol. 2002, 136, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Wu, H.; Katritch, V.; Han, G.W.; Jacobson, K.A.; Gao, Z.G.; Cherezov, V.; Stevens, R.C. Structure of an agonist-bound human A2A adenosine receptor. Science 2011, 332, 322–327. [Google Scholar] [CrossRef]
- Astrand, A.B.; Lamm Bergstrom, E.; Zhang, H.; Borjesson, L.; Soderdahl, T.; Wingren, C.; Jansson, A.H.; Smailagic, A.; Johansson, C.; Bladh, H.; et al. The discovery of a selective and potent A2a agonist with extended lung retention. Pharmacol Res. Perspect 2015, 3, e00134. [Google Scholar] [CrossRef]
- Boncler, M.; Wzorek, J.; Wolska, N.; Polak, D.; Watala, C.; Rozalski, M. Adenosine receptor agonists deepen the inhibition of platelet aggregation by P2Y12 antagonists. Vascul. Pharmacol. 2019, 113, 47–56. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lyman, E. Agonist dynamics and conformational selection during microsecond simulations of the A(2A) adenosine receptor. Biophys. J. 2012, 102, 2114–2120. [Google Scholar] [CrossRef]
- Lebon, G.; Edwards, P.C.; Leslie, A.G.; Tate, C.G. Molecular Determinants of CGS21680 Binding to the Human Adenosine A2A Receptor. Mol. Pharmacol. 2015, 87, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Van Eps, N.; Zimmer, M.; Ernst, O.P.; Prosser, R.S. Activation of the A2A adenosine G-protein-coupled receptor by conformational selection. Nature 2016, 533, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Patel, R.; Lyman, E. Ligand-dependent cholesterol interactions with the human A(2A) adenosine receptor. Chem. Phys. Lipids 2013, 169, 39–45. [Google Scholar] [CrossRef] [PubMed]
- van der Hoeven, D.; Wan, T.C.; Gizewski, E.T.; Kreckler, L.M.; Maas, J.E.; Van Orman, J.; Ravid, K.; Auchampach, J.A. A role for the low-affinity A2B adenosine receptor in regulating superoxide generation by murine neutrophils. J. Pharmacol. Exp. Ther. 2011, 338, 1004–1012. [Google Scholar] [CrossRef] [PubMed]
- Eckle, T.; Krahn, T.; Grenz, A.; Kohler, D.; Mittelbronn, M.; Ledent, C.; Jacobson, M.A.; Osswald, H.; Thompson, L.F.; Unertl, K.; et al. Cardioprotection by ecto-5’-nucleotidase (CD73) and A2B adenosine receptors. Circulation 2007, 115, 1581–1590. [Google Scholar] [CrossRef]
- Xi, J.; McIntosh, R.; Shen, X.; Lee, S.; Chanoit, G.; Criswell, H.; Zvara, D.A.; Xu, Z. Adenosine A2A and A2B receptors work in concert to induce a strong protection against reperfusion injury in rat hearts. J. Mol. Cell. Cardiol. 2009, 47, 684–690. [Google Scholar] [CrossRef] [Green Version]
- Sorrentino, C.; Miele, L.; Porta, A.; Pinto, A.; Morello, S. Myeloid-derived suppressor cells contribute to A2B adenosine receptor-induced VEGF production and angiogenesis in a mouse melanoma model. Oncotarget 2015, 6, 27478–27489. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.; Lorimer, E.; Tyburski, M.D.; Williams, C.L. beta-Adrenergic receptors suppress Rap1B prenylation and promote the metastatic phenotype in breast cancer cells. Cancer Biol. Ther. 2015, 16, 1364–1374. [Google Scholar] [CrossRef]
- Schingnitz, U.; Hartmann, K.; Macmanus, C.F.; Eckle, T.; Zug, S.; Colgan, S.P.; Eltzschig, H.K. Signaling through the A2B adenosine receptor dampens endotoxin-induced acute lung injury. J. Immunol. 2010, 184, 5271–5279. [Google Scholar] [CrossRef]
- Koscso, B.; Trepakov, A.; Csoka, B.; Nemeth, Z.H.; Pacher, P.; Eltzschig, H.K.; Hasko, G. Stimulation of A2B adenosine receptors protects against trauma-hemorrhagic shock-induced lung injury. Purinergic Signal. 2013, 9, 427–432. [Google Scholar] [CrossRef]
- Tak, E.; Ridyard, D.; Kim, J.H.; Zimmerman, M.; Werner, T.; Wang, X.X.; Shabeka, U.; Seo, S.W.; Christians, U.; Klawitter, J.; et al. CD73-dependent generation of adenosine and endothelial Adora2b signaling attenuate diabetic nephropathy. J. Am. Soc. Nephrol. 2014, 25, 547–563. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, P.G.; Tabrizi, M.A.; Fruttarolo, F.; Romagnoli, R.; Preti, D. Recent improvements in the development of A(2B) adenosine receptor agonists. Purinergic Signal. 2008, 4, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Bot, I.; de Vries, H.; Korporaal, S.J.; Foks, A.C.; Bot, M.; van Veldhoven, J.; Ter Borg, M.N.; van Santbrink, P.J.; van Berkel, T.J.; Kuiper, J.; et al. Adenosine A(2)B receptor agonism inhibits neointimal lesion development after arterial injury in apolipoprotein E-deficient mice. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Beukers, M.W.; Chang, L.C.; von Frijtag Drabbe Kunzel, J.K.; Mulder-Krieger, T.; Spanjersberg, R.F.; Brussee, J.; AP, I.J. New, non-adenosine, high-potency agonists for the human adenosine A2B receptor with an improved selectivity profile compared to the reference agonist N-ethylcarboxamidoadenosine. J. Med. Chem. 2004, 47, 3707–3709. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.R.; Klein Herenbrink, C.; van Westen, G.J.; Spoorendonk, J.A.; Hoffmann, C.; AP, I.J. A novel nonribose agonist, LUF5834, engages residues that are distinct from those of adenosine-like ligands to activate the adenosine A(2a) receptor. Mol. Pharmacol. 2012, 81, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Urmaliya, V.B.; Church, J.E.; Coupar, I.M.; Rose’Meyer, R.B.; Pouton, C.W.; White, P.J. Cardioprotection induced by adenosine A1 receptor agonists in a cardiac cell ischemia model involves cooperative activation of adenosine A2A and A2B receptors by endogenous adenosine. J. Cardiovasc. Pharmacol. 2009, 53, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Koda, K.; Salazar-Rodriguez, M.; Corti, F.; Chan, N.Y.; Estephan, R.; Silver, R.B.; Mochly-Rosen, D.; Levi, R. Aldehyde dehydrogenase activation prevents reperfusion arrhythmias by inhibiting local renin release from cardiac mast cells. Circulation 2010, 122, 771–781. [Google Scholar] [CrossRef]
- Wang, Y.; Johnston, S.C.; Bath, P.M.; Grotta, J.C.; Pan, Y.; Amarenco, P.; Wang, Y.; Simon, T.; Kim, J.S.; Jeng, J.-S.; et al. Acute dual antiplatelet therapy for minor ischaemic stroke or transient ischaemic attack. BMJ 2019, 364, l895. [Google Scholar] [CrossRef] [Green Version]
- Serebruany, V.L.; Pokov, A.N.; Fortmann, S.D.; DiNicolantonio, J.J. Disbalance between mortality and non-fatal vascular events in the CHAMPION-PHOENIX trial: The cangrelor efficacy challenge. Thromb. Haemost. 2014, 111, 3–7. [Google Scholar]
- Watala, C.; Ulicna, O.; Golanski, J.; Nocun, M.; Waczulikova, I.; Markuszewski, L.; Drzewoski, J. High glucose contributes to aspirin insensitivity in streptozotocin-diabetic rats: A multiparametric aggregation study. Blood Coagul. Fibrinolysis 2006, 17, 113–124. [Google Scholar] [CrossRef]

{kind=link}
Table 1.
Adenosine receptors (AR) receptor distribution and expression in different tissue types.
| Receptor Subtype | High Expression | Intermediary Expression | Low Expression |
|---|---|---|---|
| A1 [19] | brain (cortex, hippocampus, cerebellum); spinal cord; adrenal gland; atria; eyes | brain (excluding cortex, hippocampus, and cerebellum); skeletal muscles; adipose tissue; liver; kidneys | lungs; pancreas |
| A2A [20] | blood platelets; leukocytes; spleen; thymus | heart; lungs; blood vessels; peripheral nerves | brain |
| A2B [21,22,23] | cecum; bladder | lungs; blood vessels; mast cells; eyes | brain; adipose tissue; blood platelets; adrenal gland; kidneys |
| A3 [19] | testis; mast cells | brain (hippocampus, cerebellum) | brain (excluding hippocampus and cerebellum); heart; thyroid; adrenal gland; spleen; liver; kidneys |
Table 2.
Nomenclature and chemical structure of AR agonists.
| Name | Other Names | IUPAC Name | Structure |
|---|---|---|---|
| 2-chloroadenosine | 2-Chloro Adenosine, Cl-Ado, 2 ClAdo, 2-CADO | (2R,3R,4S,5R)-2-(6-amino-2-chloropurin-9-yl)-5-(hydroxymethyl)oxolane-3,4-diol |  |
| Regadenoson | CVT 3146, CVT-3146, CVT3146, Lexiscan, Rapiscan | 1-[6-amino-9-[(2R,3R,4S,5R)-3,4-dihydroxy-5-(hydroxymethyl)oxolan-2-yl]purin-2-yl]-N-methylpyrazole-4-carboxamide |  |
| Binodenoson | 2-((Cyclohexylmethylene) hydrazino)adenosine | (2R,3R,4S,5R)-2-{6-amino-2-[(E)-2-(cyclohexylmethylidene)hydrazin-1-yl]-9H-purin-9-yl}-5-(hydroxymethyl)oxolane-3,4-diol |  |
| PSB-0777 | PSB0777 | 4-[2-[(6-Amino-9-b-D-ribofuranosyl-9H-purin-2-yl) thio]ethyl]benzenesulfonic acid ammonium salt |  |
| PSB-15826 | - | (2S,3S,4R,5R)-5-(6-Amino-2-((2-(4-(4-fluorophenyl)piperazin-1-yl) ethyl)thio)-9H-purin-9-yl)tetrahydrofuran-2,3,4-triol |  |
| PSB-12404 | - | (2R,3R,4S,5R)-2-(6-Amino-2-(2-cyclohexylethylthio)-9Hpurin-9-yl)-5-(hydroxymethyl)tetrahydrofuran-3,4-diol |  |
| PSB-16301 | - | (2S,3S,4R,5R)-5-(6-amino-2-(phenethylthio)-9H-purin-9-yl)tetrahydrofuran-2,3,4-triol |  |
| MRE0094 | Sonedenoson, 2-[2-(4-Chlorophenyl)ethoxy]adenosine | (2R,3R,4S,5R)-2-[6-amino-2-[2-(4-chlorophenyl)ethoxy]purin-9-yl]-5-(hydroxymethyl)oxolane-3,4-diol |  |
| CV1808 | 2-phenylaminoadenosine, CV-1808 | (2R,3R,4S,5R)-2-(6-amino-2-anilinopurin-9-yl)-5-(hydroxymethyl)oxolane-3,4-diol |  |
| AMP597 | RPR 100579 | (1S,2R,3S,4R)-4-(4-(((R)-1-(3-chlorothiophen-2-yl)butan-2-yl)amino)-7H-pyrrolo [2,3-d]pyrimidin-7-yl)-N-ethyl-2,3-dihydroxycyclopentane-1-carboxamide |  |
| NECA | N-Ethyl-5’-Carboxamido Adenosine, 5’-ethylcarboxamidoadenosine | (2S,3S,4R,5R)-5-(6-aminopurin-9-yl)-N-ethyl-3,4-dihydroxyoxolane-2-carboxamide |  |
| CGS21680 | CGS-21680, Cgs 21680, 2-(4-(2-carboxyethyl)phenethylamino)-5’-N-ethylcarboxamidoadenosine | 3-[4-[2-[[6-amino-9-[(2R,3R,4S,5S)-5-(ethylcarbamoyl)-3,4-dihydroxyoxolan-2-yl]purin-2-yl]amino]ethyl]phenyl]propanoic acid |  |
| HE-NECA | HENECA, Heneca, 2-hexynyl-NECA, 2-hexynyladenosine-5’-N-ethylcarboxamide | (2S,3S,4R,5R)-5-(6-amino-2-hex-1-ynylpurin-9-yl)-N-ethyl-3,4-dihydroxyoxolane-2-carboxamide |  |
| UK-432097 | UK-432,097 | 6-(2,2-diphenylethylamino)-9-[(2R,3R,4S,5S)-5-(ethylcarbamoyl)-3,4-dihydroxyoxolan-2-yl]-N-[2-[(1-pyridin-2-ylpiperidin-4-yl)carbamoylamino]ethyl]purine-2-carboxamide |  |
| BAY 60-6583 | BAY-60-6583, BAY60-6583, 2-((6-amino-3,5-dicyano-4-(4-(cyclopropylmethoxy)phenyl)pyridin-2 yl) sulfanyl)acetamide | 2-[6-amino-3,5-dicyano-4-[4-(cyclopropylmethoxy)phenyl]pyridin -2-yl]sulfanylacetamide |  |
| LUF5834 | LUF 5834, LUF-5834, 2-Amino-4-(4-hydroxy-phenyl)-6-(1H-imidazol-2-ylmethylsulfanyl)-pyridine-3,5-dicarbonitrile | 2-amino-6-(1H-imidazol-2-ylmethylsulfanyl)-4-(4-oxocyclohexa-2,5-dien-1-ylidene)-1H-pyridine-3,5-dicarbonitrile |  |
| LUF5835 | LUF 5835, LUF-5835 | 2-amino-6-(1H-imidazol-2-ylmethylsulfanyl)--4-(3-hydroxy-phenyl) pyridine-3,5dicarbonitrile |  |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wolska, N.; Rozalski, M. Blood Platelet Adenosine Receptors as Potential Targets for Anti-Platelet Therapy. Int. J. Mol. Sci. 2019, 20, 5475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20215475
AMA Style
Wolska N, Rozalski M. Blood Platelet Adenosine Receptors as Potential Targets for Anti-Platelet Therapy. International Journal of Molecular Sciences. 2019; 20(21):5475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20215475
Chicago/Turabian StyleWolska, Nina, and Marcin Rozalski. 2019. "Blood Platelet Adenosine Receptors as Potential Targets for Anti-Platelet Therapy" International Journal of Molecular Sciences 20, no. 21: 5475. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20215475
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.