Prognostic Significance of Interferon-γ and Its Signaling Pathway in Early Breast Cancer Depends on the Molecular Subtypes

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Expression of IFN-γ and the IFN-γ Signature in Different Molecular Subtypes
2.2. Prognostic Impact of IFN-γ as a Single Gene on MFS
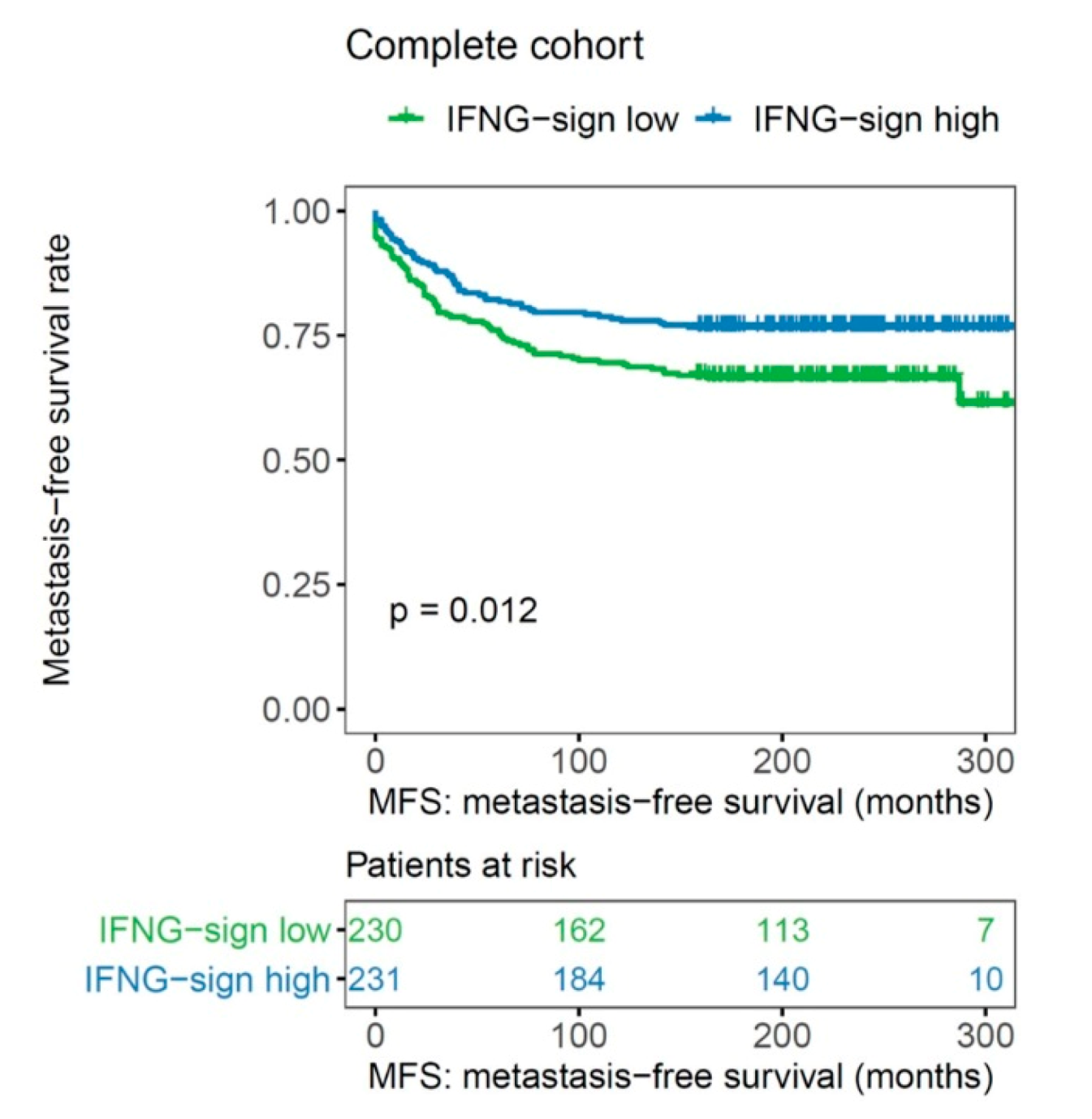
2.3. Impact of an IFN-γ Signature on MFS
3. Discussion
4. Methods
4.1. Patient Characteristics and Tissue Specimens
4.2. Gene Expression Analysis
4.3. IFN-γ Signature
4.4. Molecular Subtypes
- -
- ESR1-positive, HER2 negative, low proliferation (AURKA low) → luminal A-like
- -
- ESR1-positive, HER2 negative, high proliferation (AURKA high) → luminal B-like
- -
- HER2-positive
- -
- ESR1 negative, HER2-negative → basal-like
4.5. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| CMF | cyclophosphamide/methotrexate/5-fluorouracil |
| CXCL13 | chemokine leukocyte chemoattractant-ligand (C-X-C motif) 13 |
| EC | epirubicin/cyclophosphamide |
| ER | estrogen receptor |
| FADD | Fas-associated protein with death domain |
| HER2 | human epidermal growth factor receptor |
| HR | hazard ratio |
| IFN-γ | interferon-γ |
| IFNG | interferon-gamma |
| IFNGR1 | interferon-γ receptor 1 |
| IGKC | immunoglobulin kappa C |
| IRF1 | interferon regulatory factor 1 |
| JAK | Janus kinase |
| MHC | major histocompatibility complex |
| N | nodal status |
| NST | no special type |
| PD-1 | programmed cell death protein 1 |
| PD-L1 | programmed cell death 1 ligand 1 |
| PR | progesterone receptor |
| STAT1 | signal transducer and activator of transcription 1 |
| T | tumor size |
| Th1 | T-helper cells type I |
| TNBC | triple-negative breast cancer |
| TRAIL | tumor necrosis factor-related apoptosis-inducing ligand |
References
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denkert, C.; Loibl, S.; Noske, A.; Roller, M.; Muller, B.M.; Komor, M.; Budczies, J.; Darb-Esfahani, S.; Kronenwett, R.; Hanusch, C.; et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J. Clin. Oncol. 2010, 28, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J. Clin. Oncol. 2015, 33, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Emens, L.A. Breast Cancer Immunotherapy: Facts and Hopes. Clin. Cancer Res. 2018, 24, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Castro, F.; Cardoso, A.P.; Gonçalves, R.M.; Serre, K.; Oliveira, M.J. Interferon-Gamma at the Crossroads of Tumor Immune Surveillance or Evasion. Front. Immunol. 2018, 9, 847. [Google Scholar] [CrossRef] [Green Version]
- Rody, A.H.U.; Pusztai, L.; Liedtke, C.; Gaetje, R.; Ruckhaeberle, E.; Solbach, C.; Hanker, L.; Ahr, A.; Metzler, D.; Engels, K.; et al. T-cell metagene predicts a favorable prognosis in estrogen receptor-negative and HER2-positive breast cancers. Breast Cancer Res. 2009, 11, R15. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Böhm, D.; Von Törne, C.; Steiner, E.; Puhl, A.; Pilch, H.; Lehr, H.-A.; Hengstler, J.G.; Kolbl, H.; Gehrmann, M. The humoral immune system has a key prognostic impact in node-negative breast cancer. Cancer Res. 2008, 68, 5405–5413. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Hellwig, B.; Hammad, S.; Othman, A.; Lohr, M.; Chen, Z.; Boehm, D.; Gebhard, S.; Petry, I.; Lebrecht, A.; et al. A comprehensive analysis of human gene expression profiles identifies stromal immunoglobulin kappa C as a compatible prognostic marker in human solid tumors. Clin. Cancer Res. 2012, 18, 2695–2703. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Hellwig, B.; Hammad, S.; Othman, A.; Lohr, M.; Chen, Z.; Boehm, D.; Gebhard, S.; Petry, I.; Lebrecht, A.; et al. Prognostic impact of CD4-positive T cell subsets in early breast cancer: A study based on the FinHer trial patient population. Breast Cancer Res. 2018, 20, 15. [Google Scholar] [CrossRef] [PubMed]
- Heimes, A.S.; Madjar, K.; Edlund, K.; Battista, M.J.; Almstedt, K.; Elger, T.; Krajnak, S.; Rahnenfuhrer, J.; Brenner, W.; Hasenburg, A.; et al. Subtype-specific prognostic impact of different immune signatures in node-negative breast cancer. Breast Cancer Res. Treat. 2017, 165, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Weichselbaum, R.R.; Ishwaran, H.; Yoon, T.; Nuyten, D.S.; Baker, S.W.; Khodarev, N.; Su, A.W.; Shaikh, A.Y.; Roach, P.; Kreike, B.; et al. An interferon-related gene signature for DNA damage resistance is a predictive marker for chemotherapy and radiation for breast cancer. Proc. Natl. Acad. Sci. USA 2008, 105, 18490–18495. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, Y.; Mimura, K.; Tamaki, T.; Shiraishi, K.; Kua, L.-F.; Koh, V.; Ohmori, M.; Kimura, A.; Inoue, S.; Okayama, H.; et al. PhosphoSTAT1 expression as a potential biomarker for antiPD1/antiPDL1 immunotherapy for breast cancer. Int. J. Oncol. 2019, 54, 2030–2038. [Google Scholar]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef]
- Legrier, M.-E.; Bieche, I.; Gaston, J.; Beurdeley, A.; Yvonnet, V.; Déas, O.; Thuleau, A.; Château-Joubert, S.; Servely, J.-L.; Vacher, S.; et al. Activation of IFN/STAT1 signalling predicts response to chemotherapy in oestrogen receptor-negative breast cancer. Br. J. Cancer 2016, 114, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Narang, P.; Chen, M.; Sharma, A.A.; Anderson, K.S.; Wilson, M.A. The neoepitope landscape of breast cancer: Implications for immunotherapy. BMC Cancer 2019, 19, 200. [Google Scholar] [CrossRef] [Green Version]
- Karn, T.; Denkert, C.; Weber, K.; Holtrich, U.; Hanusch, C.; Sinn, B.; Higgs, B.; Jank, P.; Sinn, H.; Huober, J.; et al. Tumor mutational burden and immune infiltration as independent predictors of response to neoadjuvant immune checkpoint inhibition in early TNBC in GeparNuevo. Ann. Oncol. 2020, 31, 1216–1222. [Google Scholar] [CrossRef]
- Callari, M.; Musella, V.; Di Buduo, E.; Sensi, M.L.; Miodini, P.; Dugo, M.; Orlandi, R.; Agresti, R.; Paolini, B.; Carcangiu, M.L.; et al. Subtype-dependent prognostic relevance of an interferon-induced pathway metagene in node-negative breast cancer. Mol. Oncol. 2014, 8, 1278–1289. [Google Scholar] [CrossRef]
- Filipits, M.; Rudas, M.; Jakesz, R.; Dubsky, P.; Fitzal, F.; Singer, C.F.; Dietze, O.; Greil, R.; Jelen, A.; Sevelda, P.; et al. A new molecular predictor of distant recurrence in ER-positive, HER2-negative breast cancer adds independent information to conventional clinical risk factors. Clin. Cancer Res. 2011, 17, 6012–6020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haibe-Kains, B.; Desmedt, C.; Loi, S.M.; Culhane, A.C.; Bontempi, G.; Quackenbush, J.; Sotiriou, C. A three-gene model to robustly identify breast cancer molecular subtypes. J. Natl. Cancer Inst. 2012, 104, 311–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Gene Symbol | Probeset |
|---|---|---|
| Interferon-γ | IFNG | 210354_at |
| Interferon-γ receptor 1 | IFNGR1 | 202727_s_at 211676_s_at |
| Interferon-γ receptor 2 | IFNGR2 | 201642_at |
| Interferon regulatory factor 1 | IRF1 | 202531_at |
| Janus kinase 1 | JAK1 | 201648_at |
| Janus kinase 2 | JAK2 | 205841_at 205842_s_at |
| Signal transducer and activator of transcription 1 | STAT1 | 200887_s_at 209969_s_at |
| HR | 95% CI | p-Value | |||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| IFN-γ-signature | Low vs. high | 1.554 | 1.099 | 2.199 | 0.013 |
| IFN-γ | Low vs. High expression | 1.084 | 0.769 | 1.527 | 0.646 |
| Age | </=50 vs. >50 | 1.297 | 0.881 | 1.909 | 0.188 |
| T | T1 vs. T2, T3,4 | 0.480 | 0.327 | 0.705 | <0.001 |
| N | N0 vs. N1,2,3 | 0.493 | 0.344 | 0.706 | <0.001 |
| Grade | GI/II vs. III | 0.217 | 0.089 | 0.531 | 0.001 |
| ER | Neg. vs. pos. | 1.954 | 1.328 | 2.905 | 0.001 |
| PR | Neg. vs. pos. | 1.843 | 1.287 | 2.640 | 0.001 |
| HER2 | Neg. vs. pos. | 0.557 | 0.336 | 0.926 | 0.024 |
| Ki-67 | <20% vs. >20% | 0.577 | 0.389 | 0.886 | 0.006 |
| Subtype | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Luminal A-like | 0.841 (0.430–1.642) | 0.611 | 1.066 (0.477–2.380) | 0.877 |
| Luminal B-like | 1.320 (0.785–2.218) | 0.295 | 1.659 (0.909–3.028) | 0.099 |
| HER2-positive | 1.127 (0.444–2.861) | 0.801 | 1.265 (0.460–3.475) | 0.649 |
| Basal-like | 2.459 (1.040–5.815) | 0.040 | 2.779 (1.117–6.919) | 0.028 |
| Subtype | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Luminal A-like | 1.194 (0.607–2.348) | 0.607 | 1.314 (0.596–2.898) | 0.498 |
| Luminal B-like | 2.109 (1.206–3.688) | 0.009 | 2.690 (1.416–5.112) | 0.003 |
| HER2-positive | 2.669 (1.042–6.840) | 0.041 | 1.925 (0.620–5.978) | 0.257 |
| Basal-like | 2.355 (0.972–5.707) | 0.058 | 3.458 (1.154–10.359) | 0.027 |
| HR | 95% CI | p-Value | |||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| IFN-γ signature | Low vs. high | 2.287 | 1.440 | 3.633 | <0.001 |
| Ki-67 | <20% vs. >20% | 0.680 | 0.431 | 1.073 | 0.098 |
| T | T1 vs. T2,3,4 | 0.608 | 0.378 | 0.979 | 0.041 |
| N | N0 vs. N1,2,3 | 0.982 | 0.621 | 1.554 | 0.939 |
| Grade | GI/II vs. III | 0.310 | 0.110 | 0.870 | 0.026 |
| ER | Neg. vs. pos. | 2.171 | 1.003 | 4.701 | 0.049 |
| PR | Neg. vs. pos. | 0.997 | 0.506 | 1.965 | 0.993 |
| HER2 | Neg. vs. pos. | 0.329 | 0.410 | 1.348 | 0.329 |
| Number of Patients (n = 461) | Percentage (%) | |
|---|---|---|
| Age at diagnosis | ||
| ≤50 | 104 | 22.6 |
| >50 | 357 | 77.4 |
| Tumor size | ||
| T1 | 188 | 40.8 |
| T2 | 214 | 46.4 |
| T3 | 19 | 4.1 |
| T4 | 39 | 8.5 |
| missing value | 1 | 0.2 |
| Tumor grade | ||
| GI | 62 | 13.4 |
| GII | 261 | 56.6 |
| GIII | 106 | 23 |
| missing value | 32 | 6.9 |
| Lymph node status | ||
| N0 | 253 | 54.9 |
| N1 | 138 | 29.9 |
| N2 | 49 | 10.6 |
| missing value | 21 | 4.6 |
| Tumor type | ||
| Invasive ductal (NST) | 291 | 63.1 |
| Invasive lobular | 79 | 17.1 |
| others | 91 | 19.7 |
| ER | ||
| positive | 381 | 82.6 |
| negative | 79 | 17.1 |
| missing value | 1 | 0.2 |
| PR | ||
| positive | 346 | 75.1 |
| negative | 114 | 24.7 |
| missing value | 1 | 0.2 |
| HER2 | ||
| positive | 46 | 10 |
| negative | 358 | 77.7 |
| missing value | 57 | 12.3 |
| Ki-67 | ||
| >20% | 138 | 29.9 |
| ≤20% | 250 | 54.2 |
| missing value | 73 | 15.8 |
| Molecular subtypes | ||
| Luminal A | 189 | 41 |
| Luminal B | 182 | 39.5 |
| Basal-like | 51 | 11.1 |
| HER2-positive | 39 | 8.5 |
| Distant metastasis | ||
| Yes | 132 | 28.6 |
| No | 329 | 71.4 |
| Treatment cohort | ||
| N0, untreated | 200 | 43.4 |
| tamoxifen | 165 | 35.8 |
| chemotherapy | 96 | 20.8 |
| CMF | 34 | 7.4 |
| EC | 62 | 13.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heimes, A.-S.; Härtner, F.; Almstedt, K.; Krajnak, S.; Lebrecht, A.; Battista, M.J.; Edlund, K.; Brenner, W.; Hasenburg, A.; Sahin, U.; et al. Prognostic Significance of Interferon-γ and Its Signaling Pathway in Early Breast Cancer Depends on the Molecular Subtypes. Int. J. Mol. Sci. 2020, 21, 7178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197178
Heimes A-S, Härtner F, Almstedt K, Krajnak S, Lebrecht A, Battista MJ, Edlund K, Brenner W, Hasenburg A, Sahin U, et al. Prognostic Significance of Interferon-γ and Its Signaling Pathway in Early Breast Cancer Depends on the Molecular Subtypes. International Journal of Molecular Sciences. 2020; 21(19):7178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197178
Chicago/Turabian StyleHeimes, Anne-Sophie, Franziska Härtner, Katrin Almstedt, Slavomir Krajnak, Antje Lebrecht, Marco J. Battista, Karolina Edlund, Walburgis Brenner, Annette Hasenburg, Ugur Sahin, and et al. 2020. "Prognostic Significance of Interferon-γ and Its Signaling Pathway in Early Breast Cancer Depends on the Molecular Subtypes" International Journal of Molecular Sciences 21, no. 19: 7178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197178