Bone Marrow Mast Cell Antibody-Targetable Cell Surface Protein Expression Profiles in Systemic Mastocytosis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. SM Patients and Samples
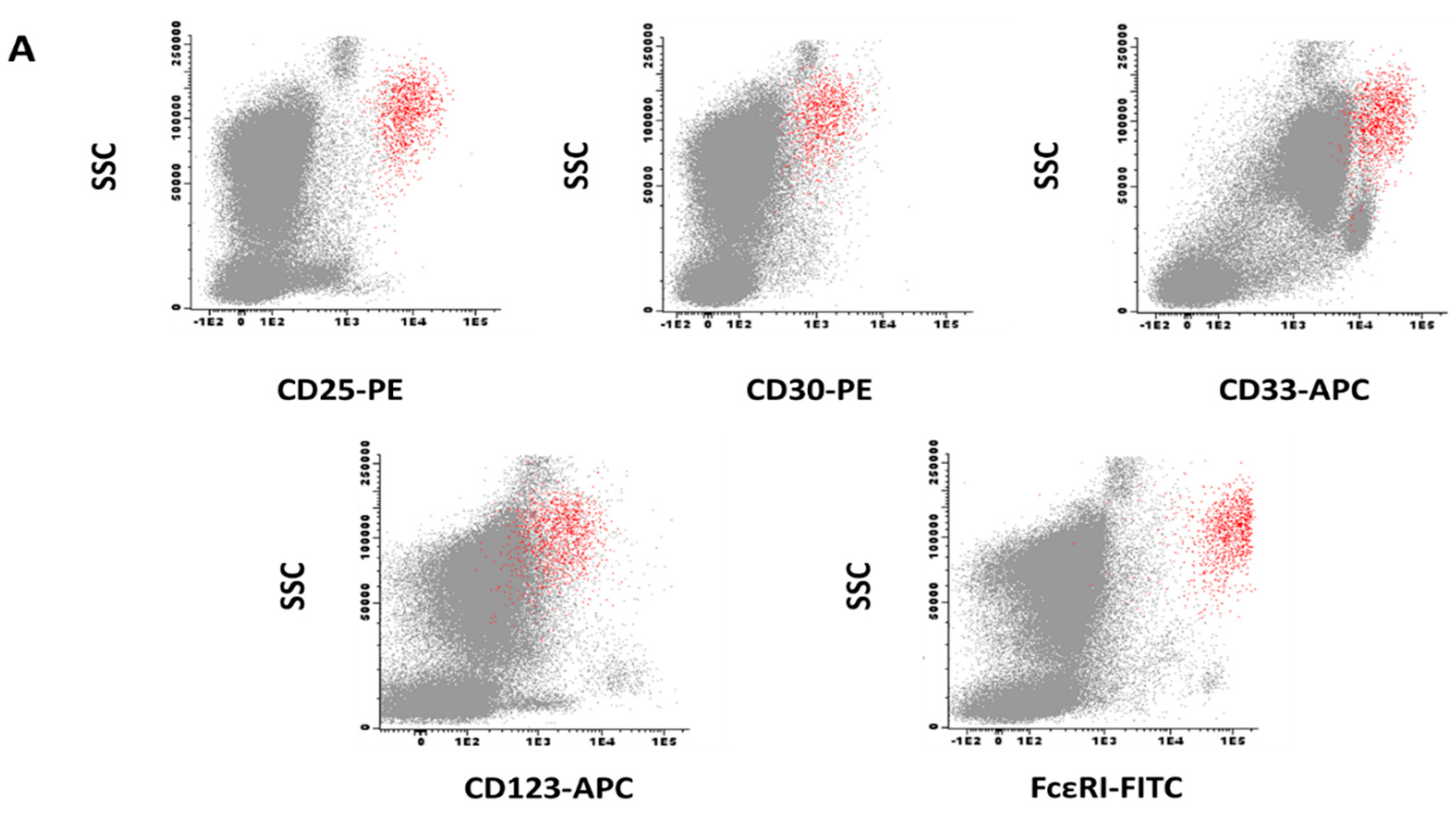
2.2. Immuno-Phenotypic Characteristics of Normal/Reactive BMMC
2.3. Immuno-Phenotypic Features of BMMC from SM Patients
2.4. Immuno-Phenotypic Features of BMMC from Patients with Different Diagnostic and Prognostic Categories of SM
3. Discussion
4. Materials and Methods
4.1. Patients, Controls, and Samples
4.2. Multi-Parameter Flow Cytometry Immuno-Phenotypic Studies
4.3. Statistical Methods
Author Contributions
Funding
Acknowledgments
Ethics Approval and Consent to Participate
Conflicts of Interest
Abbreviations
| ADC ADCC ADCP | Antibody-drug conjugate Antibody-dependent cellular cytotoxicity Antibody-dependent cellular phagocytosis; |
| AML | Acute myeloid leukemia |
| APC-H7 | Allophycocyanine-Hilite®7 |
| ASM | Aggressive systemic mastocytosis |
| BM BMMC | Bone marrow Bone marrow mast cell |
| CAR | Chimeric antigen receptor |
| CM | Cutaneous mastocytosis |
| CR | Complete remission |
| EMA | European Medicines Agency |
| FDA | US Food and Drug Administration |
| FITC | Fluorescein isothiocyanate |
| ISM | Indolent systemic mastocytosis |
| ISMMC | Indolent systemic mastocytosis with MC-restricted KIT mutation |
| ISMML | Indolent systemic mastocytosis with multilineal KIT-mutated |
| KIT | Stem cell factor receptor |
| MC | Mast cell |
| MCL | Mast cell leukemia |
| MFI ORR | Mean fluorescence intensity Overall response rate |
| PacB | Pacific blue |
| PacO | Pacific orange |
| PE | Phycoerythrin |
| PeCy7 | Phycoerythrin-cyanine 7 |
| PerCPCy5.5 | Peridinin-chlorophyll protein-cyanine 5.5 |
| PNA | Peptide nucleic acid |
| REMA | Spanish Network on Mastocytosis |
| SI | Stain index |
| SM | Systemic mastocytosis |
| SM-AHN | Systemic mastocytosis with an associated clonal non-MC lineage disease |
| SSM | Smoldering systemic mastocytosis |
| TKI | Tyrosine-kinase inhibitor |
| WDSM | Well-differentiated systemic mastocytosis |
| WHO | World Health Organization |
References
- Valent, P.; Horny, H.P.; Escribano, L.; Longley, B.J.; Li, C.Y.; Schwartz, L.B.; Marone, G.; Nunez, R.; Akin, C.; Sotlar, K.; et al. Diagnostic criteria and classification of mastocytosis: A consensus proposal. Leuk. Res. 2001, 25, 603–625. [Google Scholar] [CrossRef]
- Horny, H.P.; Akin, C.; Metcalfe, D.D.; Escribano, L.; Bennett, J.M.; Valent, P.; Bain, B.J. Mastocytosis (mast cell disease). In World Health Organization (WHO) Classification of Tumours. Pathology and Genetics. Tumours of Haematopoietic and Lymphoid Tissues; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Vardiman, J.W., Eds.; IARC Press: Lyon, France, 2008; pp. 54–63. [Google Scholar]
- Valent, P.; Akin, C.; Metcalfe, D.D. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood 2017, 129, 1420–1427. [Google Scholar] [CrossRef]
- Garcia-Montero, A.C.; Jara-Acevedo, M.; Teodosio, C.; Sanchez, M.L.; Nunez, R.; Prados, A.; Aldanondo, I.; Sanchez, L.; Dominguez, M.; Botana, L.M.; et al. KIT mutation in mast cells and other bone marrow hematopoietic cell lineages in systemic mast cell disorders: A prospective study of the Spanish Network on Mastocytosis (REMA) in a series of 113 patients. Blood 2006, 108, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Twose, I.; Jara-Acevedo, M.; Morgado, J.M.; Garcia-Montero, A.; Sanchez-Munoz, L.; Teodosio, C.; Matito, A.; Mayado, A.; Caldas, C.; Mollejo, M.; et al. Clinical, immunophenotypic, and molecular characteristics of well-differentiated systemic mastocytosis. J. Allergy Clin. Immunol. 2016, 137, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Georgin-Lavialle, S.; Lhermitte, L.; Dubreuil, P.; Chandesris, M.O.; Hermine, O.; Damaj, G. Mast cell leukemia. Blood 2013, 121, 1285–1295. [Google Scholar] [CrossRef]
- Vaes, M.; Benghiat, F.S.; Hermine, O. Targeted Treatment Options in Mastocytosis. Front. Med. 2017, 4, 110. [Google Scholar] [CrossRef]
- Escribano, L.; Akin, C.; Castells, M.; Orfao, A.; Metcalfe, D.D. Mastocytosis: Current concepts in diagnosis and treatment. Ann. Hematol. 2002, 81, 677–690. [Google Scholar]
- Valent, P. Diagnosis and management of mastocytosis: An emerging challenge in applied hematology. Hematol. Am. Soc. Hematol. Educ. Program 2015, 2015, 98–105. [Google Scholar] [CrossRef]
- Gotlib, J.; Kluin-Nelemans, H.C.; George, T.I.; Akin, C.; Sotlar, K.; Hermine, O.; Awan, F.T.; Hexner, E.; Mauro, M.J.; Sternberg, D.W.; et al. Efficacy and Safety of Midostaurin in Advanced Systemic Mastocytosis. N. Engl. J. Med. 2016, 374, 2530–2541. [Google Scholar] [CrossRef]
- Alvarez-Twose, I.; Matito, A.; Morgado, J.M.; Sanchez-Munoz, L.; Jara-Acevedo, M.; Garcia-Montero, A.; Mayado, A.; Caldas, C.; Teodosio, C.; Munoz-Gonzalez, J.I.; et al. Imatinib in systemic mastocytosis: A phase IV clinical trial in patients lacking exon 17 KIT mutations and review of the literature. Oncotarget 2017, 8, 68950–68963. [Google Scholar] [CrossRef] [PubMed]
- Lortholary, O.; Chandesris, M.O.; Bulai Livideanu, C.; Paul, C.; Guillet, G.; Jassem, E.; Niedoszytko, M.; Barete, S.; Verstovsek, S.; Grattan, C.; et al. Masitinib for treatment of severely symptomatic indolent systemic mastocytosis: A randomised, placebo-controlled, phase 3 study. Lancet 2017, 389, 612–620. [Google Scholar] [CrossRef]
- Stone, R.M.; Manley, P.W.; Larson, R.A.; Capdeville, R. Midostaurin: Its odyssey from discovery to approval for treating acute myeloid leukemia and advanced systemic mastocytosis. Blood Adv. 2018, 2, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Akin, C.; Fumo, G.; Yavuz, A.S.; Lipsky, P.E.; Neckers, L.; Metcalfe, D.D. A novel form of mastocytosis associated with a transmembrane c-kit mutation and response to imatinib. Blood 2004, 103, 3222–3225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Twose, I.; Gonzalez, P.; Morgado, J.M.; Jara-Acevedo, M.; Sanchez-Munoz, L.; Matito, A.; Mollejo, M.; Orfao, A.; Escribano, L. Complete response after imatinib mesylate therapy in a patient with well-differentiated systemic mastocytosis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, e126–e129. [Google Scholar] [CrossRef]
- Chan, E.C.; Bai, Y.; Kirshenbaum, A.S.; Fischer, E.R.; Simakova, O.; Bandara, G.; Scott, L.M.; Wisch, L.B.; Cantave, D.; Carter, M.C.; et al. Mastocytosis associated with a rare germline KIT K509I mutation displays a well-differentiated mast cell phenotype. J. Allergy Clin. Immunol. 2014, 134, 178–187. [Google Scholar] [CrossRef] [PubMed]
- De Melo Campos, P.; Machado-Neto, J.A.; Scopim-Ribeiro, R.; Visconte, V.; Tabarroki, A.; Duarte, A.S.; Barra, F.F.; Vassalo, J.; Rogers, H.J.; Lorand-Metze, I.; et al. Familial systemic mastocytosis with germline KIT K509I mutation is sensitive to treatment with imatinib, dasatinib and PKC412. Leuk. Res. 2014, 38, 1245–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.; Wang, S.A.; Konoplev, S.; Bueso-Ramos, C.E.; Thakral, B.; Miranda, R.N.; Jabbour, E.; Medeiros, L.J.; Kanagal-Shamanna, R. Well-differentiated systemic mastocytosis showed excellent clinical response to imatinib in the absence of known molecular genetic abnormalities: A case report. Medicine 2016, 95, e4934. [Google Scholar] [CrossRef]
- Scherber, R.M.; Borate, U. How we diagnose and treat systemic mastocytosis in adults. Br. J. Haematol. 2018, 180, 11–23. [Google Scholar] [CrossRef]
- Helmy, K.Y.; Patel, S.A.; Nahas, G.R.; Rameshwar, P. Cancer immunotherapy: Accomplishments to date and future promise. Ther. Deliv. 2013, 4, 1307–1320. [Google Scholar] [CrossRef]
- Ustun, C.; Arock, M.; Kluin-Nelemans, H.C.; Reiter, A.; Sperr, W.R.; George, T.; Horny, H.P.; Hartmann, K.; Sotlar, K.; Damaj, G.; et al. Advanced systemic mastocytosis: From molecular and genetic progress to clinical practice. Haematologica 2016, 101, 1133–1143. [Google Scholar] [CrossRef]
- Valent, P.; Cerny-Reiterer, S.; Herrmann, H.; Mirkina, I.; George, T.I.; Sotlar, K.; Sperr, W.R.; Horny, H.P. Phenotypic heterogeneity, novel diagnostic markers, and target expression profiles in normal and neoplastic human mast cells. Best Pract. Res. Clin. Haematol. 2010, 23, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Siebenhaar, F.; Akin, C.; Bindslev-Jensen, C.; Maurer, M.; Broesby-Olsen, S. Treatment strategies in mastocytosis. Immunol. Allergy Clin. N. Am. 2014, 34, 433–447. [Google Scholar] [CrossRef] [PubMed]
- Teodosio, C.; Garcia-Montero, A.C.; Jara-Acevedo, M.; Sanchez-Munoz, L.; Alvarez-Twose, I.; Nunez, R.; Schwartz, L.B.; Walls, A.F.; Escribano, L.; Orfao, A. Mast cells from different molecular and prognostic subtypes of systemic mastocytosis display distinct immunophenotypes. J. Allergy Clin. Immunol. 2010, 125, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Morgado, J.M.; Perbellini, O.; Johnson, R.C.; Teodosio, C.; Matito, A.; Alvarez-Twose, I.; Bonadonna, P.; Zamo, A.; Jara-Acevedo, M.; Mayado, A.; et al. CD30 expression by bone marrow mast cells from different diagnostic variants of systemic mastocytosis. Histopathology 2013, 63, 780–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, D.K.; Fauman, K.; Ross, C.; Akin, C.; Mody, R. Successful Treatment of Systemic Mastocytosis Associated with AML-M2, t(8:21) in a Child Using MRC-based AML Chemotherapy along with Gemtuzumab. J. Allergy Clin. Immunol. 2007, 119, S207. [Google Scholar] [CrossRef]
- Alvarez-Twose, I.; Martinez-Barranco, P.; Gotlib, J.; Garcia-Montero, A.; Morgado, J.M.; Jara-Acevedo, M.; Merker, J.D.; Penalver, F.J.; Matito, A.; Hou, Y.; et al. Complete response to gemtuzumab ozogamicin in a patient with refractory mast cell leukemia. Leukemia 2016, 30, 1753–1756. [Google Scholar] [CrossRef] [PubMed]
- Quintas-Cardama, A.; Amin, H.M.; Kantarjian, H.; Verstovsek, S. Treatment of aggressive systemic mastocytosis with daclizumab. Leuk. Lymphoma 2010, 51, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Borate, U.; Mehta, A.; Reddy, V.; Tsai, M.; Josephson, N.; Schnadig, I. Treatment of CD30-positive systemic mastocytosis with brentuximab vedotin. Leuk. Res. 2016, 44, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Kantarjian, H.M.; DeAngelo, D.J.; Stelljes, M.; Martinelli, G.; Liedtke, M.; Stock, W.; Gokbuget, N.; O’Brien, S.; Wang, K.; Wang, T.; et al. Inotuzumab Ozogamicin versus Standard Therapy for Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2016, 375, 740–753. [Google Scholar] [CrossRef] [Green Version]
- Kantarjian, H.M.; DeAngelo, D.J.; Advani, A.S.; Stelljes, M.; Kebriaei, P.; Cassaday, R.D.; Merchant, A.A.; Fujishima, N.; Uchida, T.; Calbacho, M.; et al. Hepatic adverse event profile of inotuzumab ozogamicin in adult patients with relapsed or refractory acute lymphoblastic leukaemia: Results from the open-label, randomised, phase 3 INO-VATE study. Lancet Haematol. 2017, 4, e387–e398. [Google Scholar] [CrossRef]
- Kreitman, R.J.; Tallman, M.S.; Robak, T.; Coutre, S.; Wilson, W.H.; Stetler-Stevenson, M.; Fitzgerald, D.J.; Lechleider, R.; Pastan, I. Phase I trial of anti-CD22 recombinant immunotoxin moxetumomab pasudotox (CAT-8015 or HA22) in patients with hairy cell leukemia. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1822–1828. [Google Scholar] [CrossRef] [PubMed]
- Kreitman, R.J.; Dearden, C.; Zinzani, P.L.; Delgado, J.; Karlin, L.; Robak, T.; Gladstone, D.E.; le Coutre, P.; Dietrich, S.; Gotic, M.; et al. Moxetumomab pasudotox in relapsed/refractory hairy cell leukemia. Leukemia 2018, 32, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Vincenti, F.; Kirkman, R.; Light, S.; Bumgardner, G.; Pescovitz, M.; Halloran, P.; Neylan, J.; Wilkinson, A.; Ekberg, H.; Gaston, R.; et al. Interleukin-2-receptor blockade with daclizumab to prevent acute rejection in renal transplantation. Daclizumab Triple Therapy Study Group. N. Engl. J. Med. 1998, 338, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Kahan, B.D.; Rajagopalan, P.R.; Hall, M. Reduction of the occurrence of acute cellular rejection among renal allograft recipients treated with basiliximab, a chimeric anti-interleukin-2-receptor monoclonal antibody. United States Simulect Renal Study Group. Transplantation 1999, 67, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Nashan, B.; Moore, R.; Amlot, P.; Schmidt, A.G.; Abeywickrama, K.; Soulillou, J.P. Randomised trial of basiliximab versus placebo for control of acute cellular rejection in renal allograft recipients. CHIB 201 International Study Group. Lancet 1997, 350, 1193–1198. [Google Scholar] [CrossRef]
- Gold, R.; Giovannoni, G.; Selmaj, K.; Havrdova, E.; Montalban, X.; Radue, E.W.; Stefoski, D.; Robinson, R.; Riester, K.; Rana, J.; et al. Daclizumab high-yield process in relapsing-remitting multiple sclerosis (SELECT): A randomised, double-blind, placebo-controlled trial. Lancet 2013, 381, 2167–2175. [Google Scholar] [CrossRef]
- Giovannoni, G.; Gold, R.; Selmaj, K.; Havrdova, E.; Montalban, X.; Radue, E.W.; Stefoski, D.; McNeill, M.; Amaravadi, L.; Sweetser, M.; et al. Daclizumab high-yield process in relapsing-remitting multiple sclerosis (SELECTION): A multicentre, randomised, double-blind extension trial. Lancet Neurol. 2014, 13, 472–481. [Google Scholar] [CrossRef]
- Giovannoni, G.; Radue, E.W.; Havrdova, E.; Riester, K.; Greenberg, S.; Mehta, L.; Elkins, J. Effect of daclizumab high-yield process in patients with highly active relapsing-remitting multiple sclerosis. J. Neurol. 2014, 261, 316–323. [Google Scholar] [CrossRef]
- Gold, R.; Radue, E.W.; Giovannoni, G.; Selmaj, K.; Havrdova, E.; Stefoski, D.; Sprenger, T.; Montalban, X.; Cohan, S.; Umans, K.; et al. Safety and efficacy of daclizumab in relapsing-remitting multiple sclerosis: 3-year results from the SELECTED open-label extension study. BMC Neurol. 2016, 16, 117. [Google Scholar] [CrossRef]
- Pro, B.; Advani, R.; Brice, P.; Bartlett, N.L.; Rosenblatt, J.D.; Illidge, T.; Matous, J.; Ramchandren, R.; Fanale, M.; Connors, J.M.; et al. Brentuximab vedotin (SGN-35) in patients with relapsed or refractory systemic anaplastic large-cell lymphoma: Results of a phase II study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2190–2196. [Google Scholar] [CrossRef]
- Younes, A.; Gopal, A.K.; Smith, S.E.; Ansell, S.M.; Rosenblatt, J.D.; Savage, K.J.; Ramchandren, R.; Bartlett, N.L.; Cheson, B.D.; de Vos, S.; et al. Results of a pivotal phase II study of brentuximab vedotin for patients with relapsed or refractory Hodgkin’s lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Gopal, A.K.; Chen, R.; Smith, S.E.; Ansell, S.M.; Rosenblatt, J.D.; Savage, K.J.; Connors, J.M.; Engert, A.; Larsen, E.K.; Chi, X.; et al. Durable remissions in a pivotal phase 2 study of brentuximab vedotin in relapsed or refractory Hodgkin lymphoma. Blood 2015, 125, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Gopal, A.K.; Smith, S.E.; Ansell, S.M.; Rosenblatt, J.D.; Savage, K.J.; Connors, J.M.; Engert, A.; Larsen, E.K.; Huebner, D.; et al. Five-year survival and durability results of brentuximab vedotin in patients with relapsed or refractory Hodgkin lymphoma. Blood 2016, 128, 1562–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pro, B.; Advani, R.; Brice, P.; Bartlett, N.L.; Rosenblatt, J.D.; Illidge, T.; Matous, J.; Ramchandren, R.; Fanale, M.; Connors, J.M.; et al. Five-year results of brentuximab vedotin in patients with relapsed or refractory systemic anaplastic large cell lymphoma. Blood 2017, 130, 2709–2717. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Illidge, T.; Fanale, M.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): A global, double-blind, randomised, phase 3 trial. Lancet 2018. [Google Scholar] [CrossRef]
- Taksin, A.L.; Legrand, O.; Raffoux, E.; de Revel, T.; Thomas, X.; Contentin, N.; Bouabdallah, R.; Pautas, C.; Turlure, P.; Reman, O.; et al. High efficacy and safety profile of fractionated doses of Mylotarg as induction therapy in patients with relapsed acute myeloblastic leukemia: A prospective study of the alfa group. Leukemia 2007, 21, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Renneville, A.; Abdelali, R.B.; Chevret, S.; Nibourel, O.; Cheok, M.; Pautas, C.; Dulery, R.; Boyer, T.; Cayuela, J.M.; Hayette, S.; et al. Clinical impact of gene mutations and lesions detected by SNP-array karyotyping in acute myeloid leukemia patients in the context of gemtuzumab ozogamicin treatment: Results of the ALFA-0701 trial. Oncotarget 2014, 5, 916–932. [Google Scholar] [CrossRef] [PubMed]
- Amadori, S.; Suciu, S.; Selleslag, D.; Aversa, F.; Gaidano, G.; Musso, M.; Annino, L.; Venditti, A.; Voso, M.T.; Mazzone, C.; et al. Gemtuzumab Ozogamicin Versus Best Supportive Care in Older Patients With Newly Diagnosed Acute Myeloid Leukemia Unsuitable for Intensive Chemotherapy: Results of the Randomized Phase III EORTC-GIMEMA AML-19 Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 972–979. [Google Scholar] [CrossRef] [Green Version]
- Moro, J.A.; Almenar, L.; Jarque, I.; Martinez-Dolz, L.; Hernandez, M.D.; Crespo, M.; Salvador, A. Heart transplantation in a patient with systemic mastocytosis. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2008, 27, 689–691. [Google Scholar] [CrossRef]
- Busse, W.; Corren, J.; Lanier, B.Q.; McAlary, M.; Fowler-Taylor, A.; Cioppa, G.D.; van As, A.; Gupta, N. Omalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthma. J. Allergy Clin. Immunol. 2001, 108, 184–190. [Google Scholar] [CrossRef]
- Corren, J.; Casale, T.; Deniz, Y.; Ashby, M. Omalizumab, a recombinant humanized anti-IgE antibody, reduces asthma-related emergency room visits and hospitalizations in patients with allergic asthma. J. Allergy Clin. Immunol. 2003, 111, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Finn, A.; Gross, G.; van Bavel, J.; Lee, T.; Windom, H.; Everhard, F.; Fowler-Taylor, A.; Liu, J.; Gupta, N. Omalizumab improves asthma-related quality of life in patients with severe allergic asthma. J. Allergy Clin. Immunol. 2003, 111, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Robyn, J.A.; Bressler, P.B.; Walker, J.C.; Shapiro, G.G.; Metcalfe, D.D. Omalizumab for the treatment of unprovoked anaphylaxis in patients with systemic mastocytosis. J. Allergy Clin. Immunol. 2007, 119, 1550–1551. [Google Scholar] [CrossRef] [PubMed]
- Douglass, J.A.; Carroll, K.; Voskamp, A.; Bourke, P.; Wei, A.; O’Hehir, R.E. Omalizumab is effective in treating systemic mastocytosis in a nonatopic patient. Allergy 2010, 65, 926–927. [Google Scholar] [CrossRef] [PubMed]
- Kontou-Fili, K.; Filis, C.I.; Voulgari, C.; Panayiotidis, P.G. Omalizumab monotherapy for bee sting and unprovoked “anaphylaxis” in a patient with systemic mastocytosis and undetectable specific IgE. Ann. Allergyasthma Immunol. 2010, 104, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Pitt, T.J.; Cisneros, N.; Kalicinsky, C.; Becker, A.B. Successful treatment of idiopathic anaphylaxis in an adolescent. J. Allergy Clin. Immunol. 2010, 126, 415–416, author reply 416. [Google Scholar] [CrossRef] [PubMed]
- Paraskevopoulos, G.; Sifnaios, E.; Christodoulopoulos, K.; Mantopoulou, F.; Papakonstantis, M.; Sabaziotis, D. Successful treatment of mastocytic anaphylactic episodes with reduction of skin mast cells after anti-IgE therapy. Eur. Ann. Allergy Clin. Immunol. 2013, 45, 52–55. [Google Scholar]
- Kibsgaard, L.; Skjold, T.; Deleuran, M.; Vestergaard, C. Omalizumab induced remission of idiopathic anaphylaxis in a patient suffering from indolent systemic mastocytosis. Acta Derm. Venereol. 2014, 94, 363–364. [Google Scholar] [CrossRef]
- Lieberoth, S.; Thomsen, S.F. Cutaneous and gastrointestinal symptoms in two patients with systemic mastocytosis successfully treated with omalizumab. Case Rep. Med. 2015, 2015, 903541. [Google Scholar] [CrossRef]
- Broesby-Olsen, S.; Vestergaard, H.; Mortz, C.G.; Jensen, B.; Havelund, T.; Hermann, A.P.; Siebenhaar, F.; Moller, M.B.; Kristensen, T.K.; Bindslev-Jensen, C.; et al. Omalizumab prevents anaphylaxis and improves symptoms in systemic mastocytosis: Efficacy and safety observations. Allergy 2018, 73, 230–238. [Google Scholar] [CrossRef]
- Chen, M.; Kim, A.; Zuraw, B.; Doherty, T.A.; Christiansen, S. Mast cell disorders: Protean manifestations and treatment responses. Ann. Allergyasthma Immunol. 2018, 121, 120–130. [Google Scholar] [CrossRef]
- Valent, P.; Ghannadan, M.; Akin, C.; Krauth, M.T.; Selzer, E.; Mayerhofer, M.; Sperr, W.R.; Arock, M.; Samorapoompichit, P.; Horny, H.P.; et al. On the way to targeted therapy of mast cell neoplasms: Identification of molecular targets in neoplastic mast cells and evaluation of arising treatment concepts. Eur. J. Clin. Investig. 2004, 34 (Suppl. 2), 41–52. [Google Scholar] [CrossRef]
- Pardanani, A. Systemic mastocytosis in adults: 2015 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2015, 90, 250–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Yin, B.; Wang, H.Y.; Wang, R.F. Current advances in T-cell-based cancer immunotherapy. Immunotherapy 2014, 6, 1265–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicodemus, C.F. Antibody-based immunotherapy of solid cancers: Progress and possibilities. Immunotherapy 2015, 7, 923–939. [Google Scholar] [CrossRef] [PubMed]
- Firor, A.E.; Jares, A.; Ma, Y. From humble beginnings to success in the clinic: Chimeric antigen receptor-modified T-cells and implications for immunotherapy. Exp. Biol. Med. 2015, 240, 1087–1098. [Google Scholar] [CrossRef] [Green Version]
- Golay, J.; Introna, M. Mechanism of action of therapeutic monoclonal antibodies: Promises and pitfalls of in vitro and in vivo assays. Arch. Biochem. Biophys. 2012, 526, 146–153. [Google Scholar] [CrossRef]
- Anikeeva, N.; Steblyanko, M.; Fayngerts, S.; Kopylova, N.; Marshall, D.J.; Powers, G.D.; Sato, T.; Campbell, K.S.; Sykulev, Y. Integrin receptors on tumor cells facilitate NK cell-mediated antibody-dependent cytotoxicity. Eur. J. Immunol. 2014, 44, 2331–2339. [Google Scholar] [CrossRef] [Green Version]
- Herter, S.; Birk, M.C.; Klein, C.; Gerdes, C.; Umana, P.; Bacac, M. Glycoengineering of therapeutic antibodies enhances monocyte/macrophage-mediated phagocytosis and cytotoxicity. J. Immunol. 2014, 192, 2252–2260. [Google Scholar] [CrossRef]
- Weiskopf, K.; Weissman, I.L. Macrophages are critical effectors of antibody therapies for cancer. mAbs 2015, 7, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.; Goetsch, L.; Dumontet, C.; Corvaia, N. Strategies and challenges for the next generation of antibody-drug conjugates. Nat. Rev. Drug Discov. 2017, 16, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Krauth, M.T.; Bohm, A.; Agis, H.; Sonneck, K.; Samorapoompichit, P.; Florian, S.; Sotlar, K.; Valent, P. Effects of the CD33-targeted drug gemtuzumab ozogamicin (Mylotarg) on growth and mediator secretion in human mast cells and blood basophils. Exp. Hematol. 2007, 35, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Van der Velden, V.H.; Boeckx, N.; Jedema, I.; te Marvelde, J.G.; Hoogeveen, P.G.; Boogaerts, M.; van Dongen, J.J. High CD33-antigen loads in peripheral blood limit the efficacy of gemtuzumab ozogamicin (Mylotarg) treatment in acute myeloid leukemia patients. Leukemia 2004, 18, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Velden, V.; van Dongen, J.J.M. Effectiveness of Gemtuzumab Ozogamicin (Mylotarg) Treatment: Cellular and Systemic Determinants. EJHP Sci. 2006, 12, 118–122. [Google Scholar]
- Siebenhaar, F.; Kuhn, W.; Zuberbier, T.; Maurer, M. Successful treatment of cutaneous mastocytosis and Meniere disease with anti-IgE therapy. J. Allergy Clin. Immunol. 2007, 120, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Matito, A.; Blazquez-Goni, C.; Morgado, J.M.; Alvarez-Twose, I.; Mollejo, M.; Sanchez-Munoz, L.; Escribano, L. Short-term omalizumab treatment in an adolescent with cutaneous mastocytosis. Ann. Allergyasthma Immunol. 2013, 111, 425–426. [Google Scholar] [CrossRef]
- Sokol, K.C.; Ghazi, A.; Kelly, B.C.; Grant, J.A. Omalizumab as a desensitizing agent and treatment in mastocytosis: A review of the literature and case report. J. Allergy Clin. Immunol. Pract. 2014, 2, 266–270. [Google Scholar] [CrossRef]
- Blatt, K.; Cerny-Reiterer, S.; Schwaab, J.; Sotlar, K.; Eisenwort, G.; Stefanzl, G.; Hoermann, G.; Mayerhofer, M.; Schneeweiss, M.; Knapp, S.; et al. Identification of the Ki-1 antigen (CD30) as a novel therapeutic target in systemic mastocytosis. Blood 2015, 126, 2832–2841. [Google Scholar] [CrossRef] [Green Version]
- Escribano, L.; Orfao, A.; Diaz Agustin, B.; Cervero, C.; Herrero, S.; Villarrubia, J.; Bravo, P.; Torrelo, A.; Montero, T.; Valdemoro, M.; et al. Human bone marrow mast cells from indolent systemic mast cell disease constitutively express increased amounts of the CD63 protein on their surface. Cytometry 1998, 34, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Maecker, H.; Trotter, J. Selecting reagents for multicolor flow cytometry with BD™ LSR II and BD FACSCanto™ systems. Nat. Methods 2008, 5, A6. [Google Scholar] [CrossRef]
- Kantor, A.B.; Moore, W.A.; Meehan, S.; Parks, D.R. A Quantitative Method for Comparing the Brightness of Antibody-dye Reagents and Estimating Antibodies Bound per Cell. Curr. Protoc. Cytom. 2016, 77, 1.30.1–1.30.23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Targeted Protein (Gene Symbol) | Monoclonal Antibody Name | Mechanism of Action | Year of Approval | Approved Indication(s) | References | ORR (CR) Rates in SM |
|---|---|---|---|---|---|---|
| CD22 (Siglec-2) | Inotuzumab ozogamicin | Immunotoxin | 2017 ¥§ | B-cell precursor (BCP) acute lymphoblastic leukemia | [30,31] | - |
| Moxetumomab pasudotox | 2018 § | Hairy cell leukemia | [32,33] | - | ||
| CD25 (IL2RA) | Daclizumab | ADCC | 1997 §# 1999 ¥# | Prophylaxis of acute organ rejection in renal transplantation | [34] | 2/5 (40%) (0/5 (0%)) [28] |
| Basiliximab | 1998 ¥§ | Prophylaxis of acute organ rejection in renal transplantation | [35,36] | - | ||
| Daclizumab | 2016 ¥§# | Relapsing forms of multiple sclerosis | [37,38,39,40] | - | ||
| CD30 (TNFRFS8) | Brentuximab vedotin | Immunotoxin/ADCP | 2011 § 2012 ¥ | Hodgkin lymphoma/cutaneous lymphoma/peripheral T-cell lymphoma | [41,42,43,44,45,46] | 2/4 50% (0/4 (0%)) [29] |
| CD33 (Siglec-3) | Gemtuzumab ozogamicin | Immunotoxin | 2000 # 2017 ¥§ | Acute myeloid leukemia | [47,48,49] | (2/2 (100%)) [27,50] |
| CD123 (IL3RA) | Talacotuzumab | ADCC | 2018 * | Acute myeloid leukemia | - | - |
| FcεRI (High-affinity immunoglobulin ε heavy chain receptor I) | Omalizumab | ADCC | 2003 § 2005 ¥ | Moderate to severe persistent asthma | [51,52,53] | 10/21 (48%) (11/21 (52%)) [54,55,56,57,58,59,60,61,62] |
| Normal BM (N = 40) | SM (N = 166) | WDSM (N = 18) | ISMMC (N = 70) | ISMML (N = 41) | ISM-AHN (N = 12) | ASM (N = 10) | ASM-AHN (N = 9) | MCL (N = 6) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| CD22 | N | 9 | 57 | 8 | 10 | 19 | 6 | 4 | 6 | 4 |
| % positive patients | 78 | 77 | 75 | 90 | 79 | 83 | 75 | 83 | 25 | |
| p-value | - | - | - | ¥ p = 0.02 | ¥ p = 0.03 | - | - | - | §$ p ≤ 0.03 | |
| % positive cells | 89 (0–100) | 93 (0–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 83 (0–100) | 75 (0–100) | 100 (100–100) | 50 (0–100) | |
| p-value | - | - | ¥ p = 0.03 | ¥ p = 0.02 | ¶¥ p = 0.03 | - | $ p = 0.03 | - | †§$ p ≤ 0.03 | |
| MFI | 1333 (8–3431) | 2629 (1–11,398) | 2187 (192–6614) | 2363 (424–5081) | 2959 (348–11,398) | 3086 (293–8612) | 3521 (246–6760) | 2841 (455–4435) | 721 (1–2398) | |
| p-value | - | - | - | - | ¥ p = 0.006 | - | - | ¥ p = 0.04 | $‡ p ≤ 0.04 | |
| CD25 | N | 40 | 166 | 18 | 70 | 41 | 12 | 10 | 9 | 6 |
| % positive patients | 0 | 89 | 33 | 99 | 100 | 92 | 100 | 100 | 33 | |
| p-value | - | * p = 0.001 | §$‖¶‡ p ≤ 0.002 | †¥ p = 0.001 | †¥ p = 0.001 | †¥ p ≤ 0.009 | †¥ p ≤ 0.003 | †¥ p ≤ 0.004 | §$‖¶‡ p ≤ 0.009 | |
| % positive cells | 0 (0–0) | 92 (0–100) | 44 (0–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 33 (0–100) | |
| p-value | - | * p = 0.001 | §$‖¶‡ p ≤ 0.005 | †¥ p = 0.001 | †¥ p = 0.001 | †¥ p ≤ 0.002 | †¥ p = 0.003 | †¥ p ≤ 0.005 | §$‖¶‡ p ≤ 0.004 | |
| MFI | 0 (0–0) | 5331 (4–21,943) | 471 (4–4159) | 6448 (806–17,552) | 5427 (2016–14,639) | 6544 (2329–16,474) | 6862 (1406–21,943) | 5371 (2376–11,108) | 1190 (21–4922) | |
| p-value | - | * p = 0.001 | §$‖¶‡ p = 0.001 | †¥ p = 0.001 | †¥ p = 0.001 | †¥ p = 0.001 | †¥ p ≤ 0.005 | †¥ p ≤ 0.008 | §$‖¶‡ p ≤ 0.008 | |
| CD30 | N | 37 | 164 | 18 | 69 | 41 | 12 | 10 | 9 | 5 |
| % positive patients | 5 | 63 | 61 | 61 | 76 | 58 | 70 | 67 | 0 | |
| p-value | - | * p = 0.001 | ¥ p = 0.02 | ¥ p = 0.008 | ¥ p = 0.001 | ¥ p = 0.03 | ¥ p = 0.01 | ¥ p = 0.02 | †§$‖¶‡ p ≤ 0.03 | |
| % positive cells | 0 (0–0) | 88 (0–100) | 94 (0–100) | 87 (0–100) | 90 (0–100) | 83 (0–100) | 90 (0–100) | 89 (0–100) | 0 (0–0) | |
| p-value | - | * p = 0.001 | ¥ p = 0.001 | ¥ p = 0.001 | ¥ p = 0.001 | ¥ p = 0.001 | ¥ p = 0.001 | ¥ p = 0.001 | †§$‖¶‡ p = 0.001 | |
| MFI | 129 (1–427) | 887 (0–6261) | 632 (202–1677) | 860 (0–3040) | 993 (199–3038) | 796 (103–2720) | 1095 (74–2847) | 1345 (202–6261) | 297 (153–495) | |
| p-value | - | * p = 0.001 | §$¥ p ≤ 0.02 | †¥ p ≤ 0.02 | †¥ p ≤ 0.01 | - | - | ¥ p = 0.02 | †§$‡ p ≤ 0.02 | |
| CD33 | N | 31 | 114 | 11 | 60 | 22 | 7 | 7 | 4 | 3 |
| % positive patients | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | |
| p-value | - | - | - | - | - | - | - | - | - | |
| % positive cells | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | |
| p-value | - | - | - | - | - | - | - | - | - | |
| MFI | 8163 (2225–16,377) | 19,667 (2308–53,009) | 16,642 (5774–50,767) | 22,673 (4926–53,009) | 20,576 (2922–44,241) | 15,566 (5441–24,537) | 10,063 (2698–18,730) | 8447 (4022–14,916) | 10,917 (2308–23,681) | |
| p-value | - | * p = 0.001 | § p = 0.03 | †¶‡ p ≤ 0.03 | ¶ p = 0.02 | - | §$ p ≤ 0.02 | § p = 0.002 | - | |
| CD123 | N | 38 | 164 | 18 | 70 | 41 | 12 | 10 | 8 | 5 |
| % positive patients | 3 | 38 | 11 | 37 | 32 | 67 | 40 | 100 | 40 | |
| p-value | - | * p = 0.001 | §‖‡ p ≤ 0.03 | †‡ p ≤ 0.03 | ‖‡ p ≤ 0.03 | †$ p ≤ 0.03 | ‡ p = 0.007 | †§$¶¥ p ≤ 0.01 | ‡ p = 0.01 | |
| % positive cells | 0 (0–0) | 64 (0–100) | 17 (0–100) | 66 (0–100) | 73 (0–100) | 70 (0–100) | 70 (0–100) | 100 (100–100) | 40 (0–100) | |
| p-value | - | * p = 0.001 | §$‖¶‡ p = 0.001 | †‡ p ≤ 0.05 | † p = 0.001 | † p = 0.001 | † p = 0.001 | †§¥ p ≤ 0.05 | ‡ p = 0.01 | |
| MFI | 84 (8–221) | 1340 (3–33 861) | 214 (3–2023) | 1024 (17–5425) | 962 (15–4045) | 3685 (24–33,861) | 939 (94–3220) | 5825 (755–18,421) | 903 (14–3085) | |
| p-value | - | * p = 0.001 | §$‖¶‡ p = 0.001 | †‡ p = 0.001 | †‡ p = 0.001 | †‡ p ≤ 0.01 | †‡ p ≤ 0.003 | †§$‖¶¥ p ≤ 0.03 | ‡ p = 0.03 | |
| FcεRI | N | 40 | 161 | 18 | 69 | 37 | 12 | 10 | 9 | 6 |
| % positive patients | 100 | 92 | 94 | 99 | 89 | 100 | 60 | 89 | 67 | |
| p-value | - | - | ¶ p = 0.02 | $¶¥ p ≤ 0.03 | §¶ p = 0.03 | ¶¥ p ≤ 0.03 | †§$‖ p ≤ 0.03 | - | §‖ p ≤ 0.03 | |
| % positive cells | 100 (100–100) | 95 (0–100) | 94 (0–100) | 100 (100–100) | 95 (0–100) | 100 (100–100) | 70 (0–100) | 100 (100–100) | 67 (0–100) | |
| p-value | - | - | § p = 0.05 | †¶¥ p ≤ 0.05 | ¶¥ p = 0.001 | ¶¥ p = 0.04 | §$‖ p ≤ 0.04 | - | §$‖ p ≤ 0.03 | |
| MFI | 29,073 (2181–81,199) | 49,387 (14–239,335) | 40,350 (110–183,969) | 78,922 (1271–239,335) | 24,084 (73–162,320) | 62,685 (1938–177,643) | 4858 (176–26,255) | 11,084 (680–36,688) | 9909 (14–52,514) | |
| p-value | - | - | §¶¥ p ≤ 0.02 | †$¶‡¥ p ≤ 0.002 | §‖¶ p ≤ 0.04 | $¶‡¥ p ≤ 0.04 | †§$‖ p ≤ 0.005 | §‖ p ≤ 0.04 | †§‖ p ≤ 0.02 |
| Marker | Clone | Fluorochrome | Source | Specificity |
|---|---|---|---|---|
| CD22 | S-HCL-1 | APC | BD Biosciences * | Sialic acid-binding Ig-like lectin 2 (Siglec-2) |
| CD25 | 2A3 | PE | BD Biosciences * | Interleukin-2 receptor, subunit α |
| CD30 | Ber-H8 | PE | BD Biosciences * | Member 8 of the tumor necrosis factor receptor superfamily |
| CD33 | P67.6 | APC | BD Biosciences * | Sialic acid-binding Ig-like lectin 3 (Siglec-3) |
| CD123 | AC145 | APC | Miltenyi Biotec † | Interleukin-3 receptor, subunit α |
| IgE | Polyclonal | FITC | Invitrogen § | High-affinity immunoglobulin ε heavy chain receptor I |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dasilva-Freire, N.; Mayado, A.; Teodosio, C.; Jara-Acevedo, M.; Álvarez-Twose, I.; Matito, A.; Sánchez-Muñoz, L.; Caldas, C.; Henriques, A.; Muñoz-González, J.I.; et al. Bone Marrow Mast Cell Antibody-Targetable Cell Surface Protein Expression Profiles in Systemic Mastocytosis. Int. J. Mol. Sci. 2019, 20, 552. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20030552
Dasilva-Freire N, Mayado A, Teodosio C, Jara-Acevedo M, Álvarez-Twose I, Matito A, Sánchez-Muñoz L, Caldas C, Henriques A, Muñoz-González JI, et al. Bone Marrow Mast Cell Antibody-Targetable Cell Surface Protein Expression Profiles in Systemic Mastocytosis. International Journal of Molecular Sciences. 2019; 20(3):552. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20030552
Chicago/Turabian StyleDasilva-Freire, Noelia, Andrea Mayado, Cristina Teodosio, María Jara-Acevedo, Iván Álvarez-Twose, Almudena Matito, Laura Sánchez-Muñoz, Carolina Caldas, Ana Henriques, Javier I. Muñoz-González, and et al. 2019. "Bone Marrow Mast Cell Antibody-Targetable Cell Surface Protein Expression Profiles in Systemic Mastocytosis" International Journal of Molecular Sciences 20, no. 3: 552. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20030552