Circulating tRNA Fragments as a Novel Biomarker Class to Distinguish Acute Stroke Subtypes

 ,
,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
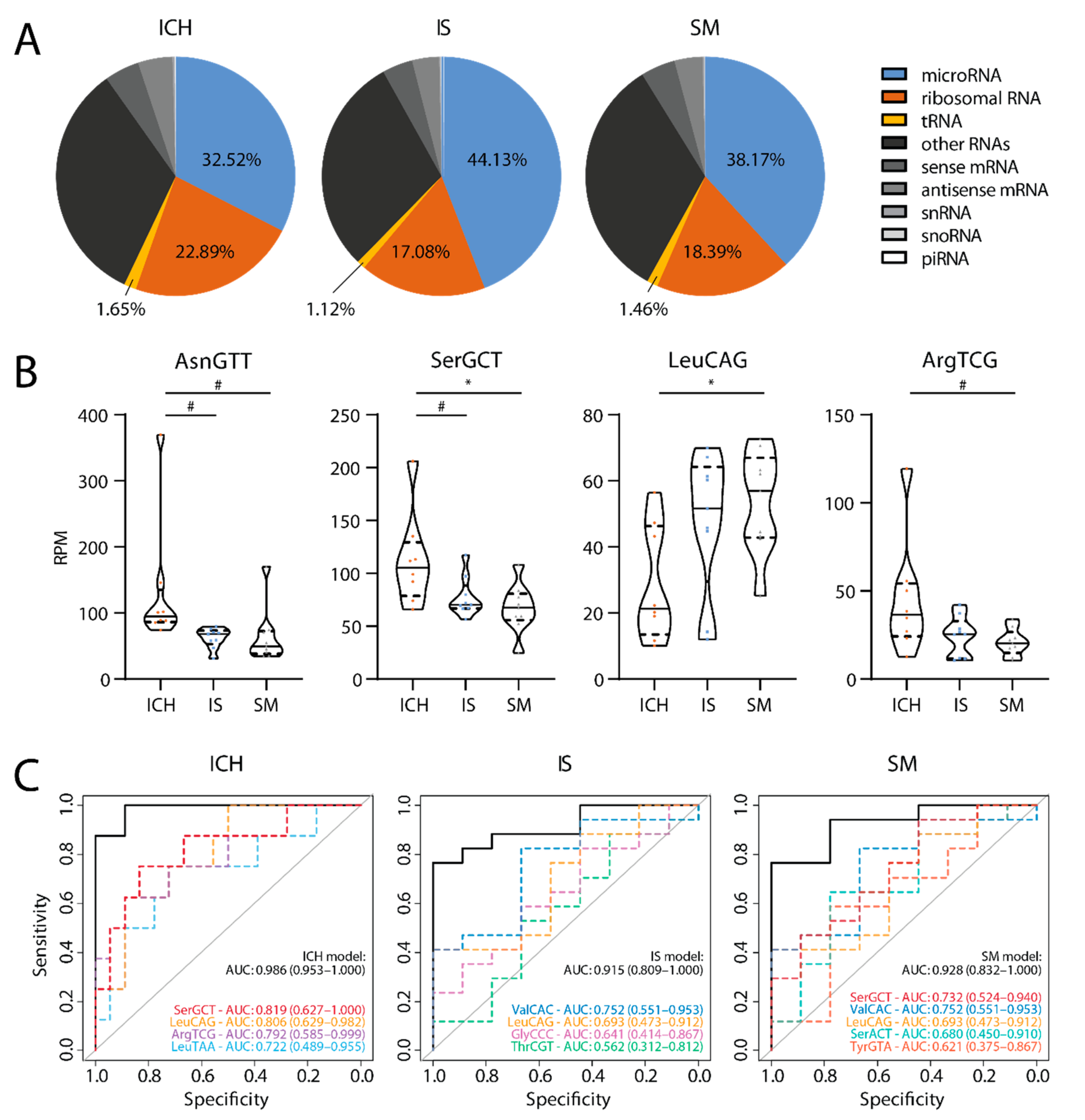
2.2. Small RNAs in Plasma
2.3. tRFs as Biomarkers
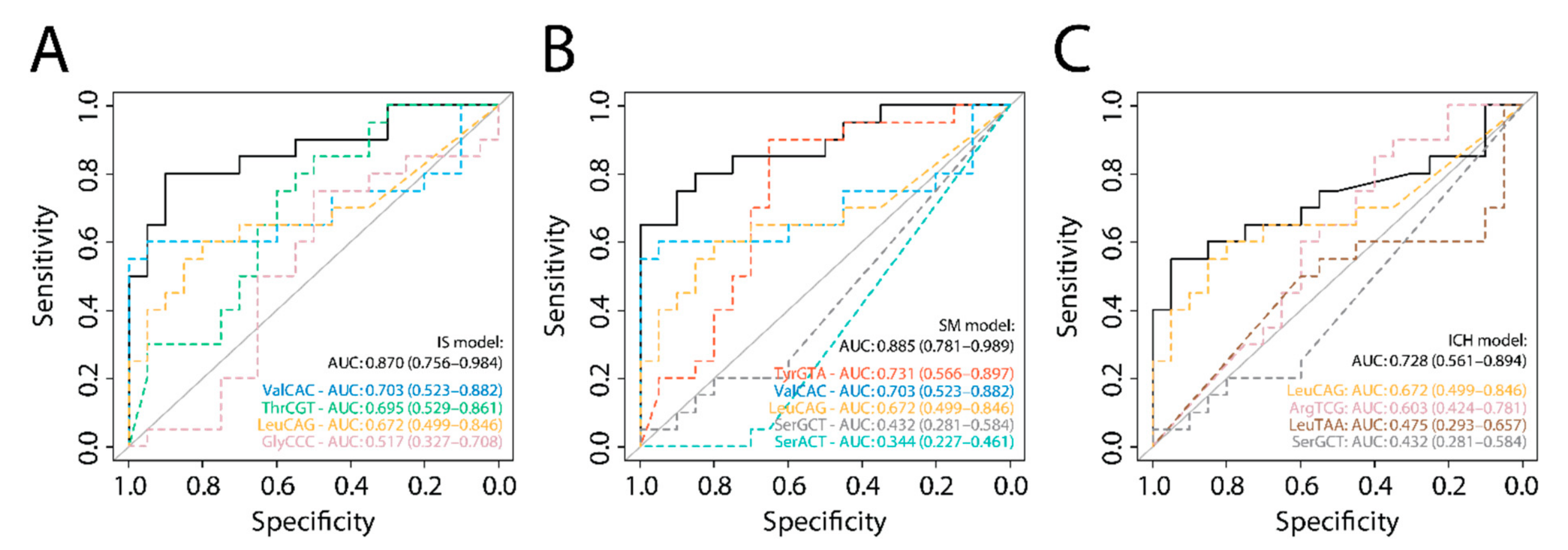
2.4. Validation of tRF Models
2.5. Common tRF Model
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patient Selection
4.3. Clinical Data
4.4. Sample Collection
4.5. Ultracentrifugation and RNA-Sequencing
4.6. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gioia, L.C.; Zewude, R.T.; Kate, M.P.; Liss, K.; Rowe, B.H.; Buck, B.; Jeerakathil, T.; Butcher, K. Prehospital systolic blood pressure is higher in acute stroke compared with stroke mimics. Neurology 2016, 86, 2146–2153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Tiedt, S.; Dichgans, M. Role of non-coding RNAs in Stroke. Stroke 2018, 49, 3098–3106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.; Tan, W.; Zhou, Y. Transfer RNA-derived small RNAs: Potential applications as novel biomarkers for disease diagnosis and prognosis. Ann. Transl. Med. 2020, 8, 1092. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xu, Z.; Sheng, J. tRNA-Derived small RNA: A novel regulatory small non-coding RNA. Genes 2018, 9, 246. [Google Scholar] [CrossRef] [Green Version]
- Dhahbi, J.M.; Spindler, S.R.; Atamna, H.; Boffelli, D.; Martin, D.I.K. Deep sequencing of serum small RNAs identifies patterns of 5’ tRNA half and YRNA fragment expression associated with breast cancer. Biomark. Cancer 2014, 6, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Hogg, M.C.; Raoof, R.; El Naggar, H.; Monsefi, N.; Delanty, N.; O’Brien, D.F.; Bauer, S.; Rosenow, F.; Henshall, D.C.; Prehn, J.H.M. Elevation in plasma tRNA fragments precede seizures in human epilepsy. J. Clin. Investig. 2019, 129, 2946–2951. [Google Scholar] [CrossRef] [Green Version]
- Tiedt, S.; Prestel, M.; Malik, R.; Schieferdecker, N.; Duering, M.; Kautzky, V.; Stoycheva, I.; Böck, J.; Northoff, B.H.; Klein, M.; et al. RNA-Seq identifies circulating miR-125a-5p, miR-125b-5p, and miR-143-3p as potential biomarkers for acute Ischemic Stroke. Circ. Res. 2017, 121, 970–980. [Google Scholar] [CrossRef]
- Li, Q.; Hu, B.; Hu, G.W.; Niu, X.; Liu, J.; Zhou, S.-m.; Zhang, C.-q.; Wang, Y.; Deng, Z.-F. tRNA-derived small non-coding RNAs in response to ischemia inhibit angiogenesis. Sci. Rep. 2016, 6, 20850. [Google Scholar] [CrossRef] [Green Version]
- Elkordy, A.; Rashad, S.; Shehabeldeen, H.; Mishima, E.; Niizuma, K.; Abe, T.; Tominaga, T. tiRNAs as a novel biomarker for cell damage assessment in in vitro ischemia-reperfusion model in rat neuronal PC12 cells. Brain Res. 2019, 1714, 8–17. [Google Scholar] [CrossRef]
- Sato, K.; Rashad, S.; Niizuma, K.; Tominaga, T. Stress induced tRNA halves (tiRNAs) as biomarkers for stroke and stroke therapy; pre-clinical study. Neuroscience 2020, 434, 44–54. [Google Scholar] [CrossRef] [PubMed]
- McArdle, H.; Hogg, M.C.; Bauer, S.; Rosenow, F.; Prehn, J.H.M.; Adamson, K.; Henshall, D.C.; Spain, E. Quantification of tRNA fragments by electrochemical direct detection in small volume biofluid samples. Sci. Rep. 2020, 10, 7516. [Google Scholar] [CrossRef]
- Besson, G.; Robert, C.; Hommel, M.; Perret, J. Is it clinically possible to distinguish nonhemorrhagic infarct from hemorrhagic stroke? Stroke 1995, 26, 1205–1209. [Google Scholar] [CrossRef]
- Ishida, T.; Inoue, T.; Niizuma, K.; Konno, N.; Suzuki, C.; Inoue, T.; Ezura, M.; Uenohara, H.; Abe, T.; Tominaga, T. Prediction of functional outcome in patients with acute stroke by measuring tRNA derivatives. Cerebrovasc. Dis. 2020, 49, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Li, P.-F.; Liu, S.-C.G.T.; Cui, H. Integrative analysis of transcriptomes highlights potential functions of transfer-RNA-derived small RNAs in experimental intracerebral hemorrhage. Aging 2020, 12, 22794–22813. [Google Scholar] [CrossRef] [PubMed]
- Burch, P.M.; Glaab, W.E.; Holder, D.J.; Phillips, J.A.; Sauer, J.-M.; Walker, E.G. Net reclassification index and integrated discrimination index are not appropriate for testing whether a biomarker improves predictive performance. Toxicol. Sci. 2017, 156, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American heart association/American stroke association. Stroke 2018, 49, 46–110. [Google Scholar] [CrossRef]
- Williams, L.S.; Yilmza, E.Y.; Lopez-Yunez, A.M. Retrospective assessment of initial stroke severity with the NIH stroke scale. Stroke 2000, 31, 858–862. [Google Scholar] [CrossRef] [Green Version]
- Coumans, F.A.W.; Brisson, A.R.; Buzas, E.I.; Dignat-George, F.; Drees, E.E.E.; Samir El-Andaloussi, S.; Emanueli, C.; Gasecka, A.; Hendrix, A.; Hill, A.F. Methodological guidelines to study extracellular vesicles. Circ. Res. 2017, 120, 1632–1648. [Google Scholar] [CrossRef] [PubMed]
- Appierto, V.; Callari, M.; Cavadini, E.; Morelli, D.; Daidone, M.G.; Tiberio, P. A lipemia-independent NanoDrop-based score to identify hemolysis in plasma and serum samples. Bioanalysis 2014, 6, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Blondal, T.; Jensby Nielsen, J.S.; Baker, A.; Andreasen, D.; Mouritzen, P.; Teilum, M.W.; Dahlsveen, I.K. Assessing sample and miRNA profile quality in serum and plasma or other biofluids. Methods 2013, 59, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Andrews, S. FastQC: A Quality Control Tool for High Throughput Sequence Data. 2010. Available online: http://www.bioinformatics.babraham.ac.uk/projects/fastqc/ (accessed on 24 November 2020).
- Aparicio-Puerta, E.; Lebron, R.; Rueda, A.; Gómez-Martín, C.; Giannoukakos, S.; Jaspez, D.; Medina, J.M.; Zubkovic, A.; Jurak, I.; Fromm, B.; et al. sRNAbench and sRNAtoolbox 2019: Intuitive fast small RNA profiling and differential expression. Nucleic. Acids Res. 2019, 47, 530–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 24 November 2020).
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total No. Patients (n = 26) | Ischemic Stroke (n = 9) | Intracerebral Hemorrhage * (n = 8) | Stroke Mimics † (n = 9) | p Value | |
|---|---|---|---|---|---|
| Age, mean (SD), y | 71 (14) | 76 (8) | 71 (14) | 65 (16) | 0.25 |
| Male sex, n (%) | 15 (58) | 6 (67) | 3 (38) | 6 (67) | 0.43 |
| Medical history, n (%) | |||||
| Ischemic stroke/TIA | 8 (31) | 3 (33) | 3 (38) | 2 (22) | 0.87 |
| Intracerebral hemorrhage | 2 (8) | 0 (0) | 2 (25) | 0 (0) | 0.09 |
| Atrial fibrillation | 5 (19) | 1 (11) | 2 (25) | 2 (22) | 0.84 |
| Diabetes Mellitus | 5 (19) | 1 (11) | 4 (50) | 0 (0) | 0.02 |
| Hyperlipidemia | 12 (46) | 6 (67) | 3 (38) | 3 (33) | 0.38 |
| Hypertension | 15 (58) | 6 (67) | 7 (89) | 2 (22) | 0.02 |
| Medication use, n (%) | |||||
| Oral anticoagulation | 5 (19) | 1 (11) | 3 (38) | 1 (11) | 0.38 |
| Antiplatelets | 8 (31) | 3 (33) | 2 (25) | 3 (33) | 1.00 |
| Hospital admission | |||||
| ODT, median (IQR), min | 78 (57–116) | 72 (45–144) | 95 (63–203) | 68 (60–102) | 0.76 |
| NIHSS ‡, median (IQR) | 8 (4–18) | 5 (4–19) | 11 (6–18) | - | |
| LAVO §, n (%) | 4 (44) | - | - | - | |
| Neuro-imaging || | |||||
| Lesion confirmed, n (%) | 8 (89) | 8 (100) | - | ||
| Reperfusion therapy | |||||
| IVT, n (%) | - | 7 (78 | - | - | - |
| EVT, n (%) | - | 4 (44) | - | - | - |
| DNT, median (IQR), min | - | 20 (17–40) | - | - | - |
| DGT, median (IQR), min | - | 56 (51–65) | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.M.; van der Bent, M.L.; Wermer, M.J.H.; van den Wijngaard, I.R.; van Zwet, E.W.; de Groot, B.; Quax, P.H.A.; Kruyt, N.D.; Nossent, A.Y. Circulating tRNA Fragments as a Novel Biomarker Class to Distinguish Acute Stroke Subtypes. Int. J. Mol. Sci. 2021, 22, 135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010135
Nguyen TTM, van der Bent ML, Wermer MJH, van den Wijngaard IR, van Zwet EW, de Groot B, Quax PHA, Kruyt ND, Nossent AY. Circulating tRNA Fragments as a Novel Biomarker Class to Distinguish Acute Stroke Subtypes. International Journal of Molecular Sciences. 2021; 22(1):135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010135
Chicago/Turabian StyleNguyen, T. Truc My, M. Leontien van der Bent, Marieke J. H. Wermer, Ido R. van den Wijngaard, Erik W. van Zwet, Bas de Groot, Paul H. A. Quax, Nyika D. Kruyt, and Anne Yaël Nossent. 2021. "Circulating tRNA Fragments as a Novel Biomarker Class to Distinguish Acute Stroke Subtypes" International Journal of Molecular Sciences 22, no. 1: 135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010135