
Blood-Based Immune Profiling Combined with Machine Learning Discriminates Psoriatic Arthritis from Psoriasis Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Population
2.2. Differences in Immune Cell Subsets between PsA and Pso
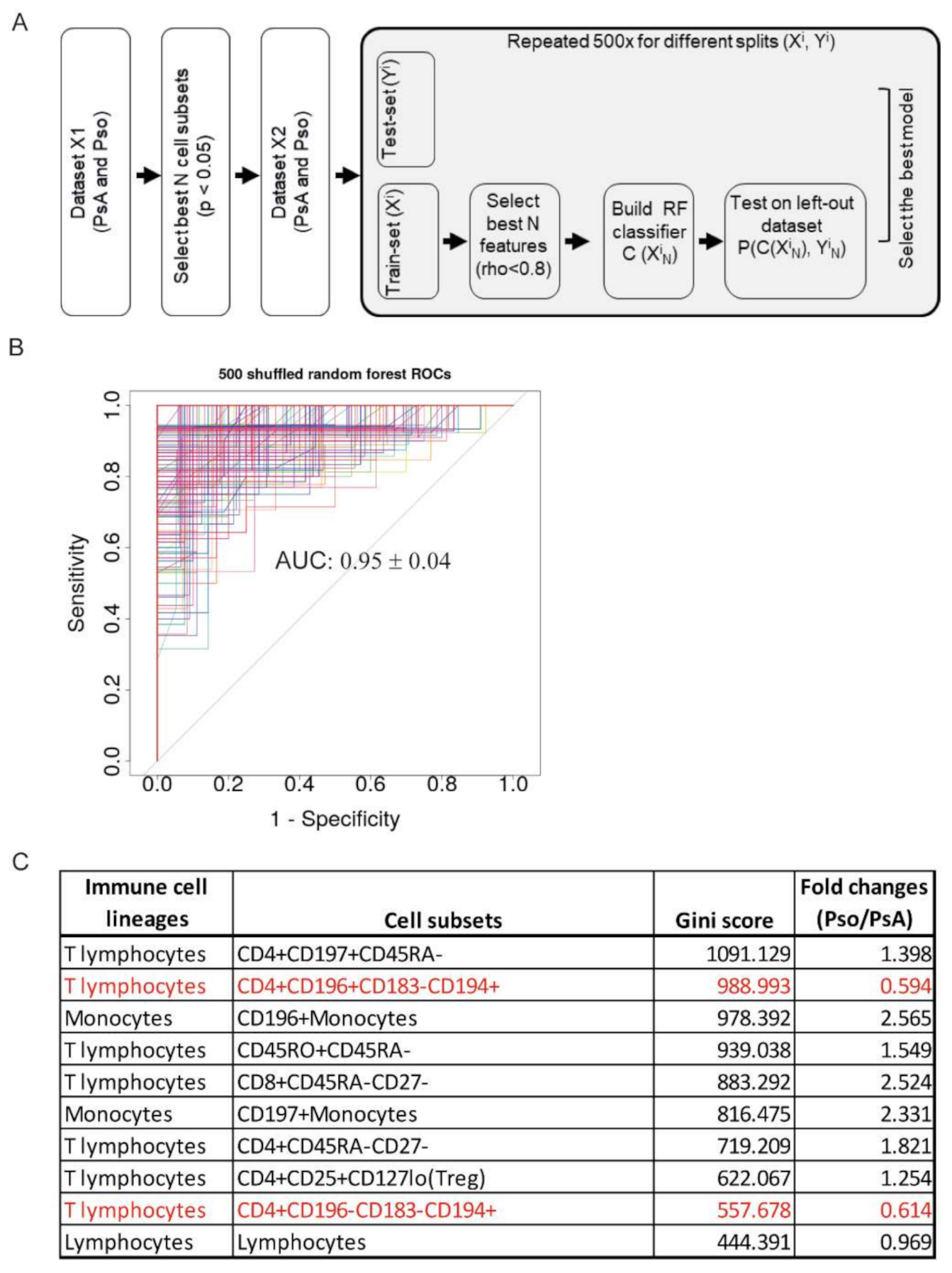
2.3. Random Forest Classification Model Reveals a Disease-Specific Immune Profile
2.4. Association of the PsA-Specific Immune Profile with Clinical Parameters
3. Discussion
4. Materials and Methods
4.1. Patients and Setting
4.2. Experimental Procedure
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Invest. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHugh, N.J.; Balachrishnan, C.; Jones, S.M. Progression of peripheral joint disease in psoriatic arthritis: A 5-yr prospective study. Rheumatology 2003, 42, 778–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mease, P.J.; Gladman, D.D.; Papp, K.A.; Khraishi, M.M.; Thaci, D.; Behrens, F.; Northington, R.; Fuiman, J.; Bananis, E.; Boggs, R.; et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J. Am. Acad. Dermato.l 2013, 69, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.F.; Mussani, F.; Chandran, V.; Eder, L.; Thavaneswaran, A.; Gladman, D.D. Patients with psoriatic arthritis have worse quality of life than those with psoriasis alone. Rheumatology 2012, 51, 571–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haroon, M.; Gallagher, P.; FitzGerald, O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann. Rheum. Dis. 2015, 74, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Abji, F.; Pollock, R.A.; Liang, K.; Chandran, V.; Gladman, D.D. Brief Report: CXCL10 Is a Possible Biomarker for the Development of Psoriatic Arthritis Among Patients with Psoriasis. Arthritis Rheumatol. 2016, 68, 2911–2916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadon, D.R.; Sengupta, R.; Nightingale, A.; Lu, H.; Dunphy, J.; Green, A.; Elder, J.T.; Nair, R.P.; Korendowych, E.; Lindsay, M.A.; et al. Serum bone-turnover biomarkers are associated with the occurrence of peripheral and axial arthritis in psoriatic disease: A prospective cross-sectional comparative study. Arthritis Res. Ther. 2017, 19, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diani, M.; Casciano, F.; Marongiu, L.; Longhi, M.; Altomare, A.; Pigatto, P.D.; Secchiero, P.; Gambari, R.; Banfi, G.; Manfredi, A.A.; et al. Increased frequency of activated CD8(+) T cell effectors in patients with psoriatic arthritis. Sci. Rep. 2019, 9, 10870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flytlie, H.A.; Hvid, M.; Lindgreen, E.; Kofod-Olsen, E.; Petersen, E.L.; Jorgensen, A.; Deleuran, M.; Vestergaard, C.; Deleuran, B. Expression of MDC/CCL22 and its receptor CCR4 in rheumatoid arthritis, psoriatic arthritis and osteoarthritis. Cytokine 2010, 49, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Benham, H.; Norris, P.; Goodall, J.; Wechalekar, M.D.; FitzGerald, O.; Szentpetery, A.; Smith, M.; Thomas, R.; Gaston, H. Th17 and Th22 cells in psoriatic arthritis and psoriasis. Arthritis Res. Ther. 2013, 15, R136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, B.; Gullick, N.J.; Walter, G.J.; Rajasekhar, M.; Garrood, T.; Evans, H.G.; Taams, L.S.; Kirkham, B.W. Interleukin-17+CD8+ T cells are enriched in the joints of patients with psoriatic arthritis and correlate with disease activity and joint damage progression. Arthritis Rheumatol. 2014, 66, 1272–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Raemdonck, K.; Umar, S.; Palasiewicz, K.; Volkov, S.; Volin, M.V.; Arami, S.; Chang, H.J.; Zanotti, B.; Sweiss, N.; Shahrara, S. CCL21/CCR7 signaling in macrophages promotes joint inflammation and Th17-mediated osteoclast formation in rheumatoid arthritis. Cell. Mol. Life Sci. 2020, 77, 1387–1399. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.P.; Zhang, H.H.; Borek, I.; Wolf, P.; Hedrick, M.N.; Singh, S.P.; Kelsall, B.L.; Clausen, B.E.; Farber, J.M. Monocyte-derived inflammatory Langerhans cells and dermal dendritic cells mediate psoriasis-like inflammation. Nat. Commun. 2016, 7, 13581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnitte, S.; Fuchs, A.; Funk, T.; Pecher, A.C.; Dörfel, D.; Henes, J. FRI0015/PHENOTYPE and function of the peripheral blood dendritic cells of psoriasis patients with and without arthritis. Ann. Rheum. Dis. 2020, 79, 578–579. [Google Scholar] [CrossRef]
- Tillett, W.; Charlton, R.; Nightingale, A.; Snowball, J.; Green, A.; Smith, C.; Shaddick, G.; McHugh, N. Interval between onset of psoriasis and psoriatic arthritis comparing the UK Clinical Practice Research Datalink with a hospital-based cohort. Rheumatology 2017, 56, 2109–2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Wijer, L.; van der Heijden, W.A.; Ter Horst, R.; Jaeger, M.; Trypsteen, W.; Rutsaert, S.; van Cranenbroek, B.; van Rijssen, E.; Joosten, I.; Joosten, L.; et al. The Architecture of Circulating Immune Cells Is Dysregulated in People Living with HIV on Long Term Antiretroviral Treatment and Relates with Markers of the HIV-1 Reservoir, Cytomegalovirus, and Microbial Translocation. Front. Immunol. 2021, 12, 661990. [Google Scholar] [CrossRef] [PubMed]
- Ter Horst, R.; Jaeger, M.; van de Wijer, L.; van der Heijden, W.A.; Janssen, A.M.W.; Smeekens, S.P.; Brouwer, M.A.E.; van Cranenbroek, B.; Aguirre-Gamboa, R.; Netea-Maier, R.T.; et al. Seasonal and Nonseasonal Longitudinal Variation of Immune Function. J. Immunol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Leijten, E.F.A.; Sigurdsson, V.; Wenink, M.H.; Radstake, T. Screening for psoriatic arthritis using the Psoriasis Epidemiology Screening Tool questionnaire: Examining the optimal cut-off. Br. J. Dermatol. 2017, 176, 1357–1359. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Gamboa, R.; Joosten, I.; Urbano, P.C.M.; van der Molen, R.G.; van Rijssen, E.; van Cranenbroek, B.; Oosting, M.; Smeekens, S.; Jaeger, M.; Zorro, M.; et al. Differential Effects of Environmental and Genetic Factors on T and B Cell Immune Traits. Cell Rep. 2016, 17, 2474–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PsA (N = 41) | Pso (N = 45) | |
|---|---|---|
| Age (years) | 56.1 ± 14.5 | 44.1 ± 15.2 |
| Female (number, %) | 22 (53.7%) | 20 (44.4%) |
| BMI | 27.0 ± 5.1 # | 29.2 ± 5.4 # |
| cDMARD (current use) | 17 (41.5%) | 4 (8.7%) |
| bDMARD (current use) | 0 (0%) | 7 (15.6%) |
| CRP | 4.8 ± 10.7 | 3.2 ± 5.0 ## |
| PASI | 2.9 ± 3.7 ### | 13.3 ± 7.3 |
| DAS28 | 2.4 ± 1.3 | - |
| PASDAS | 4.9 ± 1.1 ### | - |
| TJC28 | 2.2 ± 3.6 | - |
| TJC68 | 7.2 ± 5.8 ### | - |
| SJC28 | 1.8 ± 3.5 | - |
| SJC66 | 5.8 ± 6.4### | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulder, M.L.M.; He, X.; van den Reek, J.M.P.A.; Urbano, P.C.M.; Kaffa, C.; Wang, X.; van Cranenbroek, B.; van Rijssen, E.; van den Hoogen, F.H.J.; Joosten, I.; et al. Blood-Based Immune Profiling Combined with Machine Learning Discriminates Psoriatic Arthritis from Psoriasis Patients. Int. J. Mol. Sci. 2021, 22, 10990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010990
Mulder MLM, He X, van den Reek JMPA, Urbano PCM, Kaffa C, Wang X, van Cranenbroek B, van Rijssen E, van den Hoogen FHJ, Joosten I, et al. Blood-Based Immune Profiling Combined with Machine Learning Discriminates Psoriatic Arthritis from Psoriasis Patients. International Journal of Molecular Sciences. 2021; 22(20):10990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010990
Chicago/Turabian StyleMulder, Michelle L. M., Xuehui He, Juul M. P. A. van den Reek, Paulo C. M. Urbano, Charlotte Kaffa, Xinhui Wang, Bram van Cranenbroek, Esther van Rijssen, Frank H. J. van den Hoogen, Irma Joosten, and et al. 2021. "Blood-Based Immune Profiling Combined with Machine Learning Discriminates Psoriatic Arthritis from Psoriasis Patients" International Journal of Molecular Sciences 22, no. 20: 10990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010990