Prognostic Role of Survivin and Macrophage Infiltration Quantified on Protein and mRNA Level in Molecular Subtypes Determined by RT-qPCR of KRT5, KRT20, and ERBB2 in Muscle-Invasive Bladder Cancer Treated by Adjuvant Chemotherapy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Population
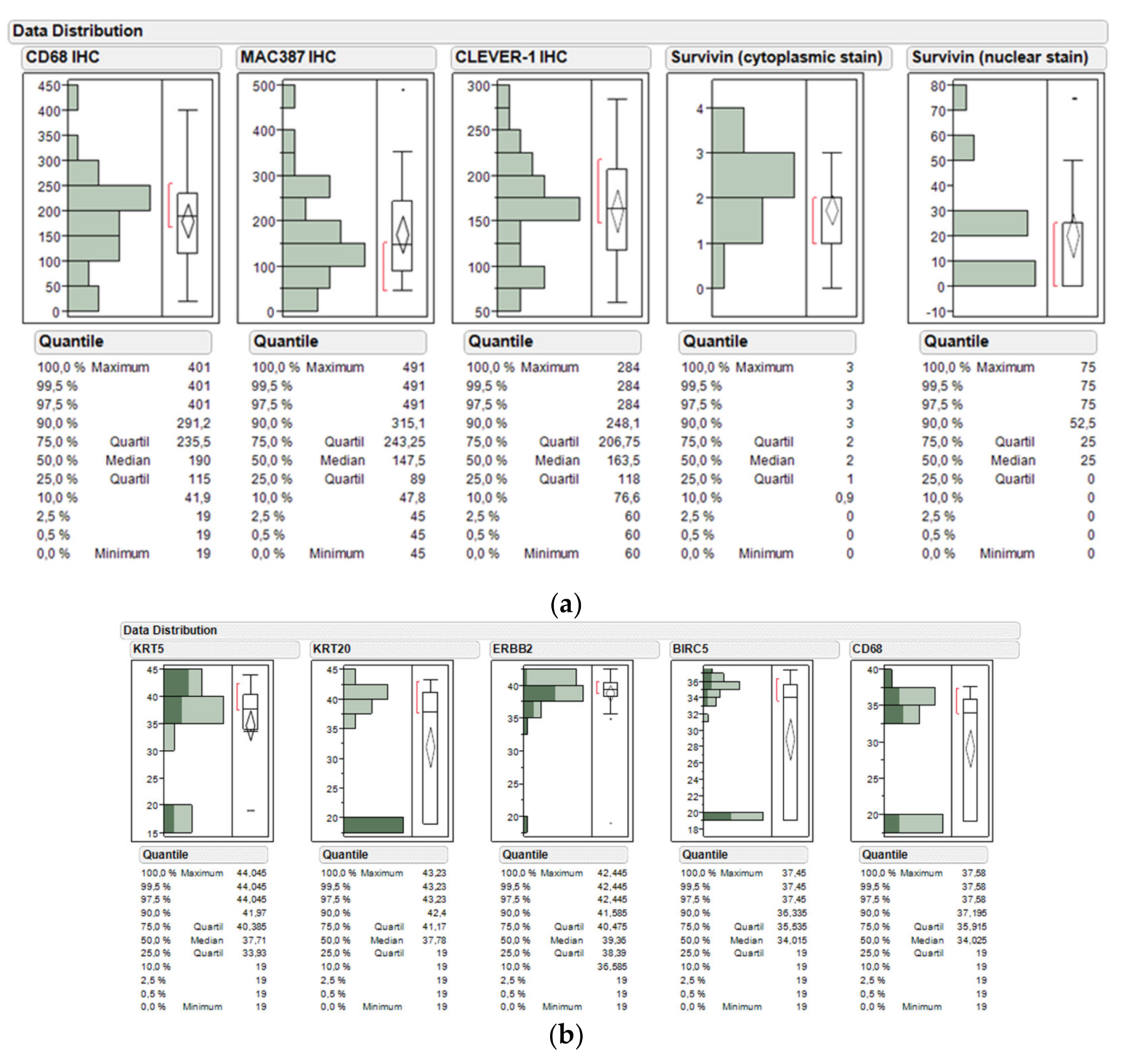
2.2. Distribution of Assessed Protein Markers across the Study Cohort
2.3. Distribution of Assessed mRNA Markers across the Study Cohort
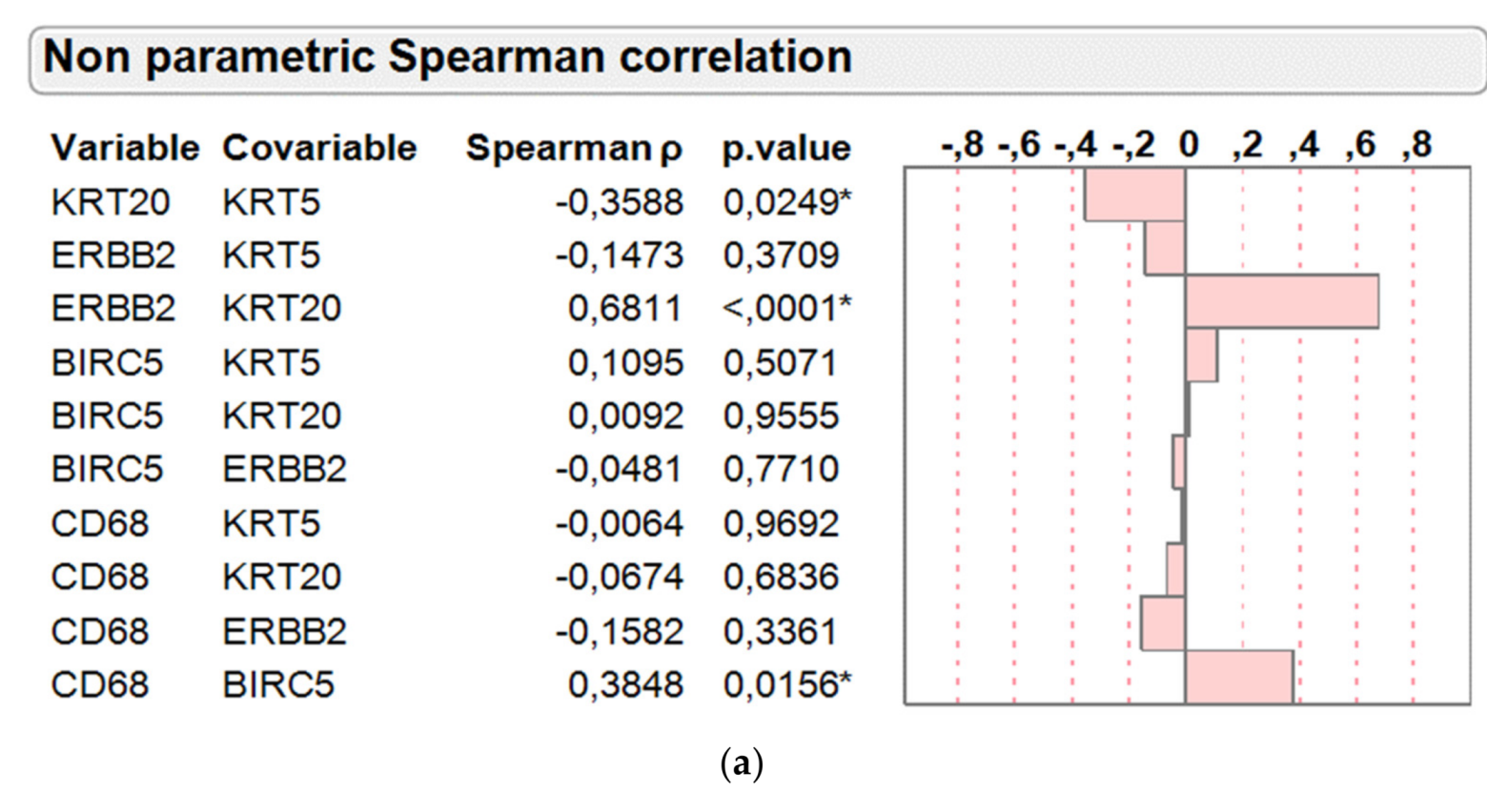
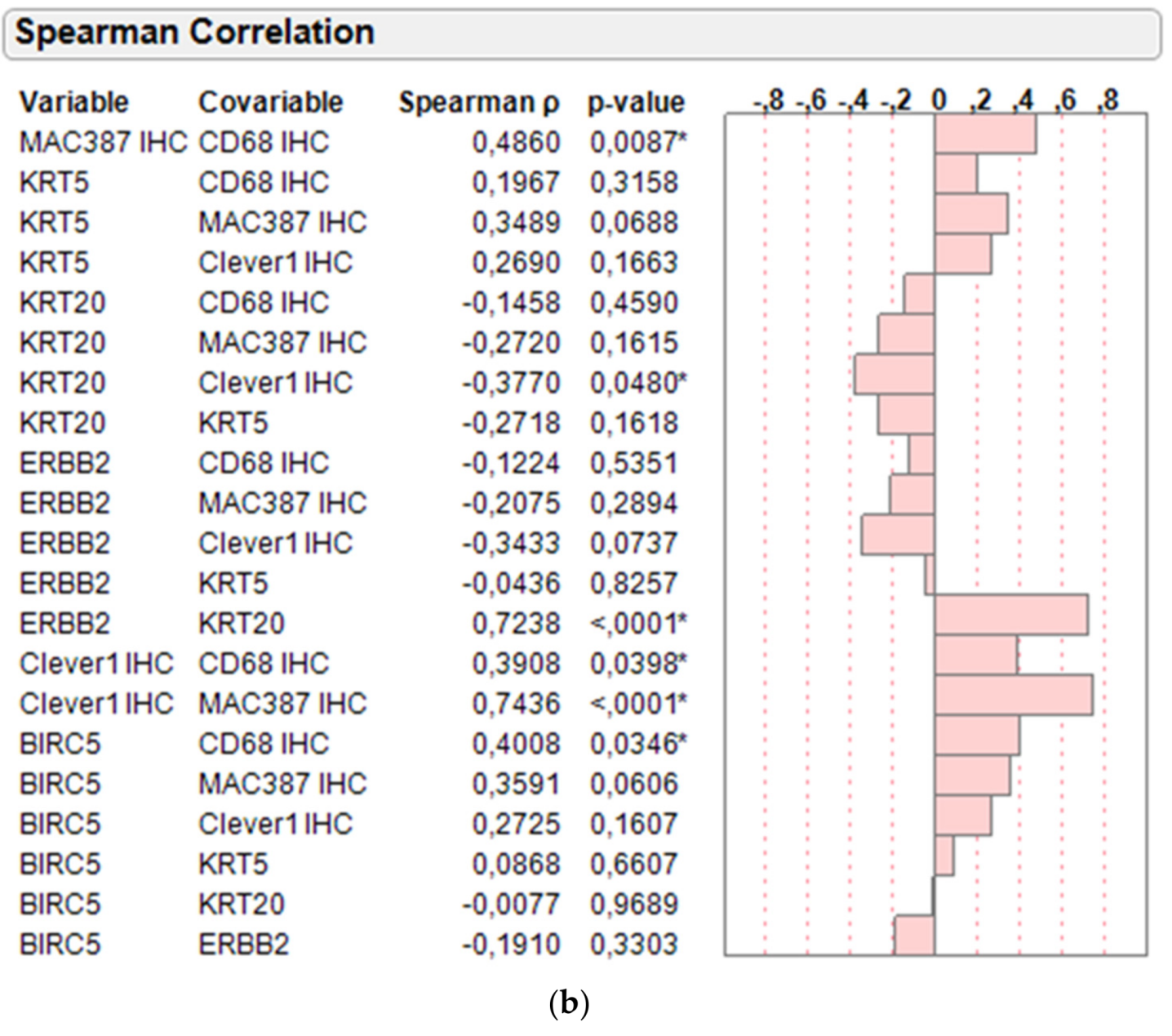
2.4. Correlation of Protein and mRNA Markers on Basis of Molecular Subtyping and Clinical Variables
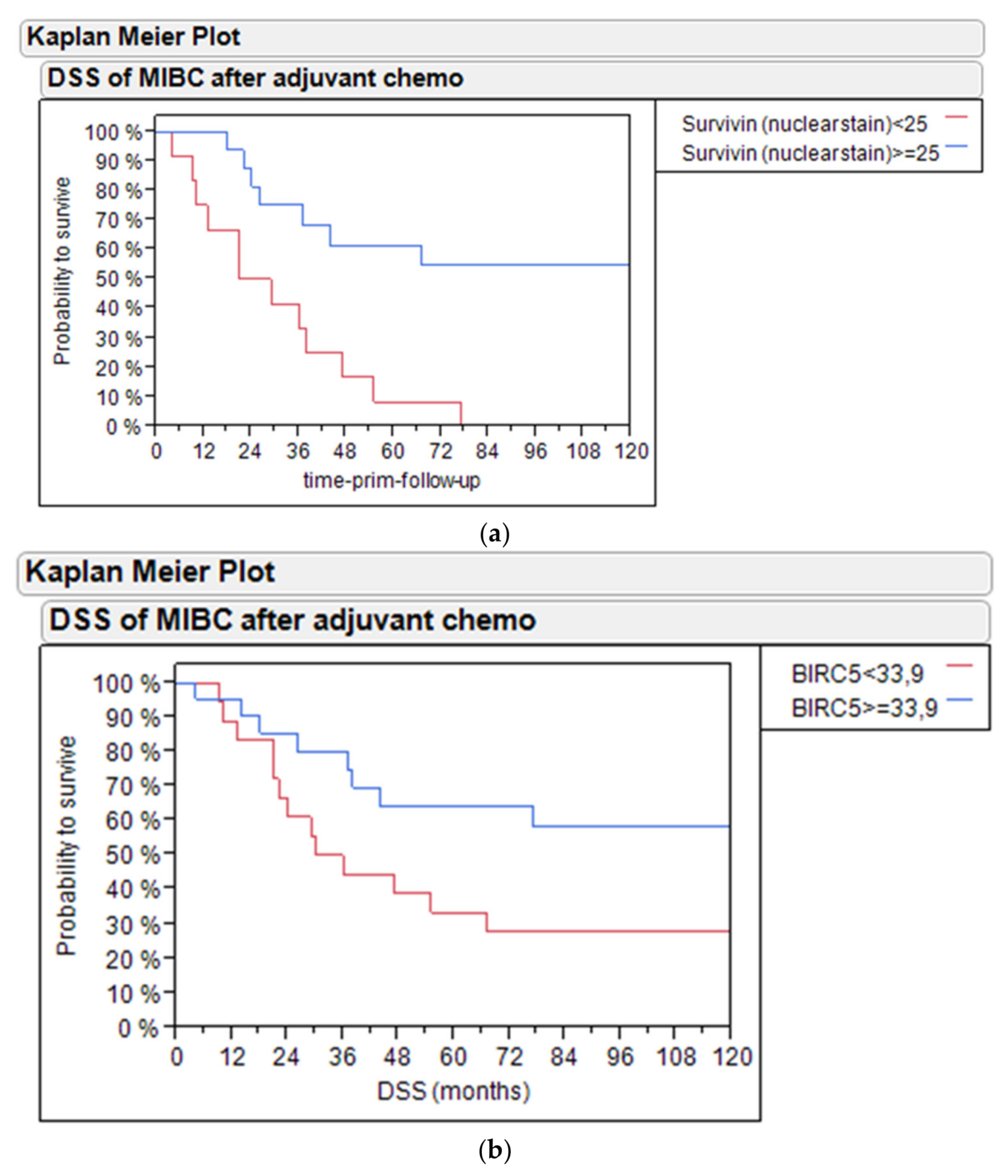
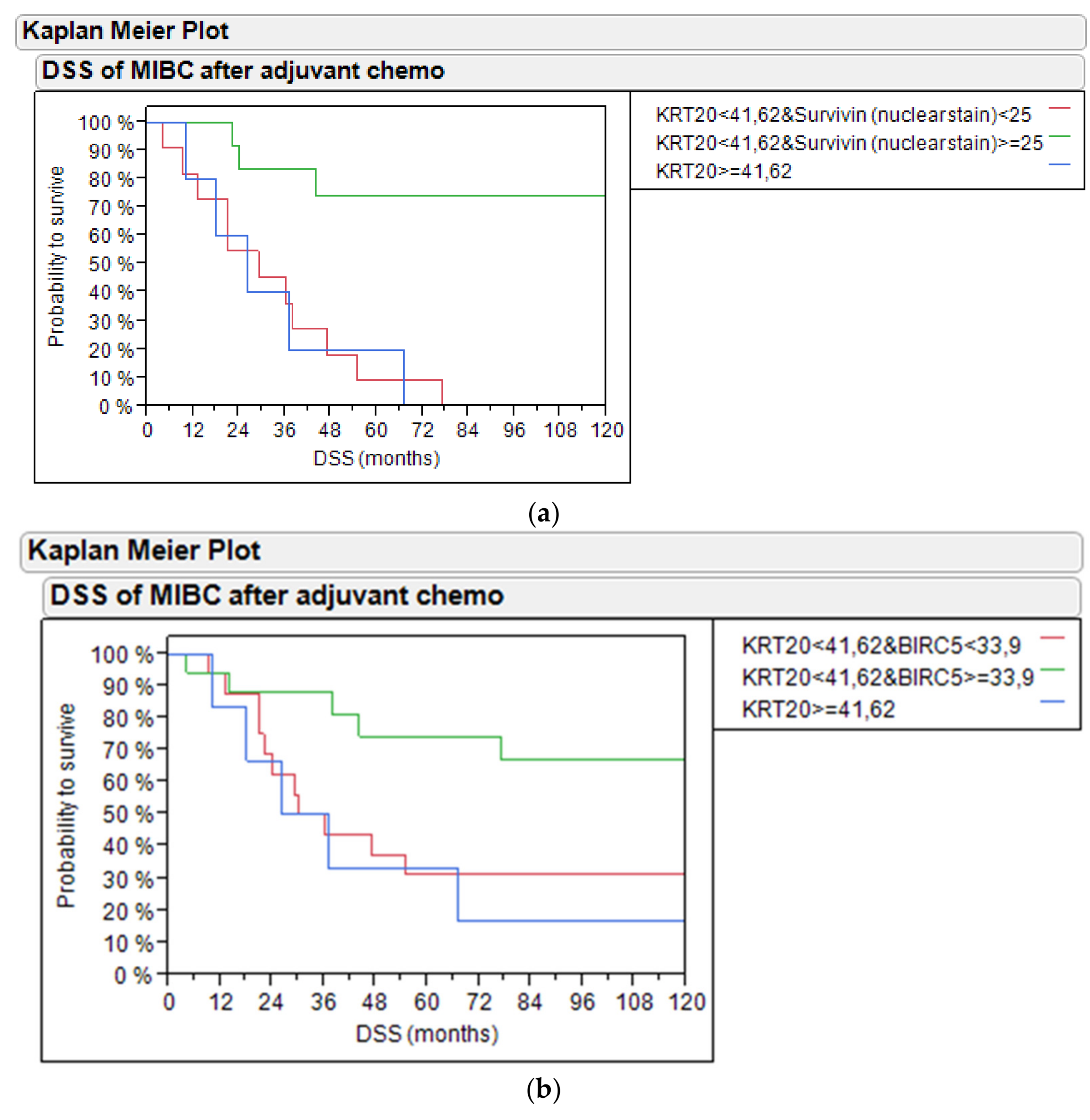
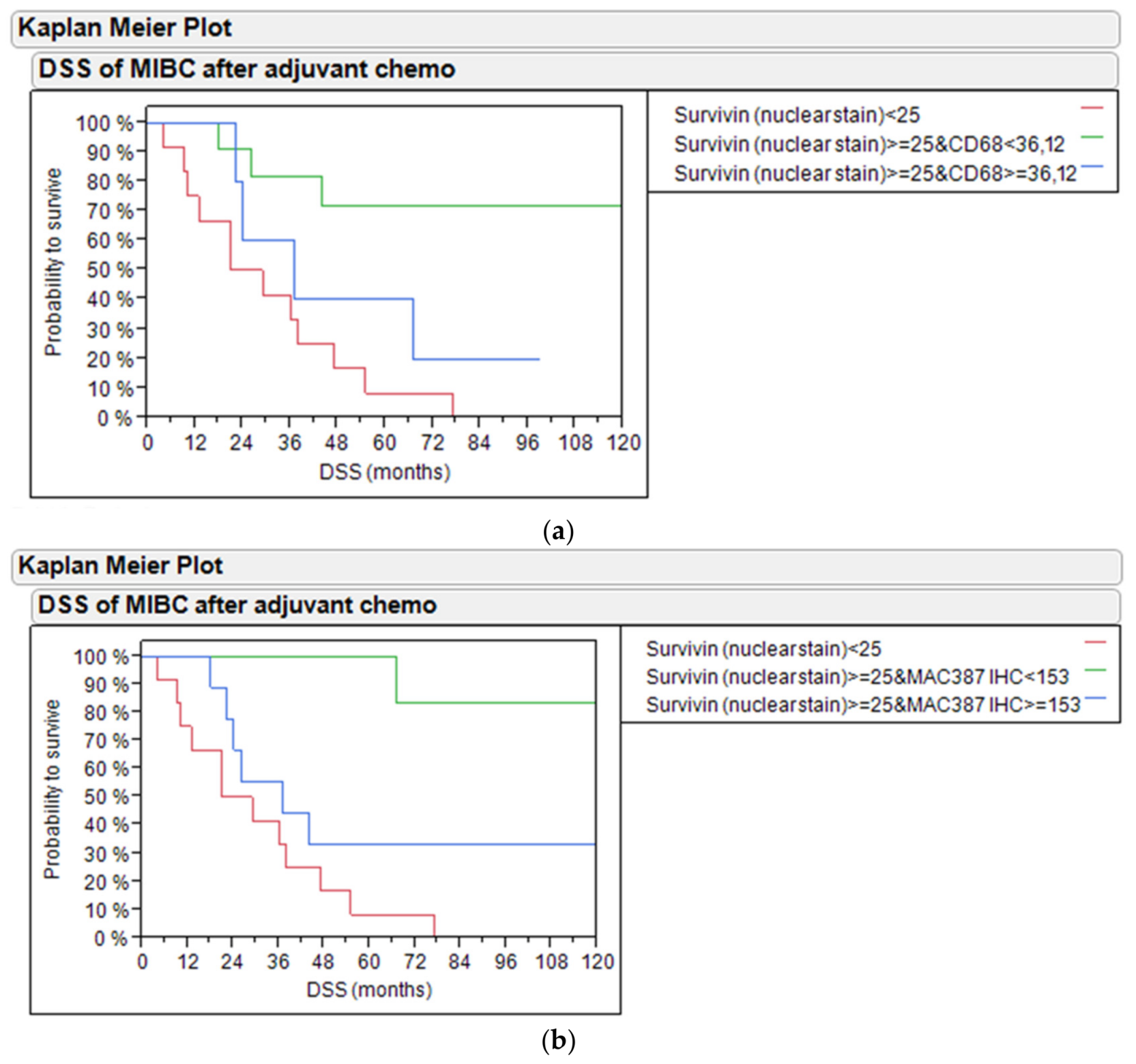
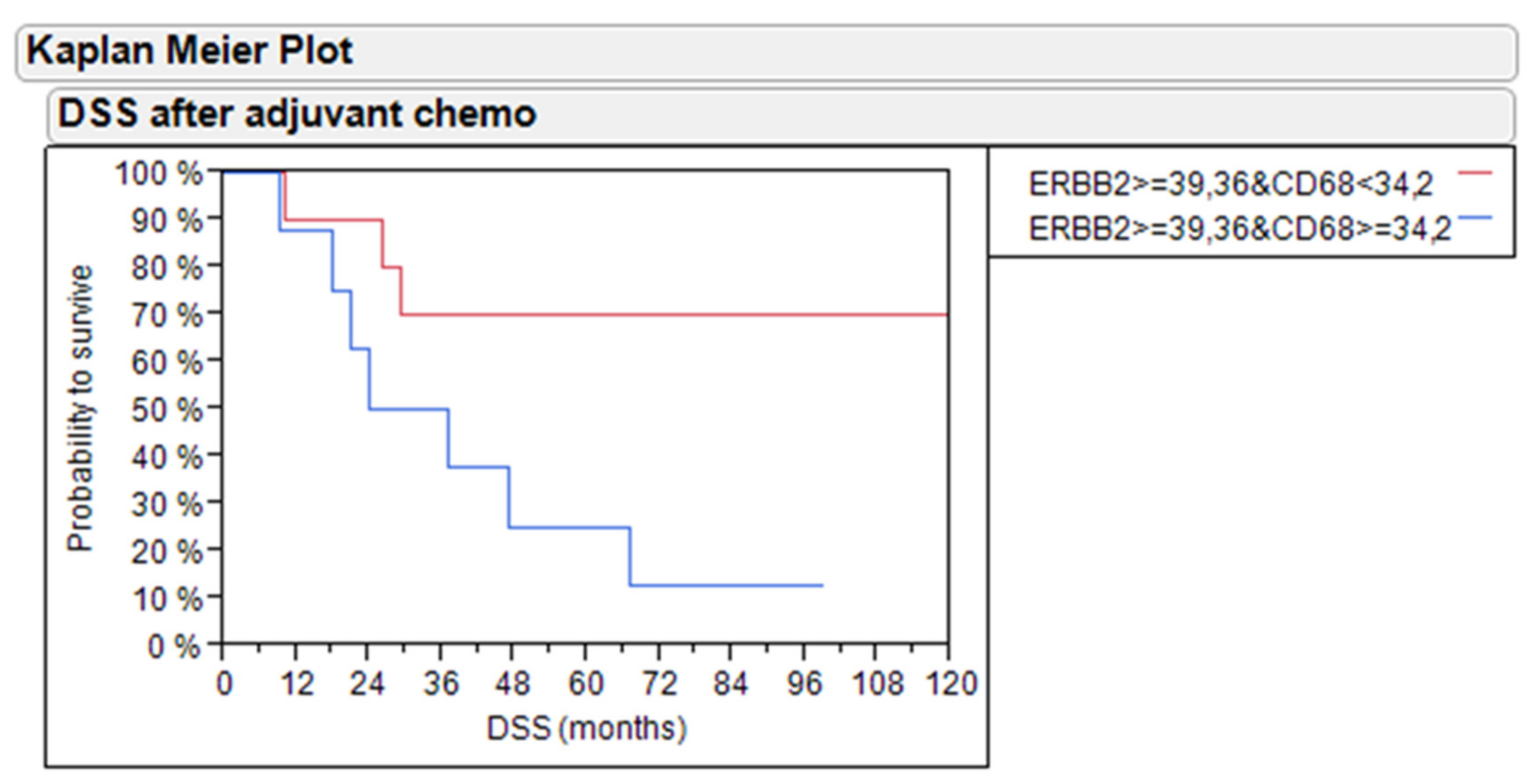
2.5. Disease-Specific Survival Analysis by Survivin and Macrophage Infiltration in Subtypes
3. Discussion
4. Materials and Methods
4.1. Patients
4.1.1. Patient Population
4.1.2. Eligibility
4.2. Pretreatment Evaluation
4.3. Assessment of Treatment Efficacy
4.4. Dose Modifications
4.5. Criteria for Follow-Up
4.6. Clinical Follow-Up and Treatment Efficacy
4.7. Procedure
4.8. Immunostaining for CD68, MAC387, and CLEVER-1
4.9. Immunostaining for Survivin
4.10. Isolation of Tumor RNA
4.11. Gene Expression by RT-qPCR
4.12. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BC | bladder cancer |
| BIRC5 | baculoviral IAP repeat containing 5 (BIRC5) |
| BMI | body mass index |
| BRCA1 | breast cancer 1 |
| Cis | carcinoma in situ |
| CLEVER-1 | common lymphatic endothelial and vascular endothelial receptor-1 |
| CR | complete response |
| DCT | Delta Cycle Threshold (gene expression based on difference of thereshold passing of individual genes when using qPCR) |
| DPX | distyrene plasticizer xylene |
| DSS | disease-specific survival |
| GC | gemcitabine and cisplatin chemotherapy |
| IHC | immunohistochemistry |
| N | lymph node status |
| MEC | methotrexate, epirubicin and cisplatin chemotherapy |
| MIBC | muscle-invasive bladder cancer |
| M | metastases status |
| MVAC | methotrexate, vinblastine, adriamycin and cisplatin chemotherapy |
| MVEC | methotrexate, vinblastine, epirubicin and cisplatin chemotherapy |
| NC | no change |
| NGS | next generation sequencing |
| NMIBC | non-muscle invasive bladder cancer |
| OS | overall survival |
| PCG | paclitaxel, cisplatin and gemcitabine chemotherapy |
| PCR | polymerase chain reaction |
| PD | progressive disease |
| PFS | progression-free survival |
| PR | partial response |
| RC | radical cystectomy |
| RECIST | Response Evaluation criteria in Solid Tumors |
| TMA | tissue microarray |
| TURB | transurethral resection of bladder |
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Witjes, J.A.; Compérat, E.; Cowan, N.C.; De Santis, M.; Gakis, G.; Lebret, T.; Ribal, M.J.; Van Der Heijden, A.G.; Sherif, A. EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2013 Guidelines. Eur. Urol. 2014, 65, 778–792. [Google Scholar] [CrossRef]
- Alfred Witjes, J.; Lebret, T.; Comperat, E.M.; De Santis, M.; Gakis, G.; Lebret, T.; Ribal, M.J.; Van der Heiden, M.J.; Sherif, A. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef]
- Kluth, L.A.; Black, P.C.; Bochner, B.H.; Catto, J.; Lerner, S.P.; Stenzl, A.; Sylvester, R.; Vickers, A.J.; Xylinas, E.; Shariat, S.F. Prognostic and Prediction Tools in Bladder Cancer: A Comprehensive Review of the Literature. Eur. Urol. 2015, 68, 238–253. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, A.-C.; Wild, P.; Leicht, C.; Bertz, S.; Danenberg, K.D.; Danenberg, P.V.; Stöhr, R.; Stöckle, M.; Lehmann, J.; Schuler, M.; et al. MDR1 and ERCC1 Expression Predict Outcome of Patients with Locally Advanced Bladder Cancer Receiving Adjuvant Chemotherapy. Neoplasia 2010, 12, 628–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, H.; Suri, P.; Gupta, J.C.; Talwar, G.; Dubey, S. Survivin: A unique target for tumor therapy. Cancer Cell Int. 2016, 16, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engels, K.; Knauer, S.; Metzler, D.; Simf, C.; Struschka, O.; Bier, C.; Mann, W.; Kovács, A.; Stauber, R.; Knauer, S.; et al. Dynamic intracellular survivin in oral squamous cell carcinoma: Underlying molecular mechanism and potential as an early prognostic marker. J. Pathol. 2007, 211, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Yang, J.; Ramnath, N.; Javle, M.M.; Tan, N. Nuclear or cytoplasmic expression of survivin: What is the significance? Int. J. Cancer 2005, 114, 509–512. [Google Scholar] [CrossRef] [Green Version]
- Uren, A.G.; Wong, L.; Pakusch, M.; Fowler, K.J.; Burrows, F.J.; Vaux, D.L.; Choo, K. Survivin and the inner centromere protein INCENP show similar cell-cycle localization and gene knockout phenotype. Curr. Boil. 2000, 10, 1319–1328. [Google Scholar] [CrossRef] [Green Version]
- Dohi, T.; Beltrami, E.; Wall, N.R.; Plescia, J.; Altieri, D.C. Mitochondrial survivin inhibits apoptosis and promotes tumorigenesis. J. Clin. Investig. 2004, 114, 1117–1127. [Google Scholar] [CrossRef]
- Dyrskjøt, L.; Reinert, T.; Algaba, F.; Christensen, E.; Nieboer, D.; Hermann, G.G.; Mogensen, K.; Beukers, W.; Marquez, M.; Segersten, U.; et al. Prognostic Impact of a 12-gene Progression Score in Non-muscle-invasive Bladder Cancer: A Prospective Multicentre Validation Study. Eur. Urol. 2017, 72, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Holness, C.L.; Simmons, D.L. Molecular cloning of CD68, a human macrophage marker related to lysosomal glycoproteins. Blood 1993, 81, 1607–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kzhyshkowska, J.; Gratchev, A.; Goerdt, S. Stabilin-1, a homeostatic scavenger receptor with multiple functions. J. Cell Mol. Med. 2006, 10, 635–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tervahartiala, M.; Taimen, P.; Mirtti, T.; Koskinen, I.; Ecke, T.; Jalkanen, S.; Boström, P.J. Immunological tumor status may predict response to neoadjuvant chemotherapy and outcome after radical cystectomy in bladder cancer. Sci. Rep. 2017, 7, 12682. [Google Scholar] [CrossRef]
- Goebeler, M.; Roth, J.; Teigelkamp, S.; Sorg, C. The monoclonal antibody MAC387 detects an epitope on the calcium-binding protein MRP14. J. Leukoc. Boil. 1994, 55, 259–261. [Google Scholar] [CrossRef]
- Netea-Maier, R.T.; Smit, J.; Netea, M.G. Metabolic changes in tumor cells and tumor-associated macrophages: A mutual relationship. Cancer Lett. 2018, 413, 102–109. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network; Cancer Genome Atlas Research Network Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [CrossRef] [Green Version]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.-L.; et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [Green Version]
- Damrauer, J.S.; Hoadley, K.A.; Chism, D.D.; Fan, C.; Tignanelli, C.; Wobker, S.E.; Yeh, J.J.; Milowsky, M.I.; Iyer, G.; Parker, J.S.; et al. Intrinsic subtypes of high-grade bladder cancer reflect the hallmarks of breast cancer biology. Proc. Natl. Acad. Sci. USA 2014, 111, 3110–3115. [Google Scholar] [CrossRef] [Green Version]
- Breyer, J.; Wirtz, R.M.; Otto, W.; Erben, P.; Kriegmair, M.C.; Stoehr, R.; Eckstein, M.; Eidt, S.; Denzinger, S. In stage pT1 non-muscle-invasive bladder cancer (NMIBC), high KRT20 and low KRT5 mRNA expression identify the luminal subtype and predict recurrence and survival. Virchows Arch. 2017, 470, 267–274. [Google Scholar] [CrossRef]
- Kamoun, A.; De Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Breyer, J.; Wirtz, R.M.; Otto, W.; Laible, M.; Schlombs, K.; Erben, P.; Kriegmair, M.C.; Stoehr, R.; Eidt, S.; Denzinger, S.; et al. Predictive value of molecular subtyping in NMIBC by RT-qPCR of ERBB2, ESR1, PGR and MKI67 from formalin fixed TUR biopsies. Oncotarget 2017, 8, 67684–67695. [Google Scholar] [CrossRef] [PubMed]
- Kriegmair, M.; Wirtz, R.; Worst, T.; Breyer, J.; Ritter, M.; Keck, B.; Boehmer, C.; Otto, W.; Eckstein, M.; Weis, C.; et al. Prognostic Value of Molecular Breast Cancer Subtypes based on Her2, ESR1, PGR and Ki67 mRNA-Expression in Muscle Invasive Bladder Cancer. Transl. Oncol. 2018, 11, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.; Gallagher, L.; Rohan, S. Survivin: Role in Diagnosis, Prognosis, and Treatment of Bladder Cancer. Adv. Anat. Pathol. 2006, 13, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Master, Z.; Yu, J.L.; Rak, J.; Dumont, D.J.; Kerbel, R.S. A role for survivin in chemoresistance of endothelial cells mediated by VEGF. Proc. Natl. Acad. Sci. USA 2002, 99, 4349–4354. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.; Tsuji, N.; Asanuma, K.; Kobayashi, D.; Yagihashi, A.; Hirata, K.; Torigoe, T.; Sato, N.; Watanabe, N. Survivin as a predictor of cis-diamminedichloroplatinum sensitivity in gastric cancer patients. Cancer Sci. 2004, 95, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Rinaldetti, S.; Wirtz, R.; Worst, T.S.; Hartmann, A.; Breyer, J.; Dyrskjøt, L.; Erben, P. FOXM1 predicts disease progression in non-muscle invasive bladder cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 1701–1709. [Google Scholar] [CrossRef] [Green Version]
- Breyer, J.; Wirtz, R.M.; Erben, P.; Rinaldetti, S.; Worst, T.S.; Stoehr, R.; Eckstein, M.; Sikic, D.; Denzinger, S.; Burger, M.; et al. FOXM1 overexpression is associated with adverse outcome and predicts response to intravesical instillation therapy in stage pT1 non-muscle-invasive bladder cancer. BJU Int. 2018, 123, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Jeon, C.; Kim, M.; Kwak, C.; Kim, H.H.; Ku, J.H. Prognostic Role of Survivin in Bladder Cancer: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e76719. [Google Scholar] [CrossRef] [Green Version]
- Als, A.B.; Von Der Maase, H.; Koed, K.; Mansilla, F.; Toldbod, H.E.; Jensen, J.L.; Jensen, K.M.; Dyrskjøt, L.; Ulhøi, B.P.; Sengeløv, L.; et al. Emmprin and Survivin Predict Response and Survival following Cisplatin-Containing Chemotherapy in Patients with Advanced Bladder Cancer. Clin. Cancer Res. 2007, 13, 4407–4414. [Google Scholar] [CrossRef] [Green Version]
- Pollard, C.; Nitz, M.; Baras, A..; Williams, P.; Moskaluk, C.; Theodorescu, D. Genoproteomic mining of urothelial cancer suggests {gamma}-glutamyl hydrolase and diazepam-binding inhibitor as putative urinary markers of outcome after chemotherapy. Am. J. Pathol. 2009, 175, 1824–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, M.M.; Irjala, H.; Mirtti, T.; Taimen, P.; Kauko, T.; Ålgars, A.; Jalkanen, S.; Boström, P.J. Tumor-Associated Macrophages Provide Significant Prognostic Information in Urothelial Bladder Cancer. PLoS ONE 2015, 10, e0133552. [Google Scholar] [CrossRef] [PubMed]
- Palani, S.; Maksimow, M.; Miiluniemi, M.; Auvinen, K.; Jalkanen, S.; Salmi, M. Stabilin-1/CLEVER-1, a type 2 macrophage marker, is an adhesion and scavenging molecule on human placental macrophages. Eur. J. Immunol. 2011, 41, 2052–2063. [Google Scholar] [CrossRef] [PubMed]
- Irjala, H.; Elima, K.; Johansson, E.-L.; Merinen, M.; Kontula, K.; Alanen, K.; Grénman, R.; Salmi, M.; Jalkanen, S. The same endothelial receptor controls lymphocyte traffic both in vascular and lymphatic vessels. Eur. J. Immunol. 2003, 33, 815–824. [Google Scholar] [CrossRef]
- Salmi, M.; Jalkanen, S. A 90-kilodalton endothelial cell molecule mediating lymphocyte binding in humans. Science 1992, 257, 1407–1409. [Google Scholar] [CrossRef]
- Gleichenhagen, J.; Arndt, C.; Casjens, S.; Meinig, C.; Gerullis, H.; Raiko, I.; Bruning, T.; Ecke, T.; Johnen, G. Evaluation of a New Survivin ELISA and UBC((R)) Rapid for the Detection of Bladder Cancer in Urine. Int. J. Mol. Sci. 2018, 19, 226. [Google Scholar] [CrossRef] [Green Version]
- Eckstein, M.; Wirtz, R.M.; Pfannstil, C.; Wach, S.; Stoehr, R.; Breyer, J.; Erlmeier, F.; Gunes, C.; Nitschke, K.; Weichert, W.; et al. A multicenter round robin test of PD-L1 expression assessment in urothelial bladder cancer by immunohistochemistry and RT-qPCR with emphasis on prognosis prediction after radical cystectomy. Oncotarget 2018, 9, 15001–15014. [Google Scholar] [CrossRef] [Green Version]
- Eckstein, M.; Strissel, P.; Strick, R.; Weyerer, V.; Wirtz, R.; Pfannstiel, C.; Wullweber, A.; Lange, F.; Erben, P.; Stoehr, R.; et al. Cytotoxic T-cell-related gene expression signature predicts improved survival in muscle-invasive urothelial bladder cancer patients after radical cystectomy and adjuvant chemotherapy. J. Immunother. Cancer 2020, 8, e000162. [Google Scholar] [CrossRef]
- Filipits, M.; Dafni, U.; Gnant, M.; Polydoropoulou, V.; Hills, M.; Kiermaier, A.; De Azambuja, E.; Larsimont, D.P.; Rojo, F.; Viale, G.; et al. Association of p27 and Cyclin D1 Expression and Benefit from Adjuvant Trastuzumab Treatment in HER2-Positive Early Breast Cancer: A TransHERA Study. Clin. Cancer Res. 2018, 24, 3079–3086. [Google Scholar] [CrossRef] [Green Version]
- Sinn, H.-P.; Schneeweiss, A.; Keller, M.; Schlombs, K.; Laible, M.; Seitz, J.; Lakis, S.; Veltrup, E.; Altevogt, P.; Eidt, S.; et al. Comparison of immunohistochemistry with PCR for assessment of ER, PR, and Ki-67 and prediction of pathological complete response in breast cancer. BMC Cancer 2017, 17, 124. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | Total Cohort | PCR Cohort | IHC & PCR Cohort |
|---|---|---|---|
| Size (n) | 50 | 39 | 28 |
| Age (years) | |||
| Average | 65 | 67 | 68.5 |
| Range | 49-80 | 48–80 | 48–80 |
| Gender | |||
| Male | 38 (76%) | 27 (69%) | 18 (64%) |
| Female | 12 (24%) | 12 (31%) | 10 (36%) |
| ECOG Performance Status | |||
| 0 | 25 (50%) | 19 (49%) | 11 (39%) |
| 1 | 17 (34%) | 13 (33%) | 11 (39%) |
| 2 | 8 (16%) | 7 (18%) | 6 (21%) |
| Lymph Node Metastases before Chemotherapy | |||
| N0 | 21 (42%) | 16 (41%) | 10 (36%) |
| N1 | 7 (14%) | 4 (10%) | 2 (7%) |
| N2 | 22 (44%) | (19 (49%) | 16 (57%) |
| Clinical outcome after Chemotherapy | |||
| Progression | 27 (54%) | 21 (54%) | 18 (64%) |
| Overall death | 36 (72%) | 29 (74%) | 23 (82%) |
| Disease specific death | 27 (54%) | 21 (54%) | 19 (68%) |
| Overall survival | 14 (28%) | 10 (26%) | 5 (18%) |
| Response to Chemotherapy | |||
| Complete response | 20 (40%) | 15 (38%) | 8 (29%) |
| Partial response | 3 (6%) | 2 (5%) | 1 (4%) |
| No change | 25 (50%) | 20 (51%) | 18 (64%) |
| KRT5 | KRT20 | ERBB2 | BIRC5 | CD68 | PS | Age | Sex | BMI | Cis | T-Prim | G-Prim | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| KRT5 | 1.0000 | −0.1522 | −0.0286 | 0.1052 | 0.0028 | −0.0493 | −0.0477 | 0.1678 | −0.2302 | −0.0040 | −0.1413 | 0.0691 |
| KRT20 | −0.01522 | 1.0000 | 0.4266 | 0.0763 | −0.1783 | −0.0443 | 0.2165 | 0.2627 | 0.0498 | −0.3599 | −0.0544 | 0.1547 |
| ERBB2 | −0.0296 | 0.4266 | 1.0000 | 0.1019 | 0.0507 | −0.2721 | 0.0280 | 0.3259 | −0.0149 | −0.0934 | −0.1754 | −0.0563 |
| BIRC5 | 0.1052 | 0.0763 | 0.1019 | 1.0000 | 0.5390 | −0.0579 | 0.2019 | 0.1273 | −0.0553 | 0.2807 | 0.1831 | 0.0858 |
| CD68 | 0.0028 | −0.1783 | 0.0507 | 0.5390 | 1.0000 | 0.1646 | 0.3190 | −0.0525 | −0.1784 | 0.2361 | 0.1812 | −0.2662 |
| PS | −0.0493 | −0.0443 | −0.2721 | −0.0578 | 0.1646 | 1.0000 | 0.3352 | −0.1978 | 0.0978 | −0.1370 | 0.1196 | −0.0217 |
| Age | −0.0477 | 0.2185 | 0.0280 | 0.2019 | 0.3190 | 0.3352 | 1.0000 | 0.1101 | −0.3689 | 0.1915 | −0.1977 | −0.0184 |
| Sex | 0.1678 | 0.2827 | 0.3259 | 0.1273 | −0.0625 | −0.1978 | 0.1101 | 1.0000 | 0.0990 | −0.0160 | −0.1514 | −0.0358 |
| BMI | −0.2302 | 0.0498 | −0.0149 | −0.0553 | −0.1784 | 0.0978 | −0.3689 | 0.0990 | 1.0000 | −0.2538 | 0.2724 | −0.0904 |
| Cis | −0.0040 | −0.3599 | −0.0934 | 0.2007 | 0.2361 | −0.1370 | 0.1915 | −0.0160 | −0.2538 | 1.0000 | −0.1852 | 0.0154 |
| T-prim | −0.1413 | −0.0544 | −0.1754 | 0.1831 | 0.1612 | 0.1196 | −0.1977 | −0.1514 | 0.2724 | −0.1852 | 1.0000 | 0.2200 |
| G-prim | 0.0691 | 0.1547 | −0.0563 | 0.0858 | −0.2662 | −0.0217 | −0.0184 | −0.0356 | −0.0904 | 0.0154 | 0.2200 | 1.0000 |
| Parameter | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.07 | 0.99–1.14 | 0.0518 |
| Sex | 0.89 | 0.27–2.98 | 0.8329 |
| BMI | 1.16 | 1.00–1.24 | 0.0499 |
| Node status | 1.95 | 1.15–3.53 | 0.0127 |
| Stage | 1.13 | 0.42–3.16 | 0.8038 |
| Grade | 0.86 | 0.33–2.29 | 0.7638 |
| KRT20 × BIRC5 Groups | |||
| KRT20 low & BIRC5 high vs. KRT20 low & BIRC5 low | 0.22 | 0.06–0.75 | 0.0144 |
| KRT20 low & BIRC5 high vs. KRT20 high | 0.24 | 0.06–0.94 | 0.0407 |
| KRT20 low & BIRC5 low vs. KRT20 high | 1.09 | 0.28–4.39 | 0.8988 |
| Parameter | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.08 | 0.94–1.25 | 0.2911 |
| Sex | 1.25 | 0.23–7.45 | 0.7979 |
| BMI | 1.19 | 0.97–1.47 | 0.0985 |
| Node status | 1.75 | 0.89–3.87 | 0.1045 |
| Stage | 0.65 | 0.19–2.11 | 0.4750 |
| Grade | 0.86 | 0.33–2.29 | 0.4989 |
| KRT20 × BIRC5 Groups | |||
| KRT20 low & BIRC5 high vs. KRT20 low & BIRC5 low | 0.15 | 0.02–0.79 | 0.0252 |
| KRT20 low & BIRC5 high vs. KRT20 high | 0.26 | 0.02–1.93 | 0.1908 |
| KRT20 low & BIRC5 low vs. KRT20 high | 1.77 | 0.41–8.92 | 0.4489 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ecke, T.H.; Kiani, A.; Schlomm, T.; Friedersdorff, F.; Rabien, A.; Jung, K.; Kilic, E.; Boström, P.; Tervahartiala, M.; Taimen, P.; et al. Prognostic Role of Survivin and Macrophage Infiltration Quantified on Protein and mRNA Level in Molecular Subtypes Determined by RT-qPCR of KRT5, KRT20, and ERBB2 in Muscle-Invasive Bladder Cancer Treated by Adjuvant Chemotherapy. Int. J. Mol. Sci. 2020, 21, 7420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197420
Ecke TH, Kiani A, Schlomm T, Friedersdorff F, Rabien A, Jung K, Kilic E, Boström P, Tervahartiala M, Taimen P, et al. Prognostic Role of Survivin and Macrophage Infiltration Quantified on Protein and mRNA Level in Molecular Subtypes Determined by RT-qPCR of KRT5, KRT20, and ERBB2 in Muscle-Invasive Bladder Cancer Treated by Adjuvant Chemotherapy. International Journal of Molecular Sciences. 2020; 21(19):7420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197420
Chicago/Turabian StyleEcke, Thorsten H., Adisch Kiani, Thorsten Schlomm, Frank Friedersdorff, Anja Rabien, Klaus Jung, Ergin Kilic, Peter Boström, Minna Tervahartiala, Pekka Taimen, and et al. 2020. "Prognostic Role of Survivin and Macrophage Infiltration Quantified on Protein and mRNA Level in Molecular Subtypes Determined by RT-qPCR of KRT5, KRT20, and ERBB2 in Muscle-Invasive Bladder Cancer Treated by Adjuvant Chemotherapy" International Journal of Molecular Sciences 21, no. 19: 7420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197420