ITIH5 and ECRG4 DNA Methylation Biomarker Test (EI-BLA) for Urine-Based Non-Invasive Detection of Bladder Cancer

 ,
, 
Abstract
:1. Introduction
2. Results
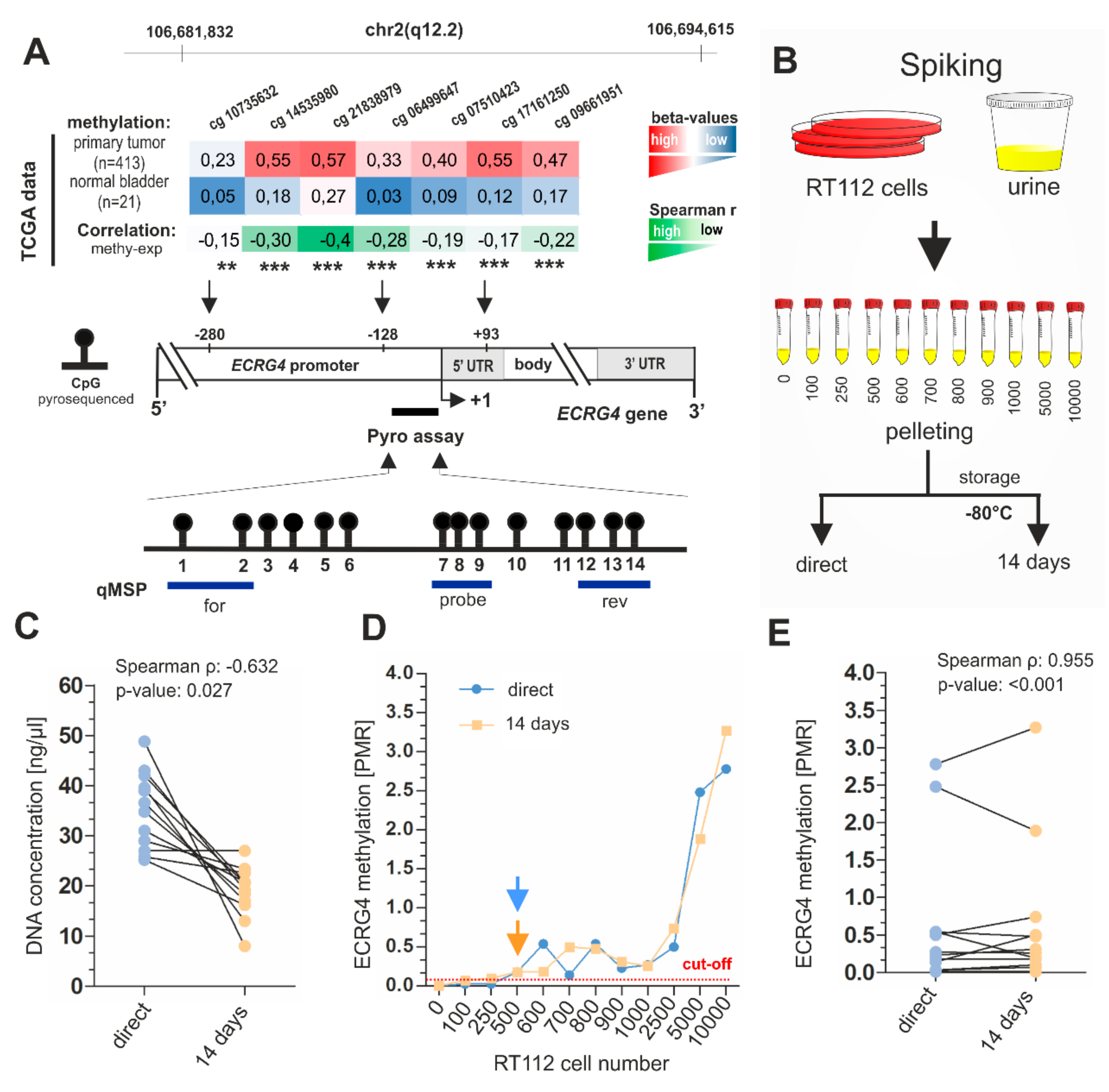
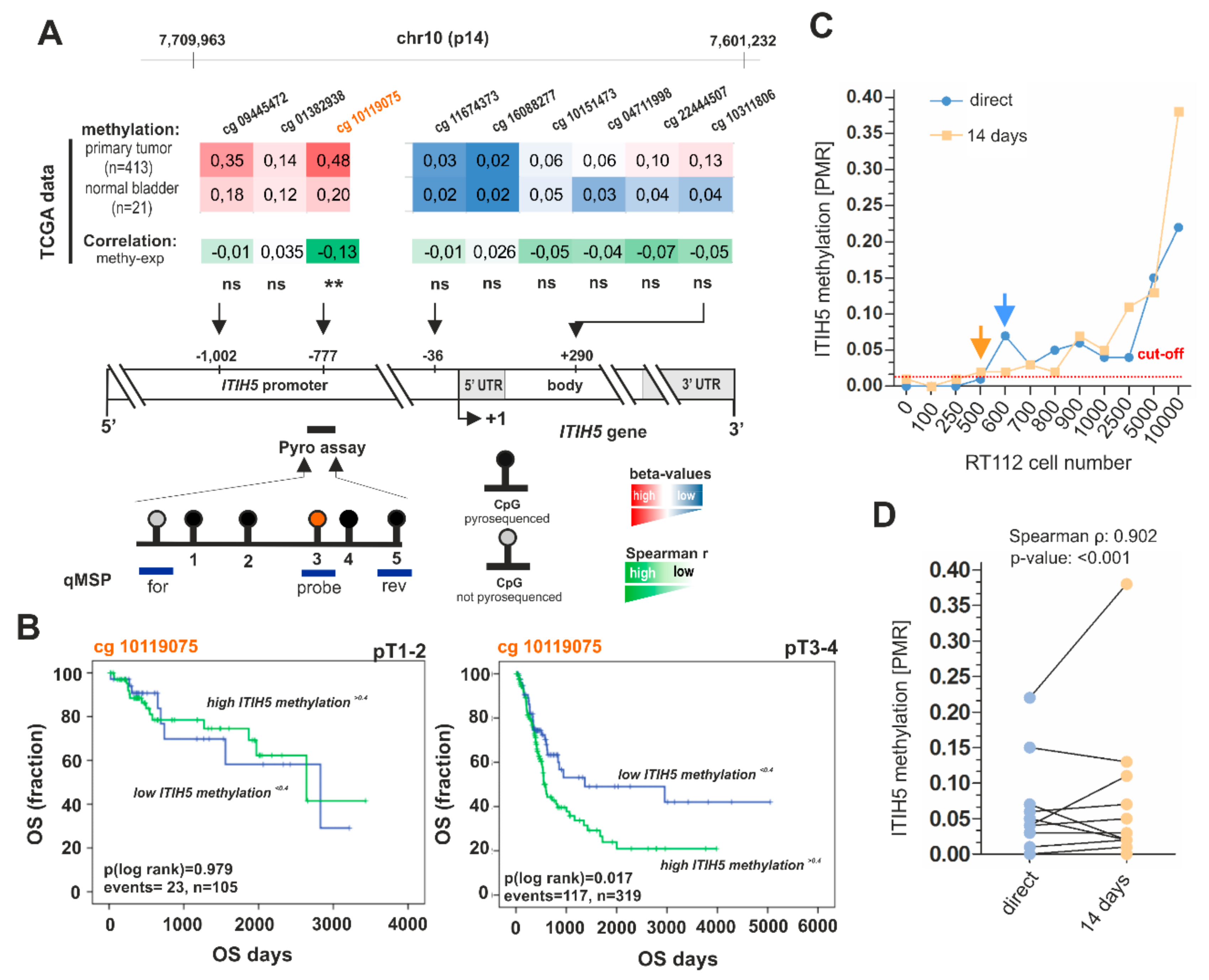
2.1. Analytical Performance of ITIH5 and ECRG4 qMSP and Pyrosequencing Biomarker Assays
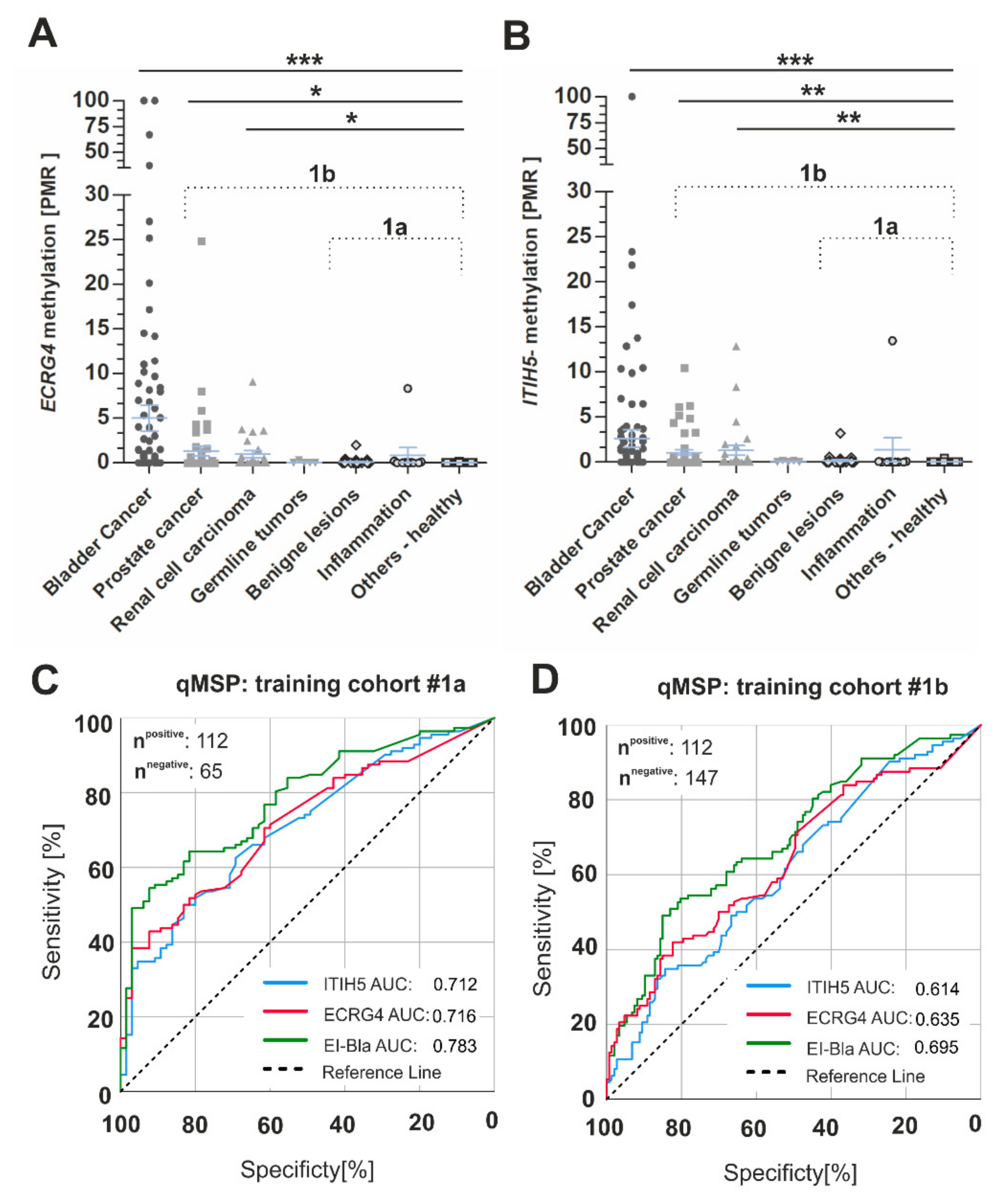
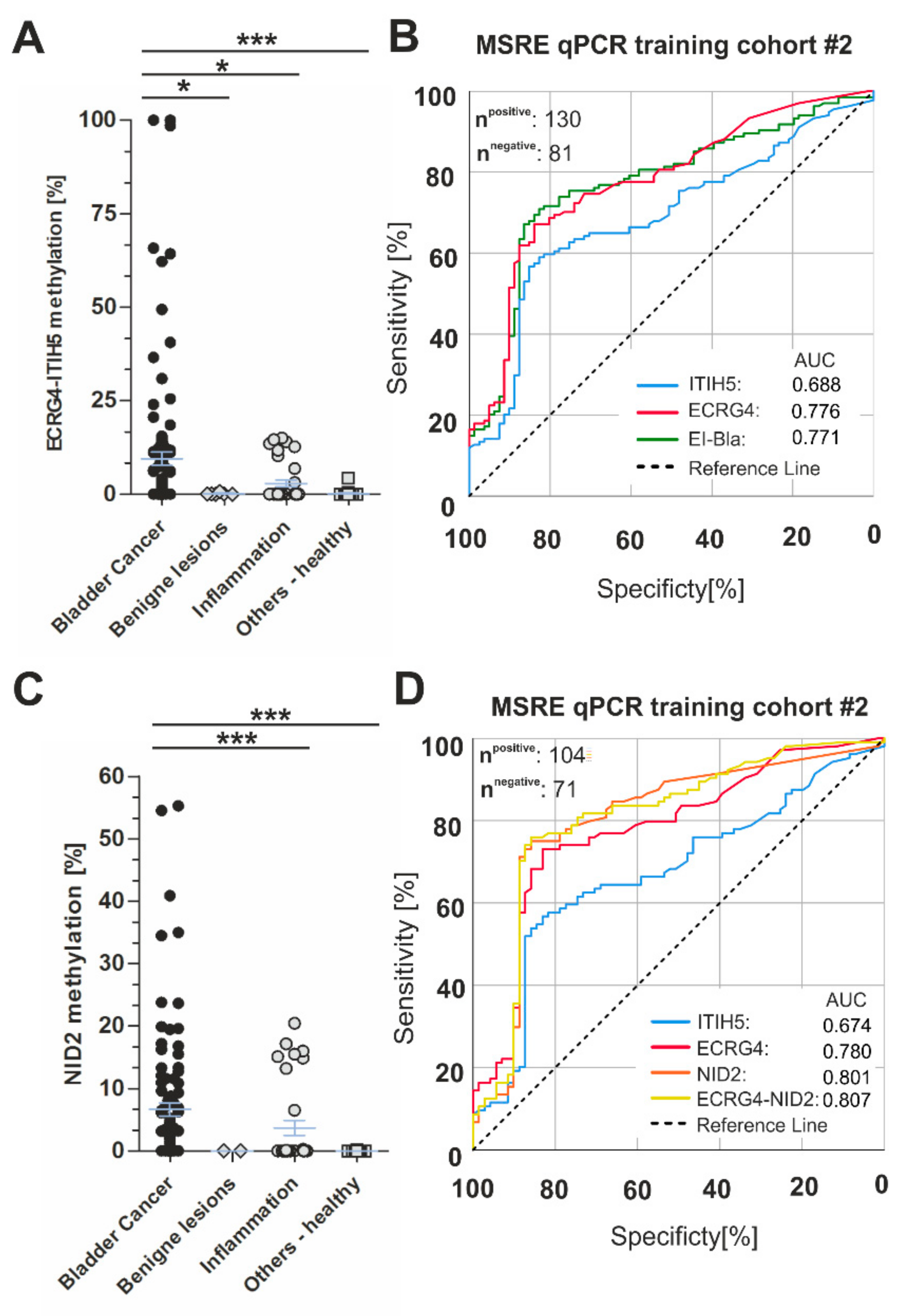
2.2. Clinical Biomarker Performance of the ECRG4-ITIH5 qMSP Test for Accurate Non-Invasive Detection of Bladder Cancer
3. Discussion
4. Materials and Methods
4.1. Cell Line
4.2. Urine Samples
4.3. DNA Extraction from Urines
4.4. DNA Bisulfite Conversion
4.5. Bisulfite-Pyrosequencing
4.6. Quantitative Methylation-Specific PCR (qMSP)
4.7. Methylation Sensitive Restriction Enzyme qPCR (MSRE) qPCR
4.8. Analytical Assay Performances
4.9. TCGA BLCA Data Set
4.10. Statistical Data Acquisition
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Yeung, C.; Dinh, T.; Lee, J. The health economics of bladder cancer: An updated review of the published literature. Pharmacoeconomics 2014, 32, 1093–1104. [Google Scholar] [CrossRef]
- Leal, J.; Luengo-Fernandez, R.; Sullivan, R.; Witjes, J.A. Economic Burden of Bladder Cancer Across the European Union. Eur. Urol. 2016, 69, 438–447. [Google Scholar] [CrossRef] [Green Version]
- Schlake, A.; Crispen, P.L.; Cap, A.P.; Atkinson, T.; Davenport, D.; Preston, D.M. NMP-22, urinary cytology, and cystoscopy: A 1 year comparison study. Can. J. Urol. 2012, 19, 6345–6350. [Google Scholar]
- National Collaborating Centre for Cancer (UK). Bladder Cancer: Diagnosis and Management; National Institute for Health and Care Excellence: London, UK, 2015. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK305022/ (accessed on 5 February 2020).
- Sarosdy, M.F.; Kahn, P.R.; Ziffer, M.D.; Love, W.R.; Barkin, J.; Abara, E.O.; Jansz, K.; Bridge, J.A.; Johansson, S.L.; Persons, D.L.; et al. Use of a multitarget fluorescence in situ hybridization assay to diagnose bladder cancer in patients with hematuria. J. Urol. 2006, 176, 44–47. [Google Scholar] [CrossRef]
- Lotan, Y.; Roehrborn, C.G. Sensitivity and specificity of commonly available bladder tumor markers versus cytology: Results of a comprehensive literature review and meta-analyses. Urology 2003, 61, 109–118. [Google Scholar] [CrossRef]
- Bhat, A.; Ritch, C.R. Urinary biomarkers in bladder cancer: Where do we stand? Curr. Opin. Urol. 2019, 29, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L. Multiprobe fluorescence in situ hybridization (UroVysion) for the detection of urothelial carcinoma - FISHing for the right catch. Acta Cytol. 2011, 55, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Behrens, T.; Stenzl, A.; Brüning, T. Factors influencing false-positive results for nuclear matrix protein 22. Eur. Urol. 2014, 66, 970–972. [Google Scholar] [CrossRef]
- Wang, Z.; Que, H.; Suo, C.; Han, Z.; Tao, J.; Huang, Z.; Ju, X.; Tan, R.; Gu, M. Evaluation of the NMP22 BladderChek test for detecting bladder cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 100648–100656. [Google Scholar] [CrossRef]
- Pichler, R.; Fritz, J.; Tulchiner, G.; Klinglmair, G.; Soleiman, A.; Horninger, W.; Klocker, H.; Heidegger, I. Increased accuracy of a novel mRNA-based urine test for bladder cancer surveillance. BJU Int. 2018, 121, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ecke, T.H.; Weiß, S.; Stephan, C.; Hallmann, S.; Arndt, C.; Barski, D.; Otto, T.; Gerullis, H. UBC® Rapid Test-A Urinary Point-of-Care (POC) Assay for Diagnosis of Bladder Cancer with a focus on Non-Muscle Invasive High-Grade Tumors: Results of a Multicenter-Study. Int. J. Mol. Sci. 2018, 19, 3841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baylin, S.B.; Jones, P.A. A decade of exploring the cancer epigenome-biological and translational implications. Nat. Rev. Cancer. 2011, 11, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Molnár, B.; Tóth, K.; Barták, B.K.; Tulassay, Z. Plasma methylated septin 9: A colorectal cancer screening marker. Expert Rev. Mol. Diagn. 2015, 15, 171–184. [Google Scholar] [CrossRef]
- Larsen, L.K.; Lind, G.E.; Guldberg, P.; Dahl, C. DNA-Methylation-Based Detection of Urological Cancer in Urine: Overview of Biomarkers and Considerations on Biomarker Design, Source of DNA, and Detection Technologies. Int. J. Mol. Sci. 2019, 20, 2657. [Google Scholar] [CrossRef] [Green Version]
- Veeck, J.; Chorovicer, M.; Naami, A.; Breuer, E.; Zafrakas, M.; Bektas, N.; Dürst, M.; Kristiansen, G.; Wild, P.J.; Hartmann, A.; et al. The extracellular matrix protein ITIH5 is a novel prognostic marker in invasive node-negative breast cancer and its aberrant expression is caused by promoter hypermethylation. Oncogene 2008, 27, 865–876. [Google Scholar] [CrossRef] [Green Version]
- Kloten, V.; Rose, M.; Kaspar, S.; von Stillfried, S.; Knüchel, R.; Dahl, E. Epigenetic inactivation of the novel candidate tumor suppressor gene ITIH5 in colon cancer predicts unfavorable overall survival in the CpG island methylator phenotype. Epigenetics 2014, 9, 1290–1301. [Google Scholar] [CrossRef] [Green Version]
- Dötsch, M.M.; Kloten, V.; Schlensog, M.; Heide, T.; Braunschweig, T.; Veeck, J.; Petersen, I.; Knüchel, R.; Dahl, E. Low expression of ITIH5 in adenocarcinoma of the lung is associated with unfavorable patients’ outcome. Epigenetics 2015, 10, 903–912. [Google Scholar] [CrossRef] [Green Version]
- Rose, M.; Gaisa, N.T.; Antony, P.; Fiedler, D.; Heidenreich, A.; Otto, W.; Denzinger, S.; Bertz, S.; Hartmann, A.; Karl, A.; et al. Epigenetic inactivation of ITIH5 promotes bladder cancer progression and predicts early relapse of pT1 high-grade urothelial tumours. Carcinogenesis 2014, 35, 727–736. [Google Scholar] [CrossRef] [Green Version]
- Rose, M.; Kloten, V.; Noetzel, E.; Gola, L.; Ehling, J.; Heide, T.; Meurer, S.K.; Gaiko-Shcherbak, A.; Sechi, A.S.; Huth, S.; et al. ITIH5 mediates epigenetic reprogramming of breast cancer cells. Mol. Cancer 2017, 16, 44. [Google Scholar] [CrossRef] [Green Version]
- Rose, M.; Meurer, S.K.; Kloten, V.; Weiskirchen, R.; Denecke, B.; Antonopoulos, W.; Deckert, M.; Knüchel, R.; Dahl, E. ITIH5 induces a shift in TGF-β superfamily signaling involving Endoglin and reduces risk for breast cancer metastasis and tumor death. Mol. Carcinog. 2018, 57, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Kurahara, H.; Young, E.D.; Natsugoe, S.; Ijichi, A.; Iwakuma, T.; Welch, D.R. Genome-wide in vivo RNAi screen identifies ITIH5 as a metastasis suppressor in pancreatic cancer. Clin. Exp. Metastasis 2017, 34, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Yue, C.M.; Deng, D.J.; Bi, M.X.; Guo, L.P.; Lu, S.H. Expression of ECRG4, a novel esophageal cancer-related gene, downregulated by CpG island hypermethylation in human esophageal squamous cell carcinoma. World J. Gastroenterol. 2003, 9, 1174–1178. [Google Scholar] [CrossRef] [PubMed]
- Li, L.W.; Yu, X.Y.; Yang, Y.; Zhang, C.P.; Guo, L.P.; Lu, S.H. Expression of esophageal cancer related gene 4 (ECRG4), a novel tumor suppressor gene, in esophageal cancer and its inhibitory effect on the tumor growth in vitro and in vivo. Int. J. Cancer 2009, 125, 1505–1513. [Google Scholar] [CrossRef]
- Tang, G.Y.; Tang, G.J.; Yin, L.; Chao, C.; Zhou, R.; Ren, G.P.; Chen, J.Y.; Zhang, W. ECRG4 acts as a tumor suppressor gene frequently hypermethylated in human breast cancer. Biosci. Rep. 2019, 39, BSR20190087. [Google Scholar] [CrossRef] [Green Version]
- Luo, L.; Wu, J.; Xie, J.; Xia, L.; Qian, X.; Cai, Z.; Li, Z. Downregulated ECRG4 is associated with poor prognosis in renal cell cancer and is regulated by promoter DNA methylation. Tumour Biol. 2016, 37, 1121–1129. [Google Scholar] [CrossRef]
- Götze, S.; Feldhaus, V.; Traska, T.; Wolter, M.; Reifenberger, G.; Tannapfel, A.; Kuhnen, C.; Martin, D.; Müller, O.; Sievers, S. ECRG4 is a candidate tumor suppressor gene frequently hypermethylated in colorectal carcinoma and glioma. BMC Cancer 2009, 9, 447. [Google Scholar] [CrossRef] [Green Version]
- Cai, Z.; Liang, P.; Xuan, J.; Wan, J.; Guo, H. ECRG4 as a novel tumor suppressor gene inhibits colorectal cancer cell growth in vitro and in vivo. Tumour Biol. 2016, 37, 9111–9120. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Renard, I.; Joniau, S.; van Cleynenbreugel, B.; Collette, C.; Naômé, C.; Vlassenbroeck, I.; Nicolas, H.; de Leval, J.; Straub, J.; Van Criekinge, W.; et al. Identification and validation of the methylated TWIST1 and NID2 genes through real-time methylation-specific polymerase chain reaction assays for the noninvasive detection of primary bladder cancer in urine samples. Eur. Urol. 2010, 58, 96–104. [Google Scholar] [CrossRef]
- Song, L.; Jia, J.; Peng, X.; Xiao, W.; Li, Y. The performance of the SEPT9 gene methylation assay and a comparison with other CRC screening tests: A meta-analysis. Sci. Rep. 2017, 7, 3032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodewijk, I.; Dueñas, M.; Rubio, C.; Munera-Maravilla, E.; Segovia, C.; Bernardini, A.; Teijeira, A.; Paramio, J.M.; Suárez-Cabrera, C. Liquid Biopsy Biomarkers in Bladder Cancer: A Current Need for Patient Diagnosis and Monitoring. Int. J. Mol. Sci. 2018, 19, 2514. [Google Scholar] [CrossRef] [Green Version]
- Costa, V.L.; Henrique, R.; Danielsen, S.A.; Duarte-Pereira, S.; Eknaes, M.; Skotheim, R.I.; Rodrigues, A.; Magalhães, J.S.; Oliveira, J.; Lothe, R.A.; et al. Three epigenetic biomarkers, GDF15, TMEFF2, and VIM, accurately predict bladder cancer from DNA-based analyses of urine samples. Clin. Cancer Res. 2010, 16, 5842–5851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Heijden, A.G.; Mengual, L.; Ingelmo-Torres, M.; Lozano, J.J.; van Rijt-van de Westerlo, C.C.M.; Baixauli, M.; Geavlete, B.; Moldoveanud, C.; Ene, C.; Dinney, C.P.; et al. Urine cell-based DNA methylation classifier for monitoring bladder cancer. Clin. Epigenetics 2018, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Hernández, H.G.; Tse, M.Y.; Pang, S.C.; Arboleda, H.; Forero, D.A. Optimizing methodologies for PCR-based DNA methylation analysis. Biotechniques 2013, 55, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Feber, A.; Dhami, P.; Dong, L.; de Winter, P.; Tan, W.S.; Martínez-Fernández, M.; Paul, D.S.; Hynes-Allen, A.; Rezaee, S.; Gurung, P.; et al. UroMark-a urinary biomarker assay for the detection of bladder cancer. Clin. Epigenetics 2017, 9, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloten, V.; Becker, B.; Winner, K.; Schrauder, M.G.; Fasching, P.A.; Anzeneder, T.; Veeck, J.; Hartmann, A.; Knüchel, R.; Dahl, E. Promoter hypermethylation of the tumor-suppressor genes ITIH5, DKK3, and RASSF1A as novel biomarkers for blood-based breast cancer screening. Breast Cancer Res. 2013, 15, R4. [Google Scholar] [CrossRef] [Green Version]
- Shahin, O.; Thalmann, G.N.; Rentsch, C.; Mazzucchelli, L.; Studer, U.E. A retrospective analysis of 153 patients treated with or without intravesical bacillus Calmette-Guerin for primary stage T1 grade 3 bladder cancer: Recurrence, progression and survival. J. Urol. 2003, 169, 96–100. [Google Scholar] [CrossRef]
- Witjes, J.A.; Morote, J.; Cornel, E.B.; Gakis, G.; van Valenberg, F.J.P.; Lozano, F.; Sternberg, I.A.; Willemsen, E.; Hegemann, M.L.; Paitan, Y.; et al. Performance of the Bladder EpiCheck™ Methylation Test for Patients Under Surveillance for Non-muscle-invasive Bladder Cancer: Results of a Multicenter, Prospective, Blinded Clinical Trial. Eur. Urol. Oncol. 2018, 1, 307–313. [Google Scholar] [CrossRef]
- Pfaffl, M.W. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001, 29, e45. [Google Scholar] [CrossRef]
- Ralser, M.; Querfurth, R.; Warnatz, H.J.; Lehrach, H.; Yaspo, M.L.; Krobitsch, S. An efficient and economic enhancer mix for PCR. Biochem. Biophys. Res. Commun. 2006, 347, 747–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mijnes, J.; Veeck, J.; Gaisa, N.T.; Burghardt, E.; de Ruijter, T.C.; Gostek, S.; Dahl, E.; Pfister, D.; Schmid, S.C.; Knüchel, R.; et al. Promoter methylation of DNA damage repair (DDR) genes in human tumor entities: RBBP8/CtIP is almost exclusively methylated in bladder cancer. Clin. Epigenetics 2018, 10, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EI-BLA qMSP | |||||
|---|---|---|---|---|---|
| Cut-Off | Specificity | Sensitivity | AUC | p-Value | Control Group |
| 0.54 | 81.5% | 64.3% | 0.783 | <0.001 | 1a |
| 0.38 | 81.6% | 50.9% | 0.695 | <0.001 | 1b |
| ITIH5 Methylation b | |||||
|---|---|---|---|---|---|
| na | Low | High | p-Value c | ||
| Age at diagnosis | |||||
| ≤70 years | 111 | 65 | 46 | 0.001 | |
| >70 years | 106 | 39 | 67 | ||
| Gender | |||||
| male | 143 | 57 | 56 | 0.150 | |
| female | 42 | 22 | 20 | ||
| Histological tumor grade d | |||||
| low grade | 19 | 4 | 15 | 0.174 | |
| high grade | 113 | 42 | 71 | ||
| Tumor stage d | |||||
| pTa | 76 | 33 | 43 | 0.024 | |
| pT1-pT4 | 54 | 13 | 41 | ||
| ECRG4 Methylation b | |||||
|---|---|---|---|---|---|
| na | Low | High | p-Value c | ||
| Age at diagnosis | |||||
| <70 years | 111 | 84 | 27 | <0.001 | |
| ≥70 years | 106 | 55 | 51 | ||
| Gender | |||||
| male | 143 | 82 | 61 | 0.802 | |
| female | 42 | 25 | 17 | ||
| Histological tumor grade d | |||||
| low grade | 19 | 10 | 9 | 0.645 | |
| high grade | 113 | 53 | 60 | ||
| Tumor staged | |||||
| pTa | 76 | 45 | 31 | 0.007 | |
| pT1-pT4 | 54 | 19 | 35 | ||
| EI-BLA MRSE qPCR | |||||
| Cut-Off | Specificity | Sensitivity | AUC | p-Value | Control Group |
| 0.52 | 80.2% | 71.6% | 0.771 | <0.001 | all |
| 0.53 | 91.9% | 69.2% | 0.850 | <0.001 | healthy |
| Single markers MSRE qPCR (control group “all”) | |||||
| Cut-Off | Specificity | Sensitivity | AUC | p-Value | Marker |
| 0.94 | 83.1% | 73.1% | 0.780 | <0.001 | ECRG4 |
| 0.77 | 83.1% | 56.7% | 0.674 | <0.001 | ITIH5 |
| 0.11 | 83.1% | 75.0% | 0.801 | <0.001 | NID2 |
| Combined ECRG4-NID2 MSRE qPCR | |||||
| Cut-Off | Specificity | Sensitivity | AUC | p-Value | Control Group |
| 0.49 | 85.9% | 75.0% | 0.807 | <0.001 | all |
| 0.49 | 97.3% | 76.0% | 0.884 | <0.001 | healthy |
| Categorization | n | % Analyzable | |
|---|---|---|---|
| Controls | 228 | 100% | |
| Age (median 61.0; range: 23–82 years) | |||
| <61.0 years | 72 | 31.6% | |
| ≥61.0 years | 80 | 35.1% | |
| na | 76 | 33.3% | |
| Gender | |||
| male | 96 | 42.1% | |
| female | 24 | 10.5% | |
| na | 108 | 47.4% | |
| Diagnosis | |||
| Healthy | 49 | 21.5% | |
| Uro-stones | 13 | 5.7% | |
| Inflammatory—Uro-cystitis | 38 | 16.7% | |
| Inflammatory—other | 8 | 3.5% | |
| Benign—BPH | 23 | 10.1% | |
| Benign—other | 17 | 7.5% | |
| PCa | 48 | 21.1% | |
| GTR | 5 | 2.2% | |
| RCC | 27 | 11.8% | |
| BCa-Asscociated a | 246 | 100% | |
| Age (median 70; range: 27–89 years) | |||
| <70 years | 119 | 48.4% | |
| ≥70 years | 127 | 51.6% | |
| Gender | |||
| male | 195 | 79.3% | |
| female | 51 | 20.7% | |
| Histological tumor grade b | |||
| low grade | 42 | 17.1% | |
| high grade | 172 | 69.9% | |
| na | 32 | 13.0% | |
| Tumor stage b | |||
| pTa | 106 | 43.1% | |
| pTis | 8 | 3.3% | |
| pT1 | 54 | 22.0% | |
| pT2 | 37 | 15.0% | |
| pT3 | 19 | 7.7% | |
| pT4 | 8 | 3.3% | |
| pTx | 8 | 3.3% | |
| na | 6 | 2.4% | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rose, M.; Bringezu, S.; Godfrey, L.; Fiedler, D.; Gaisa, N.T.; Koch, M.; Bach, C.; Füssel, S.; Herr, A.; Hübner, D.; et al. ITIH5 and ECRG4 DNA Methylation Biomarker Test (EI-BLA) for Urine-Based Non-Invasive Detection of Bladder Cancer. Int. J. Mol. Sci. 2020, 21, 1117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031117
Rose M, Bringezu S, Godfrey L, Fiedler D, Gaisa NT, Koch M, Bach C, Füssel S, Herr A, Hübner D, et al. ITIH5 and ECRG4 DNA Methylation Biomarker Test (EI-BLA) for Urine-Based Non-Invasive Detection of Bladder Cancer. International Journal of Molecular Sciences. 2020; 21(3):1117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031117
Chicago/Turabian StyleRose, Michael, Sarah Bringezu, Laura Godfrey, David Fiedler, Nadine T. Gaisa, Maximilian Koch, Christian Bach, Susanne Füssel, Alexander Herr, Doreen Hübner, and et al. 2020. "ITIH5 and ECRG4 DNA Methylation Biomarker Test (EI-BLA) for Urine-Based Non-Invasive Detection of Bladder Cancer" International Journal of Molecular Sciences 21, no. 3: 1117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21031117