
The Effectiveness of Antidiabetic Drugs in Treating Dementia: A Peek into Pharmacological and Pharmacokinetic Properties


Abstract
:1. Introduction
2. Association of Pharmacological and Pharmacokinetic Properties of Antidiabetic Drugs with a Protective Effect on Cognitive Function
2.1. The Glucose-Lowering Effect of Antidiabetic Drugs
2.2. Increasing Peripheral Insulin Level via Antidiabetic Drugs
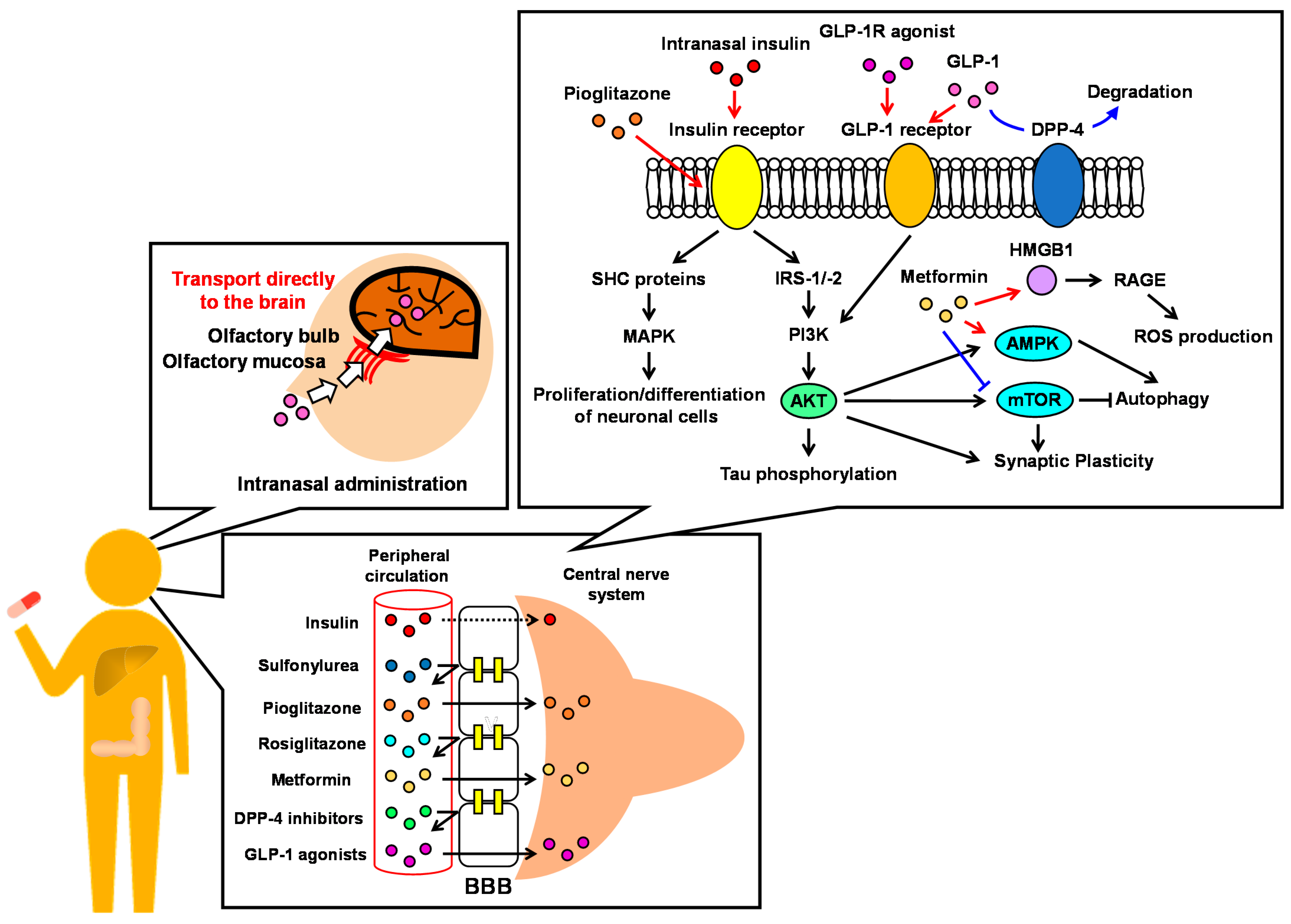
2.3. Intranasal Insulin Administration
2.4. Improvement of Insulin Resistance via Antidiabetic Drugs
2.5. GLP-1 Receptor Agonists
2.6. DPP-4 Inhibitors
2.7. Metformin
2.8. Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors
3. Summary and Future Prospective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Opara, J.A. Activities of Daily Living and Quality of Life in Alzheimer Disease. J. Med. Life 2012, 5, 162–167. [Google Scholar] [PubMed]
- Dhana, K.; Franco, O.H.; Ritz, E.M.; Ford, C.N.; Desai, P.; Krueger, K.R.; Holland, T.M.; Dhana, A.; Liu, X.; Aggarwal, N.T.; et al. Healthy Lifestyle and Life Expectancy with and without Alzheimer’s Dementia: Population Based Cohort Study. BMJ 2022, e068390. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Ott, A.; Slooter, A.J.C.; Hofman, A.; Van Harskamp, F.; Witteman, J.C.M.; Van Broeckhoven, C.; Van Duijn, C.M.; Breteler, M.M.B. Smoking and Risk of Dementia and Alzheimer’s Disease in a Population-Based Cohort Study: The Rotterdam Study. Lancet 1998, 351, 1840–1843. [Google Scholar] [CrossRef]
- Honda, T.; Ohara, T.; Yoshida, D.; Shibata, M.; Ishida, Y.; Furuta, Y.; Oishi, E.; Hirakawa, Y.; Sakata, S.; Hata, J.; et al. Development of a Dementia Prediction Model for Primary Care: The Hisayama Study. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2021, 13, 1–8. [Google Scholar] [CrossRef]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; Dugravot, A.; Akbaraly, T.; Britton, A.; Kivimäki, M.; Singh-Manoux, A. Alcohol Consumption and Risk of Dementia: 23 Year Follow-up of Whitehall II Cohort Study. BMJ 2018, 362. [Google Scholar] [CrossRef] [Green Version]
- Kumari, M.; Brunner, E.; Fuhrer, R. Minireview: Mechanisms by Which the Metabolic Syndrome and Diabetes Impair Memory. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2000, 55, 228–232. [Google Scholar] [CrossRef] [Green Version]
- Elias, M.F.; Wolf, P.A.; D’Agostino, R.B.; Cobb, J.; White, L.R. Untreated Blood Pressure Level Is Inversely Related to Cognitive Functioning: The Framingham Study. Am. J. Epidemiol. 2002, 9, 1. [Google Scholar] [CrossRef]
- Mizuhara, R.; Mitaki, S.; Takamura, M.; Abe, S.; Onoda, K.; Yamaguchi, S.; Nagai, A. Pulse Pressure Is Associated with Cognitive Performance in Japanese Non-Demented Population: A Cross-Sectional Study. BMC Neurol. 2022, 22, 137. [Google Scholar] [CrossRef]
- Xue, M.; Xu, W.; Ou, Y.N.; Cao, X.P.; Tan, M.S.; Tan, L.; Yu, J.T. Diabetes Mellitus and Risks of Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of 144 Prospective Studies. Ageing Res. Rev. 2019, 55, 100944. [Google Scholar] [CrossRef]
- Rawlings, A.M.; Sharrett, A.R.; Schneider, A.L.C.; Coresh, J.; Albert, M.; Couper, D.; Griswold, M.; Gottesman, R.F.; Wagenknecht, L.E.; Windham, B.G.; et al. Diabetes in Midlife and Cognitive Change over 20 Years: A Cohort Study. Ann. Intern. Med. 2014, 161, 785–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Global Action Plan on the Public Health Response to Dementia 2017–2025. 2017. Available online: https://www.who.int/publications-detail-redirect/global-action-plan-on-the-public-health-response-to-dementia-2017---2025 (accessed on 10 June 2022).
- Ohara, T.; Doi, Y.; Ninomiya, T.; Hirakawa, Y.; Hata, J.; Iwaki, T.; Kanba, S.; Kiyohara, Y. Glucose Tolerance Status and Risk of Dementia in the Community: The Hisayama Study. Neurology 2011, 77, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Cukierman, T.; Gerstein, H.C.; Williamson, J.D. Cognitive Decline and Dementia in Diabetes - Systematic Overview of Prospective Observational Studies. Diabetologia 2005, 48, 2460–2469. [Google Scholar] [CrossRef] [PubMed]
- Ott, A.; Stolk, R.P.; Van Harskamp, F.; Pols, H.A.P.; Hofman, A.; Breteler, M.M.B. Diabetes Mellitus and the Risk of Dementia: The Rotterdam Study. Neurology 1999, 53, 1937–1942. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Peters, S.A.E.; Woodward, M.; Arango, S.M.; Batty, G.D.; Beckett, N.; Beiser, A.; Borenstein, A.R.; Crane, P.K.; Haan, M.; et al. Type 2diabetes as a Risk Factor for Dementia in Women Compared with Men: A Pooled Analysis of 2.3 Million People Comprising More than 100,000 Cases of Dementia. Diabetes Care 2016, 39, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Bauzon, J.; Lee, G.; Cummings, J. Repurposed Agents in the Alzheimer’s Disease Drug Development Pipeline. Alzheimer’s Res. Ther. 2020, 12, 1–16. [Google Scholar] [CrossRef]
- Wium-Andersen, I.K.; Osler, M.; Jørgensen, M.B.; Rungby, J.; Wium-Andersen, M.K. Antidiabetic Medication and Risk of Dementia in Patients with Type 2 Diabetes: A Nested Case-Control Study. Eur. J. Endocrinol. 2019, 181, 499–507. [Google Scholar] [CrossRef]
- Zhou, J.B.; Tang, X.; Han, M.; Yang, J.; Simó, R. Impact of Antidiabetic Agents on Dementia Risk: A Bayesian Network Meta-Analysis. Metabolism 2020, 109, 154265. [Google Scholar] [CrossRef]
- Allen, K.V.; Frier, B.M.; Strachan, M.W.J. The Relationship between Type 2 Diabetes and Cognitive Dysfunction: Longitudinal Studies and Their Methodological Limitations. Eur. J. Pharmacol. 2004, 490, 169–175. [Google Scholar] [CrossRef]
- Havrankova, J.; Roth, J.; Brownstein, M. Insulin Receptors Are Widely Distributed in the Central Nervous System of the Rat. Nature 1978, 272, 827–829. [Google Scholar] [CrossRef]
- Ponce, E.; Witte, D.P.; Hirschhorn, R.; Huie, M.L.; Grabowski, G.A. Murine Acid α-Glucosidase. Cell-Specific MRNA Differential Expression during Development and Maturation. Am. J. Pathol. 1999, 154, 1089–1096. [Google Scholar] [CrossRef]
- Xia, Y.; Eisenman, D.; Haddad, G.G. Sulfonylurea Receptor Expression in Rat Brain: Effect of Chronic Hypoxia during Development. Pediatr. Res. 1993, 34, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Culmsee, C.; Monroe, J.; Kemp, B.E.; Mattson, M.P. AMP-Activated Protein Kinase Is Highly Expressed in Neurons in the Developing Rat Brain and Promotes Neuronal Survival Following Glucose Deprivation. J. Mol. Neurosci. 2001, 17, 45–58. [Google Scholar] [CrossRef]
- Tang, S.J.; Reis, G.; Kang, H.; Gingras, A.C.; Sonenberg, N.; Schuman, E.M. A Rapamycin-Sensitive Signaling Pathway Contributes to Long-Term Synaptic Plasticity in the Hippocampus. Proc. Natl. Acad. Sci. USA 2002, 99, 467–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, S.; Ronfani, L.; Bianchi, M.E. Regulated Expression and Subcellular Localization of HMGB1, a Chromatin Protein with a Cytokine Function. J. Intern. Med. 2004, 255, 332–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diering, G.H.; Church, J.; Numata, M. Secretory Carrier Membrane Protein 2 Regulates Cell-Surface Targeting of Brain-Enriched Na+/H+ Exchanger NHE5. J. Biol. Chem. 2009, 284, 13892–13903. [Google Scholar] [CrossRef] [Green Version]
- Warden, A.; Truitt, J.; Merriman, M.; Ponomareva, O.; Jameson, K.; Ferguson, L.B.; Mayfield, R.D.; Harris, R.A. Localization of PPAR Isotypes in the Adult Mouse and Human Brain. Sci. Rep. 2016, 6, 27618. [Google Scholar] [CrossRef]
- Stremenova, J.; Krepela, E.; Mares, V.; Trim, J.; Dbaly, V.; Marek, J.; Vanickova, Z.; Lisa, V.; Yea, C.; Sedo, A. Expression and Enzymatic Activity of Dipeptidyl Peptidase-IV in Human Astrocytic Tumours Are Associated with Tumour Grade. Int. J. Oncol. 2007, 31, 785–792. [Google Scholar] [CrossRef]
- You, G.; Lee, W.S.; Barros, E.J.G.; Kanai, Y.; Huo, T.L.; Khawaja, S.; Wells, R.G.; Nigam, S.K.; Hediger, M.A. Molecular Characteristics of Na+-Coupled Glucose Transporters in Adult and Embryonic Rat Kidney. J. Biol. Chem. 1995, 270, 29365–29371. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, E.; Roncero, I.; Chowen, J.A.; Thorens, B.; Blázquez, E. Expression of the Glucagon-like Peptide-1 Receptor Gene in Rat Brain. J. Neurochem. 1996, 66, 920–927. [Google Scholar] [CrossRef]
- Nedelcovych, M.T.; Gadiano, A.J.; Wu, Y.; Manning, A.A.; Thomas, A.G.; Khuder, S.S.; Yoo, S.W.; Xu, J.; McArthur, J.C.; Haughey, N.J.; et al. Pharmacokinetics of Intranasal versus Subcutaneous Insulin in the Mouse. ACS Chem. Neurosci. 2018, 9, 809–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahr, H.J.; Boberg, M.; Krause, H.P.; Maul, W.; Muller, F.O.; Ploschke, H.J.; Weber, H.; Wunsche, C. Pharmacokinetics of Acarbose. Part I: Absorption, Concentration in Plasma, Metabolism, and Excretion after Single Administration of [14C]Acarbose to Rats, Dogs and Man. Arzneimittelforschung 1989, 39, 1254–1260. [Google Scholar] [PubMed]
- Kumar Thakur, A.; Kumar, Y.; K Goyal, K. Pharmacotherapeutics of Miglitol: An α-Glucosidase Inhibitor. J. Anal. Pharm. Res. 2018, 7, 617–619. [Google Scholar] [CrossRef]
- Lalić-Popović, M.; Vasović, V.; Milijašević, B.; Goločorbin-Kon, S.; Al-Salami, H.; Mikov, M. Deoxycholic Acid as a Modifier of the Permeation of Gliclazide through the Blood Brain Barrier of a Rat. J. Diabetes Res. 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Lahmann, C.; Kramer, H.B.; Ashcroft, F.M. Systemic Administration of Glibenclamide Fails to Achieve Therapeutic Levels in the Brain and Cerebrospinal Fluid of Rodents. PLoS ONE 2015, 10, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Łabuzek, K.; Suchy, D.; Gabryel, B.; Bielecka, A.; Liber, S.; Okopień, B. Quantification of Metformin by the HPLC Method in Brain Regions, Cerebrospinal Fluid and Plasma of Rats Treated with Lipopolysaccharide. Pharmacol. Rep. 2010, 62, 956–965. [Google Scholar] [CrossRef]
- Grommes, C.; Karlo, J.C.; Caprariello, A.; Blankenship, D.; Dechant, A.; Landreth, G.E. The PPARγ Agonist Pioglitazone Crosses the Blood-Brain Barrier and Reduces Tumor Growth in a Human Xenograft Model. Cancer Chemother. Pharmacol. 2013, 71, 929–936. [Google Scholar] [CrossRef]
- Festuccia, W.T.; Oztezcan, S.; Laplante, M.; Berthiaume, M.; Michel, C.; Dohgu, S.; Denis, R.G.; Brito, M.N.; Brito, N.A.; Miller, D.S.; et al. Peroxisome Proliferator-Activated Receptor-γ-Mediated Positive Energy Balance in the Rat Is Associated with Reduced Sympathetic Drive to Adipose Tissues and Thyroid Status. Endocrinology 2008, 149, 2121–2130. [Google Scholar] [CrossRef]
- Holger, F.; Rudolf, B.; Andreas, G. Tissue Distribution of the Novel DPP-4 Inhibitor BI 1356 Is Dominated by Saturable Binding to Its Target in Rats. Biopharm. Drug Dispos. 2009, 30, 229–240. [Google Scholar] [CrossRef]
- Ayoub, B.M.; Mowaka, S.; Safar, M.M.; Ashoush, N.; Arafa, M.G.; Michel, H.E.; Tadros, M.M.; Elmazar, M.M.; Mousa, S.A. Repositioning of Omarigliptin as a Once-Weekly Intranasal Anti-Parkinsonian Agent. Sci. Rep. 2018, 8, 8959. [Google Scholar] [CrossRef]
- Tahara, A.; Takasu, T.; Yokono, M.; Imamura, M.; Kurosaki, E. Characterization and Comparison of Sodium-Glucose Cotransporter 2 Inhibitors in Pharmacokinetics, Pharmacodynamics, and Pharmacologic Effects. J. Pharmacol. Sci. 2016, 130, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastin, A.J.; Akerstrom, V. Entry of Exendin-4 into Brain Is Rapid but May Be Limited at High Doses. Int. J. Obes. 2003, 27, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, K.; Hölscher, C. Drugs Developed to Treat Diabetes, Liraglutide and Lixisenatide, Cross the Blood Brain Barrier and Enhance Neurogenesis. BMC Neurosci. 2012, 13, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salameh, T.S.; Rhea, E.M.; Talbot, K.; Banks, W.A. Brain Uptake Pharmacokinetics of Incretin Receptor Agonists Showing Promise as Alzheimer’s and Parkinson’s Disease Therapeutics. Biochem. Pharmacol. 2020, 180, 114187. [Google Scholar] [CrossRef] [PubMed]
- Pardridge, W.M.; Boado, R.J.; Farrell, C.R. Brain-Type Glucose Transporter (GLUT-1) Is Selectively Localized to the Blood-Brain Barrier: Studies with Quantitative Western Blotting and in Situ Hybridization. J. Biol. Chem. 1990, 265, 18035–18040. [Google Scholar] [CrossRef]
- Derosa, G.; Maffioli, P. α-Glucosidase Inhibitors and Their Use in Clinical Practice. Arch. Med. Sci. 2012, 8, 899–906. [Google Scholar] [CrossRef]
- Kim, J.Y.; Ku, Y.S.; Kim, H.J.; Trinh, N.T.; Kim, W.; Jeong, B.; Heo, T.Y.; Lee, M.K.; Lee, K.E. Oral Diabetes Medication and Risk of Dementia in Elderly Patients with Type 2 Diabetes. Diabetes Res. Clin. Pract. 2019, 154, 116–123. [Google Scholar] [CrossRef]
- Tseng, C.H. Dementia Risk in Type 2 Diabetes Patients: Acarbose Use and Its Joint Effects with Metformin and Pioglitazone. Aging Dis. 2020, 11, 658–667. [Google Scholar] [CrossRef]
- Al Haj Ahmad, R.M.; Ababneh, N.A.; Al-Domi, H.A. Brain Insulin Resistance as a Mechanistic Mediator Links Peripheral Metabolic Disorders with Declining Cognition. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102468. [Google Scholar] [CrossRef]
- De Felice, F.G.; Gonçalves, R.A.; Ferreira, S.T. Impaired Insulin Signalling and Allostatic Load in Alzheimer Disease. Nat. Rev. Neurosci. 2022, 23, 215–230. [Google Scholar] [CrossRef]
- Baura, G.D.; Foster, D.M.; Porte, D.; Kahn, S.E.; Bergman, R.N.; Cobelli, C.; Schwartz, M.W. Saturable Transport of Insulin from Plasma into the Central Nervous System of Dogs in Vivo. A Mechanism for Regulated Insulin Delivery to the Brain. J. Clin. Investig. 1993, 92, 1824–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Secnik, J.; Xu, H.; Schwertner, E.; Hammar, N.; Alvarsson, M.; Winblad, B.; Eriksdotter, M.; Garcia-Ptacek, S.; Religa, D. The Association of Antidiabetic Medications and Mini-Mental State Examination Scores in Patients with Diabetes and Dementia. Alzheimer’s Res. Ther. 2021, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mehta, H.B.; Mehta, V.; Goodwin, J.S. Association of Hypoglycemia with Subsequent Dementia in Older Patients with Type 2 Diabetes Mellitus. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2017, 72, 1110–1116. [Google Scholar] [CrossRef]
- Leonard, C.E.; Han, X.; Brensinger, C.M.; Bilker, W.B.; Cardillo, S.; Flory, J.H.; Hennessy, S. Comparative Risk of Serious Hypoglycemia with Oral Antidiabetic Monotherapy: A Retrospective Cohort Study. Pharmacoepidemiol. Drug Saf. 2018, 27, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Han, E.; Han, K.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; Ko, S.-H.; Lee, Y. Severe Hypoglycemia Increases Dementia Risk and Related Mortality: A Nationwide, Population-Based Cohort Study. J. Clin. Endocrinol. Metab. 2022, 107, e1976–e1986. [Google Scholar] [CrossRef]
- Han, S.J. Hypoglycemia and Dementia Risk in Older Patients with Type 2 Diabetes Mellitus: A Propensity-Score Matched Analysis of a Population-Based Cohort Study (Diabetes Metab J 2020;44:125-33). Diabetes Metab. J. 2020, 44, 360–361. [Google Scholar] [CrossRef]
- Jha, R.M.; Rani, A.; Desai, S.M.; Raikwar, S.; Mihaljevic, S.; Munoz-Casabella, A.; Kochanek, P.M.; Catapano, J.; Winkler, E.; Citerio, G.; et al. Sulfonylurea Receptor 1 in Central Nervous System Injury: An Updated Review. Int. J. Mol. Sci. 2021, 22, 1899. [Google Scholar] [CrossRef]
- Nelson, P.T.; Estus, S.; Abner, E.L.; Parikh, I.; Malik, M.; Neltner, J.H.; Ighodaro, E.; Wang, W.X.; Wilfred, B.R.; Wang, L.S.; et al. ABCC9 Gene Polymorphism Is Associated with Hippocampal Sclerosis of Aging Pathology. Acta Neuropathol. 2014, 127, 825–843. [Google Scholar] [CrossRef] [Green Version]
- Dugan, A.J.; Nelson, P.T.; Katsumata, Y.; Shade, L.M.P.; Boehme, K.L.; Teylan, M.A.; Cykowski, M.D.; Mukherjee, S.; Kauwe, J.S.K.; Hohman, T.J.; et al. Analysis of Genes (TMEM106B, GRN, ABCC9, KCNMB2, and APOE) Implicated in Risk for LATE-NC and Hippocampal Sclerosis Provides Pathogenetic Insights: A Retrospective Genetic Association Study. Acta Neuropathol. Commun. 2021, 9, 1–18. [Google Scholar] [CrossRef]
- Meredith, M.E.; Salameh, T.S.; Banks, W.A. Intranasal Delivery of Proteins and Peptides in the Treatment of Neurodegenerative Diseases. AAPS J. 2015, 17, 780–787. [Google Scholar] [CrossRef] [Green Version]
- Craft, S.; Raman, R.; Chow, T.W.; Rafii, M.S.; Sun, C.K.; Rissman, R.A.; Donohue, M.C.; Brewer, J.B.; Jenkins, C.; Harless, K.; et al. Safety, Efficacy, and Feasibility of Intranasal Insulin for the Treatment of Mild Cognitive Impairment and Alzheimer Disease Dementia: A Randomized Clinical Trial. JAMA Neurol. 2020, 77, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Plum, L.; Schubert, M.; Brüning, J.C. The Role of Insulin Receptor Signaling in the Brain. Trends Endocrinol. Metab. 2005, 16, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Wolski, K. Effect of Rosiglitazone on the Risk of Myocardial Infarction and Death from Cardiovascular Causes. N. Engl. J. Med. 2007, 356, 2457–2471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Wang, L.N.; Jia, J.P. Peroxisome Proliferator-Activated Receptor-Gamma Agonists for Alzheimer’s Disease and Amnestic Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Drugs Aging 2015, 32, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.K.; Alexander, R.C.; Welsh-Bohmer, K.A.; Culp, M.; Chiang, C.; O’Neil, J.; Evans, R.M.; Harrigan, P.; Plassman, B.L.; Burke, J.R.; et al. Safety and Efficacy of Pioglitazone for the Delay of Cognitive Impairment in People at Risk of Alzheimer’s Disease (TOMMORROW): A Prognostic Biomarker Study and a Phase 3, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Neurol. 2021, 20, 537–547. [Google Scholar] [CrossRef]
- Hassan, M.; Eskilsson, A.; Nilsson, C.; Jonsson, C.; Jacobsson, H.; Refai, E.; Larsson, S.; Efendic, S. In Vivo Dynamic Distribution of 131I-Glucagon-like Peptide-1 (7-36) Amide in the Rat Studied by Gamma Camera. Nucl. Med. Biol. 1999, 26, 413–420. [Google Scholar] [CrossRef]
- Katsurada, K.; Yada, T. Neural Effects of Gut- and Brain-Derived Glucagon-like Peptide-1 and Its Receptor Agonist. J. Diabetes Investig. 2016, 7, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Kieffer, T.J.; Mcintosh, C.H.S.; Pederson, R.A. Degradation of Glucose-Dependent Insulinotropic Polypeptide and Truncated Glucagon-Like Peptide 1 in Vitro and in Viuo by Dipeptidyl Peptidase IV. Endocrinology 1995, 136, 3585–3596. [Google Scholar] [CrossRef]
- Kabahizi, A.; Wallace, B.; Lieu, L.; Chau, D.; Dong, Y.; Hwang, E.S.; Williams, K.W. Glucagon-like Peptide-1 (GLP-1) Signalling in the Brain: From Neural Circuits and Metabolism to Therapeutics. Br. J. Pharmacol. 2022, 179, 600–624. [Google Scholar] [CrossRef]
- Mehan, S.; Bhalla, S.; Siddiqui, E.M.; Sharma, N.; Shandilya, A.; Khan, A. Potential Roles of Glucagon-Like Peptide-1 and Its Analogues in Dementia Targeting Impaired Insulin Secretion and Neurodegeneration. Degener. Neurol. Neuromuscul. Dis. 2022, Volume 12, 31–59. [Google Scholar] [CrossRef]
- Athauda, D.; Foltynie, T. The Glucagon-like Peptide 1 (GLP) Receptor as a Therapeutic Target in Parkinson’s Disease: Mechanisms of Action. Drug Discov. Today 2016, 21, 802–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nørgaard, C.H.; Friedrich, S.; Hansen, C.T.; Gerds, T.; Ballard, C.; Møller, D.V.; Knudsen, L.B.; Kvist, K.; Zinman, B.; Holm, E.; et al. Treatment with Glucagon-like Peptide-1 Receptor Agonists and Incidence of Dementia: Data from Pooled Double-blind Randomized Controlled Trials and Nationwide Disease and Prescription Registers. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Secnik, J.; Xu, H.; Schwertner, E.; Hammar, N.; Alvarsson, M.; Winblad, B.; Eriksdotter, M.; Garcia-Ptacek, S.; Religa, D. Dementia Diagnosis Is Associated with Changes in Antidiabetic Drug Prescription: An Open-Cohort Study of ~130,000 Swedish Subjects over 14 Years. J. Alzheimer’s Dis. 2020, 76, 1581–1594. [Google Scholar] [CrossRef] [PubMed]
- Gejl, M.; Gjedde, A.; Egefjord, L.; Møller, A.; Hansen, S.B.; Vang, K.; Rodell, A.; Brændgaard, H.; Gottrup, H.; Schacht, A.; et al. In Alzheimer’s Disease, 6-Month Treatment with GLP-1 Analog Prevents Decline of Brain Glucose Metabolism: Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Front. Aging Neurosci. 2016, 8, 1–10. [Google Scholar] [CrossRef]
- Cukierman-Yaffe, T.; Gerstein, H.C.; Colhoun, H.M.; Diaz, R.; García-Pérez, L.E.; Lakshmanan, M.; Bethel, A.; Xavier, D.; Probstfield, J.; Riddle, M.C.; et al. Effect of Dulaglutide on Cognitive Impairment in Type 2 Diabetes: An Exploratory Analysis of the REWIND Trial. Lancet Neurol. 2020, 19, 582–590. [Google Scholar] [CrossRef]
- Andleeb, S.; Nadia, A.; Waqar, H.; Nouman, R. In Silico Discovery of Potential Inhibitors against Dipeptidyl Peptidase-4: A Major Biological Target of Type-2 Diabetes Mellitus. Int. J. Clin. Microbiol. Biochem. Technol. 2020, 3, 001–010. [Google Scholar] [CrossRef] [Green Version]
- Biessels, G.J.; Verhagen, C.; Janssen, J.; van den Berg, E.; Wallenstein, G.; Zinman, B.; Espeland, M.A.; Johansen, O.E. Effects of Linagliptin vs Glimepiride on Cognitive Performance in Type 2 Diabetes: Results of the Randomised Double-Blind, Active-Controlled CAROLINA-COGNITION Study. Diabetologia 2021, 64, 1235–1245. [Google Scholar] [CrossRef]
- Biessels, G.J.; Verhagen, C.; Janssen, J.; Van Den Berg, E.; Zinman, B.; Rosenstock, J.; George, J.T.; Passera, A.; Schnaidt, S.; Johansen, O.E. Effect of Linagliptin on Cognitive Performance in Patients with Type 2 Diabetes and Cardiorenal Comorbidities: The CARMELINA Randomized Trial. Diabetes Care 2019, 42, 1930–1938. [Google Scholar] [CrossRef]
- Zhou, G.; Myers, R.; Li, Y.; Chen, Y.; Shen, X.; Fenyk-Melody, J.; Wu, M.; Ventre, J.; Doebber, T.; Fujii, N.; et al. Role of AMP-Activated Protein Kinase in Mechanism of Metformin Action. J. Clin. Investig. 2001, 108, 1167–1174. [Google Scholar] [CrossRef]
- Kalender, A.; Selvaraj, A.; Kim, S.Y.; Gulati, P.; Brûlé, S.; Viollet, B.; Kemp, B.E.; Bardeesy, N.; Dennis, P.; Schlager, J.J.; et al. Metformin, Independent of AMPK, Inhibits MTORC1 in a Rag GTPase-Dependent Manner. Cell Metab. 2010, 11, 390–401. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Lee, H.Y.; Ahn, J.; Hyun, M.; Lee, I.; Min, K.J.; You, Y.J. NHX-5, Anl Endosomal Na+/H+ Exchanger, Is Associated with Metformin Action. J. Biol. Chem. 2016, 291, 18591–18599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horiuchi, T.; Sakata, N.; Narumi, Y.; Kimura, T.; Hayashi, T.; Nagano, K.; Liu, K.; Nishibori, M.; Tsukita, S.; Yamada, T.; et al. Metformin Directly Binds the Alarmin HMGB1 and Inhibits Its Proinflammatory Activity. J. Biol. Chem. 2017, 292, 8436–8446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Dai, W.; Zhu, X.; Ma, T. A Review of Autophagy Mechanism of Statins in the Potential Therapy of Alzheimer ’ s Disease. J. Integr Neurosci. 2022, 21. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Huang, N.; Liu, J.; Huang, J.; Shi, J.; Jin, F. AMPK: A Bridge between Diabetes Mellitus and Alzheimer’s Disease. Behav. Brain Res. 2021, 400, 113043. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Lee, D.H.; Song, J. HMGB1 Signaling Pathway in Diabetes-Related Dementia: Blood-Brain Barrier Breakdown, Brain Insulin Resistance, and Aβ Accumulation. Biomed. Pharmacother. 2022, 150, 112933. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Ying, S.; Ma, Q.; Li, H.; Li, J.; Song, J. Metformin Ameliorates HMGB1-Mediated Oxidative Stress through MTOR Pathway in Experimental Periodontitis. Genes Dis. 2021, in press. [CrossRef]
- Campbell, J.M.; Stephenson, M.D.; De Courten, B.; Chapman, I.; Bellman, S.M.; Aromataris, E. Metformin Use Associated with Reduced Risk of Dementia in Patients with Diabetes: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2018, 65, 1225–1236. [Google Scholar] [CrossRef] [Green Version]
- Tabatabaei Malazy, O.; Bandarian, F.; Qorbani, M.; Mohseni, S.; Mirsadeghi, S.; Peimani, M.; Larijani, B. The Effect of Metformin on Cognitive Function: A Systematic Review and Meta-Analysis. J. Psychopharmacol. 2022. [CrossRef]
- Koenig, A.M.; Mechanic-Hamilton, D.; Xie, S.X.; Combs, M.F.; Cappola, A.R.; Xie, L.; Detre, J.A.; Wolk, D.A.; Arnold, S.E. Effects of the Insulin Sensitizer Metformin in Alzheimer Disease: Pilot Data From a Randomized Placebo-Controlled Crossover Study. Alzheimer Dis. Assoc. Disord. 2017, 31, 107–113. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Perez, T.; Chang, H.; Mehta, P.; Steffener, J.; Pradabhan, G.; Ichise, M.; Manly, J.; Devanand, D.P.; Bagiella, E. Metformin in Amnestic Mild Cognitive Impairment: Results of a Pilot Randomized Placebo Controlled Clinical Trial. J. Alzheimer’s Dis. 2016, 51, 501–514. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, S.; Rizvi, S.M.D.; Shakil, S.; Riyaz, S.; Biswas, D.; Jahan, R. Forxiga (Dapagliflozin): Plausible Role in the Treatment of Diabetes-Associated Neurological Disorders. Biotechnol. Appl. Biochem. 2016, 63, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Shakil, S. Molecular Interaction of Anti-Diabetic Drugs With Acetylcholinesterase and Sodium Glucose Co-Transporter 2. J. Cell. Biochem. 2017, 118, 3855–3865. [Google Scholar] [CrossRef] [PubMed]
- Mui, J.V.; Zhou, J.; Lee, S.; Leung, K.S.K.; Lee, T.T.L.; Chou, O.H.I.; Tsang, S.L.; Wai, A.K.C.; Liu, T.; Wong, W.T.; et al. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors vs. Dipeptidyl Peptidase-4 (DPP4) Inhibitors for New-Onset Dementia: A Propensity Score-Matched Population-Based Study With Competing Risk Analysis. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Perna, S.; Mainardi, M.; Astrone, P.; Gozzer, C.; Biava, A.; Bacchio, R.; Spadaccini, D.; Solerte, S.B.; Rondanelli, M. 12-Month Effects of Incretins versus SGLT2-Inhibitors on Cognitive Performance and Metabolic Profile. A Randomized Clinical Trial in the Elderly with Type-2 Diabetes Mellitus. Clin. Pharmacol. Adv. Appl. 2018, 10, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Pharmacological Effect | Target Protein | Brain Expression | Ref. | |
|---|---|---|---|---|
| Insulin | Activates insulin receptor signaling | Insulin receptor | Yes | [21] |
| α-Glucosidase inhibitors | Suppress glucose absorption | α-Glucosidase | Yes | [22] |
| Sulfonylureas | Promote insulin secretion | Sulfonylurea receptor | Yes | [23] |
| Metformin | Improves insulin sensitivity, etc. * | AMPK, etc. * | Yes | [24,25,26,27] |
| Thiazolidinediones | Improve insulin sensitivity | PPARγ | Yes | [28] |
| DPP-4 inhibitors | Prevent GLP-1 breakdown | DPP-4 | Yes | [29] |
| SGLT2 inhibitors | Promote glucose excretion | SGLT2 | No | [30] |
| GLP-1 receptor agonists | Activate GLP-1 receptor signaling | GLP-1 receptor | Yes | [31] |
| Drug | Species | Dose | Administration Route | Plasma Level | Brain Level | Plasma/Brain | Ref. | |
|---|---|---|---|---|---|---|---|---|
| Insulin | Subcutaneous insulin | Mouse | 2.4 IU | Subcutaneous injections | AUC0-t = 520,351 h·μIU/mL | AUC0-t = 2537 h·μIU/mL | 0.005 | [32] |
| Intranasal insulin | Mouse | 2.4 IU | Intranasal administration | AUC0-t = 354 h·μIU/mL | AUC0-t = 3442 h·μIU/mL | 9.72 | [32] | |
| a-Glucosidase inhibitors | Acarbose | Human | 200 mg. | Oral administration | Absorbed only 1–2% of dose | N.D. | N.D. | [33] |
| Miglitol | Human | 50 mg | Oral administration | AUC0-t = 5998 ng·h/mL | Permeation from BBB is low | N.D. | [34] | |
| Sulfonylureas | Gliclazide | Rat | 20 mg/kg | Intraarterial injection | Concentration = 15.99 μg/ml | Concentration = 1.71 µg/g | 0.12 g·mL | [35] |
| Glibenclamide | Rat | 50 mg/kg | Intraperitoneal injection | Concentration = 34 μg/ml | Concentration = 85 ng/ml | 0.0025 | [36] | |
| Biguanides | Metformin | Rat | 150 mg/kg | Oral administration | Concentration = 13.8 µmol/L | Concentration = 13.5 µmol/L | 0.99 | [37] |
| Thiazolidinediones | Pioglitazone | Mouse | 10.2 mg/kg | Oral administration | N.D. | Concentration = 712.6 pmol/L | N.D. | [38] |
| Rosiglitazone | Rodent | Unknown | Unknown | N.D. | 0.045% Inject/g tissue | 20–30 µL/g *,† | [39] | |
| DPP-4 inhibitors | Linagliptin | Rat | 2 mg/kg | Intravenous injection | N.D. | BLD | N.D. | [40] |
| Omarigliptin | Rat | 5 mg/kg | Oral administration | Concentration = 2688.79 ng/mL | Concentration = 621.75 ng/g | 0.23 g·mL | [41] | |
| Trelagliptin | Rat | 20 mg/kg | Oral administration | Concentration = 1754.79 ng/mL | N.D. | N.D. | [41] | |
| SGLT2 inhibitors | Ipragliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 4520 ng·h/mL | AUC0-t = 2020 ng·h/g | 0.5 mL/g | [42] |
| Dapagliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 2970 ng·h/mL | AUC0-t = 904 ng·h/g | 0.3 mL/g | [42] | |
| Tofogliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 1010 ng·h/mL | AUC0-t = 315 ng·h/g | 0.3 mL/g | [42] | |
| Canagliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 1620 ng·h/mL | AUC0-t = 532 ng·h/g | 0.3 mL/g | [42] | |
| Empagliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 626 ng·h/mL | AUC0-t = 313 ng·h/g | 0.5 mL/g | [42] | |
| Luseogliflozin | Mouse | 3 mg/kg | Oral administration | AUC0-t = 478 ng·h/mL | AUC0-t = 157 ng·h/g | 0.3 mL/g | [42] | |
| GLP-1 receptor agonists | Exenatide | Mouse | Unknown | Intravenous injection | N.D. | Concentration = 17.8 µL/g | N.D. | [43] |
| Liraglutide | Mouse | 250 nmol/kg | Intraperitoneal injection | N.D. | Concentration = 200–300 pmol/L * | N.D. | [44] | |
| Lixisenatide | Mouse | 250 nmol/kg | Intraperitoneal injection | N.D. | Concentration = 100–150 pmol/L* | N.D. | [44] | |
| Semaglutide | Mouse | 1 × 106 cpm | Intravenous injection | N.D. | Brain influx rates = N.S. | N.D. | [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogura, J.; Yamaguchi, H. The Effectiveness of Antidiabetic Drugs in Treating Dementia: A Peek into Pharmacological and Pharmacokinetic Properties. Int. J. Mol. Sci. 2022, 23, 6542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23126542
Ogura J, Yamaguchi H. The Effectiveness of Antidiabetic Drugs in Treating Dementia: A Peek into Pharmacological and Pharmacokinetic Properties. International Journal of Molecular Sciences. 2022; 23(12):6542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23126542
Chicago/Turabian StyleOgura, Jiro, and Hiroaki Yamaguchi. 2022. "The Effectiveness of Antidiabetic Drugs in Treating Dementia: A Peek into Pharmacological and Pharmacokinetic Properties" International Journal of Molecular Sciences 23, no. 12: 6542. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23126542