SYK Targeting Represents a Potential Therapeutic Option for Relapsed Resistant Pediatric ETV6-RUNX1 B-Acute Lymphoblastic Leukemia Patients

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
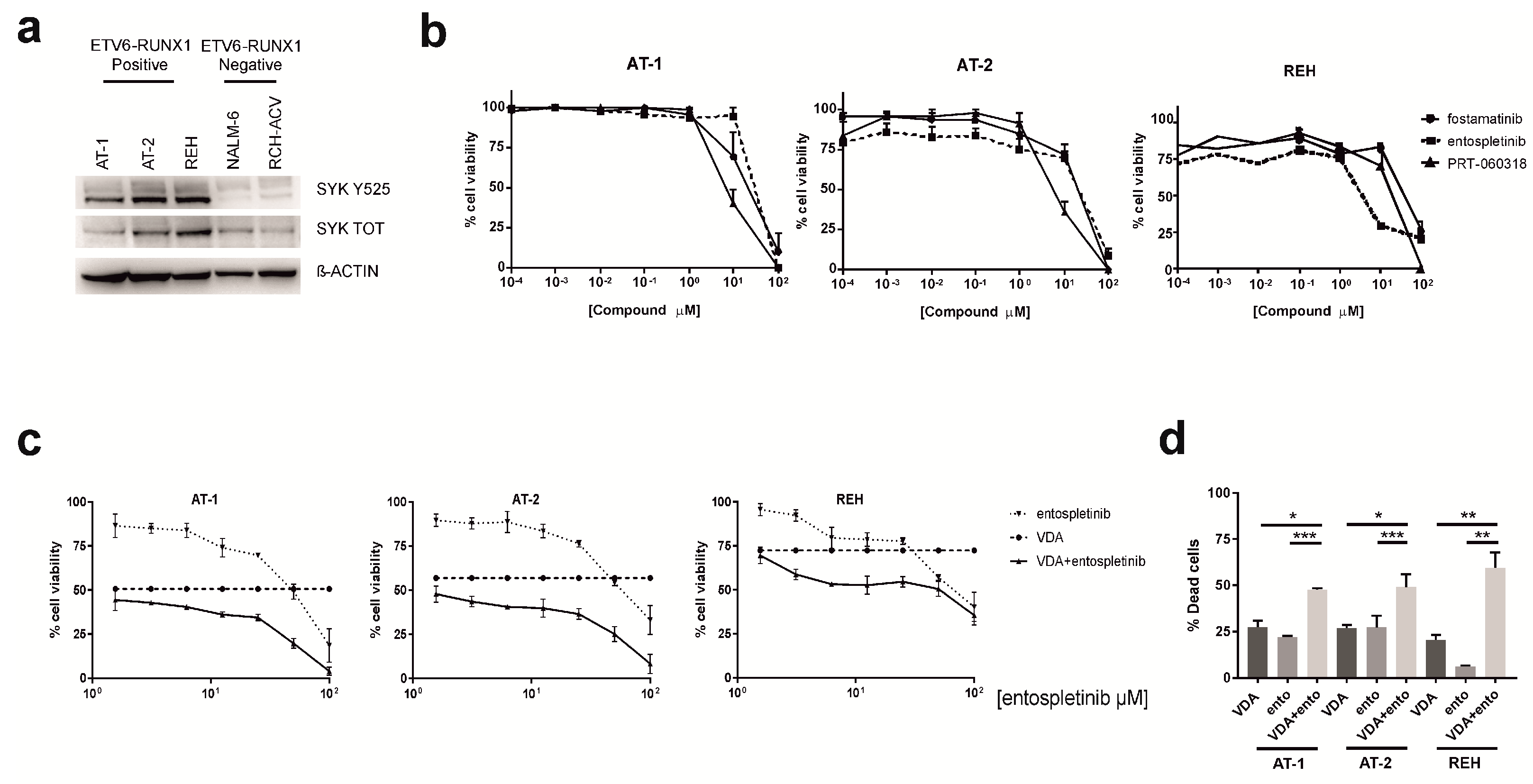
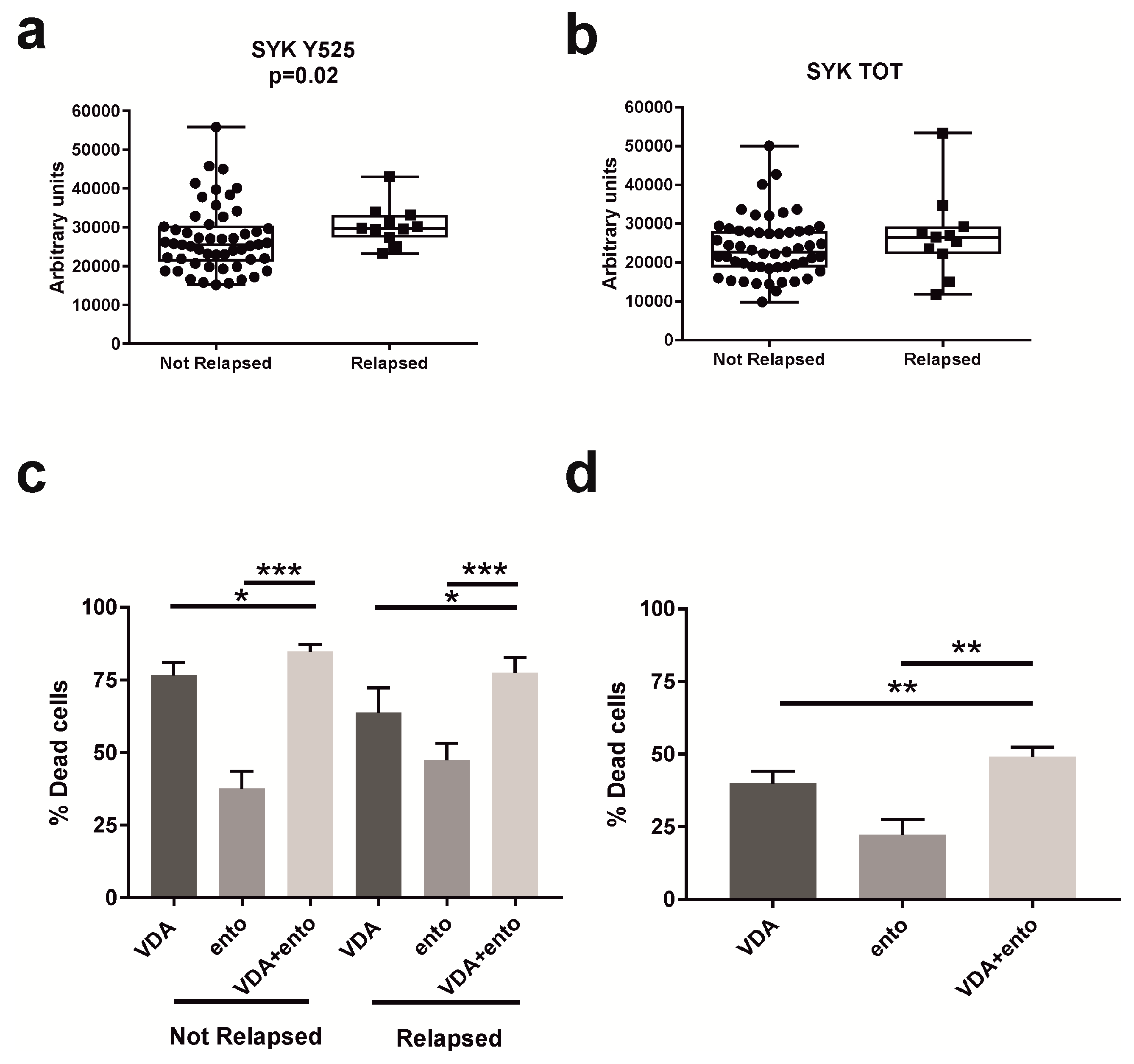
2. Results
3. Discussion
4. Materials and Methods
4.1. Cell Lines and Primary Samples
4.2. SYK Inhibitors
4.3. MTT Assay
4.4. Annexin V-PI Assay
4.5. Western Blot
4.6. Phospho-Flow Cytometry
4.7. RPPA
4.8. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morrow, M.; Horton, S.; Kioussis, D.; Brady, H.J.; Williams, O. TEL-AML1 promotes development of specific hematopoietic lineages consistent with preleukemic activity. Blood 2004, 103, 3890–3896. [Google Scholar] [CrossRef] [PubMed]
- Chow, C.D.; Dalla-Pozza, L.; Gottlieb, D.J.; Hertzberg, M.S. Two cases of very late relapsing ALL carrying the TEL-AML1 fusion gene. Leukemia 1999, 13, 1893–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franca, R.; Favretto, D.; Granzotto, M.; Decorti, G.; Rabusin, M.; Stocco, G. Epratuzumab and Blinatumomab as Therapeutic Antibodies for Treatment of Pediatric Acute Lymphoblastic Leukemia: Current Status and Future Perspectives. Curr. Med. Chem. 2017, 24, 1050–1065. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, A.; Eckert, C.; Meyr, F.; Koerner, G.; von Stackelberg, A.; Ullmann, R.; Türkmen, S.; Henze, G.; Seeger, K. Copy number genome alterations are associated with treatment response and outcome in relapsed childhood ETV6/RUNX1-positive acute lymphoblastic leukemia. Haematologica 2014, 99, 706–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perova, T.; Grandal, I.; Nutter, L.M.; Papp, E.; Matei, I.R.; Beyene, J.; Kowalski, P.E.; Hitzler, J.K.; Minden, M.D.; Guidos, C.J.; et al. Therapeutic potential of spleen tyrosine kinase inhibition for treating high-risk precursor B cell acute lymphoblastic leukemia. Sci. Transl. Med. 2014, 6, 236ra62. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.; Schweighoffer, E.; Colucci, F.; Di Santo, J.P.; Tybulewicz, V.L. Tyrosine kinase SYK: Essential functions for immunoreceptor signalling. Immunol. Today 2000, 21, 148–154. [Google Scholar] [CrossRef]
- Mócsai, A.; Ruland, J.; Tybulewicz, V.L.J. The SYK tyrosine kinase: A crucial player in diverse biological functions. Nat. Rev. Immunol 2010, 10, 387–402. [Google Scholar] [CrossRef] [PubMed]
- Leseux, L.; Hamdi, S.M.; Al Saati, T.; Capilla, F.; Recher, C.; Laurent, G.; Bezombes, C. Syk-dependent mTOR activation in follicular lymphoma cells. Blood 2006, 108, 4156–4162. [Google Scholar] [CrossRef] [PubMed]
- Köhrer, S.; Havranek, O.; Seyfried, F.; Hurtz, C.; Coffey, G.P.; Kim, E.; Ten Hacken, E.; Jäger, U.; Vanura, K.; O′Brien, S.; et al. Pre-BCR signaling in precursor B-cell acute lymphoblastic leukemia regulates PI3K/AKT, FOXO1 and, M.Y.C.; and can be targeted by SYK inhibition. Leukemia 2016, 30, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Serafin, V.; Capuzzo, G.; Milani, G.; Minuzzo, S.A.; Pinazza, M.; Bortolozzi, R.; Bresolin, S.; Porcù, E.; Frasson, C.; Indraccolo, S.; et al. Glucocorticoid resistance is reverted by LCK inhibition in pediatric T-cell acute lymphoblastic leukemia. Blood 2017, 130, 2750–2761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wossning, T.; Herzog, S.; Köhler, F.; Meixlsperger, S.; Kulathu, Y.; Mittler, G.; Abe, A.; Fuchs, U.; Borkhardt, A.; Jumaa, H. Deregulated Syk inhibits differentiation and induces growth factor-independent proliferation of pre-B cells. J. Exp. Med. 2006, 203, 2829–2840. [Google Scholar] [CrossRef] [PubMed]
- Boros, K.; Puissant, A.; Back, M.; Alexe, G.; Bassil, C.F.; Sinha, P. Increased SYK activity is associated with unfavorable outcome among patients with acute myeloid leukemia. Oncotarget 2015, 6, 25575–25587. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.S.; Kropf, J.E.; Lee, T.; Blomgren, P.; Xu, J.; Zhao, Z.; Gallion, S.; Whitney, J.A.; Maclin, D.; Lansdon, E.B.; et al. Discovery of GS-9973, a selective and orally efficacious inhibitor of spleen tyrosine kinase. J. Med. Chem. 2014, 57, 3856–3873. [Google Scholar] [CrossRef] [PubMed]
- Grausenburger, R.; Bastelberger, S.; Eckert, C.; Kauer, M.; Stanulla, M.; Frech, C.; Bauer, E.; Stoiber, D.; von Stackelberg, A.; Attarbaschi, A.; et al. Genetic alterations in glucocorticoid signaling pathway components are associated with adverse prognosis in children with relapsed ETV6/RUNX1-positive acute lymphoblastic leukemia. Leuk. Lymphoma 2016, 57, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Markham, A. Fostamatinib: First Global Approval. Drugs 2018, 78, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Reilly, M.P.; Sinha, U.; André, P.; Taylor, S.M.; Pak, Y.; Deguzman, F.R.; Nanda, N.; Pandey, A.; Stolla, M.; Bergmeier, W.; et al. PRT-060318, a novel Syk inhibitor, prevents heparin-induced thrombocytopenia and thrombosis in a transgenic mouse model. Blood 2011, 117, 2241–2246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conter, V.; Bartram, C.R.; Valsecchi, M.G.; Schrauder, A.; Panzer-Grümayer, R.; Möricke, A.; Aricò, M.; Zimmermann, M.; Mann, G.; De Rossi, G.; et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: Results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood 2010, 115, 3206–3214. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.C.; Talalay, P. Quantitative analysis of dose-effect relationships: The combined effects of multiple drugs or enzyme inhibitors. Adv. Enzyme Regul. 1984, 22, 27–55. [Google Scholar] [CrossRef]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serafin, V.; Porcù, E.; Cortese, G.; Mariotto, E.; Veltri, G.; Bresolin, S.; Basso, G.; Accordi, B. SYK Targeting Represents a Potential Therapeutic Option for Relapsed Resistant Pediatric ETV6-RUNX1 B-Acute Lymphoblastic Leukemia Patients. Int. J. Mol. Sci. 2019, 20, 6175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246175
Serafin V, Porcù E, Cortese G, Mariotto E, Veltri G, Bresolin S, Basso G, Accordi B. SYK Targeting Represents a Potential Therapeutic Option for Relapsed Resistant Pediatric ETV6-RUNX1 B-Acute Lymphoblastic Leukemia Patients. International Journal of Molecular Sciences. 2019; 20(24):6175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246175
Chicago/Turabian StyleSerafin, Valentina, Elena Porcù, Giuliana Cortese, Elena Mariotto, Giulia Veltri, Silvia Bresolin, Giuseppe Basso, and Benedetta Accordi. 2019. "SYK Targeting Represents a Potential Therapeutic Option for Relapsed Resistant Pediatric ETV6-RUNX1 B-Acute Lymphoblastic Leukemia Patients" International Journal of Molecular Sciences 20, no. 24: 6175. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20246175