The Precursor for Nerve Growth Factor (proNGF) in Thyroid Cancer Lymph Node Metastases: Correlation with Primary Tumour and Pathological Variables

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
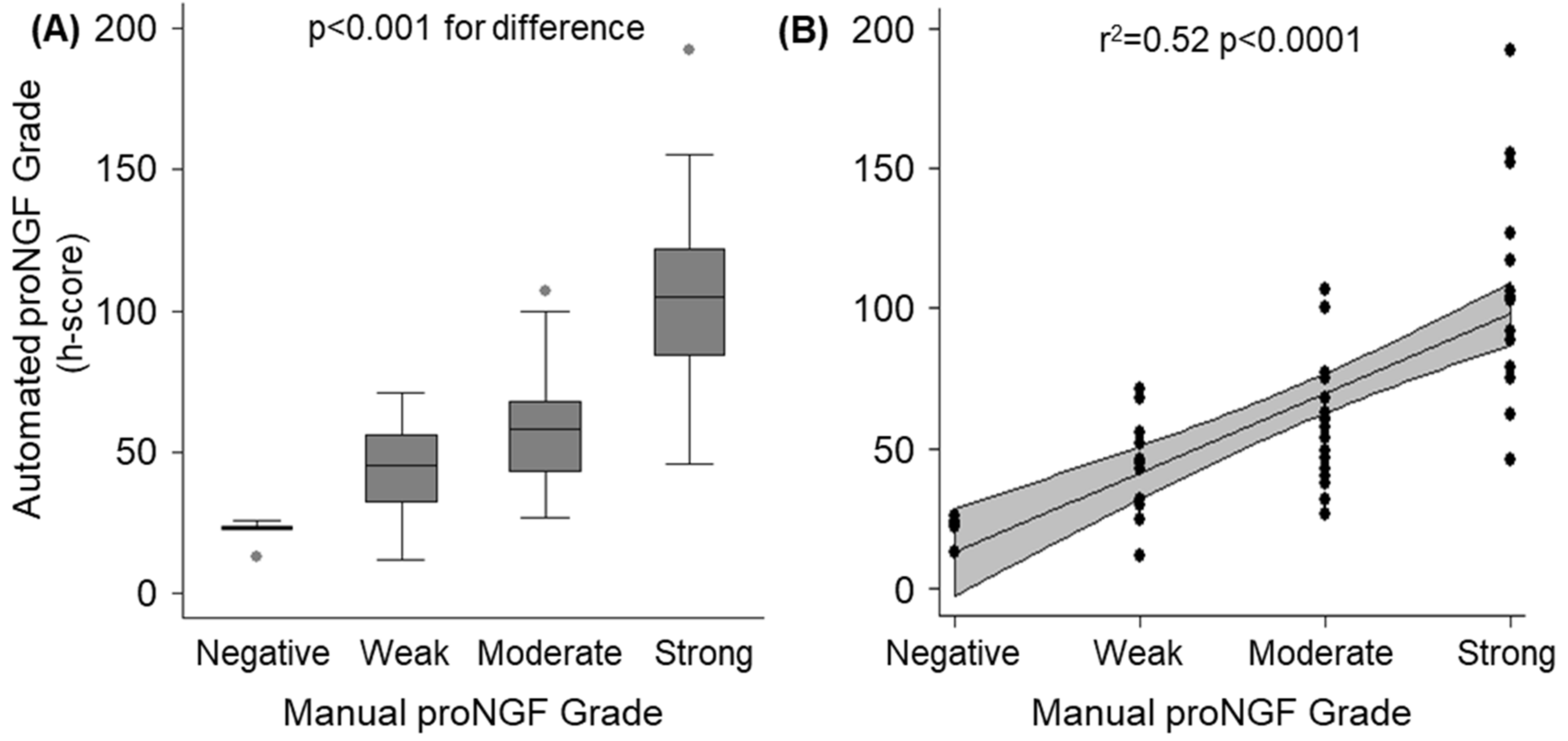
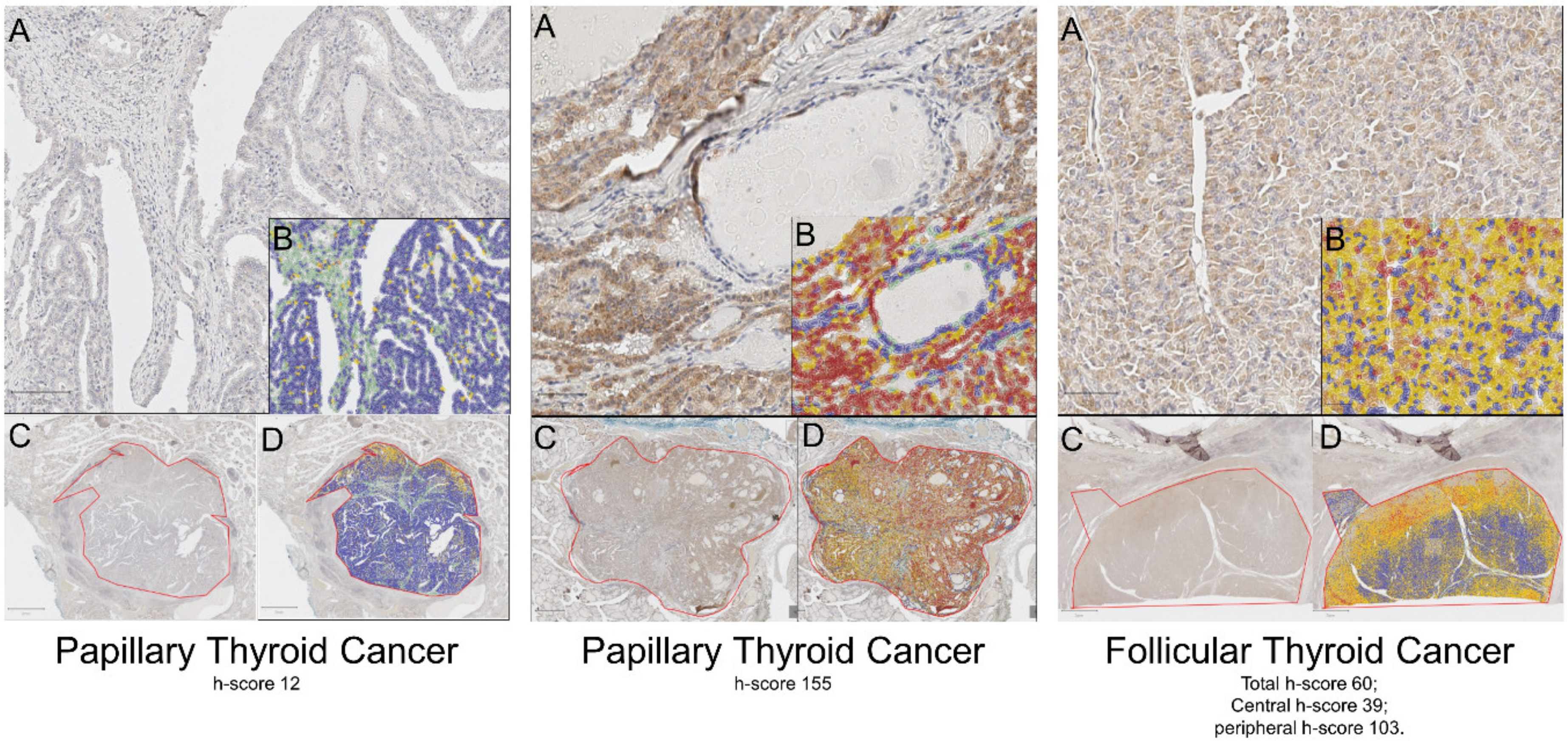
2.1. Validation of Automated Scoring Algorithm (h-score)
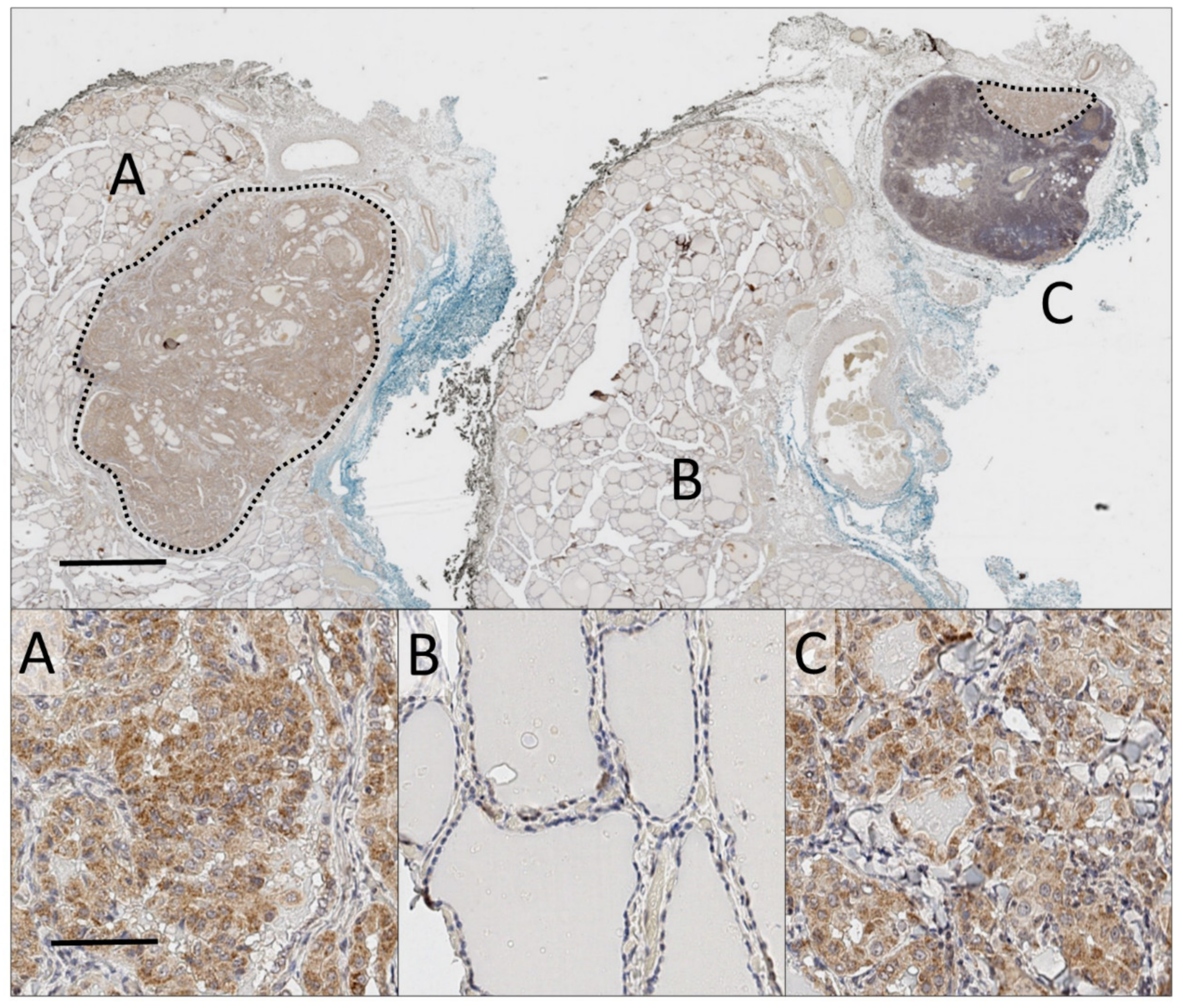
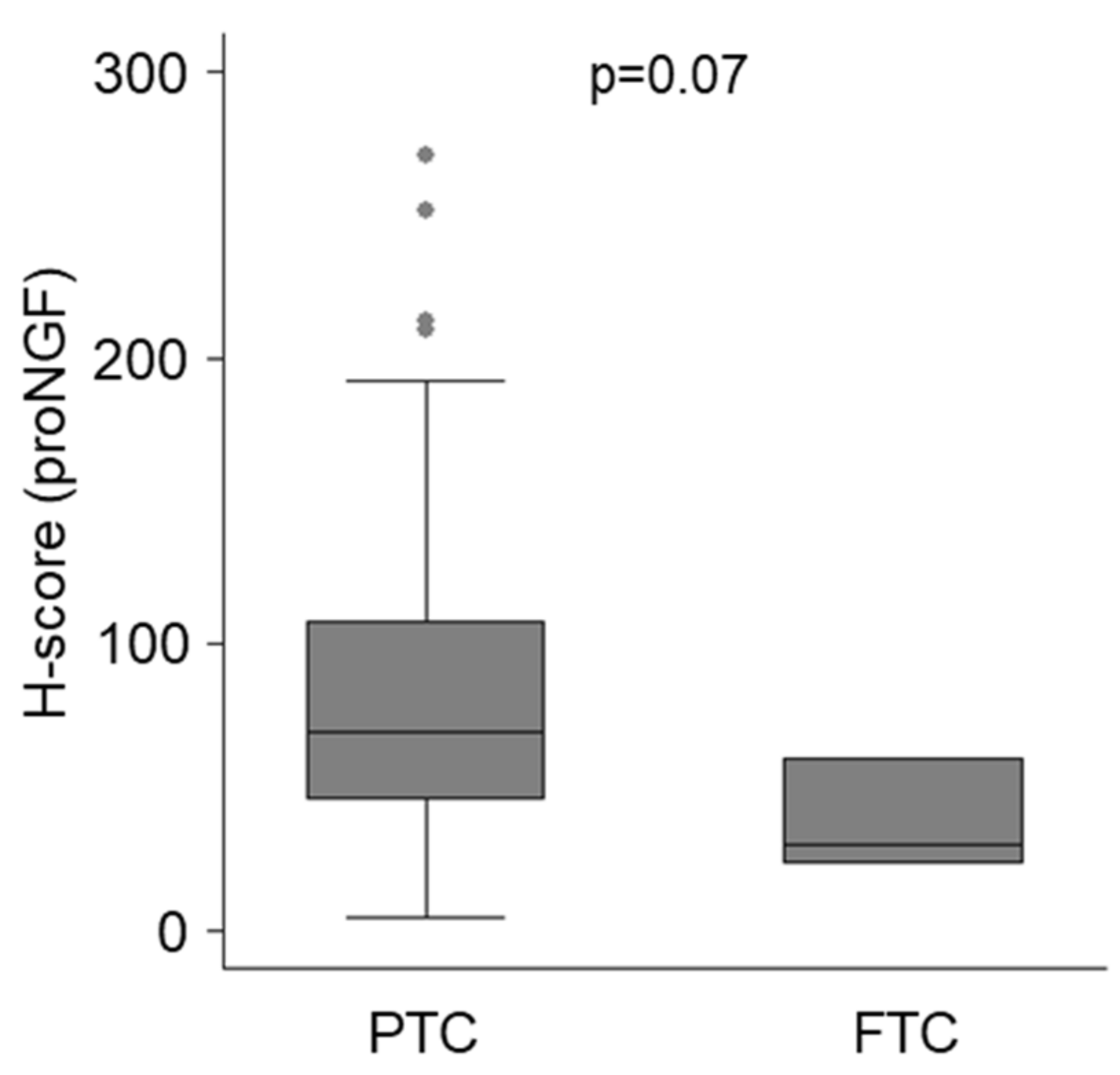
2.2. ProNGF Expression in Thyroid Cancer
2.3. ProNGF Expression in Lymph Node Metastases Positively Correlates with Primary Tumours
2.4. ProNGF Expression is not Associated with High Risk Clinical Features
2.5. ProNGF Expression in Primary Tumours does not Predict Metastases
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
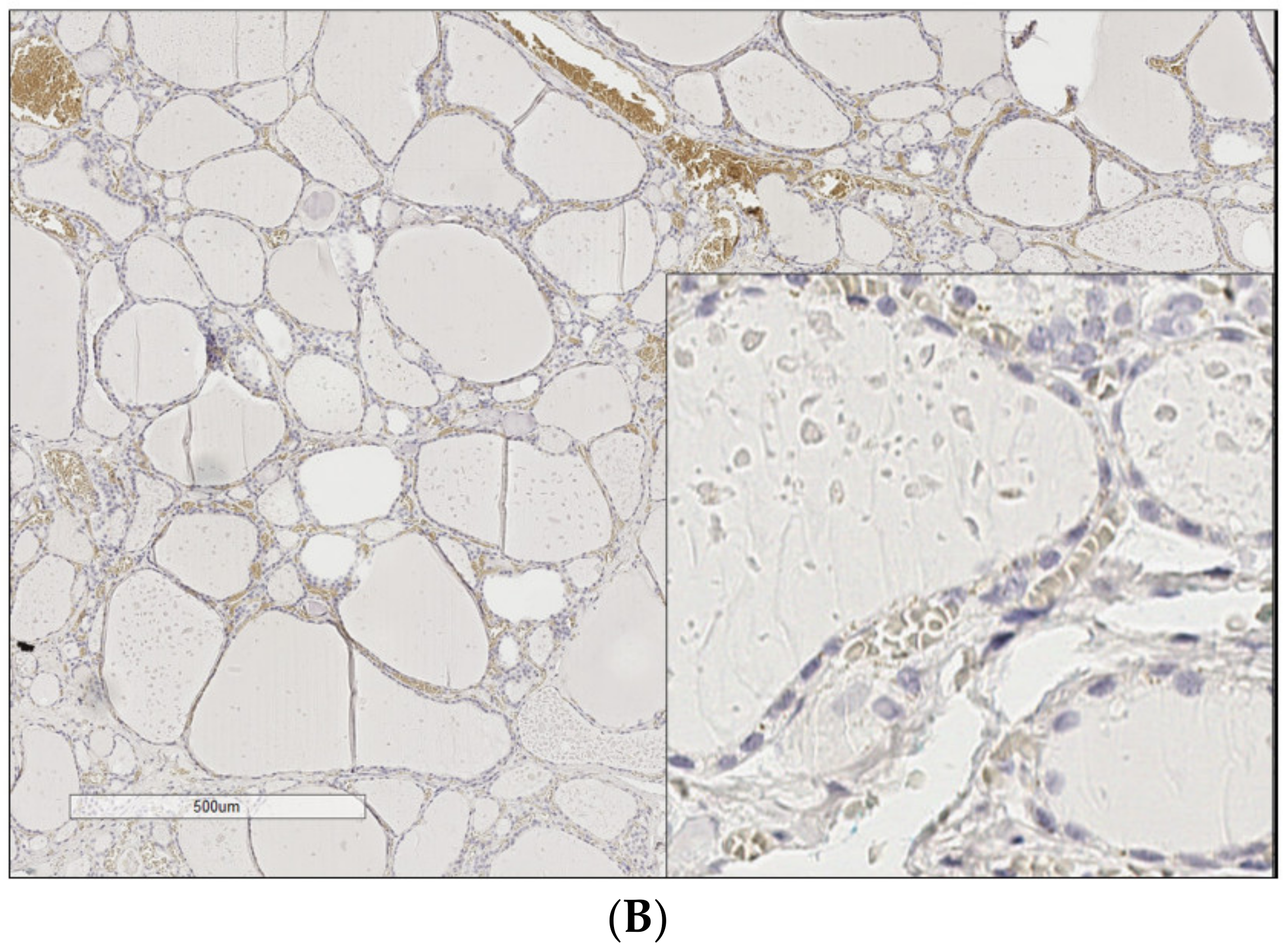
4.2. Immunohistochemistry
4.3. Digital Quantification
4.4. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AJCC | American Joint Committee on Cancer |
| DAB | 3′3′ diaminobenzidine |
| ProNGF | Precursor for nerve growth factor |
| TNM | Tumour, Nodes, Metastases Staging System |
Appendix A


Appendix B

References
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974-2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Sciuto, R.; Romano, L.; Rea, S.; Marandino, F.; Sperduti, I.; Maini, C.L. Natural history and clinical outcome of differentiated thyroid carcinoma: A retrospective analysis of 1503 patients treated at a single institution. Ann. Oncol. 2009, 20, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Randolph, G.W.; Duh, Q.Y.; Heller, K.S.; LiVolsi, V.A.; Mandel, S.J.; Steward, D.L.; Tufano, R.P.; Tuttle, R.M. American Thyroid Association Surgical Affairs Committee’s Taskforce on Thyroid Cancer Nodal Surgery. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 2012, 22, 1144–1152. [Google Scholar] [PubMed]
- Sugitani, I.; Kasai, N.; Fujimoto, Y.; Yanagisawa, A. A novel classification system for patients with PTC: Addition of the new variables of large (3 cm or greater) nodal metastases and reclassification during the follow-up period. Surgery 2004, 135, 139–148. [Google Scholar] [CrossRef]
- Hondermarck, H. Neurotrophins and their receptors in breast cancer. Cytokine Growth Factor Rev. 2012, 23, 357–365. [Google Scholar] [CrossRef]
- Adriaenssens, E.; Vanhecke, E.; Saule, P.; Mougel, A.; Page, A.; Romon, R.; Nurcombe, V.; Le Bourhis, X.; Hondermarck, H. Nerve growth factor is a potential therapeutic target in breast cancer. Cancer Res. 2008, 68, 346–351. [Google Scholar] [CrossRef]
- Pundavela, J.; Demont, Y.; Jobling, P.; Lincz, L.F.; Roselli, S.; Thorne, R.F.; Bond, D.; Bradshaw, R.A.; Walker, M.M.; Hondermarck, H. ProNGF correlates with Gleason score and is a potential driver of nerve infiltration in prostate cancer. Am. J. Pathol. 2014, 184, 3156–3162. [Google Scholar] [CrossRef]
- Hayakawa, Y.; Sakitani, K.; Konishi, M.; Asfaha, S.; Niikura, R.; Tomita, H.; Renz, B.W.; Tailor, Y.; Macchini, M.; Middelhoff, M.; et al. Nerve Growth Factor Promotes Gastric Tumorigenesis through Aberrant Cholinergic Signaling. Cancer Cell 2017, 31, 21–34. [Google Scholar] [CrossRef]
- Renz, B.W.; Takahashi, R.; Tanaka, T.; Macchini, M.; Hayakawa, Y.; Dantes, Z.; Maurer, H.C.; Chen, X.; Jiang, Z.; Westphalen, C.B.; et al. beta2 Adrenergic-Neurotrophin Feedforward Loop Promotes Pancreatic Cancer. Cancer Cell 2018, 33, 75–90. [Google Scholar] [CrossRef]
- Faulkner, S.; Roselli, S.; Demont, Y.; Pundavela, J.; Choquet, G.; Leissner, P.; Oldmeadow, C.; Attia, J.; Walker, M.M.; Hondermarck, H. ProNGF is a potential diagnostic biomarker for thyroid cancer. Oncotarget 2016, 7, 28488–28497. [Google Scholar] [CrossRef] [PubMed]
- Demont, Y.; Corbet, C.; Page, A.; Ataman-Önal, Y.; Choquet-Kastylevsky, G.; Fliniaux, I.; Le Bourhis, X.; Toillon, R.A.; Bradshaw, R.A.; Hondermarck, H. Pro-nerve Growth Factor Induces Autocrine Stimulation of Breast Cancer Cell Invasion through Tropomyosin-related Kinase A (TrkA) and Sortilin Protein. J. Biol. Chem. 2012, 287, 1923–1931. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, R.A.; Pundavela, J.; Biarc, J.; Chalkley, R.J.; Burlingame, A.L.; Hondermarck, H. NGF and ProNGF: Regulation of neuronal and neoplastic responses through receptor signaling. Adv. Biol. Regul. 2015, 58, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Tomellini, E.; Touil, Y.; Lagadec, C.; Julien, S.; Ostyn, P.; Ziental-Gelus, N.; Meignan, S.; Lengrand, J.; Adriaenssens, E.; Polakowska, R.; et al. Nerve growth factor and proNGF simultaneously promote symmetric self-renewal, quiescence, and epithelial to mesenchymal transition to enlarge the breast cancer stem cell compartment. Stem Cells 2015, 33, 342–353. [Google Scholar] [CrossRef]
- Pundavela, J.; Roselli, S.; Faulkner, S.; Attia, J.; Scott, R.J.; Thorne, R.F.; Forbes, J.F.; Bradshaw, R.A.; Walker, M.M.; Jobling, P.; et al. Nerve fibers infiltrate the tumor microenvironment and are associated with nerve growth factor production and lymph node invasion in breast cancer. Mol. Oncol. 2015, 9, 1626–1635. [Google Scholar] [CrossRef]
- Magnon, C.; Hall, S.J.; Lin, J.; Xue, X.; Gerber, L.; Freedland, S.J.; Frenette, P.S. Autonomic Nerve Development Contributes to Prostate Cancer Progression. Science 2013, 341, 1236361. [Google Scholar] [CrossRef]
- Boilly, B.; Faulkner, S.; Jobling, P.; Hondermarck, H. Nerve Dependence: From Regeneration to Cancer. Cancer Cell 2017, 31, 342–354. [Google Scholar] [CrossRef]
- Zhao, C.-M.; Hayakawa, Y.; Kodama, Y.; Muthupalani, S.; Westphalen, C.B.; Andersen, G.T.; Flatberg, A.; Johannessen, H.; Friedman, R.A.; Renz, B.W.; et al. Denervation suppresses gastric tumorigenesis. Sci. Transl. Med. 2014, 6, 250ra115. [Google Scholar] [CrossRef]
- Peterson, S.C.; Eberl, M.; Vagnozzi, A.N.; Belkadi, A.; Veniaminova, N.A.; Verhaegen, M.E.; Bichakjian, C.K.; Ward, N.L.; Dlugosz, A.A.; Wong, S.Y. Basal cell carcinoma preferentially arises from stem cells within hair follicle and mechanosensory niches. Cell Stem Cell 2015, 16, 400–412. [Google Scholar] [CrossRef]
- Zahalka, A.H.; Arnal-Estape, A.; Maryanovich, M.; Nakahara, F.; Cruz, C.D.; Finley, L.W.S.; Frenette, P.S. Adrenergic nerves activate an angio-metabolic switch in prostate cancer. Science 2017, 358, 321–326. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernandez, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ProNGF Quantification (h-score) | ||||||
|---|---|---|---|---|---|---|
| n | Primary Tumour | p-Value | n | Nodal Metastasis | p-Value | |
| Overall | 56 | 57 (42–84) | 56 | 94 (50–147) | 0.002 1 | |
| Age | 0.96 | 0.32 | ||||
| <55 years | 34 | 58 (43–89) | 34 | 95 (57–122) | ||
| ≥55 years | 22 | 55 (32–77) | 22 | 86 (46–123) | ||
| Sex | 0.20 | 0.85 | ||||
| Male | 21 | 71 (46–100) | 21 | 96 (46–148) | ||
| Female | 35 | 54 (40–71) | 35 | 90 (51–146) | ||
| Histopathology | 0.36 | 0.11 | ||||
| Papillary | 53 | 58 (43–89) | 53 | 96 (51–148) | ||
| Classical | 27 | 54 (43–92) | 27 | 106 (64–149) | ||
| Follicular-variant | 26 | 60 (46–89) | 26 | 70 (49–130) | ||
| Follicular | 2 | 42 (23–60) | 2 | 45 (30–60) | ||
| Anaplastic | 1 | 32 | 1 | 67 | ||
| Tumour size | 0.02 | |||||
| Primary <4 cm | 48 | 62 (45–96) | ||||
| Primary ≥4 cm | 8 | 38 (25–55) | ||||
| Total lymph node <3 cm | 44 | 105 (57–149) | 0.02 | |||
| Total lymph node ≥3 cm | 12 | 59 (44–64) | ||||
| Metastasis within node <2 mm | 10 | 148 (94–175) | 0.04 | |||
| Metastasis within node ≥2 mm | 46 | 82 (49–123) | ||||
| Vascular invasion | 0.32 | |||||
| Absent | 35 | 56 (43–100) | ||||
| Present | 21 | 58 (43–68) | ||||
| Extra-thyroidal extension | 0.43 | |||||
| Absent | 19 | 56 (45–106) | ||||
| Present | 37 | 58 (40–75) | ||||
| AJCC TNM 8 Stage | 0.005 | |||||
| I and II | 46 | 63 (45–100) | ||||
| III and IV | 10 | 38 (23–54) | ||||
| Nodal metastases (location) | 0.004 | |||||
| Central neck only (N1a) | 33 | 109 (64–152) | ||||
| Central + lateral neck (N1b) | 23 | 60 (40–96) | ||||
| Timing of metastases | 0.11 | |||||
| At time of primary tumour | 49 | 99 (56–148) | ||||
| >6 months from primary | 7 | 57 (46–96) | ||||
| Parameter | Estimate (95% CI) | p-Value |
|---|---|---|
| (A) Primary Tumour: | ||
| Age (>= 55 years) | −6.1 (−35.9 to 23.7) | 0.7 |
| Sex (male) | −2.7 (−27.3 to 21.8) | 0.8 |
| Size (>= 4 cm) | −9.1 (−28.8 to 10.6) | 0.4 |
| Extra-thyroidal extension | −14 (−29.0 to 1.0) | 0.067 |
| Vascular Invasion | −11.6 (−36.4 to 13.2) | 0.4 |
| Multi-focal | −1.7 (−19.1 to 15.7) | 0.8 |
| (B) Lymph node metastasis | ||
| Age (>= 55 years) | −13.8 (−32.5 to 4.9) | 0.1 |
| Sex (male) | −34.8 (−59.9 to −9.6) | 0.008 |
| Size (>= 2 mm) | −29.1 (−65.34 to 7.2) | 0.1 |
| Location (lateral neck site, N1b) | −47.1 (−73.8 to −20.5) | 0.001 |
| Timing (> 6 months post primary) | −23.7 (−52 to 4.6) | 0.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowe, C.W.; Dill, T.; Faulkner, S.; Gedye, C.; Paul, J.W.; Tolosa, J.M.; Jones, M.; King, S.; Smith, R.; Hondermarck, H. The Precursor for Nerve Growth Factor (proNGF) in Thyroid Cancer Lymph Node Metastases: Correlation with Primary Tumour and Pathological Variables. Int. J. Mol. Sci. 2019, 20, 5924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235924
Rowe CW, Dill T, Faulkner S, Gedye C, Paul JW, Tolosa JM, Jones M, King S, Smith R, Hondermarck H. The Precursor for Nerve Growth Factor (proNGF) in Thyroid Cancer Lymph Node Metastases: Correlation with Primary Tumour and Pathological Variables. International Journal of Molecular Sciences. 2019; 20(23):5924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235924
Chicago/Turabian StyleRowe, Christopher W., Tony Dill, Sam Faulkner, Craig Gedye, Jonathan W. Paul, Jorge M. Tolosa, Mark Jones, Simon King, Roger Smith, and Hubert Hondermarck. 2019. "The Precursor for Nerve Growth Factor (proNGF) in Thyroid Cancer Lymph Node Metastases: Correlation with Primary Tumour and Pathological Variables" International Journal of Molecular Sciences 20, no. 23: 5924. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235924