Axitinib in Ponatinib-Resistant B-Cell Acute Lymphoblastic Leukemia Harboring a T315L Mutation

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
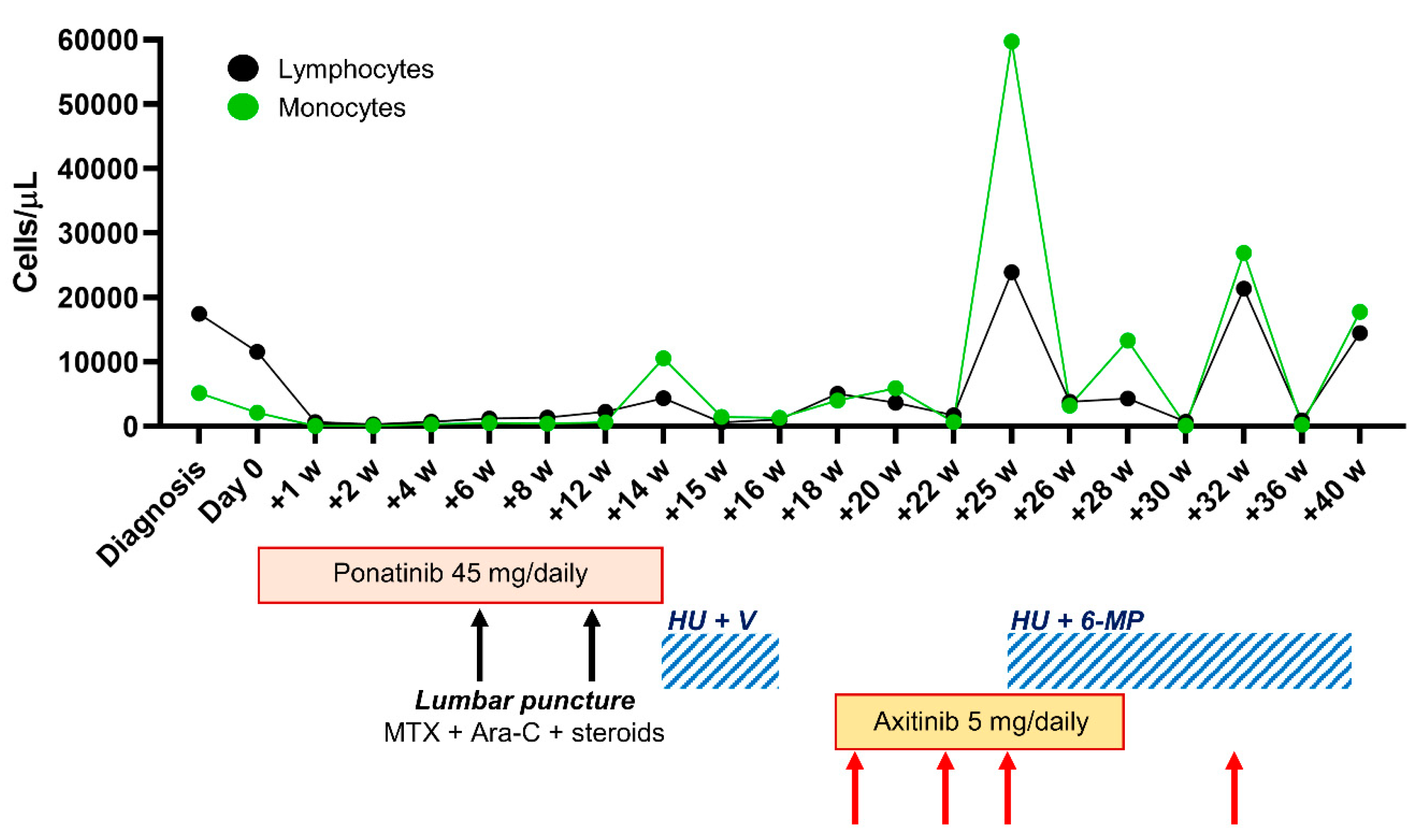
2. Case Presentation
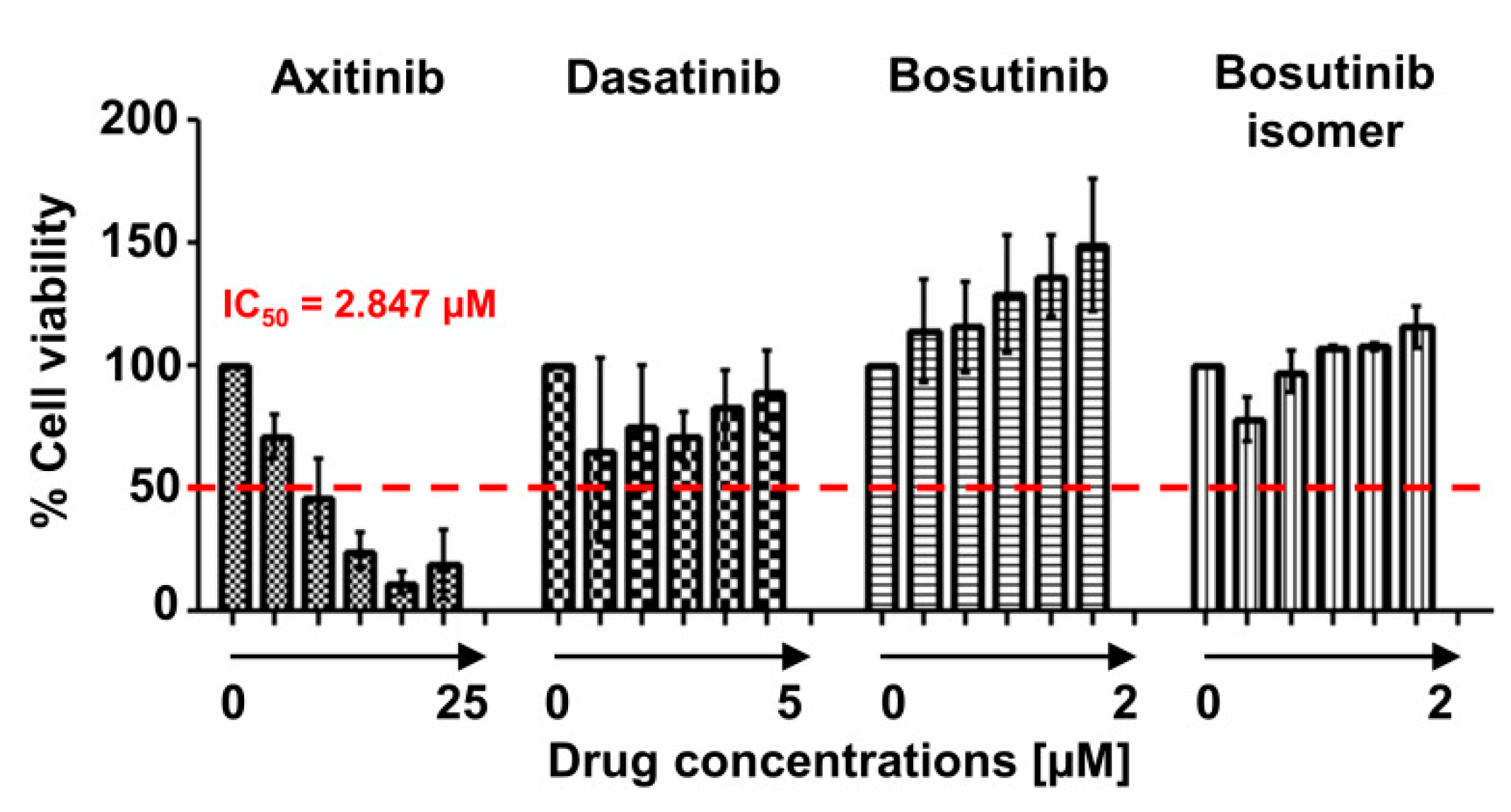
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moorman, A.V. New and emerging prognostic and predictive genetic biomarkers in B-cell precursor acute lymphoblastic leukemia. Haematologica 2016, 101, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belver, L.; Ferrando, A. The genetics and mechanisms of T cell acute lymphoblastic leukaemia. Nat. Rev. Cancer 2016, 16, 494–507. [Google Scholar] [CrossRef] [PubMed]
- Mullighan, C.G.; Collins-Underwood, J.R.; Phillips, L.A.; Loudin, M.G.; Liu, W.; Zhang, J.; Ma, J.; Coustan-Smith, E.; Harvey, R.C.; Willman, C.L.; et al. Rearrangement of CRLF2 in B-progenitor- and Down syndrome-associated acute lymphoblastic leukemia. Nat. Genet. 2009, 41, 1243–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacobucci, I.; Mullighan, C.G. Genetic Basis of Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2017, 35, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Plasschaert, S.L.; Kamps, W.A.; Vellenga, E.; de Vries, E.G.; de Bont, E.S. Prognosis in childhood and adult acute lymphoblastic leukaemia: A question of maturation? Cancer Treat. Rev. 2004, 30, 37–51. [Google Scholar] [CrossRef]
- Ottmann, O.; Dombret, H.; Martinelli, G.; Simonsson, B.; Guilhot, F.; Larson, R.A.; Rege-Cambrin, G.; Radich, J.; Hochhaus, A.; Apanovitch, A.M.; et al. Dasatinib induces rapid hematologic and cytogenetic responses in adult patients with Philadelphia chromosome positive acute lymphoblastic leukemia with resistance or intolerance to imatinib: Interim results of a phase 2 study. Blood 2007, 110, 2309–2315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignetti, M.; Fazi, P.; Cimino, G.; Martinelli, G.; Di Raimondo, F.; Ferrara, F.; Meloni, G.; Ambrosetti, A.; Quarta, G.; Pagano, L.; et al. Imatinib plus steroids induces complete remissions and prolonged survival in elderly Philadelphia chromosome-positive patients with acute lymphoblastic leukemia without additional chemotherapy: Results of the Gruppo Italiano Malattie Ematologiche dell’Adulto (GIMEMA) LAL0201-B protocol. Blood 2007, 109, 3676–3678. [Google Scholar] [PubMed] [Green Version]
- Foà, R.; Vitale, A.; Vignetti, M.; Meloni, G.; Guarini, A.; De Propris, M.S.; Elia, L.; Paoloni, F.; Fazi, P.; Cimino, G.; et al. GIMEMA Acute Leukemia Working Party. Dasatinib as first-line treatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood 2011, 118, 6521–6528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamai, M.; Inukai, T.; Kojika, S.; Abe, M.; Kagami, K.; Harama, D.; Shinohara, T.; Watanabe, A.; Oshiro, H.; Akahane, K.; et al. T315I mutation of BCR-ABL1 into human Philadelphia chromosome-positive leukemia cell lines by homologous recombination using the CRISPR/Cas9 system. Sci. Rep. 2018, 8, 9966. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Jabbour, E.J.; Ravandi, F.; Short, N.J.; Thomas, D.A.; Garcia-Manero, G.; Daver, N.G.; Kadia, T.M.; Konopleva, M.Y.; Jain, N.; et al. Hyper-CVAD plus ponatinib versus hyper-CVAD plus dasatinib as frontline therapy for patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: A propensity score analysis. Cancer 2016, 122, 3650–3656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okabe, S.; Tauchi, T.; Tanaka, Y.; Sakuta, J.; Ohyashiki, K. Anti-leukemic activity of axitinib against cells harboring the BCR-ABL T315I point mutation. J. Hematol. Oncol. 2015, 8, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pemovska, T.; Johnson, E.; Kontro, M.; Repasky, G.A.; Chen, J.; Wells, P.; Cronin, C.N.; McTigue, M.; Kallioniemi, O.; Porkka, K.; et al. Axitinib effectively inhibits BCR-ABL1(T315I) with a distinct binding conformation. Nature 2015, 519, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Zabriskie, M.S.; Eide, C.A.; Yan, D.; Vellore, N.A.; Pomicter, A.D.; Savage, S.L.; Druker, B.J.; Deininger, M.W.; O’Hare, T. Extreme mutational selectivity of axitinib limits its potential use as a targeted therapeutic for BCR-ABL1-positive leukemia. Leukemia 2016, 30, 1418–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelli Luserna Di Rorà, A.; Beeharry, N.; Imbrogno, E.; Ferrari, A.; Robustelli, V.; Righi, S.; Sabattini, E.; Verga Falzacappa, M.V.; Ronchini, C.; Testoni, N.; et al. Targeting WEE1 to enhance conventional therapies for acute lymphoblastic leukemia. J. Hematol. Oncol. 2018, 11, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boddu, P.; Shah, A.R.; Borthakur, G.; Verstovsek, S.; Garcia-Manero, G.; Daver, N.; Kadia, T.; Ravandi, F.; Jain, N.; Alhuraiji, A.; et al. Life after ponatinib failure: Outcomes of chronic and accelerated phase CML patients who discontinued ponatinib in the salvage setting. Leuk. Lymphoma 2018, 59, 1312–1322. [Google Scholar] [CrossRef] [PubMed]
- Ting, S.; Mixue, X.; Lixia, Z.; Xueying, L.; Wanzhuo, X.; Xiujin, Y. T315I mutation exerts a dismal prognosis on adult BCR-ABL1-positive acute lymphoblastic leukemia, and salvage therapy with ponatinib or CAR-T cell and bridging to allogeneic hematopoietic stem cell transplantation can improve clinical outcomes. Ann. Hematol. 2020, 99, 829–834. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giudice, V.; Ghelli Luserna di Rorà, A.; Serio, B.; Guariglia, R.; Giannini, M.B.; Ferrari, A.; Simonetti, G.; Selleri, C.; Martinelli, G. Axitinib in Ponatinib-Resistant B-Cell Acute Lymphoblastic Leukemia Harboring a T315L Mutation. Int. J. Mol. Sci. 2020, 21, 9724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249724
Giudice V, Ghelli Luserna di Rorà A, Serio B, Guariglia R, Giannini MB, Ferrari A, Simonetti G, Selleri C, Martinelli G. Axitinib in Ponatinib-Resistant B-Cell Acute Lymphoblastic Leukemia Harboring a T315L Mutation. International Journal of Molecular Sciences. 2020; 21(24):9724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249724
Chicago/Turabian StyleGiudice, Valentina, Andrea Ghelli Luserna di Rorà, Bianca Serio, Roberto Guariglia, Maria Benedetta Giannini, Anna Ferrari, Giorgia Simonetti, Carmine Selleri, and Giovanni Martinelli. 2020. "Axitinib in Ponatinib-Resistant B-Cell Acute Lymphoblastic Leukemia Harboring a T315L Mutation" International Journal of Molecular Sciences 21, no. 24: 9724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21249724