
Ovarian Folliculogenesis and Uterine Endometrial Receptivity after Intermittent Vaginal Injection of Recombinant Human Follicle-Stimulating Hormone in Infertile Women Receiving In Vitro Fertilization and in Immature Female Rats

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
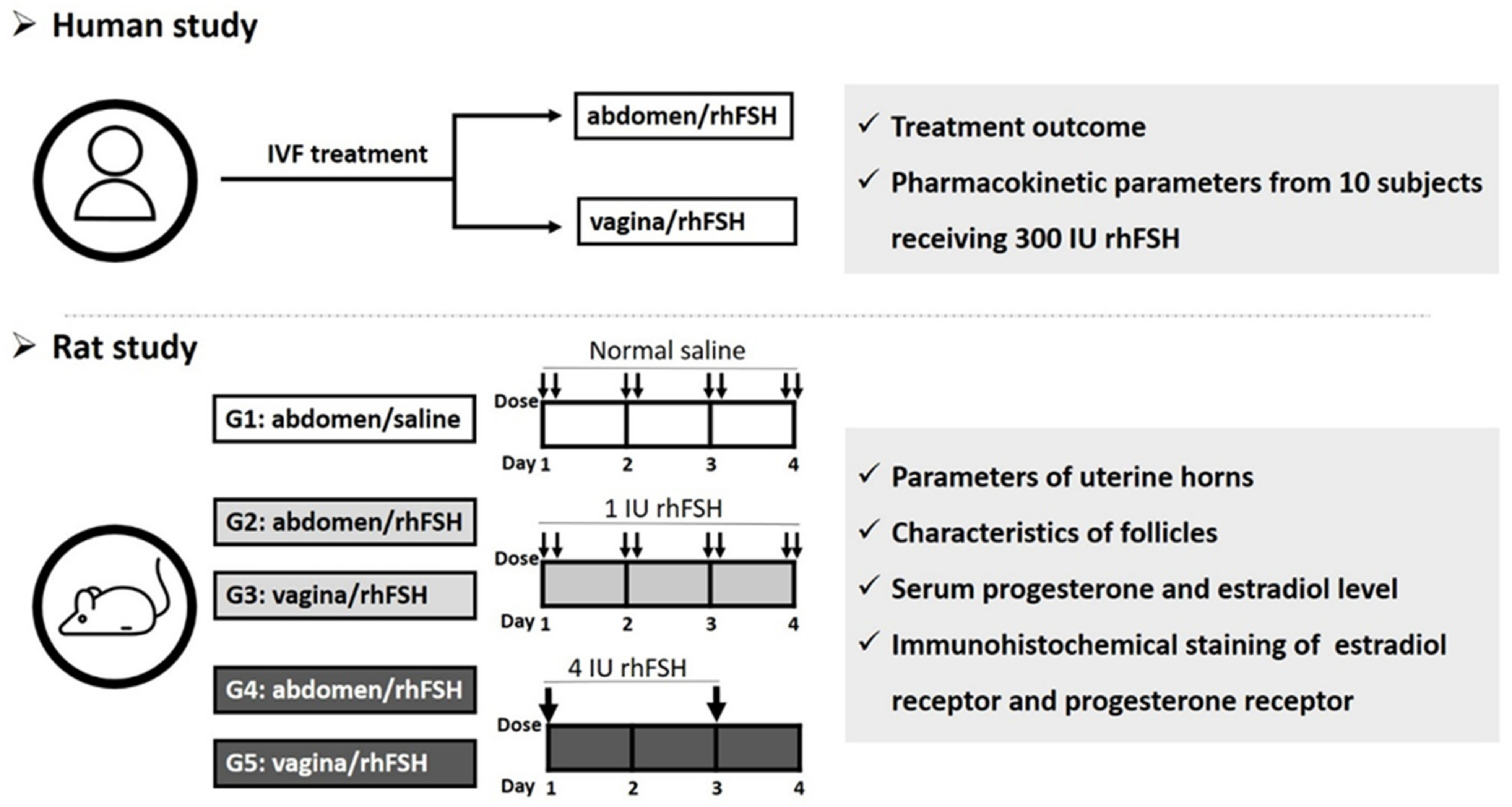
2.1. Human Study
2.2. Rat Study
2.2.1. Parameters of Uterine Horns
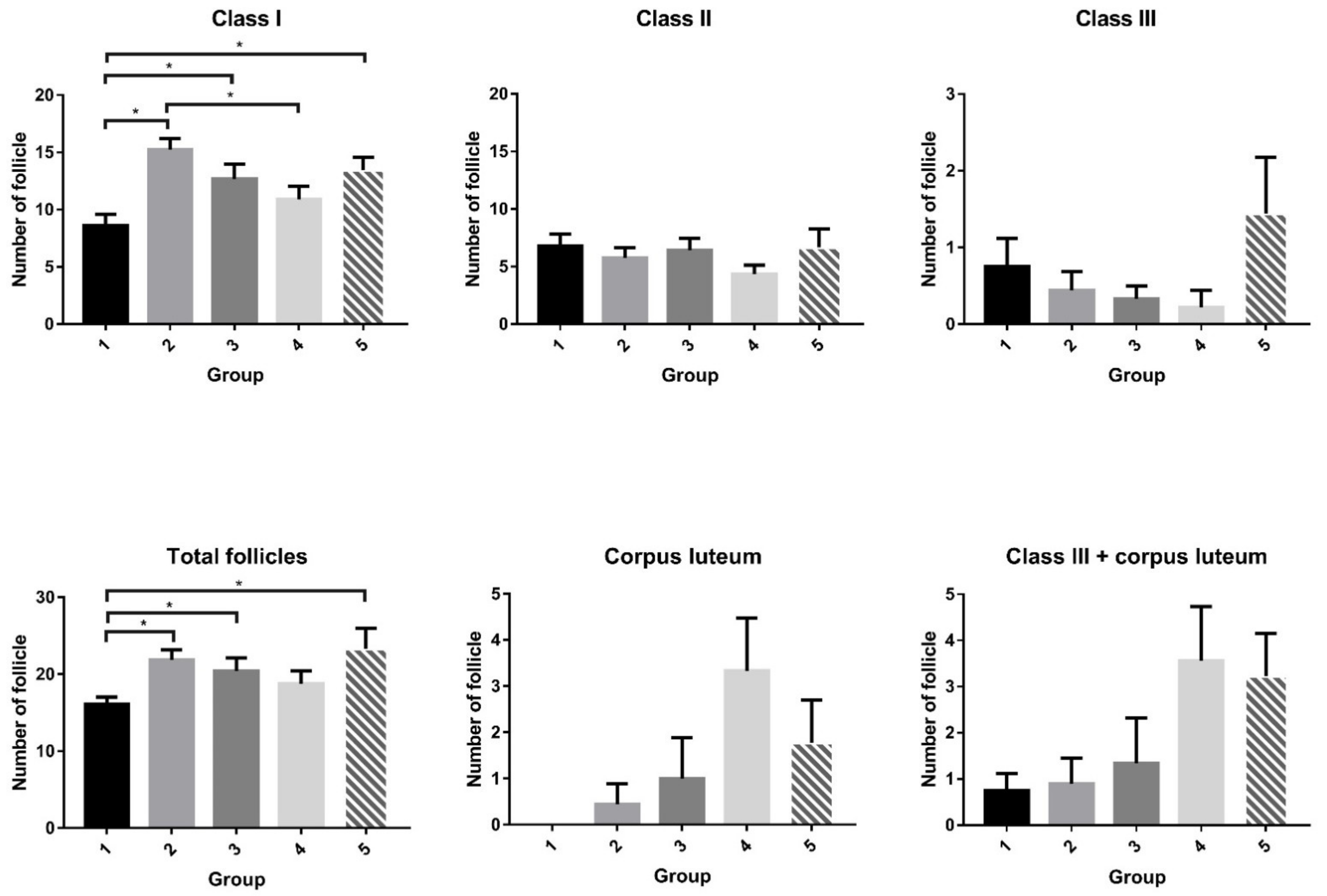
2.2.2. Characteristics of Follicles
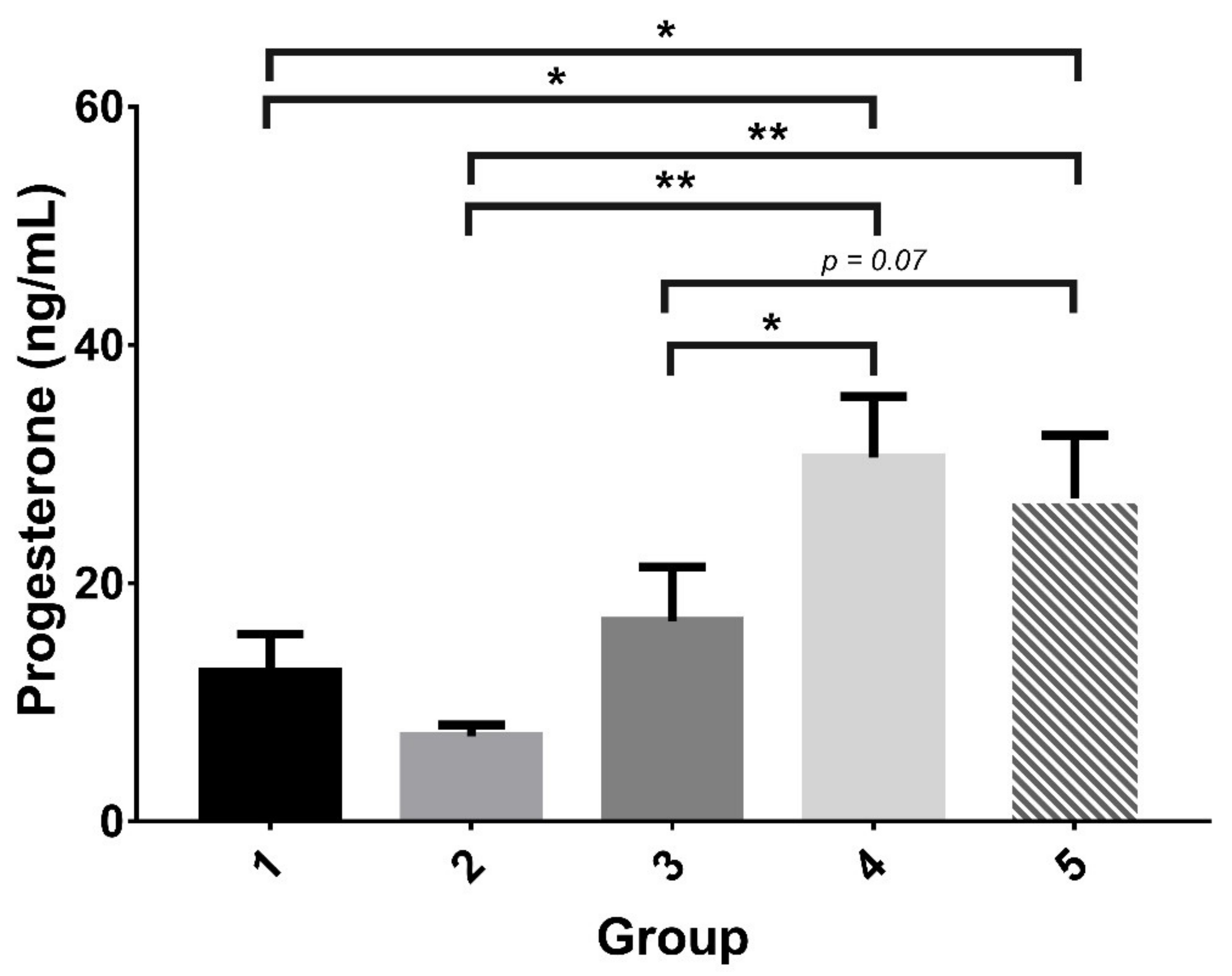
2.2.3. Serum Progesterone Level and Detection of ER and PR
3. Discussion
4. Materials and Methods
4.1. Human Study
4.1.1. Participants
Clinical IVF Treatment
Pharmacokinetic Study
Clinical Measurements
Safety Parameters
Measurement of Serum Hormone Levels
4.2. Animal Study
4.2.1. Rats
4.2.2. Experiments
4.2.3. Measurement of Endometrium and Classification of Follicles
4.2.4. Hormone Analysis
4.2.5. Immunohistochemistry of ER and PR
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zegers-Hochschild, F.; Adamson, G.D.; de Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Vanderpoel, S. International committee for monitoring assisted reproductive technology (ICMART) and the world health organization (WHO) revised glossary of ART terminology, 2009. Fertil. Steril. 2009, 92, 1520–1524. [Google Scholar] [CrossRef]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef]
- Zhao, Y.; Brezina, P.; Hsu, C.C.; Garcia, J.; Brinsden, P.R.; Wallach, E. In vitro fertilization: Four decades of reflections and promises. Biochim. Biophys. Acta 2011, 1810, 843–852. [Google Scholar] [CrossRef]
- Lunenfeld, B.; Bilger, W.; Longobardi, S.; Alam, V.; D’Hooghe, T.; Sunkara, S.K. The development of gonadotropins for clinical use in the treatment of infertility. Front. Endocrinol. 2019, 10, 429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirtea, P.; de Ziegler, D.; Poulain, M.; Ayoubi, J.M. New twists in ovarian stimulation and their practical implications. Front. Med. 2019, 6, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauser, B.C.; Diedrich, K.; Devroey, P. Predictors of ovarian response: Progress towards individualized treatment in ovulation induction and ovarian stimulation. Hum. Reprod. Update 2008, 14, 1–14. [Google Scholar] [CrossRef]
- Nyboe Andersen, A.; Nelson, S.M.; Fauser, B.C.; García-Velasco, J.A.; Klein, B.M.; Arce, J.C. Individualized versus conventional ovarian stimulation for in vitro fertilization: A multicenter, randomized, controlled, assessor-blinded, phase 3 noninferiority trial. Fertil Steril 2017, 107, 387–396.e348. [Google Scholar] [CrossRef] [Green Version]
- Drakopoulos, P.; Blockeel, C.; Stoop, D.; Camus, M.; de Vos, M.; Tournaye, H.; Polyzos, N.P. Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos? Hum. Reprod. 2016, 31, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Baker, V.L.; Brown, M.B.; Luke, B.; Conrad, K.P. Association of number of retrieved oocytes with live birth rate and birth weight: An analysis of 231,815 cycles of in vitro fertilization. Fertil Steril 2015, 103, 931–938.e932. [Google Scholar] [CrossRef] [Green Version]
- Vermey, B.G.; Chua, S.J.; Zafarmand, M.H.; Wang, R.; Longobardi, S.; Cottell, E.; Beckers, F.; Mol, B.W.; Venetis, C.A.; D’Hooghe, T. Is there an association between oocyte number and embryo quality? A systematic review and meta-analysis. Reprod. Biomed. Online 2019, 39, 751–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Gaast, M.H.; Eijkemans, M.J.; van der Net, J.B.; de Boer, E.J.; Burger, C.W.; van Leeuwen, F.E.; Fauser, B.C.; Macklon, N.S. Optimum number of oocytes for a successful first IVF treatment cycle. Reprod. Biomed. Online 2006, 13, 476–480. [Google Scholar] [CrossRef]
- Sunkara, S.K.; Rittenberg, V.; Raine-Fenning, N.; Bhattacharya, S.; Zamora, J.; Coomarasamy, A. Association between the number of eggs and live birth in IVF treatment: An analysis of 400 135 treatment cycles. Hum. Reprod. 2011, 26, 1768–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulson, R.J. Introduction: Contemporary approaches to alternative ovarian stimulation strategies for in vitro fertilization. Fertil Steril 2017, 108, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.B. Pituitary control of ovarian function--concepts derived from gonadotrophin therapy. Aust. N. Z. J. Obstet. Gynaecol. 1978, 18, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Van Santbrink, E.J.; Hop, W.C.; van Dessel, T.J.; de Jong, F.H.; Fauser, B.C. Decremental follicle-stimulating hormone and dominant follicle development during the normal menstrual cycle. Fertil Steril 1995, 64, 37–43. [Google Scholar] [CrossRef]
- Le Cotonnec, J.Y.; Porchet, H.C.; Beltrami, V.; Khan, A.; Toon, S.; Rowland, M. Clinical pharmacology of recombinant human follicle-stimulating hormone (FSH). I. Comparative pharmacokinetics with urinary human FSH. Fertil Steril 1994, 61, 669–678. [Google Scholar]
- Voortman, G.; Mannaerts, B.M.; Huisman, J.A. A dose proportionality study of subcutaneously and intramuscularly administered recombinant human follicle-stimulating hormone (Follistim/Puregon) in healthy female volunteers. Fertil. Steril. 2000, 73, 1187–1193. [Google Scholar] [CrossRef]
- Ben-Rafael, Z.; Levy, T.; Schoemaker, J. Pharmacokinetics of follicle-stimulating hormone: Clinical significance. Fertil Steril 1995, 63, 689–700. [Google Scholar] [CrossRef]
- Bustillo, M. Unsuccessful oocyte retrieval: Technical artefact or genuine ‘empty follicle syndrome’? Reprod. Biomed. Online 2004, 8, 59–67. [Google Scholar] [CrossRef]
- Bühler, K. Managing infertility with the follitropin alfa prefilled pen injector–patient considerations. Ther. Clin. Risk Manag. 2015, 11, 995. [Google Scholar] [CrossRef] [Green Version]
- Van Tilborg, T.C.; Torrance, H.L.; Oudshoorn, S.C.; Eijkemans, M.J.C.; Koks, C.A.M.; Verhoeve, H.R.; Nap, A.W.; Scheffer, G.J.; Manger, A.P.; Schoot, B.C.; et al. Individualized versus standard FSH dosing in women starting IVF/ICSI: An RCT. Part 1: The predicted poor responder. Hum. Reprod. 2017, 32, 2496–2505. [Google Scholar] [CrossRef] [Green Version]
- Toftager, M.; Bogstad, J.; Bryndorf, T.; Løssl, K.; Roskær, J.; Holland, T.; Prætorius, L.; Zedeler, A.; Nilas, L.; Pinborg, A. Risk of severe ovarian hyperstimulation syndrome in GnRH antagonist versus GnRH agonist protocol: RCT including 1050 first IVF/ICSI cycles. Hum. Reprod. 2016, 31, 1253–1264. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.C.; Kuo, H.C.; Hsu, C.T.; Gu, Q. Abdominal mesotherapy injection extended the absorption of follicle-stimulating hormone. Fertil. Steril. 2011, 95, 2134–2136.e2131. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-C.; Hsu, R.; Chang, H.H.; Hsu, I.; Dorjee, S. Extended injection intervals of gonadotropins by intradermal administration in IVF treatment. J. Clin. Endocrinol. Metab. 2021. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Hsu, L.; Hsu, I.; Chiu, Y.-J.; Dorjee, S. Live birth in woman with premature ovarian insufficiency receiving ovarian administration of platelet-rich plasma (PRP) in combination with gonadotropin: A case report. Front. Endocrinol. 2020, 11, 50. [Google Scholar] [CrossRef]
- Hsu, C.C.; Hsu, I.; Hsu, L.; Chiu, Y.J.; Dorjee, S. Resumed ovarian function and pregnancy in early menopausal women by whole dimension subcortical ovarian administration of platelet-rich plasma and gonadotropins. Menopause 2021, 28, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Bulletti, C.; de Ziegler, D.; Flamigni, C.; Giacomucci, E.; Polli, V.; Bolelli, G.; Franceschetti, F. Targeted drug delivery in gynaecology: The first uterine pass effect. Hum. Reprod. 1997, 12, 1073–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, D.T.; Opavsky, M.A. Superovulation of immature rats by continuous infusion of follicle-stimulating hormone. Biol. Reprod. 1988, 39, 511–518. [Google Scholar] [CrossRef] [PubMed]
- The Practice Committee of the American Society for Reproductive Medicine. Progesterone supplementation during the luteal phase and in early pregnancy in the treatment of infertility: An educational bulletin. Fertil. Steril. 2008, 89, 789–792. [Google Scholar] [CrossRef]
- Zarutskie, P.W.; Phillips, J.A. A meta-analysis of the route of administration of luteal phase support in assisted reproductive technology: Vaginal versus intramuscular progesterone. Fertil. Steril. 2009, 92, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Woad, K.J.; Mann, G.E.; Craigon, J.; Raine-Fenning, N.; Robinson, R.S. Evaluation of progestogen supplementation for luteal phase support in fresh in vitro fertilization cycles. Fertil. Steril. 2019, 112, 491–502.e493. [Google Scholar] [CrossRef]
- Hsu, C.C.; Hsu, C.T. Conception using vaginal administration of gonadotrophins in IVF: A case report. Reprod. Biomed. Online 2006, 12, 170–173. [Google Scholar] [CrossRef]
- Hsu, C.C.; Hsu, C.T.; Gu, Q.; Wang, S.T. Intermittent vaginal injections of gonadotrophins for ovarian stimulation in IVF treatment. Reprod Biomed. Online 2008, 16, 617–620. [Google Scholar] [CrossRef]
- Revelli, A.; Casano, S.; Salvagno, F.; Delle Piane, L. Milder is better? Advantages and disadvantages of "mild" ovarian stimulation for human in vitro fertilization. Reprod. Biol. Endocrinol. RBE 2011, 9, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humaidan, P.; Alviggi, C.; Fischer, R.; Esteves, S.C. The novel POSEIDON stratification of ‘Low prognosis patients in Assisted Reproductive Technology’ and its proposed marker of successful outcome. F1000 Res. 2016, 5, 2911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youssef, M.A.; van Wely, M.; Al-Inany, H.; Madani, T.; Jahangiri, N.; Khodabakhshi, S.; Alhalabi, M.; Akhondi, M.; Ansaripour, S.; Tokhmechy, R.; et al. A mild ovarian stimulation strategy in women with poor ovarian reserve undergoing IVF: A multicenter randomized non-inferiority trial. Hum. Reprod. 2017, 32, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Su, R.; Wu, Y. Cumulative live birth rate and cost-effectiveness analysis of gonadotropin releasing hormone-antagonist protocol and multiple minimal ovarian stimulation in poor responders. Front. Endocrinol. 2020, 11, 605939. [Google Scholar] [CrossRef]
- Lolis, D.E.; Tsolas, O.; Messinis, I.E. The follicle-stimulating hormone threshold level for follicle maturation in superovulated cycles. Fertil. Steril. 1995, 63, 1272–1277. [Google Scholar] [CrossRef]
- Nargund, G.; Fauser, B.C.J.M. Mild ovarian stimulation for IVF is the smartest way forward. Reprod. BioMed. Online 2020, 41, 569–571. [Google Scholar] [CrossRef]
- Berkkanoglu, M.; Ozgur, K. What is the optimum maximal gonadotropin dosage used in microdose flare-up cycles in poor responders? Fertil. Steril. 2010, 94, 662–665. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Kuo, H.-C.; Hsu, C.-T.; Gu, Q. The absorption and uptake of recombinant human follicle-stimulating hormone through vaginal subcutaneous injections–A pharmacokinetic study. Reprod. Biol. Endocrinol. 2009, 7, 107. [Google Scholar] [CrossRef] [Green Version]
- Voortman, G.; Post, J.; van de Schoemaker, R.C.; van Gerven, J.M.A. Bioequivalence of subcutaneous injections of recombinant human follicle stimulating hormone (Puregon) by Pen-injector and syringe. Hum. Reprod. 1999, 14, 1698–1702. [Google Scholar] [CrossRef] [Green Version]
- Biasoni, V.; Patriarca, A.; Dalmasso, P.; Bertagna, A.; Manieri, C.; Benedetto, C.; Revelli, A. Ovarian sensitivity index is strongly related to circulating AMH and may be used to predict ovarian response to exogenous gonadotropins in IVF. Reprod. Biol. Endocrinol. 2011, 9, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alviggi, C.; Conforti, A.; Esteves, S.C.; Vallone, R.; Venturella, R.; Staiano, S.; Castaldo, E.; Andersen, C.Y.; De Placido, G. Understanding ovarian hypo-response to exogenous gonadotropin in ovarian stimulation and its new proposed marker—The follicle-to-oocyte (FOI) index. Front. Endocrinol. 2018, 9, 589. [Google Scholar] [CrossRef]
- Zachow, R.J.; Ramski, B.E.; Lee, H. Modulation of estrogen production and 17beta-hydroxysteroid dehydrogenase-type 1, cytochrome P450 aromatase, c-met, and protein kinase Balpha messenger ribonucleic acid content in rat ovarian granulosa cells by hepatocyte growth factor and follicle-stimulating hormone. Biol. Reprod. 2000, 62, 1851–1857. [Google Scholar] [PubMed] [Green Version]
- Lauson, H.; Heller, C.G.; Golden, J.; Sevringhaus, E. The immature rat uterus in the assay of estrogenic substances, and a comparison of estradiol, estrone and estriol12¹². Endocrinology 1939, 24, 35–44. [Google Scholar] [CrossRef]
- Stevenson, P.M.; Loraine, J.A. Pituitary gonadotropins--chemistry, extraction, and immunoassay. Adv. Clin. Chem 1971, 14, 1–63. [Google Scholar]
- Carson, D.D.; Bagchi, I.; Dey, S.K.; Enders, A.C.; Fazleabas, A.T.; Lessey, B.A.; Yoshinaga, K. Embryo implantation. Dev. Biol. 2000, 223, 217–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagchi, I.C.; Li, Q.; Cheon, Y.P.; Mantena, S.R.; Kannan, A.; Bagchi, M.K. Use of the progesterone receptor antagonist RU 486 to identify novel progesterone receptor-regulated pathways in implantation. Semin. Reprod. Med. 2005, 23, 38–45. [Google Scholar] [CrossRef]
- Giudice, L.C. Elucidating endometrial function in the post-genomic era. Hum. Reprod. Update 2003, 9, 223–235. [Google Scholar] [CrossRef] [Green Version]
- Lessey, B.A. Endometrial responsiveness to steroid hormones: A moving target. J. Soc. Gynecol. Investig. 2004, 11, 61–62. [Google Scholar] [CrossRef] [PubMed]
- Psychoyos, A. Hormonal control of ovoimplantation. Vitam. Horm. 1973, 31, 201–256. [Google Scholar]
- Huet, Y.M.; Andrews, G.K.; Dey, S.K. Modulation of c-myc protein in the mouse uterus during pregnancy and by steroid hormones. Prog. Clin. Biol. Res. 1989, 294, 401–412. [Google Scholar]
- Graham, J.D.; Clarke, C.L. Physiological action of progesterone in target tissues. Endocr. Rev. 1997, 18, 502–519. [Google Scholar]
- Mulac-Jericevic, B.; Conneely, O.M. Reproductive tissue selective actions of progesterone receptors. Reproduction 2004, 128, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tranguch, S.; Smith, D.F.; Dey, S.K. Progesterone receptor requires a co-chaperone for signalling in uterine biology and implantation. Reprod. Biomed. Online 2006, 13, 651–660. [Google Scholar] [CrossRef]
- Giangrande, P.H.; Kimbrel, E.A.; Edwards, D.P.; McDonnell, D.P. The opposing transcriptional activities of the two isoforms of the human progesterone receptor are due to differential cofactor binding. Mol. Cell. Biol. 2000, 20, 3102–3115. [Google Scholar] [CrossRef] [Green Version]
- Pellicer, A.; Valbuena, D.; Cano, F.; Remohí, J.; Simón, C. Lower implantation rates in high responders: Evidence for an altered endocrine milieu during the preimplantation period. Fertil. Steril. 1996, 65, 1190–1195. [Google Scholar] [CrossRef]
- Simón, C.; Garcia Velasco, J.J.; Valbuena, D.; Peinado, J.A.; Moreno, C.; Remohí, J.; Pellicer, A. Increasing uterine receptivity by decreasing estradiol levels during the preimplantation period in high responders with the use of a follicle-stimulating hormone step-down regimen. Fertil. Steril. 1998, 70, 234–239. [Google Scholar] [CrossRef]
- Ma, W.G.; Song, H.; Das, S.K.; Paria, B.C.; Dey, S.K. Estrogen is a critical determinant that specifies the duration of the window of uterine receptivity for implantation. Proc. Natl. Acad. Sci. USA 2003, 100, 2963–2968. [Google Scholar] [CrossRef] [Green Version]
- Walton, E.A.; Armstrong, D.T. Implantation and later fetal development in immature rats given a superovulatory dose of pregnant mare’s serum gonadotropin, later neutralized by antiserum. Biol. Reprod. 1982, 27, 841–846. [Google Scholar] [CrossRef] [Green Version]
- Ertzeid, G.; Storeng, R. The impact of ovarian stimulation on implantation and fetal development in mice. Hum. Reprod. 2001, 16, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leyva-Gómez, G.; Del Prado-Audelo, M.L.; Ortega-Peña, S.; Mendoza-Muñoz, N.; Urbán-Morlán, Z.; González-Torres, M.; González-Del Carmen, M.; Figueroa-González, G.; Reyes-Hernández, O.D.; Cortés, H. Modifications in vaginal microbiota and their Influence on drug release: Challenges and opportunities. Pharmaceutics 2019, 11, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, N.M.; Sola-Leyva, A.; Saez-Lara, M.J.; Plaza-Diaz, J.; Tubić-Pavlović, A.; Romero, B.; Clavero, A.; Mozas-Moreno, J.; Fontes, J.; Altmäe, S. New opportunities for endometrial health by modifying uterine microbial composition: Present or future? Biomolecules 2020, 10, 593. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.V.; Kafka, J.K.; Ferreira, V.H.; Roth, K.; Kaushic, C. Innate and adaptive immune responses in male and female reproductive tracts in homeostasis and following HIV infection. Cell. Mol. Immunol. 2014, 11, 410–427. [Google Scholar] [CrossRef] [Green Version]
- Benner, M.; Ferwerda, G.; Joosten, I.; van der Molen, R.G. How uterine microbiota might be responsible for a receptive, fertile endometrium. Hum. Reprod. Update 2018, 24, 393–415. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Song, X.; Wei, W.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [Green Version]
- Mannaerts, B.; Uilenbroek, J.; Schot, P.; De Leeuw, R. Folliculogenesis in hypophysectomized rats after treatment with recombinant human follicle-stimulating hormone. Biol. Reprod. 1994, 51, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Osman, P. Rate and course of atresia during follicular development in the adult cyclic rat. J. Reprod. Fertil. 1985, 73, 261–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.; Garverick, H.A.; Smith, G.W.; Smith, M.F.; Hamilton, S.A.; Youngquist, R.S. Expression of follicle-stimulating hormone and luteinizing hormone receptor messenger ribonucleic acids in bovine follicles during the first follicular wave. Biol. Reprod. 1995, 53, 951–957. [Google Scholar] [CrossRef] [Green Version]
- Bao, B.; Kumar, N.; Karp, R.M.; Garverick, H.A.; Sundaram, K. Estrogen receptor-beta expression in relation to the expression of luteinizing hormone receptor and cytochrome P450 enzymes in rat ovarian follicles. Biol. Reprod. 2000, 63, 1747–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, B.; Calder, M.D.; Xie, S.; Smith, M.F.; Salfen, B.E.; Youngquist, R.S.; Garverick, H.A. Expression of steroidogenic acute regulatory protein messenger ribonucleic acid is limited to theca of healthy bovine follicles collected during recruitment, selection, and dominance of follicles of the first follicular wave. Biol. Reprod. 1998, 59, 953–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abdominal Administration Conventional SC (n = 45) | Vaginal Administration (n = 45) | t | p Value | |
|---|---|---|---|---|
| Characteristics | Mean ± SD | Mean ± SD | ||
| Age (years) | 38.24 ± 3.37 | 39.09 ± 3.94 | 1.092 | 0.278 |
| BMI (kg/m2) | 23.58 ± 3.30 | 22.55 ± 3.54 | −1.435 | 0.155 |
| Serum hormone levels and ovarian follicle counts at baseline (Day 2) | ||||
| AMH (ng/mL) | 0.80 ± 0.32 | 0.72 ± 0.37 | −1.087 | 0.280 |
| FSH (IU/L) | 7.97 ± 6.59 | 10.20 ± 7.76 | 1.414 | 0.161 |
| Estradiol (pg/mL) | 19.88 ± 17.01 | 16.53 ± 8.83 | −1.051 | 0.297 |
| Luteinizing hormone (IU/L) | 1.48 ± 1.34 | 1.47 ± 1.50 | −0.027 | 0.978 |
| Progesterone (ng/mL) | 0.66 ± 0.43 | 0.66 ± 0.26 | −0.049 | 0.961 |
| AFC_baseline (number) | 4.86 ± 2.50 | 3.77 ± 1.91 | −1.900 | 0.062 |
| Total gonadotropin dose (IU) | 2905.43 ± 967.40 | 2014.77 ± 489.16 | −5.473 | <0.001 * |
| Serum hormone levels and ovarian follicle counts on day of ovulation triggering by hCG | ||||
| Estradiol (pg/mL) | 543.87 ± 365.60 | 390.44 ± 363.25 | −1.963 | 0.053 |
| Luteinizing hormone (IU/L) | 2.61 ± 5.77 | 2.49 ± 4.32 | −0.100 | 0.921 |
| Progesterone (ng/mL) | 1.07 ± 0.47 | 1.65 ± 1.85 | 1.807 | 0.078 |
| Ovarian follicle count | ||||
| Follicles < 12 mm (number) | 0.93 ± 0.96 | 1.00 ± 1.04 | 0.315 | 0.754 |
| Follicles ≥ 12 and <16 mm (number) | 1.56 ± 1.50 | 1.78 ± 1.65 | −0.049 | 0.961 |
| Follicles ≥ 16 mm (number) | 2.83 ± 2.51 | 2.24 ± 3.45 | 0.668 | 0.506 |
| Follicles < 12 mm/total follicles (%) | 19.76 ± 18.87 | 22.52 ± 22.05 | 0.633 | 0.528 |
| Follicles ≥ 12 and <16 mm/total follicles (%) | 29.17 ± 22.34 | 37.61 ± 24.78 | 1.172 | 0.243 |
| Follicles ≥ 16 mm/total follicles (%) | 48.87 ± 23.01 | 43.27 ± 22.95 | −1.225 | 0.107 |
| Oocytes retrieved | ||||
| Total oocytes (number) | 5.33 ± 3.39 | 4.67 ± 4.48 | −1.051 | 0.297 |
| Mature oocytes (number) | 4.59 ± 3.29 | 3.70 ± 4.33 | −1.435 | 0.160 |
| Mature oocytes/total oocytes (%) | 83.28 ± 17.09 | 77.54 ± 24.49 | −1.265 | 0.210 |
| OSI (IU) | 755.3 ± 639.9 | 768.7 ± 532.6 | −0.108 | 0.6541 |
| FORT (%) | 58.39 ± 26.62 | 60.8 ± 26.17 | −0.431 | 0.5687 |
| FOI (%) | 82.86 ± 32.73 | 86.41 ± 27.13 | −0.561 | 0.1613 |
| Endometrial thickness (mm) | 8.95 ± 1.97 | 8.78 ± 2.00 | −0.385 | 0.701 |
| UABF _R-PI | 1.99 ± 0.80 | 1.97 ± 0.68 | −0.109 | 0.913 |
| UABF _R-RI | 0.79 ± 0.18 | 0.83 ± 0.10 | 1.104 | 0.274 |
| UABF _L-PI | 2.25 ± 0.94 | 2.21 ± 0.82 | −0.181 | 0.857 |
| UABF _L-RI | 0.85 ± 0.12 | 0.89 ± 0.19 | 0.931 | 0.355 |
| Fresh ET_number | 1.43 ± 0.63 | 1.48 ± 0.55 | −0.411 | 0.507 |
| Pregnancy n, (%;/case had ET) | 7 (24.1%; 7/29) | 10 (24.4%; 10/41) | - | 0.909 |
| Abdominal Administration (n = 10) | Vaginal Administration (n = 10) | t | p Value | |
|---|---|---|---|---|
| Characteristics | Mean ± SD | Mean ± SD | ||
| Age (years) | 31.2 ± 7.3 | - | ||
| BMI (kg/m2) | 19.4 ± 2.1 | - | ||
| Pharmacokinetic parameters of FSH determined from serum samples | ||||
| Tmax (h) | 14.97 ± 8.65 | 5.31 ± 3.52 | −3.106 | 0.013 * |
| Cmax (IU/L) | 13.02 ± 1.56 | 15.77 ± 4.33 | 1.827 | 0.101 |
| AUC (IU×h/L) | 1104.85 ± 227.16 | 1723.57 ± 595.46 | 3.171 | 0.011 * |
| CL/F (L/h) | 0.28 ± 0.04 | 0.19 ± 0.06 | −4.208 | 0.002 * |
| V/F (L) | 16.89 ± 4.80 | 18.59 ± 3.96 | 1.184 | 0.267 |
| K01 (h−1) | 0.64 ± 1.55 | 1.75 ± 2.27 | 1.174 | 0.271 |
| T1/2_absorption (h) | 8.06 ± 9.60 | 1.42 ± 1.11 | −2.072 | 0.068 |
| K10 (h−1) | 0.02 ± 0.00 | 0.01 ± 0.00 | −6.843 | <0.001 * |
| T1/2_elimination (h) | 41.26 ± 8.10 | 69.99 ± 13.67 | 6.416 | <0.001 * |
| Pharmacokinetic parameters of FSH determined from urine samples | ||||
| MRT last_urine (h) | 132.00 ±101.98 | 124.80 ± 86.01 | −0.270 | 0.787 |
| AUC_urine (IU × h/L) | 1160.34 ± 841.76 | 1072.64 ± 861.38 | −0.151 | 0.880 |
| Cumulative elimination dose_urine (IU) | 46.74 ± 32.48 | 38.83 ± 30.94 | −0.756 | 0.450 |
| Percentage of cumulative elimination dose_urine (Cumulative elimination dose/300 IU × 100%) | 15.58 ± 10.83 | 12.94 ± 10.31 | −0.756 | 0.450 |
| Cl_urine(L/h) | 0.05 ± 0.04 | 0.05 ± 0.03 | −0.454 | 0.650 |
| Group | G1 | G2 | G3 | G4 | G5 | Statistical Analysis | |
|---|---|---|---|---|---|---|---|
| Site | abdominal | vaginal | abdominal | vaginal | |||
| Unit | 0 IU (n = 8) | 1 IU (n = 9) | 1 IU (n = 9) | 4 IU (n = 9) | 4 IU (n = 9) | ||
| Mean ± S.E.M | Mean ± S.E.M | Mean ± S.E.M | Mean ± S.E.M | Mean ± S.E.M | p value | post hoc | |
| Parameters of uterine horns | |||||||
| Diameter of the uterus (μm) | 1314.71 ± 82.18 | 1344.13 ± 132.88 | 1520.88 ± 85.19 | 1577.00 ± 93.89 | 1618.89 ± 113.61 | 0.162 | - |
| Folding of the endometrial layer(μm) | 2822.00 ± 190.39 | 3654.13 ± 775.06 | 4295.75 ± 724.88 | 3591.22 ± 559.06 | 3812.11 ± 701.09 | 0.769 | - |
| Height of epithelial cell layer of the endometrium(μm) | 12.77 ± 0.52 | 20.60 ± 3.12 | 19.30 ± 2.36 | 20.27 ± 2.07 | 23.76 ± 3.26 | 0.017 * | G1 < G2, G1 < G3, G1 < G4, G1 < G5 |
| Total area of the uterus (μm2) | 1258,524.14 ± 133,695.87 | 1298,781.75 ± 248,034.88 | 1599,036.38 ± 222,079.93 | 1660,589.89 ± 185,274.63 | 1880,074.33 ± 234,992.75 | 0.274 | - |
| Area of the endometrial layer (μm2) | 552,151.43 ± 53,531.43 | 561,074.75 ± 77,514.61 | 706,550.50 ± 69,589.57 | 611,389.89 ± 73,587.71 | 794,114.11 ± 119,099.95 | 0.268 | - |
| Number of follicles of each class | |||||||
| Class I | 8.6 ± 0.9 | 15.2 ± 0.9 | 12.7 ± 1.3 | 10.9 ± 1.2 | 13.4 ± 1.1 | 0.007 * | G1 < G2, G1 < G3, G1 < G5, G4 < G2 |
| Class II | 6.7 ± 1.0 | 5.8 ± 0.9 | 6.4 ± 1.0 | 4.3 ± 0.8 | 6.7 ± 1.6 | 0.493 | - |
| Class III | 0.7 ± 0.3 | 0.4 ± 0.2 | 0.3 ± 0.1 | 0.2 ± 0.2 | 1.4 ± 0.7 | 0.472 | - |
| Total number of follicles | 16.1 ± 0.9 | 21.9 ± 1.3 | 20.4 ± 1.7 | 18.8 ± 1.7 | 23.3 ± 2.7 | 0.041 * | G1 < G2, G1 < G3, G1 < G5, |
| Corpus luteum | 0.0 ± 0.0 | 0.4 ± 0.4 | 1.0 ± 0.8 | 3.3 ± 1.1 | 1.8 ± 0.9 | 0.064 | G1 < G4 |
| Class III + corpus luteum | 0.8 ± 0.3 | 0.9 ± 0.6 | 1.3 ± 0.9 | 3.6 ± 1.2 | 3.2 ± 0.9 | 0.220 | - |
| Hormone analysis | |||||||
| Progesterone (ng/mL) | 9.50 ± 1.38 | 6.35 ± 0.64 | 13.30 ± 3.42 | 30.54 ± 5.14 | 27.09 ± 5.33 | 0.004 * | G1 < G4, G1 < G5, G2 < G4, G2 < G5, G3 < G4 |
| Estradiol (pg/mL) | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.999 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-C.; Hsu, L.; Hsueh, Y.-S.; Lin, C.-Y.; Chang, H.H.; Hsu, C.-T. Ovarian Folliculogenesis and Uterine Endometrial Receptivity after Intermittent Vaginal Injection of Recombinant Human Follicle-Stimulating Hormone in Infertile Women Receiving In Vitro Fertilization and in Immature Female Rats. Int. J. Mol. Sci. 2021, 22, 10769. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910769
Hsu C-C, Hsu L, Hsueh Y-S, Lin C-Y, Chang HH, Hsu C-T. Ovarian Folliculogenesis and Uterine Endometrial Receptivity after Intermittent Vaginal Injection of Recombinant Human Follicle-Stimulating Hormone in Infertile Women Receiving In Vitro Fertilization and in Immature Female Rats. International Journal of Molecular Sciences. 2021; 22(19):10769. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910769
Chicago/Turabian StyleHsu, Chao-Chin, Leonard Hsu, Yuan-Shuo Hsueh, Chih-Ying Lin, Hui Hua Chang, and Chao-Tien Hsu. 2021. "Ovarian Folliculogenesis and Uterine Endometrial Receptivity after Intermittent Vaginal Injection of Recombinant Human Follicle-Stimulating Hormone in Infertile Women Receiving In Vitro Fertilization and in Immature Female Rats" International Journal of Molecular Sciences 22, no. 19: 10769. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910769