
Prognostic Value of BUB1 for Predicting Non-Muscle-Invasive Bladder Cancer Progression

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Screening Test
2.1.1. Transcriptome Profiles in Patients with NMIBC
2.1.2. Comparison of DEGs in Two Different Cohorts
2.2. Training Test
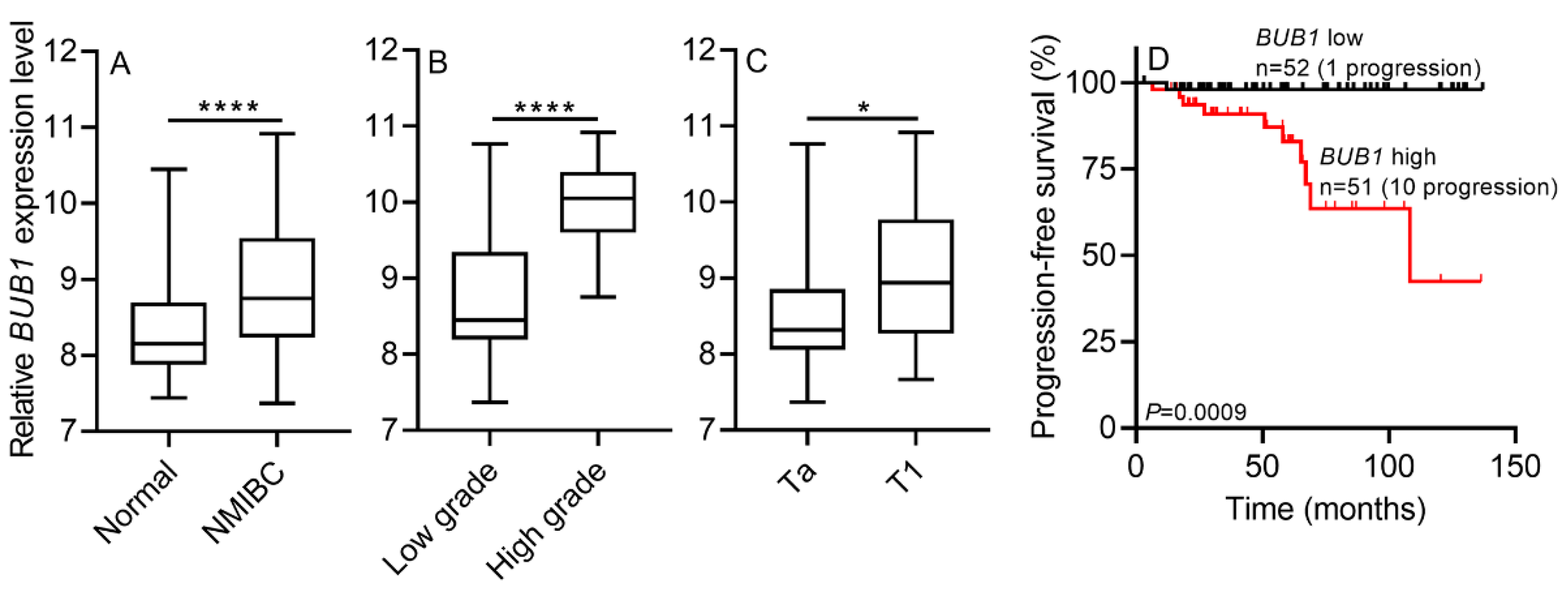
2.2.1. BUB1 mRNA Expression in NMIBC Tissues
2.2.2. BUB1 mRNA Expression Correlates with NMIBC Prognosis
2.3. Validation Test
2.3.1. BUB1 mRNA Expression in the GSE13507 Dataset: Internal Validation
2.3.2. BUB1 mRNA Expression in the E-MTAT-4321 Dataset: External Validation
2.4. BUB1 Inhibits G2/M Cell Cycle Arrest in Human BCa Cells
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jallepalli, P.V.; Lengauer, C. Chromosome segregation and cancer: Cutting through the mystery. Nat. Rev. Cancer 2001, 1, 109–117. [Google Scholar] [CrossRef]
- Lengauer, C.; Kinzler, K.W.; Vogelstein, B. Genetic instabilities in human cancers. Nature 1998, 396, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Masuda, A.; Takahashi, T. Chromosome instability in human lung cancers: Possible underlying mechanisms and potential consequences in the pathogenesis. Oncogene 2002, 21, 6884–6897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kops, G.J.; Weaver, B.A.; Cleveland, D.W. On the road to cancer: Aneuploidy and the mitotic checkpoint. Nat. Rev. Cancer 2005, 5, 773–785. [Google Scholar] [CrossRef]
- Bolanos-Garcia, V.M.; Blundell, T.L. BUB1 and BUBR1: Multifaceted kinases of the cell cycle. Trends Biochem. Sci. 2011, 36, 141–150. [Google Scholar] [CrossRef] [Green Version]
- King, R.W. When 2 + 2 = 5: The origins and fates of aneuploid and tetraploid cells. Biochim. Biophys. Acta 2008, 1786, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.Y.; Han, Y.K.; Park, G.-Y.; Kim, S.D.; Lee, C.G. Bub1 is required for maintaining cancer stem cells in breast cancer cell lines. Sci. Rep. 2015, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Katsaros, D.; Shen, Y.; Fu, Y.; Canuto, E.M.; Benedetto, C.; Lu, L.; Chu, W.-M.; Risch, H.A.; Yu, H. Biological and clinical significance of MAD2L1 and BUB1, genes frequently appearing in expression signatures for breast cancer prognosis. PLoS ONE 2015, 10, e0136246. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.J.; Pan, Y.; Chen, X.Y.; Hou, P.F. BUB1 promotes proliferation of liver cancer cells by activating SMAD2 phosphorylation. Oncol. Lett. 2020, 19, 3506–3512. [Google Scholar] [CrossRef]
- Peng, X.; Wang, J.; Li, D.; Chen, X.; Liu, K.; Zhang, C.; Lai, Y. Identification of grade-related genes and construction of a robust genomic-clinicopathologic nomogram for predicting recurrence of bladder cancer. Medicine 2020, 99, e23179. [Google Scholar] [CrossRef]
- Cancer Statistics. Available online: https://www.cancer.gov/about-cancer/understanding/statistics (accessed on 25 September 2020).
- Bryan, R.T.; Collins, S.I.; Daykin, M.C.; Zeegers, M.P.; Cheng, K.K.; Wallace, D.M.A.; Sole, G.M. Mechanisms of recurrence of Ta/T1 bladder cancer. Ann. R. Coll. Surg. Engl. 2010, 92, 519–524. [Google Scholar] [CrossRef] [Green Version]
- Van Lingen, A.V.; Arends, T.J.; Witjes, J.A. Expert review, an update in current and developing intravesical therapies for non-muscle-invasive bladder cancer. Expert Rev. Anticancer Ther. 2013, 13, 1257–1268. [Google Scholar] [CrossRef]
- Zagouri, F.; Peroukidis, S.; Tzannis, K.; Kouloulias, V.; Bamias, A. Current clinical practice guidelines on chemotherapy and radiotherapy for the treatment of non-metastatic muscle-invasive urothelial cancer: A systematic review and critical evaluation by the Hellenic Genito-Urinary Cancer Group (HGUCG). Crit. Rev. Oncol. Hematol. 2015, 93, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Böhle, A.; Burger, M.; Compérat, E.; Kaasinen, E.; Palou, J. EAU Guidelines on Non-Muscle Invasive (Ta, T1, CIS) Bladder Cancer; EAU Guidel. Edn. presented at the EAU Annual Congress Amsterdam 2020; EAU Guidelines Office: Arnhem, The Netherlands, 2020; ISBN 978-94-92671-07-3. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 23 November 2021).
- Van Rhijn, B.W. Combining molecular and pathologic data to prognosticate non-muscle-invasive bladder cancer. Urol. Oncol. 2012, 30, 518–523. [Google Scholar] [CrossRef]
- Shi, R.; Bao, X.; Rogowski, P.; Schäfer, C.; Schmidt-Hegemann, N.-S.; Unger, K.; Lu, S.; Sun, J.; Buchner, A.; Stief, C. Establishment and Validation of an Individualized Cell Cycle Process-Related Gene Signature to Predict Cancer-Specific Survival in Patients with Bladder Cancer. Cancers 2020, 12, 1146. [Google Scholar] [CrossRef]
- Babjuk, P.M.; Definition of Very High-Risk and Refractory NMIBC. Plenary Session 03—Challenges Across the Spectrum of Bladder Cancer. Available online: https://www.urotoday.com/conference-highlights/eau-2020/bladder-cancer/123158-eau-2020-definition-of-very-high-risk-and-refractory-non-muscle-invasive-bladder-cancer.html (accessed on 18 July 2020).
- Otto, T.; Sicinski, P. Cell cycle proteins as promising targets in cancer therapy. Nat. Rev. Cancer 2017, 17, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeggo, P.A.; Pearl, L.H.; Carr, A.M. DNA repair, genome stability and cancer: A historical perspective. Nat. Rev. Cancer 2016, 16, 35. [Google Scholar] [CrossRef] [Green Version]
- Ricke, R.M.; van Ree, J.H.; van Deursen, J.M. Whole chromosome instability and cancer: A complex relationship. Trends Genet. 2008, 24, 457–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-David, U.; Amon, A. Context is everything: Aneuploidy in cancer. Nat. Rev. Genet. 2020, 21, 44–62. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.J.; Cleveland, D.W. Boveri revisited: Chromosomal instability, aneuploidy and tumorigenesis. Nat. Rev. Mol. Cell Biol. 2009, 10, 478–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schvartzman, J.-M.; Sotillo, R.; Benezra, R. Mitotic chromosomal instability and cancer: Mouse modelling of the human disease. Nat. Rev. Cancer 2010, 10, 102–115. [Google Scholar] [CrossRef] [Green Version]
- Ricke, R.M.; Jeganathan, K.B.; van Deursen, J.M. Bub1 overexpression induces aneuploidy and tumor formation through Aurora B kinase hyperactivation. J. Cell Biol. 2011, 193, 1049–1064. [Google Scholar]
- Nezi, L.; Musacchio, A. Sister chromatid tension and the spindle assembly checkpoint. Curr. Opin. Cell Biol. 2009, 21, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Shichiri, M.; Yoshinaga, K.; Hisatomi, H.; Sugihara, K.; Hirata, Y. Genetic and epigenetic inactivation of mitotic checkpoint genes hBUB1 and hBUBR1 and their relationship to survival. Cancer Res. 2002, 62, 13–17. [Google Scholar] [PubMed]
- Hempen, P.M.; Kurpad, H.; Calhoun, E.S.; Abraham, S.; Kern, S.E. A double missense variation of the BUB1 gene and a defective mitotic spindle checkpoint in the pancreatic cancer cell line Hs766T. Hum. Mutat. 2003, 21, 445. [Google Scholar] [PubMed]
- Alizadeh, A.A.; Eisen, M.B.; Davis, R.E.; Ma, C.; Lossos, I.S.; Rosenwald, A.; Boldrick, J.C.; Sabet, H.; Tran, T.; Yu, X. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 2000, 403, 503–511. [Google Scholar]
- Shigeishi, H.; Oue, N.; Kuniyasu, H.; Wakikawa, A.; Yokozaki, H.; Ishikawa, T.; Yasui, W. Expression of Bub1 gene correlates with tumor proliferating activity in human gastric carcinomas. Pathobiology 2001, 69, 24–29. [Google Scholar] [CrossRef]
- Van De Vijver, M.J.; He, Y.D.; Van’t Veer, L.J.; Dai, H.; Hart, A.A.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J. A gene-expression signature as a predictor of survival in breast cancer. N. Engl. J. Med. 2002, 347, 1999–2009. [Google Scholar] [PubMed] [Green Version]
- Piao, J.; Zhu, L.; Sun, J.; Li, N.; Dong, B.; Yang, Y.; Chen, L. High expression of CDK1 and BUB1 predicts poor prognosis of pancreatic ductal adenocarcinoma. Gene 2019, 701, 15–22. [Google Scholar] [CrossRef]
- Li, L.; Xu, D.-B.; Zhao, X.-L.; Hao, T.-Y. Combination analysis of Bub1 and Mad2 expression in endometrial cancer: Act as a prognostic factor in endometrial cancer. Arch. Gynecol. Obstet. 2013, 288, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Fujibayashi, Y.; Isa, R.; Nishiyama, D.; Sakamoto-Inada, N.; Kawasumi, N.; Yamaguchi, J.; Kuwahara-Ota, S.; Matsumura-Kimoto, Y.; Tsukamoto, T.; Chinen, Y. Aberrant BUB1 Overexpression Promotes Mitotic Segregation Errors and Chromosomal Instability in Multiple Myeloma. Cancers 2020, 12, 2206. [Google Scholar]
- Kim, W.J.; Kim, E.J.; Kim, S.K.; Kim, Y.J.; Ha, Y.S.; Jeong, P.; Kim, M.J.; Yun, S.J.; Lee, K.M.; Moon, S.K.; et al. Predictive value of progression-related gene classifier in primary non-muscle invasive bladder cancer. Mol. Cancer 2010, 9, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Univariate Cox Analysis | Multivariate Cox Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age <65 (Ref.) vs. >65 | 1.946 (0.661–5.722) | 0.227 | ||
| Gender Male (Ref.) vs. Female | 1.872 (0.520–6.737) | 0.337 | ||
| Tumor size ≤1 cm (Ref.) vs. 2–3 cm | ||||
| 1.563 (0.476–4.536) | 0.670 | |||
| Multiplicity | ||||
| Single | Ref. | |||
| 2–7 >7 | 1.664 (0.437–6.326) 5.178 (0.890–30.116) | 0.455 0.067 | ||
| 2004 WHO grade Low (Ref.) vs. High | ||||
| 5.808 (2.045–16.493) | 0.001 * | 4.629 (1.593–13.450) | 0.005 * | |
| Stage Ta (Ref.) vs. T1 | ||||
| 0.765 (0.261–2.243) | 0.626 | |||
| BCG No (Ref.) vs. Yes | ||||
| 1.415 (0.474–4.225) | 0.534 | |||
| BUB1 expression Low expression (Ref.) vs. High expression | 6.076 (1.367–27.007) | 0.018 * | 4.642 (1.021–21.097) | 0.047 * |
| BUB1 Expression Low Expression (Ref.) vs. High Expression | Univariate Cox Analysis | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Internal validation cohort a (n = 103) | 15 (1.9–115) | 0.011 * |
| External validation cohort b (n = 450) | 5.7 (2.2–15) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piao, X.-M.; You, C.; Byun, Y.J.; Kang, H.W.; Noh, J.; Lee, J.; Lee, H.Y.; Kim, K.; Kim, W.T.; Yun, S.J.; et al. Prognostic Value of BUB1 for Predicting Non-Muscle-Invasive Bladder Cancer Progression. Int. J. Mol. Sci. 2021, 22, 12756. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312756
Piao X-M, You C, Byun YJ, Kang HW, Noh J, Lee J, Lee HY, Kim K, Kim WT, Yun SJ, et al. Prognostic Value of BUB1 for Predicting Non-Muscle-Invasive Bladder Cancer Progression. International Journal of Molecular Sciences. 2021; 22(23):12756. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312756
Chicago/Turabian StylePiao, Xuan-Mei, Chaelin You, Young Joon Byun, Ho Won Kang, Junho Noh, Jaehyun Lee, Hee Youn Lee, Kyeong Kim, Won Tae Kim, Seok Joong Yun, and et al. 2021. "Prognostic Value of BUB1 for Predicting Non-Muscle-Invasive Bladder Cancer Progression" International Journal of Molecular Sciences 22, no. 23: 12756. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312756