
Acquired Idiopathic Generalized Anhidrosis (AIGA) and Its Complications: Implications for AIGA as an Autoimmune Disease


Abstract
:1. Introduction
2. Epidemiology of AIGA and CholU with Anhidrosis/Hypohidrosis
3. Two Mechanisms of CholU and Relation to Anhidrosis/Hypohidrosis
4. Immunological Findings in AIGA
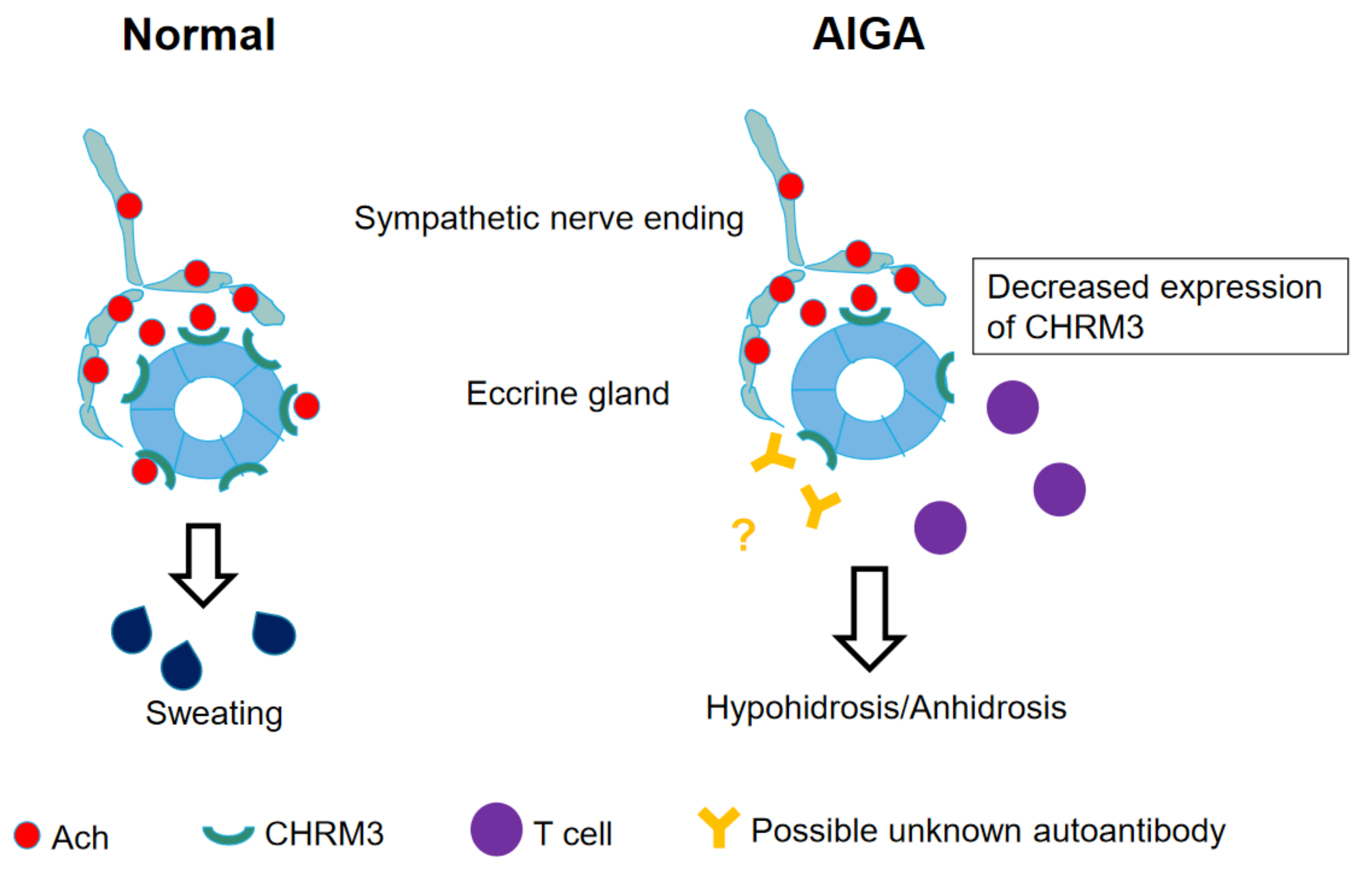
5. Decreased Expression of CHRM3 in AIGA
6. Autoimmune Diseases as Representative Complications or Comorbidities of AIGA
6.1. Central Diabetes Insipidus
6.2. Rheumatoid Arthritis
6.3. Crohn’s Disease
6.4. Alopecia Areata
6.5. Vitiligo Vulgaris and Vogt-Koyanagi-Harada Disease
6.6. Lichen Planus
7. AIGA-Associated Autoimmune Diseases in Our Cases and Literature
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Munetsugu, T.; Fujimoto, T.; Oshima, Y.; Sano, K.; Murota, H.; Satoh, T.; Iwase, S.; Asahina, M.; Nakazato, Y.; Yokozeki, H. Revised guideline for the diagnosis and treatment of acquired idiopathic generalized anhidrosis in Japan. J. Dermatol. 2017, 44, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Tokura, Y. Direct and indirect action modes of acetylcholine in cholinergic urticaria. Allergol. Int. 2021, 70, 39–44. [Google Scholar] [CrossRef]
- Sawada, Y.; Nakamura, M.; Bito, T.; Fukamachi, S.; Kabashima, R.; Sugita, K.; Hino, R.; Tokura, Y. Cholinergic urticaria: Studies on the muscarinic cholinergic receptor M3 in anhidrotic and hypohidrotic skin. J. Investig. Dermatol. 2010, 130, 2683–2686. [Google Scholar] [CrossRef] [Green Version]
- Iida, T.; Nakamura, M.; Inazawa, M.; Munetsugu, T.; Nishida, M.; Fujimoto, T.; Sasaki, Y.; Ohshima, Y.; Nakazato, Y.; Namiki, T.; et al. Prognosis after steroid pulse therapy and seasonal effect in acquired idiopathic generalized anhidrosis. J. Dermatol. 2021, 48, 271–278. [Google Scholar]
- Mok, Z.R.; Tey, H.L. Acquired idiopathic generalized anhidrosis: Successful treatment with cyclosporine in two cases. Dermatol. Ther. 2018, 31, e12579. [Google Scholar]
- Pargfrieder, C.; Struhal, W.; Sega, W.; Klein, G.; Sepp, N.; Exler, G. Acquired idiopathic generalized anhidrosis in a young Austrian patient. JAAD Case Rep. 2018, 4, 222–225. [Google Scholar] [CrossRef] [Green Version]
- Palm, F.; Loser, C.; Gronau, W.; Voigtlander, V.; Grau, A.J. Successful treatment of acquired idiopathic generalized anhidrosis. Neurology 2007, 68, 532–533. [Google Scholar] [CrossRef]
- Wolinia, U. Acquired idiopathic generalized anhidrosis. J. Dermatol. Case Rep. 2014, 8, 120–121. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Villaverde, R.; Sanchez Cano, D. Acquired idiopathic generalized anhidrosis. Actas Dermosifiliogr. 2006, 97, 551–552. [Google Scholar] [CrossRef]
- Brantely, E.; Mutasim, D.F.; Heaton, C. Acquired idiopathic generalized anhidrosis: Case report. Cutis 2011, 87, 21–23. [Google Scholar]
- Kay, D.; Maibach, H. Pruritus and acquired anhidrosis-two unusual cases. Arch. Dermatol. 1969, 100, 291–293. [Google Scholar] [CrossRef]
- Weigand, D.; Everett, M. Acquired generalized anhidrosis. Arch. Dermatol. 1966, 93, 443–445. [Google Scholar] [CrossRef]
- Ohshima, Y.; Yanagishita, T.; Ito, K.; Tamada, Y.; Nishimura, N.; Inukai, Y.; Iwase, S.; Watanabe, D. A case of acquired idiopathic generalized anhidrosis in a 2-year-old infant. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1446–1448. [Google Scholar] [CrossRef] [PubMed]
- Hiragun, T.; Hiragun, M.; Ishii, K.; Kan, T.; Hide, M. Sweat allergy: Extrinsic or intrinsic? J. Dermatol. Sci. 2017, 87, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiragun, T.; Ishii, K.; Hiragun, M.; Suzuki, H.; Kan, T.; Mihara, S.; Yanase, Y.; Bartels, J.; Schroder, J.M.; Hide, M. Fungal protein MGL_1304 in sweat is an allergen for atopic dermatitis patients. J. Allergy Clin. Immunol. 2013, 132, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, S.; Aoshima, M.; Tokura, Y. Studies on hidrotic condition and sweating recovery after corticosteroid-pulse therapy in seven patients with acquired idiopathic generalized anhidrosis/anhidrotic or hypohidrotic cholinergic urticarial. Jpn. J. Dermatol. 2016, 126, 1263–1271. (In Japanese) [Google Scholar]
- Sawada, Y.; Nakamura, M.; Bito, T.; Sakabe, J.; Kabashima-Kubo, R.; Hino, R.; Kobayashi, M.; Tokura, Y. Decreased expression of acetylcholine esterase in cholinergic urticarial with hypohidrosis or anhidrosis. J. Investig. Dermatol. 2014, 134, 276–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honma, M.; Iinuma, S.; Kanno, K.; Komatsu, S.; Minami-Hori, M.; Ishida-Yamamoto, A. Correlation of disease activity and serum level of carcinoembryonic antigen in acquired idiopathic generalized anhidrosis: A case report. J. Dermatol. 2015, 42, 900–902. [Google Scholar] [CrossRef] [Green Version]
- Honma, M.; Iinuma, S.A.; Kanno, K.; Komatsu, S.; Minami-Hori, M.; Iizuka, H.; Ishida-Yamamoto, A. Serum carcinoembryonic antigen (CEA) as a clinical marker in acquired idiopathic generalized anhidrosis: A close correlation between serum CEA level and disease activity. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1379–1383. [Google Scholar] [CrossRef]
- Iizuka, T.; Suzuki, T.; Nakano, K.; Sueki, H. Immunolocalization of aquaporin-5 in normal human skin and hypohidrotic skin diseases. J. Dermatol. 2012, 39, 344–349. [Google Scholar] [CrossRef]
- Haustein, U.F.; Schliebs, R.; Schaller, J. Changes in muscarinic acetylcholine receptor binding in skin slices of cholinergic urticaria. Acta Derm-Venereol. 1990, 70, 208–211. [Google Scholar] [PubMed]
- Fantozzi, R.; Masini, E.; Blandina, P.; Mannaioni, P.F.; Bani-Sacchi, T. Release of histamine from rat mast cells by acetylcholine. Nature 1978, 273, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Blandina, P.; Fantozzi, R.; Mannaioni, P.F.; Masini, E. Characteristics of histamine release evoked by acetylcholine in isolated rat mast cells. J. Physiol. 1980, 301, 281–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrahy, A.; Moran, C.; Thompson, C.J. Diagnosis and management of central diabetes insipidus in adults. Clin. Endocrinol. 2019, 90, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Imura, H.; Nakao, K.; Shimatsu, A.; Ogawa, Y.; Sando, T.; Fujisawa, I.; Yamabe, H. Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. N. Engl. J. Med. 1993, 329, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, A.; Tago, O.; Motegi, S.; Hattori, T.; Nagai, Y.; Takahashi, M.; Arakawa, K.; Ishikawa, O. A case of diabetes insipidus diagnosed from the development of acquired systemic anhidrosis. Jpn. J. Clin. Dermatol. 2013, 67, 681–684. (In Japanese) [Google Scholar]
- Asahina, M.; Suzuki, A.; Tamura, N.; Yoshida, T.; Hattori, T. A case of acquired idiopathic generalized anhidrosis that developed central diabetes insipidus during the course. Jpn. J. Perspirat. Res. 2004, 11, 12–14. (In Japanese) [Google Scholar]
- Imura, K.; Kasuya, A.; Tokura, Y. Acquired idiopathic generalized anhidrosis: A case accompanied by central diabetes insipidus. J. Vis. Dermatol. 2020, 19, 237–239. (In Japanese) [Google Scholar]
- Kurachi, H.; Kurihara, Y.; Kobayashi, K.; Ouchi, T.; Funakoshi, T.; Amagai, M.; Yamagami, J. A case of acquired idiopathic generalized anhidrosis that developed in patients with rheumatoid arthritis and diabetes. Jpn. J. Dermatol. 2018, 128, 72. (In Japanese) [Google Scholar]
- Ohshima, Y.; Itoh, K.; Tamada, Y.; Watanabe, D.; Nishimura, N.; Iwase, S.; Sugenoya, J. Treatment of patients with acquired idiopathic generalized anhidrosis. Jpn. J. Perspirat. Res. 2011, 18, 3–6. (In Japanese) [Google Scholar]
- Ramos, G.P.; Papadakis, K.A. Mechanisms of disease: Inflammatory bowel diseases. Mayo. Clin. Proc. 2019, 94, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Geremia, A.; Biancheri, P.; Allan, P.; Corazza, G.R.; Sabatino, A.D. Innate and adaptive immunity in inflammatory bowel disease. Autoimmun. Rev. 2014, 13, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, Y.; Mizukawa, Y.; Yamazaki, Y.; Ohyama, M. A case of acquired idiopathic generalized anhidrosis with alopecia areata. Nishinihon J. Dermatol. 2019, 81, 240. (In Japanese) [Google Scholar]
- Ito, T.; Tokura, Y. The role of cytokines and chemokines in the T-cell-mediated autoimmune process in alopecia areata. Exp. Dermatol. 2014, 23, 787–791. [Google Scholar]
- Zeberkiewicz, M.; Rudnicka, L.; Malejczyk, J. Immunology of alopecia areata. Cent Eur. J. Immunol. 2020, 45, 325–333. [Google Scholar]
- Saito, H.; Yamada, T. A case of acquired idiopathic generalized anhidrosis with vitiligo vulgaris that developed after influenza infection. Jpn. J. Perspirat. Res. 2015, 22, 7–9. (In Japanese) [Google Scholar]
- Sakaguchi, M.; Tsuruta, D.; Ishii, N.; Hamada, T.; Ohata, C.; Furumura, M.; Hashimoto, T. Development of acquired idiopathic generalized anhidrosis in a case of Vogt-Koyanagi-Harada disease. Eur. J. Dermatol. 2013, 23, 724–725. [Google Scholar] [CrossRef] [PubMed]
- Le Poole, I.C.; Wankowicz-Kalinska, A.; Van den Wijngaard, R.M.; Nickoloff, B.J.; Das, P.K. Autoimmune aspects of depigmentation in vitiligo. J. Investig. Dermatol. Symp. Proc. 2004, 9, 68–72. [Google Scholar]
- Narita, T.; Oiso, N.; Fukai, K.; Kabashima, K.; Kawada, A.; Suzuki, T. Generalized vitiligo and associated autoimmune diseases in Japanese patients and their families. Allergol. Int. 2011, 60, 505–508. [Google Scholar] [CrossRef] [Green Version]
- Oiso, N.; Suzuki, T.; Fukai, K.; Katayama, I.; Kawada, A. Nonsegmental vitiligo and autoimmune mechanism. Dermatol. Res. Pract. 2011, 2011, 1. [Google Scholar] [CrossRef] [Green Version]
- Kemp, E.H.; Gawkrodger, D.J.; Watson, P.F.; Weetman, A.P. Immunoprecipitation of melanogenic enzyme autoantigens with vitiligo sera: Evidence for cross-reactive autoantibodies to tyrosinase and tyrosinase-related protein-2 (TRP-2). Clin. Exp. Immunol. 1997, 109, 495–500. [Google Scholar]
- Vrijman, C.; Kroon, M.W.; Limpens, J.; Leeflang, M.M.G.; Luiten, R.M.; Van der Veen, J.P.W.; Wolkerstorfer, A.; Spuls, P.I. The prevalence of thyroid disease in ptients with vitiligo: A systemic review. Br. J. Dermatol. 2012, 167, 1224–1235. [Google Scholar]
- Gangadharan, G.; Citron, S.; Surendran, D. Acquired idiopathic generalized anhidrosis. Indian J. Dermatol. 2015, 60, 422. [Google Scholar] [CrossRef]
- Mushtaq, S. Lichen planus and alopecia areata co-localization. Indian J. Dermatol. 2021, 66, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Cojocaru, M.; Cojocaru, I.M.; Silosi, I. Multiple autoimmune syndrome. Maedica 2010, 5, 132–134. [Google Scholar]
- Ogura, Y.; Hanai, S.; Kageyama, R.; Aoshima, M.; Ohtsuka, K.; Yagi, H.; Tokura, Y. A case of acquired idiopathic generalized anhidrosis accompanied by hypogammaglobulinemia. Jpn. J. Clin. Dermatol. 2020, 74, 1015–1020. (In Japanese) [Google Scholar]
- Kersh, A.E.; Schuchter, L.M.; Elenitsas, R.; Chu, E.Y. Hypohidrosis as an immune-related adverse event of checkpoint inhibitor therapy. Immunotherapy 2020, 12, 951–956. [Google Scholar] [CrossRef]
- Asahina, M.; Sano, K.; Fujinuma, Y.; Kuwabara, S. Investigation of antimuscarinic receptor autoantibodies in patients with acquired idiopathic generalized anhidrosis. Intern. Med. 2013, 52, 2733–2737. [Google Scholar] [CrossRef] [Green Version]
- Yanagishita, T. Acquired idiopathic generalized anhidrosis. Jpn. J. Dermatol. 2021, 131, 35–41. (In Japanese) [Google Scholar]
- Yang, P.; Qian, F.Y.; Zhang, M.F.; Xu, A.L.; Wang, X.; Jiang, B.P.; Zhou, L.L. Th17 cell pathogenicity and plasticity in rheumatoid arthritis. J. Leukoc. Biol. 2019, 106, 1233–1240. [Google Scholar]
- Tokura, Y.; Phadungsaksawasdi, P.; Kurihara, K.; Fujiyama, T.; Honda, T. Pathophysiology of skin resident memory T cells. Front. Immunol. 2021, 11, 618897. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cases | Age | Sex | Complication or Comorbidity | Period from AIGA Onset to the First Visit | Lymphocyte Infiltration around the Sweat Glands in Non-Sweat Area | CHRM3 Expression | Clinical Outcome with Steroid Pulse Therapy |
|---|---|---|---|---|---|---|---|
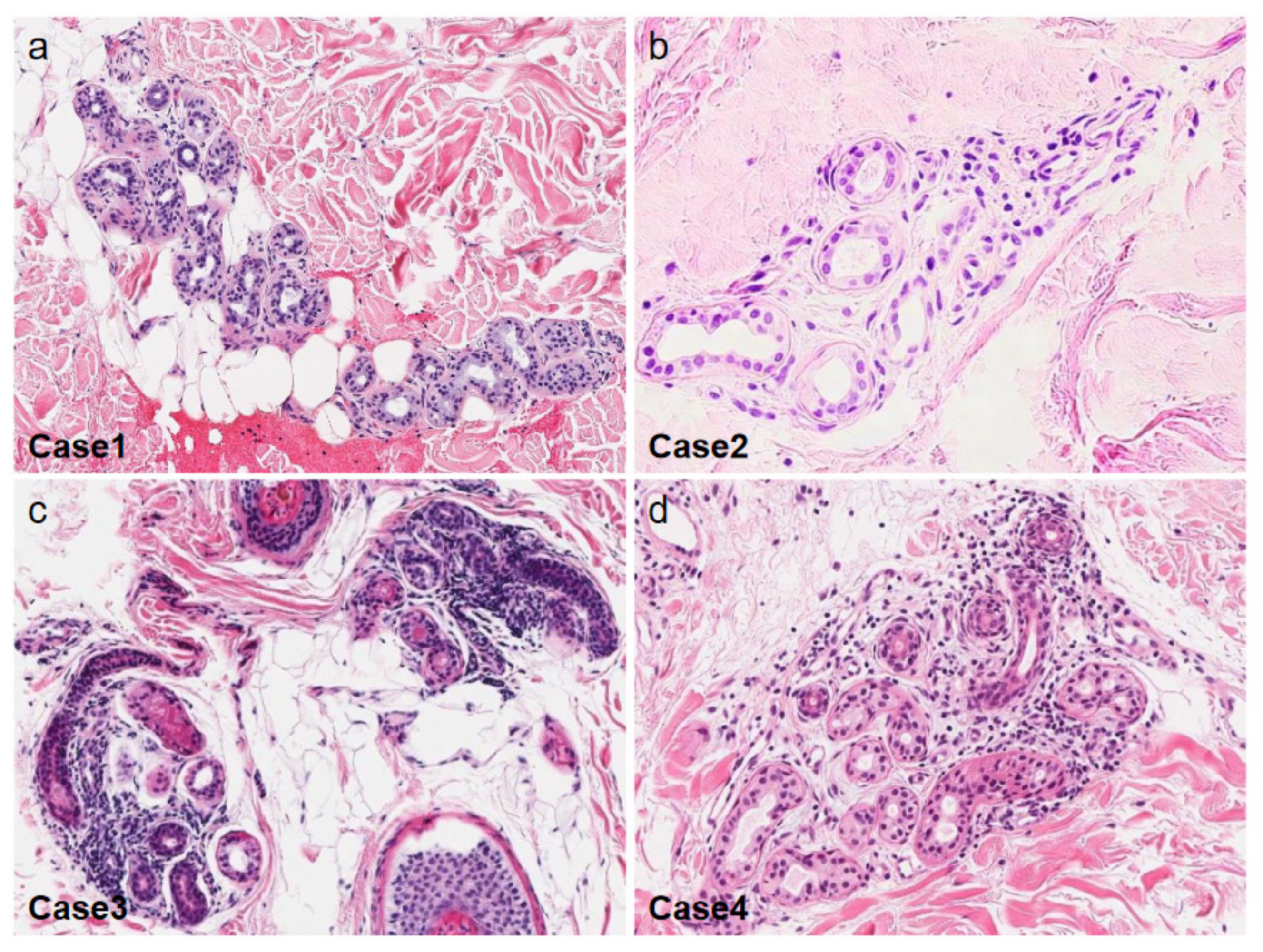
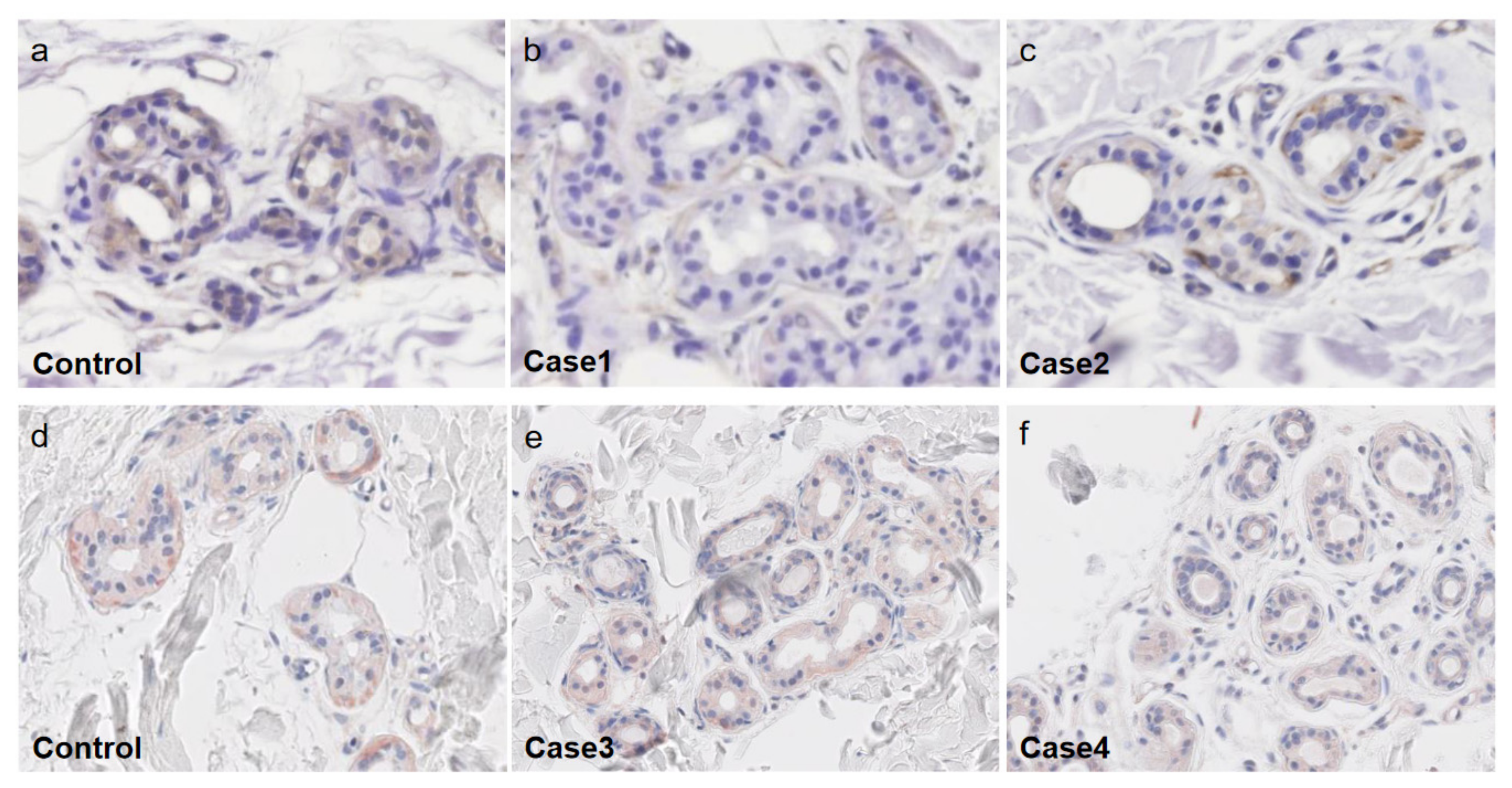
| Our case1 | 55 | M | Central diabetes insipidus | 15 years | Mild Mild sweat glands atrophy | Decreased | Improved sweating |
| Our case2 | 41 | M | Hypogammaglobulinemia | 10 years | Almost none Mild sweat glands atrophy | Decreased | No significant improvement in sweating |
| Our case3 | 42 | M | Basedow’s disease | 2 years | Mild to moderate | Decreased | Improved sweating |
| Our case4 | 32 | M | Pulmonary sarcoidosis, Psoriasis vulgaris | 3 months | Mild | Decreased | Improved sweating |
| Shimoda et al., 2019 | 43 | M | Alopecia areata | 1 year | Mild | N/A | Improved sweating |
| Kurachi et al., 2018 | 67 | M | Rheumatoid arthritis | 2 months | Almost none | N/A | Improved sweating |
| Gangadharan et al., 2015 | 47 | M | Lichen planus | 3 years | None Absence of sweat glands | N/A | Improved sweating |
| Saito et al., 2015 | 50 | M | Vitiligo vulgaris | 5 months | Moderate | N/A | Improved sweating |
| Sakaguchi et al., 2013 | 45 | M | Vogt-Koyanagi-Harada disease | 20 years | Mild Sweat glands atrophy | N/A | Improved sweating |
| Ohshima et al., 2011 | 41 | M | Crohn’s disease | 3 months | None | N/A | Improved sweating |
| Asahina et al., 2004 | 25 | M | Central diabetes insipidus | 19 months | None | N/A | Improved sweating |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kageyama, R.; Honda, T.; Tokura, Y. Acquired Idiopathic Generalized Anhidrosis (AIGA) and Its Complications: Implications for AIGA as an Autoimmune Disease. Int. J. Mol. Sci. 2021, 22, 8389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168389
Kageyama R, Honda T, Tokura Y. Acquired Idiopathic Generalized Anhidrosis (AIGA) and Its Complications: Implications for AIGA as an Autoimmune Disease. International Journal of Molecular Sciences. 2021; 22(16):8389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168389
Chicago/Turabian StyleKageyama, Reiko, Tetsuya Honda, and Yoshiki Tokura. 2021. "Acquired Idiopathic Generalized Anhidrosis (AIGA) and Its Complications: Implications for AIGA as an Autoimmune Disease" International Journal of Molecular Sciences 22, no. 16: 8389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168389