Temporomandibular Joint Osteoarthritis: Regenerative Treatment by a Stem Cell Containing Advanced Therapy Medicinal Product (ATMP)—An In Vivo Animal Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
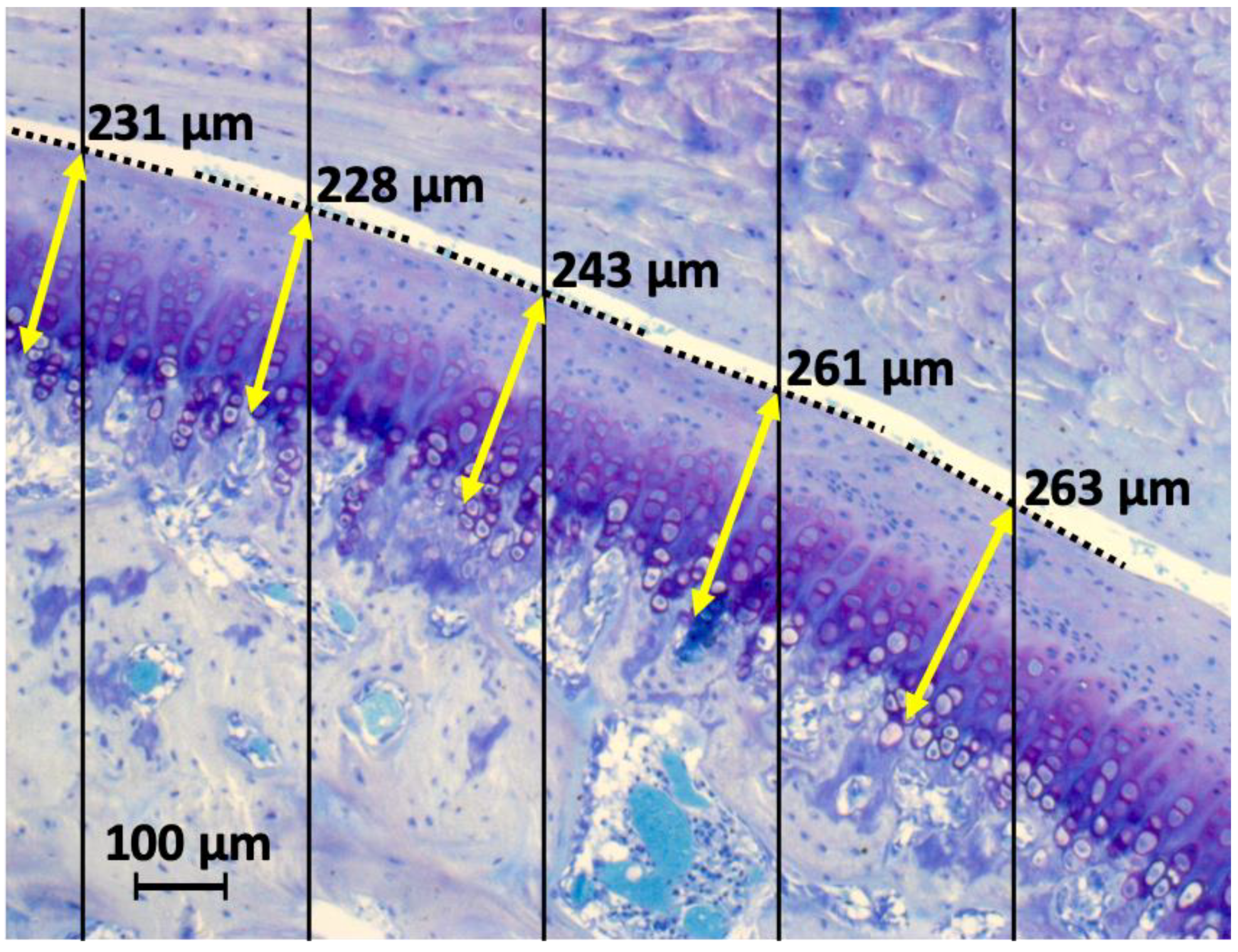
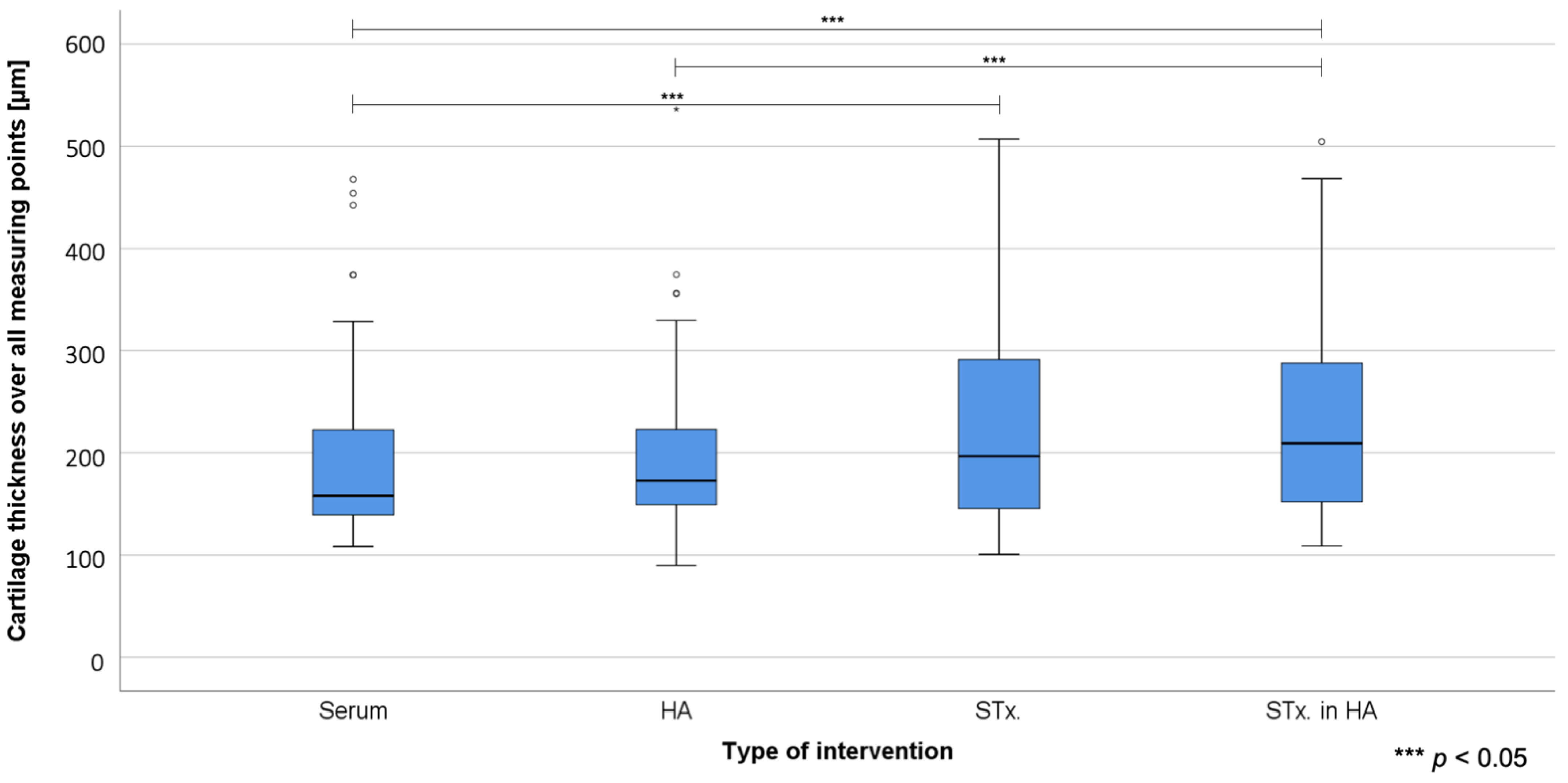
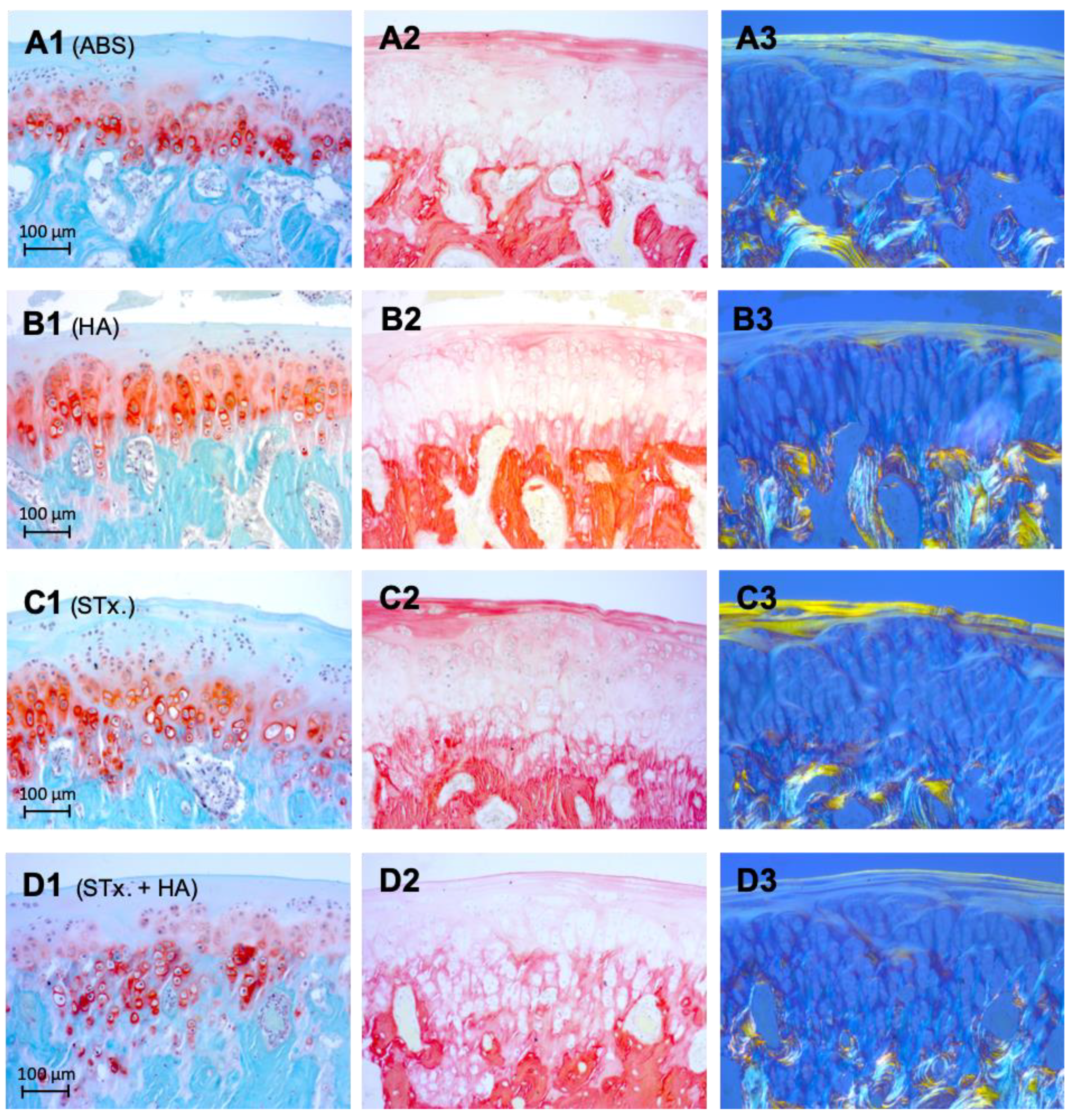
2.1. Histological Analysis and Cartilage Thickness Measurement
2.2. Back-Scattered Electron Imaging (BEI)
3. Discussion
4. Materials and Methods
4.1. Animals—General Information/Anesthesia and Surgery
4.2. Harvesting, Processing and Characterization of Stromal Cells (Preliminary Work)
4.2.1. SVF Isolation and Short-Term Incubation
4.2.2. Immunophenotypic Characterization of Short-Term Incubated Cells (Oxacells HP) In Vitro
4.2.3. Multilineage Differentiation of Short-Term Incubated Cells (Oxacells HP) In Vitro
4.3. Histological Analysis
4.4. Scanning Electron Microscopy
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ATMP | Advanced therapy medicinal product |
| TMJ-OA | Temporomandibular joint osteoarthritis |
| TMJ | Temporomandibular joint |
| TMD | Temporomandibular disorder |
| ABS | Treatment group 1: AB Serum |
| HA | Treatment group 2: Hyaluronic acid |
| STx. | Treatment group 3: Mesenchymal stromal cells (Oxacells HP) |
| HA + STx. | Treatment group 4: Hyaluronic acid + Mesenchymal stromal cells (Oxacells HP) |
| TMJD | Temporomandibular joint disorders |
| RDC | Research Diagnostic Criteria |
| TENS | Transcutaneous electrical nerve stimulation |
| NSAID | Non-steroidal anti-inflammatory drugs |
| PRP | Platelet Rich Plasma |
| MSC | Mesenchymal stromal cells |
| ESC | Embryonic stromal cells |
| ISCT | International Society for Cellular Therapy |
| ASC | Adipose-derived stromal cells |
| SVF | Stromal vascular fraction |
| BEI | Back-scattered electron imaging |
| AC | Articular cartilage |
| SMZ | Subchondral mineralized zone |
| GAG | Glycosaminoglycans |
| ADSC | Adipose tissue-derived stromal cells |
| PDLSC | Periodontal ligament stromal cells |
| SCAP | Stromal cells from apical papilla |
| DFPC | Dental follicle progenitor cells |
| DPSC | Dental pulp stromal cells |
| MPC | Mesenchymal progenitor cells |
| hMSC | Human mesenchymal stromal cells |
| ACLT | Anterior cruciate ligament transaction |
| PBS | Phosphate-buffered saline |
| PMMA | Polymethylmethacrylate |
References
- Gopal, K.; Shankar, R.; Vardhan, H. Prevalence of temporo‑mandibular joint disorders in symptomatic and asymptomatic patients: A cross‑sectional study. Int. J. Adv. Sci. 2014, 1, 14–20. [Google Scholar]
- Milam, S. Pathophysiology and epidemiology of TMJ. J. Musculoskelet. Neuronal Interact. 2003, 3, 382–390. [Google Scholar] [PubMed]
- Su, N.; Liu, Y.; Yang, X.; Shen, J.; Wang, H. Association of malocclusion, self-reported bruxism and chewing-side preference with oral health-related quality of life in patients with temporomandibular joint osteoarthritis. Int. Dent. J. 2018, 68, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, S.; LeResche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. 1992, 6, 301–355. [Google Scholar] [PubMed]
- Wang, X.D.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current Understanding of Pathogenesis and Treatment of TMJ Osteoarthritis. J. Dent. Res. 2015, 94, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Alqutaibi, A.; Aboalrejal, A. Types of occlusal splint in management of temporomandibular disorders (TMD). J. Arthritis 2015, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Ok, S.-M.; Lee, J.; Kim, Y.-I.; Lee, J.-Y.; Kim, K.B.; Jeong, S.-H. Anterior condylar remodeling observed in stabilization splint therapy for temporomandibular joint osteoarthritis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Nicolakis, P.; Erdogmus, C.B.; Kollmitzer, J.; Kerschan-Schindl, K.; Sengstbratl, M.; Nuhr, M.; Crevenna, R.; Fialka-Moser, V. Long-term outcome after treatment of temporomandibular joint osteoarthritis with exercise and manual therapy. Cranio 2002, 20, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Treacy, K. Awareness/relaxation training and transcutaneous electrical neural stimulation in the treatment of bruxism. J. Oral Rehabil. 1999, 26, 280–287. [Google Scholar] [CrossRef]
- Cairns, B.E. Pathophysiology of TMD pain–basic mechanisms and their implications for pharmacotherapy. J. Oral Rehabil. 2010, 37, 391–410. [Google Scholar] [CrossRef]
- Hersh, E.V.; Balasubramaniam, R.; Pinto, A. Pharmacologic management of temporomandibular disorders. Oral Maxillofac. Surg. Clin. N. Am. 2008, 20, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Guarda-Nardini, L.; Stifano, M.; Brombin, C.; Salmaso, L.; Manfredini, D. A one-year case series of arthrocentesis with hyaluronic acid injections for temporomandibular joint osteoarthritis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2007, 103, e14–e22. [Google Scholar] [CrossRef] [PubMed]
- Hegab, A.F.; Ali, H.E.; Elmasry, M.; Khallaf, M.G. Platelet-rich plasma injection as an effective treatment for temporomandibular joint osteoarthritis. J. Oral Maxillofac. Surg. 2015, 73, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Bonnini, S.; Arboretti, R.; Guarda-Nardini, L. Temporomandibular joint osteoarthritis: An open label trial of 76 patients treated with arthrocentesis plus hyaluronic acid injections. Int. J. Oral Maxillofac. Surg. 2009, 38, 827–834. [Google Scholar] [CrossRef]
- Rigon, M.; Pereira, L.M.; Bortoluzzi, M.C.; Loguercio, A.D.; Ramos, A.L.; Cardoso, J.R. Arthroscopy for temporomandibular disorders. Cochrane Database Syst. Rev. 2011, 11, CD006385. [Google Scholar]
- Thambar, S.; Kulkarni, S.; Armstrong, S.; Nikolarakos, D. Botulinum toxin in the management of temporomandibular disorders: A systematic review. Br. J. Oral Maxillofac. Surg. 2020, 58, 508–519. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Manfredini, D.; Ferronato, G. Temporomandibular joint total replacement prosthesis: Current knowledge and considerations for the future. Int. J. Oral Maxillofac. Surg. 2008, 37, 103–110. [Google Scholar] [CrossRef]
- Van Bellinghen, X.; Idoux-Gillet, Y.; Pugliano, M.; Strub, M.; Bornert, F.; Clauss, F.; Schwinté, P.; Keller, L.; Benkirane-Jessel, N.; Kuchler-Bopp, S. Temporomandibular joint regenerative medicine. Int. J. Mol. Sci. 2018, 19, 446. [Google Scholar] [CrossRef] [Green Version]
- Friedenstein, A.J.; Petrakova, K.V.; Kurolesova, A.I.; Frolova, G.P. Heterotopic transplants of bone marrow. Transplantation 1968, 6, 230–247. [Google Scholar] [CrossRef]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Gong, Z.; Li, J.; Meng, Q.; Fang, W.; Long, X. The pilot study of fibrin with temporomandibular joint derived synovial stem cells in repairing TMJ disc perforation. BioMed Res. Int. 2014, 2014, 454021. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Squillaro, T.; Peluso, G.; Galderisi, U. Clinical trials with mesenchymal stem cells: An update. Cell Transplant. 2016, 25, 829–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, J.K.; Wulur, I.; Alfonso, Z.; Hedrick, M.H. Fat tissue: An underappreciated source of stem cells for biotechnology. Trends Biotechnol. 2006, 24, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Born, S.; Dörfel, M.J.; Hartjen, P.; Yekani, S.A.H.; Luecke, J.; Meutsch, J.K.; Westphal, J.K.; Birkelbach, M.; Köhnke, R.; Smeets, R. A short-term plastic adherence incubation of the stromal vascular fraction leads to a predictable GMP-compliant cell-product. Bioimpacts 2019, 9, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, C.; Hawthorn, R.; Harris, R. Anatomy and histology of the human temporomandibular joint. Monogr. Oral Sci. 1975, 4, 1–26. [Google Scholar]
- Delatte, M.; Von den Hoff, J.W.; Van Rheden, R.E.; Kuijpers-Jagtman, A.M. Primary and secondary cartilages of the neonatal rat: The femoral head and the mandibular condyle. Eur. J. Oral Sci. 2004, 112, 156–162. [Google Scholar] [CrossRef]
- Detamore, M.S.; Hegde, J.N.; Wagle, R.R.; Almarza, A.J.; Montufar-Solis, D.; Duke, P.J.; Athanasiou, K.A. Cell type and distribution in the porcine temporomandibular joint disc. J. Oral Maxillofac. Surg. 2006, 64, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Plumb, M.; Aspden, R.M. The response of elderly human articular cartilage to mechanical stimuli in vitro. Osteoarthr. Cartil. 2005, 13, 1084–1091. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, D. TMJ bioengineering: A review. J. Oral Biol. Craniofac. Res. 2013, 3, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Centeno, C.J.; Busse, D.; Kisiday, J.; Keohan, C.; Freeman, M.; Karli, D. Increased knee cartilage volume in degenerative joint disease using percutaneously implanted, autologous mesenchymal stem cells. Pain Physician 2008, 11, 343–353. [Google Scholar] [PubMed]
- Vangsness Jr, C.T.; Jack Farr, I.; Boyd, J.; Dellaero, D.T.; Mills, C.R.; LeRoux-Williams, M. Adult human mesenchymal stem cells delivered via intra-articular injection to the knee following partial medial meniscectomy: A randomized, double-blind, controlled study. J. Bone Joint Surg. Am. 2014, 96, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzute, T.; Lynch, K.; Pei, M. Impact of tissue-specific stem cells on lineage-specific differentiation: A focus on the musculoskeletal system. Stem Cell Rev. 2015, 11, 119–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäenpää, K.; Ellä, V.; Mauno, J.; Kellomäki, M.; Suuronen, R.; Ylikomi, T.; Miettinen, S. Use of adipose stem cells and polylactide discs for tissue engineering of the temporomandibular joint disc. J. R. Soc. Interface 2010, 7, 177–188. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Yap, A.U.; Toh, W.S. Stem cells for temporomandibular joint repair and regeneration. Stem Cell Rev. 2015, 11, 728–742. [Google Scholar] [CrossRef]
- Ahtiainen, K.; Mauno, J.; Ellä, V.; Hagström, J.; Lindqvist, C.; Miettinen, S.; Ylikomi, T.; Kellomäki, M.; Seppänen, R. Autologous adipose stem cells and polylactide discs in the replacement of the rabbit temporomandibular joint disc. J. R. Soc. Interface 2013, 10, 20130287. [Google Scholar] [CrossRef]
- Carboni, A.; Amodeo, G.; Perugini, M.; Arangio, P.; Orsini, R.; Scopelliti, D. Temporomandibular disorders clinical and anatomical outcomes after fat-derived stem cells injection. J. Craniofacial Surg. 2019, 30, 793–797. [Google Scholar] [CrossRef]
- Saito, M.T.; Silvério, K.G.; Casati, M.Z.; Sallum, E.A.; Nociti Jr, F.H. Tooth-derived stem cells: Update and perspectives. World J. Stem Cells 2015, 7, 399–407. [Google Scholar] [CrossRef]
- Guo, L.; Li, J.; Qiao, X.; Yu, M.; Tang, W.; Wang, H.; Guo, W.; Tian, W. Comparison of odontogenic differentiation of human dental follicle cells and human dental papilla cells. PLoS ONE 2013, 8, e62332. [Google Scholar] [CrossRef] [Green Version]
- Sedgley, C.M.; Botero, T.M. Dental stem cells and their sources. Dent. Clin. N. Am. 2012, 56, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; He, N.; Feng, C.; Liu, V.; Zhang, L.; Wang, F.; He, J.; Zhu, T.; Wang, S.; Qiao, W. Human adipose-derived mesenchymal progenitor cells engraft into rabbit articular cartilage. Int. J. Mol. Sci. 2015, 16, 12076–12091. [Google Scholar] [CrossRef]
- Xing, D.; Wu, J.; Wang, B.; Liu, W.; Liu, W.; Zhao, Y.; Wang, L.; Li, J.J.; Liu, A.; Zhou, Q. Intra-articular delivery of umbilical cord-derived mesenchymal stem cells temporarily retard the progression of osteoarthritis in a rat model. Int. J. Rheum. Dis. 2020, 23, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yang, G.; Park, J.; Choi, J.; Kang, E.; Lee, B.-K. Therapeutic effect of mesenchymal stem cells derived from human umbilical cord in rabbit temporomandibular joint model of osteoarthritis. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Teo, K.Y.W.; Chuah, S.J.; Lai, R.C.; Lim, S.K.; Toh, W.S. MSC exosomes alleviate temporomandibular joint osteoarthritis by attenuating inflammation and restoring matrix homeostasis. Biomaterials 2019, 200, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Toh, W.S.; Foldager, C.B.; Pei, M.; Hui, J.H.P. Advances in mesenchymal stem cell-based strategies for cartilage repair and regeneration. Stem Cell Rev. 2014, 10, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chu, W.; Lai, R.; Lim, S.; Hui, J.; Toh, W. Exosomes derived from human embryonic mesenchymal stem cells promote osteochondral regeneration. Osteoarthr. Cartil. 2016, 24, 2135–2140. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Cheng, H.; Cheung, K.; Chan, D.; Chan, B. Mesenchymal stem cell-collagen microspheres for articular cartilage repair: Cell density and differentiation status. Acta Biomater. 2014, 10, 1919–1929. [Google Scholar] [CrossRef]
- Ferreira, M.S.V.; Jahnen-Dechent, W.; Labude, N.; Bovi, M.; Hieronymus, T.; Zenke, M.; Schneider, R.K.; Neurs, S. Cord blood-hematopoietic stem cell expansion in 3D fibrin scaffolds with stromal support. Biomaterials 2012, 33, 6987–6997. [Google Scholar] [CrossRef]
- Suhaeb, A.M.; Naveen, S.; Mansor, A.; Kamarul, T. Hyaluronic acid with or without bone marrow derived-mesenchymal stem cells improves osteoarthritic knee changes in rat model: A preliminary report. Indian J. Exp. Biol. 2011, 50, 383–390. [Google Scholar]
- Sato, M.; Uchida, K.; Nakajima, H.; Miyazaki, T.; Guerrero, A.R.; Watanabe, S.; Roberts, S.; Baba, H. Direct transplantation of mesenchymal stem cells into the knee joints of Hartley strain guinea pigs with spontaneous osteoarthritis. Arthritis Res. Ther. 2012, 14, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Duan, X.; Fan, Z.; Chen, L.; Xing, F.; Xu, Z.; Chen, Q.; Xiang, Z. Mesenchymal stem cells in combination with hyaluronic acid for articular cartilage defects. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chiang, E.-R.; Ma, H.-L.; Wang, J.-P.; Liu, C.-L.; Chen, T.-H.; Hung, S.-C. Allogeneic mesenchymal stem cells in combination with hyaluronic acid for the treatment of osteoarthritis in rabbits. PLoS ONE 2016, 11, e0149835. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, I.S.; Cho, T.H.; Lee, K.B.; Hwang, S.J.; Tae, G.; Noh, I.; Lee, S.H.; Park, Y.; Sun, K. Bone regeneration using hyaluronic acid-based hydrogel with bone morphogenic protein-2 and human mesenchymal stem cells. Biomaterials 2007, 28, 1830–1837. [Google Scholar] [CrossRef]
- Yoshioka, M.; Shimizu, C.; Harwood, F.L.; Coutts, R.D.; Amiel, D. The effects of hyaluronan during the development of osteoarthritis. Osteoarthr. Cartil. 1997, 5, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Kavalkovich, K.W.; Boynton, R.E.; Murphy, J.M.; Barry, F. Chondrogenic differentiation of human mesenchymal stem cells within an alginate layer culture system. In Vitro Cell. Dev. Biol. Anim. 2002, 38, 457–466. [Google Scholar] [CrossRef]
- Maniwa, S.; Ochi, M.; Motomura, T.; Nishikori, T.; Chen, J.; Naora, H. Effects of hyaluronic acid and basic fibroblast growth factor on motility of chondrocytes and synovial cells in culture. Acta Orthop. Scand. 2001, 72, 299–303. [Google Scholar] [CrossRef]
- Wittig, O.; Diaz-Solano, D.; Cardier, J. Viability and functionality of mesenchymal stromal cells loaded on collagen microspheres and incorporated into plasma clots for orthopaedic application: Effect of storage conditions. Injury 2018, 49, 1052–1057. [Google Scholar] [CrossRef]
- Gomez, M.; Wittig, O.; Diaz-Solano, D.; Cardier, J.E. Mesenchymal Stromal Cell Transplantation Induces Regeneration of Large and Full-Thickness Cartilage Defect of the Temporomandibular Joint. Cartilage 2020, 1947603520926711. [Google Scholar] [CrossRef]
- Maumus, M.; Peyrafitte, J.-A.; d’Angelo, R.; Fournier-Wirth, C.; Bouloumié, A.; Casteilla, L.; Sengenès, C.; Bourin, P. Native human adipose stromal cells: Localization, morphology and phenotype. Int. J. Obes. 2011, 35, 1141–1153. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.-E.; Park, Y.-C.; Seo, B.-K.; Lee, J.-D.; Baek, Y.-H.; Choi, D.-Y.; Park, D.-S. Cartilage protective and chondrogenic capacity of WIN-34B, a new herbal agent, in the collagenase-induced osteoarthritis rabbit model and in progenitor cells from subchondral bone. Evid. Based Complementary Altern. Med. 2013, 2013, 527561. [Google Scholar] [CrossRef] [PubMed]
- Barzelay, A.; Levy, R.; Kohn, E.; Sella, M.; Shani, N.; Meilik, B.; Entin-Meer, M.; Gur, E.; Loewenstein, A.; Barak, A. Power-assisted liposuction versus tissue resection for the isolation of adipose tissue–derived mesenchymal stem cells: Phenotype, senescence, and multipotency at advanced passages. Aesthet. Surg. J. 2015, 35, NP230–NP240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641–648. [Google Scholar] [PubMed] [Green Version]
- Zhu, M.; Heydarkhan-Hagvall, S.; Hedrick, M.; Benhaim, P.; Zuk, P. Manual isolation of adipose-derived stem cells from human lipoaspirates. J. Vis. Exp. 2013, 26, e50585. [Google Scholar] [CrossRef] [PubMed]
- Hahn, M.; Vogel, M.; Delling, G. Undecalcified preparation of bone tissue: Report of technical experience and development of new methods. Virchows Arch. 1991, 418, 1–7. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Cells/Fluid | Mean (M, µm) | Standard Deviation (SD, µm) |
|---|---|---|---|
| 1 | AB Serum (ABS) | 195.26 | 86.78 |
| 2 | Hyaluronic Acid (HA) | 195.24 | 81.58 |
| 3 | Mesenchymal Stromal Cells (STx.) | 228.78 | 103.62 |
| 4 | Mesenchymal Stromal Cells in hyaluronic acid (HA + STx.) | 231.14 | 92.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köhnke, R.; Ahlers, M.O.; Birkelbach, M.A.; Ewald, F.; Krueger, M.; Fiedler, I.; Busse, B.; Heiland, M.; Vollkommer, T.; Gosau, M.; et al. Temporomandibular Joint Osteoarthritis: Regenerative Treatment by a Stem Cell Containing Advanced Therapy Medicinal Product (ATMP)—An In Vivo Animal Trial. Int. J. Mol. Sci. 2021, 22, 443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010443
Köhnke R, Ahlers MO, Birkelbach MA, Ewald F, Krueger M, Fiedler I, Busse B, Heiland M, Vollkommer T, Gosau M, et al. Temporomandibular Joint Osteoarthritis: Regenerative Treatment by a Stem Cell Containing Advanced Therapy Medicinal Product (ATMP)—An In Vivo Animal Trial. International Journal of Molecular Sciences. 2021; 22(1):443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010443
Chicago/Turabian StyleKöhnke, Robert, Marcus Oliver Ahlers, Moritz Alexander Birkelbach, Florian Ewald, Michael Krueger, Imke Fiedler, Björn Busse, Max Heiland, Tobias Vollkommer, Martin Gosau, and et al. 2021. "Temporomandibular Joint Osteoarthritis: Regenerative Treatment by a Stem Cell Containing Advanced Therapy Medicinal Product (ATMP)—An In Vivo Animal Trial" International Journal of Molecular Sciences 22, no. 1: 443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010443