
Plocabulin, a Novel Tubulin Inhibitor, Has Potent Antitumour Activity in Patient-Derived Xenograft Models of Soft Tissue Sarcoma

 , and
, and
Abstract
:1. Introduction
2. Results
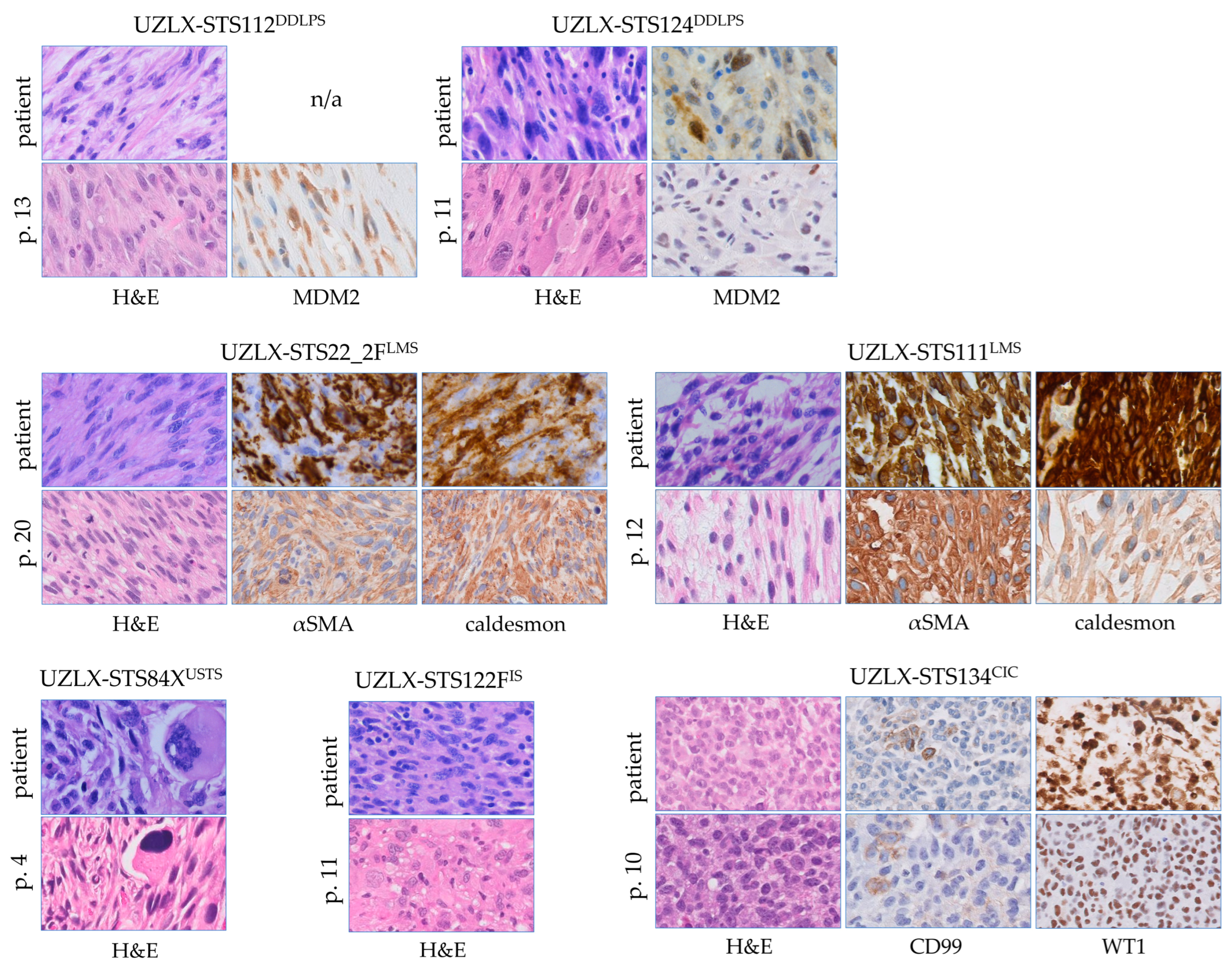
2.1. All PDX Models Were Histologically Stable
2.2. No Severe Toxicity Was Associated with Plocabulin Treatment
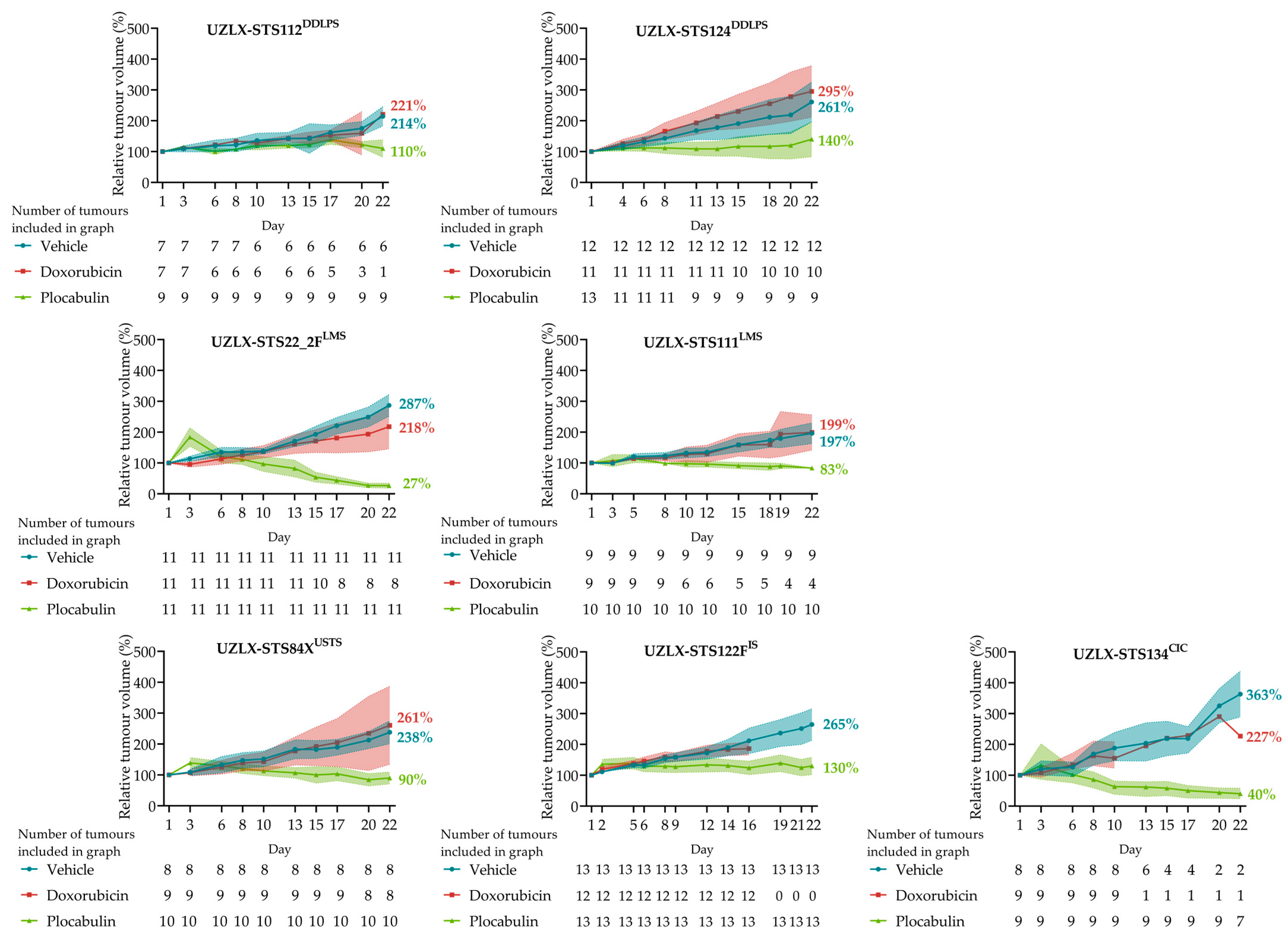
2.3. Plocabulin Resulted in Tumour Shrinkage in LMS, CIC and USTS Models, and in Tumour Volume Stabilisation in DDLPS and IS
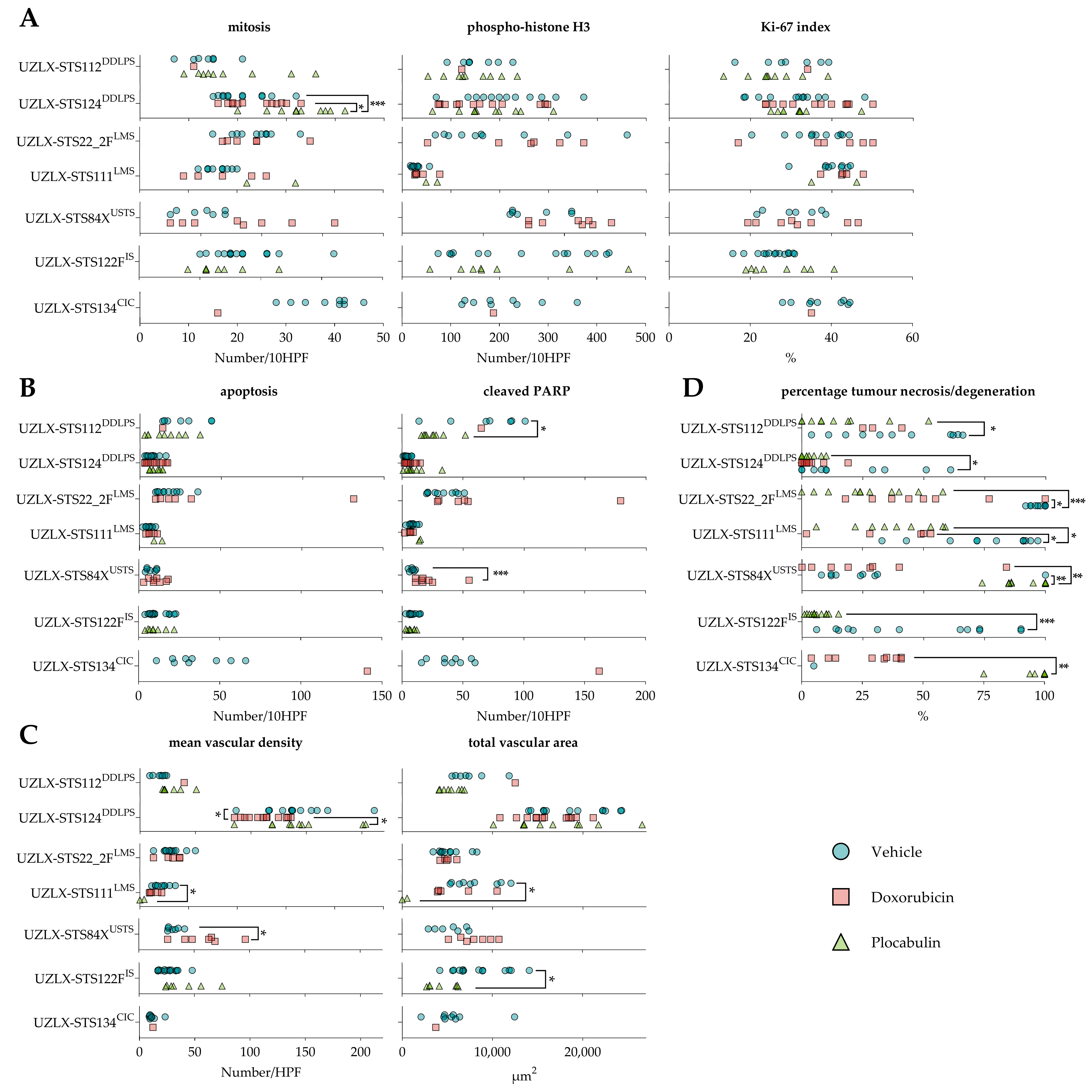
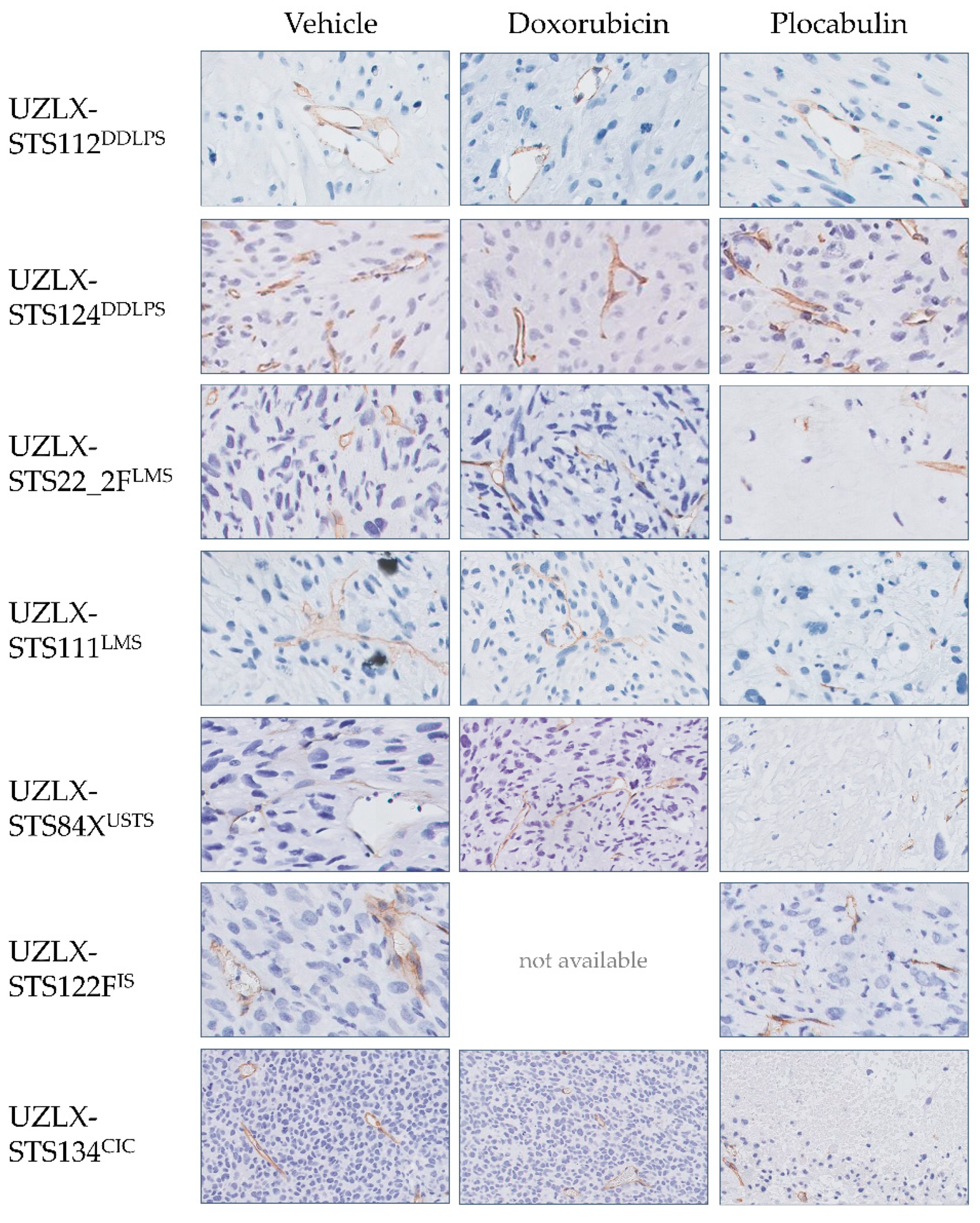
2.4. Plocabulin Treatment Induced Necrosis and Degenerative Changes in All Histological Subtypes
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Xenograft Models
4.3. Drug Preparation
4.4. Experimental Design
4.5. Tumour Volume Measurement
4.6. Immunohistochemistry
4.7. Histological Assessment
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.M.; Bridge, J.A.; Hogendoorn, P.C.W.; Mertens, F. WHO Classification of Tumours of Soft Tissue and Bone, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- Christie-Large, M.; James, S.L.J.; Tiessen, L.; Davies, A.M.; Grimer, R.J. Imaging strategy for detecting lung metastases at presentation in patients with soft tissue sarcomas. Eur. J. Cancer 2008, 44, 1841–1845. [Google Scholar] [CrossRef] [PubMed]
- Bozzo, A.; Seow, H.; Pond, G.; Ghert, M. Changes in soft-tissue sarcoma treatment patterns over time: A population-based study in a country with universal and centralized healthcare. Sarcoma 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, L.H.; Litière, S.; Sleijfer, S.; Benson, C.; Italiano, A.; Kasper, B.; Messiou, C.; Gelderblom, H.; Wardelmann, E.; Le Cesne, A.; et al. Prognostic factors for soft tissue sarcoma patients with lung metastases only who are receiving first-line chemotherapy: An exploratory, retrospective analysis of the European Organization for Research and Treatment of Cancer-soft tissue and bone sarcoma. Int. J. Cancer 2018, 142, 2610–2620. [Google Scholar] [CrossRef]
- In, G.K.; Hu, J.S.; Tseng, W.W. Treatment of advanced, metastatic soft tissue sarcoma: Latest evidence and clinical considerations. Ther. Adv. Med. Oncol. 2017, 9, 533–550. [Google Scholar] [CrossRef]
- Ryan, C.W.; Merimsky, O.; Agulnik, M.; Blay, J.-Y.; Schuetze, S.M.; Van Tine, B.A.; Jones, R.L.; Elias, A.D.; Choy, E.; Alcindor, T.; et al. PICASSO III: A phase III, placebo-controlled study of doxorubicin with or without palifosfamide in patients with metastatic soft tissue sarcoma. J. Clin. Oncol. 2016, 34, 3898–3905. [Google Scholar] [CrossRef]
- Tap, W.D.; Papai, Z.; Tine, B.A.; Attia, S.; Ganjoo, K.N.; Jones, R.L.; Schuetze, S.; Reed, D.; Chawla, S.P.; Riedel, R.F.; et al. Doxorubicin plus evofosfamide versus doxorubicin alone in locally advanced, unresectable or metastatic soft-tissue sarcoma (TH CR-406/SARC021): An international, multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2017, 18, 1089–1103. [Google Scholar] [CrossRef]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.-Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.J.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef] [Green Version]
- Le Cesne, A.; Blay, J.-Y.; Cupissol, D.; Italiano, A.; Delcambre, C.; Penel, N.; Isambert, N.; Chevreau, C.; Bompas, E.; Bertucci, F.; et al. Results of a prospective randomized phase III T-SAR trial comparing trabectedin (T) vs best supportive care (BSC) in patients with pretreated advanced soft tissue sarcoma (ASTS): A French Sarcoma Group (FSG) trial. J. Clin. Oncol. 2018, 36 (Suppl. S15), 11508. [Google Scholar] [CrossRef]
- Schöffski, P.; Chawla, S.; Maki, R.G.; Italiano, A.; Gelderblom, H.; Choy, E.; Grignani, G.; Camargo, V.; Bauer, S.; Rha, S.Y.; et al. Eribulin versus dacarbazine in previously treated patients with advanced liposarcoma or leiomyosarcoma: A randomised, open-label, multicentre, phase 3 trial. Lancet 2016, 387, 1629–1637. [Google Scholar] [CrossRef]
- Maki, R.G.; Wathen, J.K.; Patel, S.R.; Priebat, D.A.; Okuno, S.H.; Samuels, B.; Fanucchi, M.; Harmon, D.C.; Schuetze, S.M.; Reinke, D.; et al. Randomized phase II study of gemcitabine and docetaxel compared with gemcitabine alone in patients with metastatic soft tissue sarcomas: Results of sarcoma alliance for research through collaboration study 002. J. Clin. Oncol. 2007, 25, 2755–2763. [Google Scholar] [CrossRef] [PubMed]
- García-Del-Muro, X.; López-Pousa, A.L.; Maurel, J.; Martín, J.; Martínez-Trufero, J.; Casado, A.; Gómez-España, A.; Fra, J.; Cruz, J.; Poveda, A.; et al. Randomized phase II study comparing gemcitabine plus dacarbazine versus dacarbazine alone in patients with previously treated soft tissue sarcoma: A Spanish group for research on sarcomas study. J. Clin. Oncol. 2011, 29, 2528–2533. [Google Scholar] [CrossRef] [PubMed]
- Koliou, P.; Karavasilis, V.; Theochari, M.; Pollack, S.M.; Jones, R.L.; Thway, K. Advances in the treatment of soft tissue sarcoma: Focus on eribulin. Cancer Manag. Res. 2018, 10, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Martín, M.J.; Coello, L.; Fernández, R.; Reyes, F.; Rodríguez, A.; Murcia, C.; Garranzo, M.; Mateo, C.; Sánchez-Sancho, F.; Bueno, S.; et al. Isolation and first total synthesis of PM050489 and PM060184, two new marine anticancer compounds. J. Am. Chem. Soc. 2013, 135, 10164–10171. [Google Scholar] [CrossRef]
- Martínez-Díez, M.; Guillén-Navarro, M.J.; Pera, B.; Bouchet, B.P.; Martínez-Leal, J.F.; Barasoain, I.; Cuevas, C.; Andreu, J.M.; García-Fernández, L.F.; Díaz, J.F.; et al. PM060184, a new tubulin binding agent with potent antitumor activity including P-glycoprotein over-expressing tumors. Biochem. Pharmacol. 2014, 88, 291–302. [Google Scholar] [CrossRef]
- Prota, A.E.; Bargsten, K.; Diaz, J.F.; Marsh, M.; Cuevas, C.; Liniger, M.; Neuhaus, C.; Andreu, J.M.; Altmann, K.-H.; Steinmetz, M.O. A new tubulin-binding site and pharmacophore for microtubule-destabilizing anticancer drugs. Proc. Natl. Acad. Sci. USA 2014, 111, 13817–13821. [Google Scholar] [CrossRef] [Green Version]
- Pera, B.; Barasoain, I.; Pantazopoulou, A.; Canales, A.; Matesanz, R.; Rodriguez-Salarichs, J.; García-Fernandez, L.F.; Moneo, V.; Jiménez-Barbero, J.; Galmarini, C.M.; et al. New interfacial microtubule inhibitors of marine origin, PM050489/PM060184, with potent antitumor activity and a distinct mechanism. ACS Chem. Biol. 2013, 8, 2084–2094. [Google Scholar] [CrossRef]
- Galmarini, C.M.; Martin, M.; Bouchet, B.P.; Guillen-Navarro, M.J.; Martínez-Diez, M.; Martinez-Leal, J.F.; Akhmanova, A.; Aviles, P. Plocabulin, a novel tubulin-binding agent, inhibits angiogenesis by modulation of microtubule dynamics in endothelial cells. BMC Cancer 2018, 18, 164. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wozniak, A.; Wellens, J.; Gebreyohannes, Y.K.; Guillén, M.J.; Avilés, P.M.; Debiec-Rychter, M.; Sciot, R.; Schöffski, P. Plocabulin, a novel tubulin inhibitor, has potent antitumor activity in patient-derived xenograft models of gastrointestinal stromal tumors. Transl. Oncol. 2020, 13, 100832. [Google Scholar] [CrossRef]
- Elez, E.; Gomez-Roca, C.; Matos-Pita, A.; Argiles, G.; Valentin, T.; Coronado, C.; Iglesias, J.; Macarulla, T.; Betrian, S.; Fudio, S.; et al. First-in-human phase I study of the microtubule inhibitor plocabulin in patients with advanced solid tumors. Investig. New Drug 2019, 37, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Cornillie, J.; Wozniak, A.; Li, H.; Wang, Y.; Boeckx, B.; Gebreyohannes, Y.K.; Wellens, J.; Vanleeuw, U.; Hompes, D.; Stas, M.; et al. Establishment and characterization of histologically and molecularly stable soft-tissue sarcoma xenograft models for biological studies and preclinical drug testing. Mol. Cancer Ther. 2019, 18, 1168–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidi, K.; Jahanban-Esfahlan, R.; Zarghami, N. Tumor rim cells: From resistance to vascular targeting agents to complete tumor ablation. Tumor Biol. 2017, 39, 1010428317691001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, J.H.; Rockley, K.L.; Santis, C.; Mohamed, A.K. Vascular disrupting agents in cancer treatment: Cardiovascular toxicity and implications for co-administration with other cancer chemotherapeutics. Pharmacol. Therapeut. 2019, 202, 18–31. [Google Scholar] [CrossRef]
- Sleijfer, S.; Ray-Coquard, I.; Papai, Z.; Cesne, A.L.; Scurr, M.; Schöffski, P.; Collin, F.; Pandite, L.; Marreaud, S.; De Brauwer, A.; et al. Pazopanib, a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft tissue sarcoma: A phase II study from the European Organisation for Research and Treatment of Cancer–Soft Tissue and Bone Sarcoma Group (EORTC Study 62043). J. Clin. Oncol. 2009, 27, 3126–3132. [Google Scholar]
- van der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Van Glabbeke, M.; Verweij, J.; Judson, I.; Nielsen, O.S. EORTC soft tissue and bone sarcoma group. progression-free rate as the principal end-point for phase II trials in soft-tissue sarcomas. Eur. J. Cancer 2002, 38, 543–549. [Google Scholar] [CrossRef]
- Grünwald, V.; Litière, S.; Young, R.; Messiou, C.; Lia, M.; Wardelmann, E.; Van Der Graaf, W.; Gronchi, A.; Judson, I.; Stbsg, E. Absence of progression, not extent of tumour shrinkage, defines prognosis in soft-tissue sarcoma—An analysis of the EORTC 62012 study of the EORTC STBSG. Eur. J. Cancer 2016, 64, 44–51. [Google Scholar] [CrossRef]
- Pantazopoulou, A.; Galmarini, C.M.; Peñalva, M.A. Molecular basis of resistance to the microtubule-depolymerizing antitumor compound plocabulin. Sci. Rep. 2018, 8, 8616. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.K.; Bressler, K.; Patel, H.; Balasingam, N.; Thakor, N. Role of eukaryotic initiation factors during cellular stress and cancer progression. J. Nucleic Acids 2016, 2016, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Rieker, R.J.; Weitz, J.; Lehner, B.; Egerer, G.; Mueller, A.; Kasper, B.; Schirmacher, P.; Joos, S.; Mechtersheimer, G. Genomic profiling reveals subsets of dedifferentiated liposarcoma to follow separate molecular pathways. Virchows Arch. 2010, 456, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Gilliam, L.A.A.; Moylan, J.S.; Callahan, L.A.; Sumandea, M.P.; Reid, M.B. Doxorubicin causes diaphragm weakness in murine models of cancer chemotherapy. Muscle Nerve 2011, 43, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreidieh, F.Y.; Moukadem, H.A.; Saghir, N.S.E. Overview, prevention and management of chemotherapy extravasation. World J. Clin. Oncol. 2016, 7, 87. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, M.; Amant, F.; Biankin, A.V.; Budinská, E.; Byrne, A.T.; Caldas, C.; Clarke, R.B.; de Jong, S.; Jonkers, J.; Mælandsmo, G.M.; et al. Patient-derived xenograft models: An emerging platform for translational cancer research. Cancer Discov. 2014, 4, 998–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornillie, J.; Wozniak, A.; Van Renterghem, B.; Van Winkel, N.; Wellens, J.; Gebreyohannes, Y.K.; Debiec-Rychter, M.; Sciot, R.; Hompes, D.; Schöffski, P. Assessment of the platelet-derived growth factor receptor alpha antibody olaratumab in a panel of patient-derived soft tissue sarcoma xenografts. BMC Cancer 2019, 19, 724. [Google Scholar] [CrossRef]
- Cornillie, J.; Wozniak, A.; Pokreisz, P.; Casazza, A.; Vreys, L.; Wellens, J.; Vanleeuw, U.; Gebreyohannes, Y.K.; Debiec-Rychter, M.; Sciot, R.; et al. In vivo antitumoral efficacy of PHAC-ALGP-doxorubicin, an enzyme-activated doxorubicin prodrug, in patient-derived soft tissue sarcoma xenograft models. Mol. Cancer Ther. 2017, 16, 1566–1575. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Wozniak, A.; Sciot, R.; Cornillie, J.; Wellens, J.; Van Looy, T.; Vanleeuw, U.; Stas, M.; Hompes, D.; Debiec-Rychter, M.; et al. Pazopanib, a receptor tyrosine kinase inhibitor, suppresses tumor growth through angiogenesis in dedifferentiated liposarcoma xenograft models. Transl. Oncol. 2014, 7, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Floris, G.; Debiec-Rychter, M.; Sciot, R.; Stefan, C.; Fieuws, S.; Machiels, K.; Atadja, P.; Wozniak, A.; Faa, G.; Schöffski, P. High efficacy of panobinostat towards human gastrointestinal stromal tumors in a xenograft mouse model. Clin. Cancer Res. 2009, 15, 4066–4076. [Google Scholar] [CrossRef] [Green Version]
- Weidner, N.; Semple, J.P.; Welch, W.R.; Folkman, J. Tumor angiogenesis and metastasis—Correlation in invasive breast carcinoma. N. Engl. J. Med. 1991, 324, 1–8. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Average Absolute Tumour Volume | Average Relative Tumour Volume | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Day 1, mm3 | Day 22, mm3 | p-Value Compared to Day 1 (WMP) | Day 22 (95% CI), % | p-Value of Kruskal–Wallis Test | p-Value Compared to Vehicle (DMC) | p-Value Compared to Doxorubicin (DMC) | |||
| Dedifferentiated liposarcoma | UZLX-STS124DDLPS | Vehicle | 268.7 | 663.8 | 0.0005 | 261 (196–326) | 0.003 | n/a | >0.9999 |
| Doxorubicin | 416.0 | 769.9 | 0.002 | 295 (211–379) | >0.9999 | n/a | |||
| Plocabulin | 661.6 | 726.8 | 0.1641 | 140 (83–197) | 0.0186 | 0.0042 | |||
| UZLX-STS112DDLPS | Vehicle | 395.6 | 897.0 | 0.0313 | 214 (182–246) | 0.0002 | n/a | n/a ** | |
| Doxorubicin | 580.7 | 904.7 | n/a ** | 221 (n/a **) | n/a ** | n/a | |||
| Plocabulin | 375.0 | 431.8 | 0.2031 | 110 (82–138) | 0.0043 | n/a | |||
| Leiomyosarcoma | UZLX-STS22_2FLMS | Vehicle | 236.9 | 660.2 | 0.001 | 287 (252–322) | <0.0001 | n/a | 0.674 |
| Doxorubicin | 327.0 | 662.2 | 0.0156 | 218 (146–290) | 0.674 | n/a | |||
| Plocabulin | 337.5 | 87.1 | 0.001 | 27 (19–35) | <0.0001 | 0.0091 | |||
| UZLX-STS111LMS | Vehicle | 501.2 | 958.8 | 0.0039 | 197 (163–231) | 0.0003 | n/a | n/a ** | |
| Doxorubicin | 552 | 1249.4 | 0.125 | 199 (142–256) | n/a ** | n/a | |||
| Plocabulin | 483.8 | 395.9 | 0.0039 | 83 (77–89) | 0.001 | 0.0068 | |||
| Undifferentiated sarcoma | UZLX-STS84XUS | Vehicle | 249.2 | 570.6 | 0.0078 | 238 (190–332) | 0.0004 | n/a | >0.9999 |
| Doxorubicin | 222.4 | 489.4 | 0.0156 | 261 (84–597) | >0.9999 | n/a | |||
| Plocabulin | 259.6 | 217.1 | 0.0371 | 90 (65–155) | 0.0013 | 0.0041 | |||
| Intimal sarcoma | UZLX-STS84XIS | Vehicle | 373.8 | 967.0 | 0.0002 | 265 (214–316) | n/a | n/a | n/a ** |
| Doxorubicin | 316.8 | n/a ** | n/a ** | n/a ** (n/a **) | n/a ** | n/a | |||
| Plocabulin | 311.5 | 375.6 | 0.1099 | 130 (102–158) | <0.0001 *** | n/a | |||
| CIC-rearranged sarcoma | UZLX-STS134CIC | Vehicle | 894.3 | 1994.9 | n/a ** | 363 (289–438) * | 0.0167 | n/a | >0.9999 |
| Doxorubicin | 1594.5 | 574.1 | n/a ** | 227 (n/a **) | >0.9999 | n/a | |||
| Plocabulin | 1463.4 | 470.0 | 0.0156 | 40 (24–58) * | 0.0704 | 0.6496 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Wozniak, A.; Cornillie, J.; Avilés, P.; Debiec-Rychter, M.; Sciot, R.; Schöffski, P. Plocabulin, a Novel Tubulin Inhibitor, Has Potent Antitumour Activity in Patient-Derived Xenograft Models of Soft Tissue Sarcoma. Int. J. Mol. Sci. 2022, 23, 7454. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23137454
Wang Y, Wozniak A, Cornillie J, Avilés P, Debiec-Rychter M, Sciot R, Schöffski P. Plocabulin, a Novel Tubulin Inhibitor, Has Potent Antitumour Activity in Patient-Derived Xenograft Models of Soft Tissue Sarcoma. International Journal of Molecular Sciences. 2022; 23(13):7454. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23137454
Chicago/Turabian StyleWang, Yannick, Agnieszka Wozniak, Jasmien Cornillie, Pablo Avilés, Maria Debiec-Rychter, Raf Sciot, and Patrick Schöffski. 2022. "Plocabulin, a Novel Tubulin Inhibitor, Has Potent Antitumour Activity in Patient-Derived Xenograft Models of Soft Tissue Sarcoma" International Journal of Molecular Sciences 23, no. 13: 7454. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23137454