
Mutation Analysis of Radioresistant Early-Stage Cervical Cancer

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Mutation Screening of Stage IB Cervical Tumors
2.2. Investigation of the Effects of the KRASmt/SMAD4mt Signature In Vitro
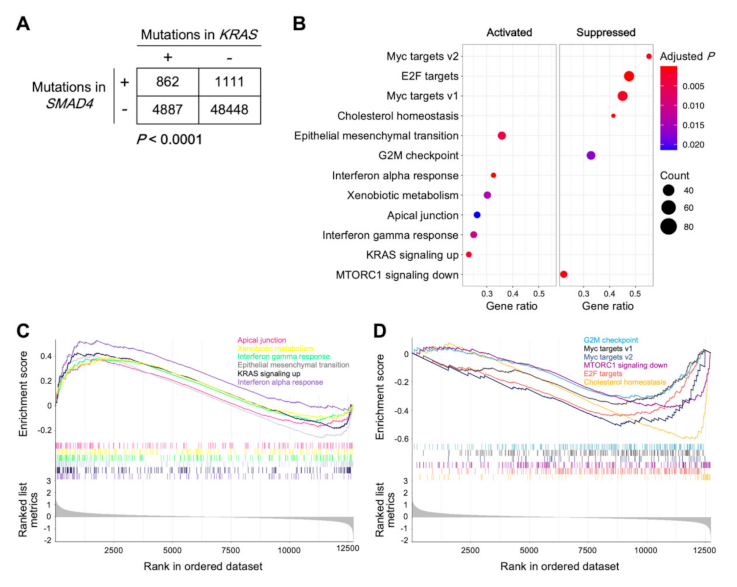
2.3. Gene Set Enrichment Analysis of Tumors Carrying the KRASmt/SMAD4mt Signature
2.4. Sensitivity of Cells Carrying the KRASmt/SMAD4mt Signature to Carbon Ion Radiotherapy
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Identification of Somatic Mutations
4.3. Human Papillomavirus Genotyping
4.4. Mutation Analysis of Data from a Public Database
4.5. Cell Culture
4.6. siRNA Knockdown
4.7. Immunoblotting
4.8. Irradiation
4.9. Clonogenic Assays
4.10. Gene Set Enrichment Analysis
4.11. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N.; ESMO Guidelines Committee. Cervical cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv72–iv83. [Google Scholar] [CrossRef]
- Pötter, R.; Tanderup, K.; Schmid, M.P.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. MRI-guided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I): A multicentre prospective cohort study. Lancet Oncol. 2021, 22, 538–547. [Google Scholar] [CrossRef]
- Suzuki, Y.; Nakano, T.; Ohno, T.; Kato, S.; Niibe, Y.; Morita, S.; Tsujii, H. Oxygenated and reoxygenated tumors show better local control in radiation therapy for cervical cancer. Int. J. Gynecol. Cancer 2006, 16, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Torres-Roca, J.F. A molecular assay of tumor radiosensitivity: A roadmap towards biology-based personalized radiation therapy. Per. Med. 2012, 9, 547–557. [Google Scholar] [CrossRef] [Green Version]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Ojesina, A.I.; Lichtenstein, L.; Freeman, S.S.; Pedamallu, C.S.; Imaz-Rosshandler, I.; Pugh, T.J.; Cherniack, A.D.; Ambrogio, L.; Cibulskis, K.; Bertelsen, B.; et al. Landscape of genomic alterations in cervical carcinomas. Nature 2014, 506, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Integrated genomic and molecular characterization of cervical cancer. Nature 2017, 543, 378–384. [Google Scholar] [CrossRef]
- OncoKB Website. Available online: https://www.oncokb.org/ (accessed on 19 October 2021).
- ClinVar Website. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/clinvar/ (accessed on 19 October 2021).
- cBioPortal Website. Available online: https://www.cbioportal.org/ (accessed on 19 October 2021).
- Sonkin, D.; Hassan, M.; Murphy, D.J.; Tatarinova, T.V. Tumor suppressors status in cancer cell line Encyclopedia. Mol. Oncol. 2013, 7, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Wang, L.G.; Han, Y.; He, Q.Y. clusterProfiler: An R package for comparing biological themes among gene clusters. OMICS 2012, 16, 284–287. [Google Scholar] [CrossRef]
- Ghandi, M.; Huang, F.W.; Jané-Valbuena, J.; Kryukov, G.V.; Lo, C.C.; McDonald, E.R., 3rd; Barretina, J.; Gelfand, E.T.; Bielski, C.M.; Li, H.; et al. Next-generation characterization of the Cancer Cell Line Encyclopedia. Nature 2019, 569, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Durante, M.; Orecchia, R.; Loeffler, J.S. Charged-particle therapy in cancer: Clinical uses and future perspectives. Nat. Rev. Clin. Oncol. 2017, 14, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Nuryadi, E.; Sasaki, Y.; Hagiwara, Y.; Permata, T.B.M.; Sato, H.; Komatsu, S.; Yoshimoto, Y.; Murata, K.; Ando, K.; Kubo, N.; et al. Mutational analysis of uterine cervical cancer that survived multiple rounds of radiotherapy. Oncotarget 2018, 9, 32642–32652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, B.; Guo, J.; Sheng, Y.; Wu, G.; Zhao, Y. Human papillomavirus-negative cervical cancer: A comprehensive review. Front. Oncol. 2021, 10, 606335. [Google Scholar] [CrossRef]
- Gien, L.T.; Beauchemin, M.C.; Thomas, G. Adenocarcinoma: A unique cervical cancer. Gynecol. Oncol. 2010, 116, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Zhang, M.; Zhou, C.; Wang, W.; Yang, H.; Ye, W. The role of epithelial-mesenchymal transition in regulating radioresistance. Crit. Rev. Oncol. Hematol. 2020, 150, 102961. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.W.; Hong, D.W.; Hong, S.H. PB01 suppresses radio-resistance by regulating ATR signaling in human non-small-cell lung cancer cells. Sci. Rep. 2021, 11, 12093. [Google Scholar] [CrossRef]
- Rajput, M.; Singh, R.; Singh, N.; Singh, R.P. EGFR-mediated Rad51 expression potentiates intrinsic resistance in prostate cancer via EMT and DNA repair pathways. Life Sci. 2021, 286, 120031. [Google Scholar] [CrossRef]
- Omabe, K.; Uduituma, S.; Igwe, D.; Omabe, M. Deeper insight in metastatic cancer progression; epithelial-to-mesenchymal transition and genomic instability: Implications on treatment resistance. Curr. Mol. Med. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liermann, J.; Shinoto, M.; Syed, M.; Debus, J.; Herfarth, K.; Naumann, P. Carbon ion radiotherapy in pancreatic cancer: A review of clinical data. Radiother. Oncol. 2020, 147, 145–150. [Google Scholar] [CrossRef]
- Mizoe, J.E.; Hasegawa, A.; Jingu, K.; Takagi, R.; Bessyo, H.; Morikawa, T.; Tonoki, M.; Tsuji, H.; Kamada, T.; Tsujii, H.; et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother. Oncol. 2012, 103, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Matsunobu, A.; Imai, R.; Kamada, T.; Imaizumi, T.; Tsuji, H.; Tsujii, H.; Shioyama, Y.; Honda, H.; Tatezaki, S.; Working Group for Bone and Soft Tissue Sarcomas. Impact of carbon ion radiotherapy for unresectable osteosarcoma of the trunk. Cancer 2012, 118, 4555–4563. [Google Scholar] [CrossRef] [PubMed]
- PTCOG Website. Facilities in Operation. Available online: https://www.ptcog.ch/index.php/facilities-in-operation (accessed on 19 October 2021).
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer: Results from the phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimoto, Y.; Sasaki, Y.; Murata, K.; Noda, S.E.; Miyasaka, Y.; Hamamoto, J.; Furuya, M.; Hirato, J.; Suzuki, Y.; Ohno, T.; et al. Mutation profiling of uterine cervical cancer patients treated with definitive radiotherapy. Gynecol. Oncol. 2020, 159, 546–553. [Google Scholar] [CrossRef] [PubMed]
- The Human Protein Atlas Website. Available online: https://www.proteinatlas.org (accessed on 21 December 2021).
- Ohno, T.; Noda, S.E.; Okonogi, N.; Murata, K.; Shibuya, K.; Kiyohara, H.; Tamaki, T.; Ando, K.; Oike, T.; Ohkubo, Y.; et al. In-room computed tomography-based brachytherapy for uterine cervical cancer: Results of a 5-year retrospective study. J. Radiat. Res. 2017, 58, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, H.; Niimi, A.; Yasuhara, T.; Permata, T.B.M.; Hagiwara, Y.; Isono, M.; Nuryadi, E.; Sekine, R.; Oike, T.; Kakoti, S.; et al. DNA double-strand break repair pathway regulates PD-L1 expression in cancer cells. Nat. Commun. 2017, 8, 1751. [Google Scholar] [CrossRef]
- Shibata, A.; Moiani, D.; Arvai, A.S.; Perry, J.; Harding, S.M.; Genois, M.M.; Maity, R.; van Rossum-Fikkert, S.; Kertokalio, A.; Romoli, F.; et al. DNA double-strand break repair pathway choice is directed by distinct MRE11 nuclease activities. Mol. Cell 2014, 53, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Franken, N.A.; Rodermond, H.M.; Stap, J.; Haveman, J.; van Bree, C. Clonogenic assay of cells in vitro. Nat. Protoc. 2006, 1, 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Oike, T.; Hirota, Y.; Maulany, D.; Darwis, N.; Shibata, A.; Ohno, T. Comparison of clonogenic survival data obtained by pre- and post-irradiation methods. J. Pers. Med. 2020, 10, 171. [Google Scholar] [CrossRef]
- Anakura, M.; Nachankar, A.; Kobayashi, D.; Amornwichet, N.; Hirota, Y.; Shibata, A.; Oike, T.; Nakano, T. Radiosensitivity differences between EGFR mutant and wild-type lung cancer cells are larger at lower doses. Int. J. Mol. Sci. 2019, 20, 3635. [Google Scholar] [CrossRef] [Green Version]
- Kagawa, K.; Murakami, M.; Hishikawa, Y.; Abe, M.; Akagi, T.; Yanou, T.; Kagiya, G.; Furusawa, Y.; Ando, K.; Nojima, K.; et al. Preclinical biological assessment of proton and carbon ion beams at Hyogo Ion Beam Medical Center. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 928–938. [Google Scholar] [CrossRef]
- Kobayashi, D.; Oike, T.; Shibata, A.; Niimi, A.; Kubota, Y.; Sakai, M.; Amornwhichet, N.; Yoshimoto, Y.; Hagiwara, Y.; Kimura, Y.; et al. Mitotic catastrophe is a putative mechanism underlying the weak correlation between sensitivity to carbon ions and cisplatin. Sci. Rep. 2017, 7, 40588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osu, N.; Kobayashi, D.; Shirai, K.; Musha, A.; Sato, H.; Hirota, Y.; Shibata, A.; Oike, T.; Ohno, T. Relative biological effectiveness of carbon ions for head-and-neck squamous cell carcinomas according to human papillomavirus status. J. Pers. Med. 2020, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Cancer Cell Line Encyclopedia Website. Available online: https://sites.broadinstitute.org/ccle/ (accessed on 19 October 2021).
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. Limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Gene Set Enrichment Analysis Website. Available online: http://www.gsea-msigdb.org/gsea/index.jsp (accessed on 19 October 2021).
- Gu, W.; Kim, M.; Wang, L.; Yang, Z.; Nakajima, T.; Tsushima, Y. Multi-omics analysis of ferroptosis regulation patterns and characterization of tumor microenvironment in patients with oral squamous cell carcinoma. Int. J. Biol. Sci. 2021, 17, 3476–3492. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 18) | Case #1 | Case #2 |
|---|---|---|---|
| Follow-up period (months) | 63 (19–124) | 23 | 19 |
| Age (years) | 15 (27–80) | 43 | 64 |
| Histological type | |||
| Squamous | 16 | 1 | |
| Adeno | 2 | 1 | |
| HPV type | |||
| 16 | 8 | 1 | |
| 18 | 2 | ||
| Others | 4 | ||
| Not detected | 4 | 1 | |
| FIGO | |||
| IB1 | 10 | 1 | |
| IB2 | 8 | 1 | |
| Tumor diameter (mm) | |||
| <40 | 10 | 1 | |
| 40–60 | 6 | 1 | |
| >60 | 2 | ||
| Pelvic LN involvement | |||
| Negative | 12 | 1 | 1 |
| Positive | 6 | ||
| PALN involvement | |||
| Negative | 18 | 1 | 1 |
| Positive | 0 | ||
| Concurrent chemotherapy | |||
| Yes | 8 | 1 | |
| No | 10 | 1 |
| Patient | Gene | Mutation | OncoKB | ClinVar | |
|---|---|---|---|---|---|
| Oncogenicity | Function | ||||
| Case #1 | MLH1 | R659* | Likely oncogenic | Likely LoF | Pathogenic |
| FGFR2 | R6P | Unknown | Unknown | Benign | |
| Case #2 | KRAS | G12S | Oncogenic | GoF | Pathogenic |
| SMAD4 | P356L | Predicted oncogenic | Unknown | Not listed | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oike, T.; Sekiguchi, Y.; Yoshimoto, Y.; Oike, T.; Ando, K.; Gu, W.; Sasaki, Y.; Tokino, T.; Iwase, A.; Ohno, T. Mutation Analysis of Radioresistant Early-Stage Cervical Cancer. Int. J. Mol. Sci. 2022, 23, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23010051
Oike T, Sekiguchi Y, Yoshimoto Y, Oike T, Ando K, Gu W, Sasaki Y, Tokino T, Iwase A, Ohno T. Mutation Analysis of Radioresistant Early-Stage Cervical Cancer. International Journal of Molecular Sciences. 2022; 23(1):51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23010051
Chicago/Turabian StyleOike, Tae, Yoshihito Sekiguchi, Yuya Yoshimoto, Takahiro Oike, Ken Ando, Wenchao Gu, Yasushi Sasaki, Takashi Tokino, Akira Iwase, and Tatsuya Ohno. 2022. "Mutation Analysis of Radioresistant Early-Stage Cervical Cancer" International Journal of Molecular Sciences 23, no. 1: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23010051