
Applications of Circulating Tumor Cells and Circulating Tumor DNA in Precision Oncology for Breast Cancers

 and
and
Abstract
:1. Introduction
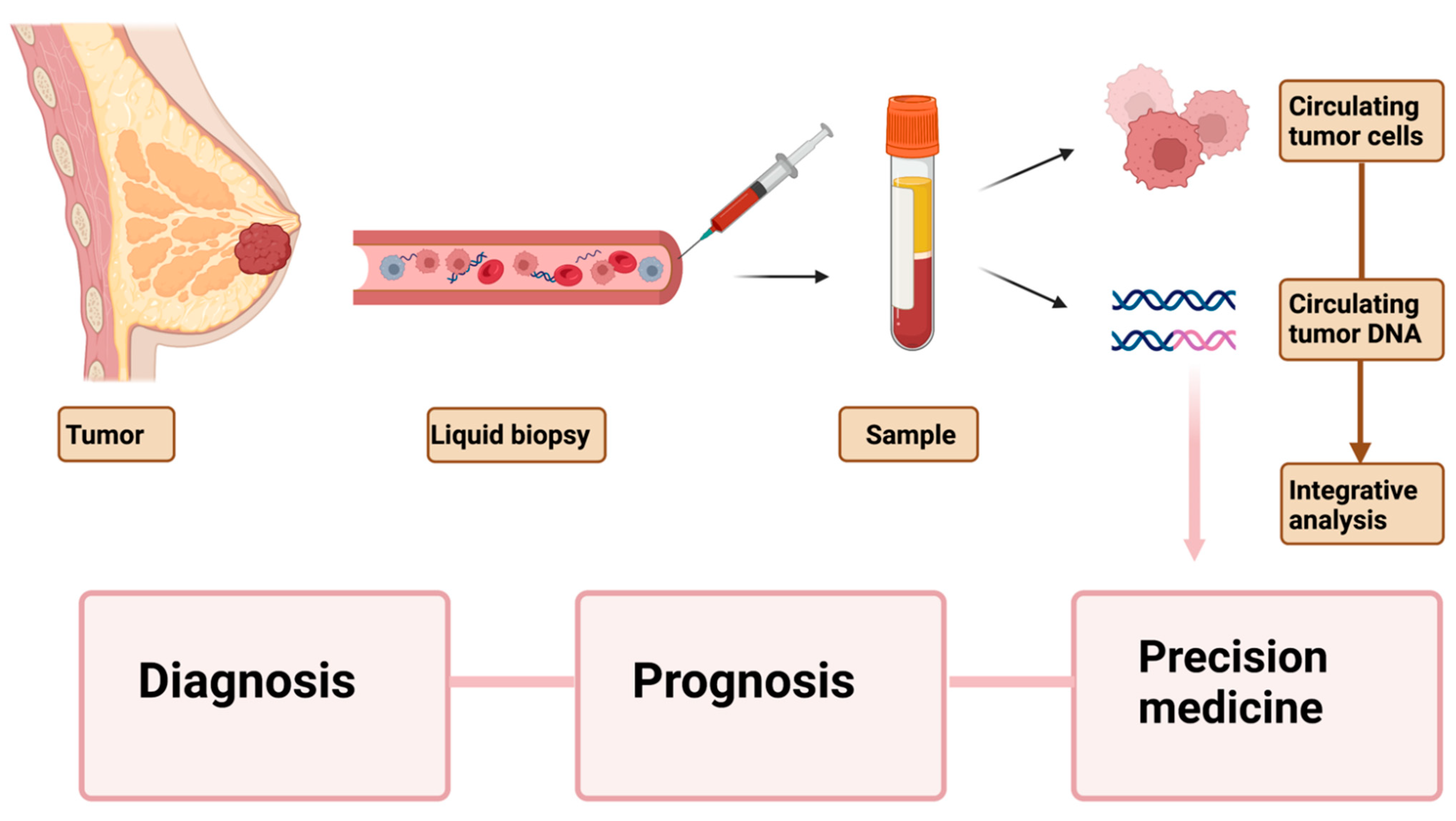
2. Current Understanding and Utility of Liquid Biopsy Markers
3. Circulating Tumor Cells and Circulating Tumor DNA
4. CTCs in Early Stage Breast Cancer
5. CtDNA in Early Stage Breast Cancer
6. CTCs in Metastatic Breast Cancer
7. ctDNA in Metastatic Breast Cancer
8. Use of Circulating Tumor Markers for Precision Medicine
9. Drawbacks of Existing Liquid Biopsy Approaches
10. Leveraging Next-Generation Sequencing Methods for the Application of Liquid Biopsy Markers toward Personalized Medicine of Breast Cancer
11. Integrating CTCs and cfDNA Data for Better Prognosis
12. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Prat, A.; Perou, C.M. Deconstructing the molecular portraits of breast cancer. Mol. Oncol. 2011, 5, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.A.; Perou, C.M.; Livasy, C.A.; Dressler, L.G.; Cowan, D.; Conway, K.; Karaca, G.; Troester, M.A.; Tse, C.K.; Edmiston, S.; et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006, 295, 2492–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creighton, C.J. The molecular profile of luminal B breast cancer. Biologics 2012, 6, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Bauer, K.R.; Brown, M.; Cress, R.D.; Parise, C.A.; Caggiano, V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: A population-based study from the California cancer Registry. Cancer 2007, 109, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Siddharth, S.; Sharma, D. Racial Disparity and Triple-Negative Breast Cancer in African-American Women: A Multifaceted Affair between Obesity, Biology, and Socioeconomic Determinants. Cancers 2018, 10, 514. [Google Scholar] [CrossRef] [Green Version]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The triple negative paradox: Primary tumor chemosensitivity of breast cancer subtypes. Clin. Cancer Res. 2007, 13, 2329–2334. [Google Scholar] [CrossRef] [Green Version]
- Ellington, T.D.; Miller, J.W.; Henley, S.J.; Wilson, R.J.; Wu, M.; Richardson, L.C. Trends in Breast Cancer Incidence, by Race, Ethnicity, and Age Among Women Aged ≥ 20 Years—United States, 1999–2018. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 43–47. [Google Scholar] [CrossRef]
- Heller, D.R.; Chiu, A.S.; Farrell, K.; Killelea, B.K.; Lannin, D.R. Why Has Breast Cancer Screening Failed to Decrease the Incidence of de Novo Stage IV Disease? Cancers 2019, 11, 500. [Google Scholar] [CrossRef] [Green Version]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef] [Green Version]
- Lauby-Secretan, B.; Loomis, D.; Straif, K. Breast-Cancer Screening--Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 373, 1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilgour, E.; Rothwell, D.G.; Brady, G.; Dive, C. Liquid Biopsy-Based Biomarkers of Treatment Response and Resistance. Cancer Cell 2020, 37, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, A.; Pantel, K. Liquid Biopsies, What We Do Not Know (Yet). Cancer Cell 2017, 31, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashworth, T.R. A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Aust. Med. J. 1869, 14, 146. [Google Scholar]
- Mandel, P.; Metais, P. Nuclear Acids In Human Blood Plasma. C. R. Seances Soc. Biol. Fil. 1948, 142, 241–243. [Google Scholar]
- Leon, S.A.; Shapiro, B.; Sklaroff, D.M.; Yaros, M.J. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res. 1977, 37, 646–650. [Google Scholar]
- Stroun, M.; Anker, P.; Maurice, P.; Lyautey, J.; Lederrey, C.; Beljanski, M. Neoplastic characteristics of the DNA found in the plasma of cancer patients. Oncology 1989, 46, 318–322. [Google Scholar] [CrossRef]
- Sorenson, G.D.; Pribish, D.M.; Valone, F.H.; Memoli, V.A.; Bzik, D.J.; Yao, S.L. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol. Biomark. Prev. 1994, 3, 67–71. [Google Scholar]
- Jahr, S.; Hentze, H.; Englisch, S.; Hardt, D.; Fackelmayer, F.O.; Hesch, R.D.; Knippers, R. DNA fragments in the blood plasma of cancer patients: Quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001, 61, 1659–1665. [Google Scholar]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bauerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef]
- Stroun, M.; Lyautey, J.; Lederrey, C.; Olson-Sand, A.; Anker, P. About the possible origin and mechanism of circulating DNA apoptosis and active DNA release. Clin. Chim. Acta 2001, 313, 139–142. [Google Scholar] [CrossRef]
- Stroun, M.; Maurice, P.; Vasioukhin, V.; Lyautey, J.; Lederrey, C.; Lefort, F.; Rossier, A.; Chen, X.Q.; Anker, P. The origin and mechanism of circulating DNA. Ann. N. Y. Acad. Sci. 2000, 906, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.C.; Jiang, P.; Chan, C.W.; Sun, K.; Wong, J.; Hui, E.P.; Chan, S.L.; Chan, W.C.; Hui, D.S.; Ng, S.S.; et al. Noninvasive detection of cancer-associated genome-wide hypomethylation and copy number aberrations by plasma DNA bisulfite sequencing. Proc. Natl. Acad. Sci. USA 2013, 110, 18761–18768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, S.J.; Tsui, D.W.; Murtaza, M.; Biggs, H.; Rueda, O.M.; Chin, S.F.; Dunning, M.J.; Gale, D.; Forshew, T.; Mahler-Araujo, B.; et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N. Engl. J. Med. 2013, 368, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Hindson, B.J.; Ness, K.D.; Masquelier, D.A.; Belgrader, P.; Heredia, N.J.; Makarewicz, A.J.; Bright, I.J.; Lucero, M.Y.; Hiddessen, A.L.; Legler, T.C.; et al. High-throughput droplet digital PCR system for absolute quantitation of DNA copy number. Anal. Chem. 2011, 83, 8604–8610. [Google Scholar] [CrossRef]
- Quail, M.A.; Smith, M.; Coupland, P.; Otto, T.D.; Harris, S.R.; Connor, T.R.; Bertoni, A.; Swerdlow, H.P.; Gu, Y. A tale of three next generation sequencing platforms: Comparison of Ion Torrent, Pacific Biosciences and Illumina MiSeq sequencers. BMC Genom. 2012, 13, 341. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.; Zhuge, J.; Zhang, W.W. Sensitive detection of BRAF V600E mutation by Amplification Refractory Mutation System (ARMS)-PCR. Biomark. Res. 2013, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Adler, C.; Ahammed, Z.; Allgower, C.; Amonett, J.; Anderson, B.D.; Anderson, M.; Averichev, G.S.; Balewski, J.; Barannikova, O.; Barnby, L.S.; et al. Centrality dependence of high-p(T) hadron suppression in Au+Au collisions at sqrt[s(NN)]=130 GeV. Phys. Rev. Lett. 2002, 89, 202301. [Google Scholar] [CrossRef] [Green Version]
- Milbury, C.A.; Li, J.; Makrigiorgos, G.M. PCR-based methods for the enrichment of minority alleles and mutations. Clin. Chem. 2009, 55, 632–640. [Google Scholar] [CrossRef] [Green Version]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [Green Version]
- Gidwani, R.; Franks, J.A.; Enogela, E.M.; Caston, N.E.; Williams, C.P.; Aswani, M.S.; Azuero, A.; Rocque, G.B. Survival in the Real World: A National Analysis of Patients Treated for Early-Stage Breast Cancer. JCO Oncol. Pract. 2022, 18, e235–e249. [Google Scholar] [CrossRef] [PubMed]
- Riethdorf, S.; Muller, V.; Zhang, L.; Rau, T.; Loibl, S.; Komor, M.; Roller, M.; Huober, J.; Fehm, T.; Schrader, I.; et al. Detection and HER2 expression of circulating tumor cells: Prospective monitoring in breast cancer patients treated in the neoadjuvant GeparQuattro trial. Clin. Cancer Res. 2010, 16, 2634–2645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xenidis, N.; Ignatiadis, M.; Apostolaki, S.; Perraki, M.; Kalbakis, K.; Agelaki, S.; Stathopoulos, E.N.; Chlouverakis, G.; Lianidou, E.; Kakolyris, S.; et al. Cytokeratin-19 mRNA-positive circulating tumor cells after adjuvant chemotherapy in patients with early breast cancer. J. Clin. Oncol. 2009, 27, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Sandri, M.T.; Zorzino, L.; Cassatella, M.C.; Bassi, F.; Luini, A.; Casadio, C.; Botteri, E.; Rotmensz, N.; Adamoli, L.; Nole, F. Changes in circulating tumor cell detection in patients with localized breast cancer before and after surgery. Ann. Surg. Oncol. 2010, 17, 1539–1545. [Google Scholar] [CrossRef]
- Serrano, M.J.; Rovira, P.S.; Martinez-Zubiaurre, I.; Rodriguez, M.D.; Fernandez, M.; Lorente, J.A. Dynamics of circulating tumor cells in early breast cancer under neoadjuvant therapy. Exp. Ther. Med. 2012, 4, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Pierga, J.Y.; Bidard, F.C.; Mathiot, C.; Brain, E.; Delaloge, S.; Giachetti, S.; de Cremoux, P.; Salmon, R.; Vincent-Salomon, A.; Marty, M. Circulating tumor cell detection predicts early metastatic relapse after neoadjuvant chemotherapy in large operable and locally advanced breast cancer in a phase II randomized trial. Clin. Cancer Res. 2008, 14, 7004–7010. [Google Scholar] [CrossRef] [Green Version]
- Bidard, F.C.; Belin, L.; Delaloge, S.; Lerebours, F.; Ngo, C.; Reyal, F.; Alran, S.; Giacchetti, S.; Marty, M.; Lebofsky, R.; et al. Time-Dependent Prognostic Impact of Circulating Tumor Cells Detection in Non-Metastatic Breast Cancer: 70-Month Analysis of the REMAGUS02 Study. Int. J. Breast Cancer 2013, 2013, 130470. [Google Scholar] [CrossRef]
- Lucci, A.; Hall, C.S.; Lodhi, A.K.; Bhattacharyya, A.; Anderson, A.E.; Xiao, L.; Bedrosian, I.; Kuerer, H.M.; Krishnamurthy, S. Circulating tumour cells in non-metastatic breast cancer: A prospective study. Lancet Oncol. 2012, 13, 688–695. [Google Scholar] [CrossRef]
- Hall, C.; Karhade, M.; Laubacher, B.; Anderson, A.; Kuerer, H.; DeSynder, S.; Lucci, A. Circulating Tumor Cells After Neoadjuvant Chemotherapy in Stage I-III Triple-Negative Breast Cancer. Ann. Surg. Oncol. 2015, 22 (Suppl. 3), S552–S558. [Google Scholar] [CrossRef]
- Rack, B.; Schindlbeck, C.; Juckstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J. Natl. Cancer Inst. 2014, 106, dju066. [Google Scholar] [CrossRef]
- Pierga, J.Y.; Petit, T.; Levy, C.; Ferrero, J.M.; Campone, M.; Gligorov, J.; Lerebours, F.; Roche, H.; Bachelot, T.; Charafe-Jauffret, E.; et al. Pathological response and circulating tumor cell count identifies treated HER2+ inflammatory breast cancer patients with excellent prognosis: BEVERLY-2 survival data. Clin. Cancer Res. 2015, 21, 1298–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierga, J.Y.; Bidard, F.C.; Autret, A.; Petit, T.; Andre, F.; Dalenc, F.; Levy, C.; Ferrero, J.M.; Romieu, G.; Bonneterre, J.; et al. Circulating tumour cells and pathological complete response: Independent prognostic factors in inflammatory breast cancer in a pooled analysis of two multicentre phase II trials (BEVERLY-1 and -2) of neoadjuvant chemotherapy combined with bevacizumab. Ann. Oncol. 2017, 28, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.; O’Neill, A.; Alpaugh, K.; Wolff, A.C.; Northfelt, D.W.; Dang, C.T.; Sledge, G.W.; Miller, K.D. Association of Circulating Tumor Cells with Late Recurrence of Estrogen Receptor-Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.R.; Seagle, B.L.; Friedl, T.W.P.; Rack, B.; Lato, K.; Fink, V.; Cristofanilli, M.; Donnelly, E.D.; Janni, W.; Shahabi, S.; et al. Association of Circulating Tumor Cell Status with Benefit of Radiotherapy and Survival in Early-Stage Breast Cancer. JAMA Oncol. 2018, 4, e180163. [Google Scholar] [CrossRef] [Green Version]
- Trapp, E.; Janni, W.; Schindlbeck, C.; Juckstock, J.; Andergassen, U.; de Gregorio, A.; Alunni-Fabbroni, M.; Tzschaschel, M.; Polasik, A.; Koch, J.G.; et al. Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer During Follow-Up and Prognosis. J. Natl. Cancer Inst. 2019, 111, 380–387. [Google Scholar] [CrossRef]
- Rossi, T.; Gallerani, G.; Angeli, D.; Cocchi, C.; Bandini, E.; Fici, P.; Gaudio, M.; Martinelli, G.; Rocca, A.; Maltoni, R.; et al. Single-Cell NGS-Based Analysis of Copy Number Alterations Reveals New Insights in Circulating Tumor Cells Persistence in Early-Stage Breast Cancer. Cancers 2020, 12, 2490. [Google Scholar] [CrossRef]
- Beaver, J.A.; Jelovac, D.; Balukrishna, S.; Cochran, R.; Croessmann, S.; Zabransky, D.J.; Wong, H.Y.; Toro, P.V.; Cidado, J.; Blair, B.G.; et al. Detection of cancer DNA in plasma of patients with early-stage breast cancer. Clin. Cancer Res. 2014, 20, 2643–2650. [Google Scholar] [CrossRef] [Green Version]
- Riva, F.; Bidard, F.C.; Houy, A.; Saliou, A.; Madic, J.; Rampanou, A.; Hego, C.; Milder, M.; Cottu, P.; Sablin, M.P.; et al. Patient-Specific Circulating Tumor DNA Detection during Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer. Clin. Chem. 2017, 63, 691–699. [Google Scholar] [CrossRef] [Green Version]
- Phallen, J.; Sausen, M.; Adleff, V.; Leal, A.; Hruban, C.; White, J.; Anagnostou, V.; Fiksel, J.; Cristiano, S.; Papp, E.; et al. Direct detection of early-stage cancers using circulating tumor DNA. Sci. Transl Med. 2017, 9, eaan2415. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Murillas, I.; Chopra, N.; Comino-Mendez, I.; Beaney, M.; Tovey, H.; Cutts, R.J.; Swift, C.; Kriplani, D.; Afentakis, M.; Hrebien, S.; et al. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. JAMA Oncol. 2019, 5, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Murillas, I.; Schiavon, G.; Weigelt, B.; Ng, C.; Hrebien, S.; Cutts, R.J.; Cheang, M.; Osin, P.; Nerurkar, A.; Kozarewa, I.; et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci. Transl. Med. 2015, 7, 302ra133. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Murillas, I.; Turner, N.C. Clinical Benefit of Circulating Tumor DNA Analysis in Follow-up of Patients With Early-Stage Breast Cancer-Reply. JAMA Oncol. 2020, 6, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Rothe, F.; Silva, M.J.; Venet, D.; Campbell, C.; Bradburry, I.; Rouas, G.; de Azambuja, E.; Maetens, M.; Fumagalli, D.; Rodrik-Outmezguine, V.; et al. Circulating Tumor DNA in HER2-Amplified Breast Cancer: A Translational Research Substudy of the NeoALTTO Phase III Trial. Clin. Cancer Res. 2019, 25, 3581–3588. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhao, W.; Wei, W.; You, Z.; Ou, X.; Sun, M.; Yin, Y.; Tang, X.; Zhao, Z.; Hu, C.; et al. Parallel Analyses of Somatic Mutations in Plasma Circulating Tumor DNA (ctDNA) and Matched Tumor Tissues in Early-Stage Breast Cancer. Clin. Cancer Res. 2019, 25, 6546–6553. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, B.J.; Cordoba, G.D.; Aranda, A.G.; Alvarez, M.; Vicioso, L.; Perez, C.L.; Hernando, C.; Bermejo, B.; Parreno, A.J.; Lluch, A.; et al. Detection of TP53 and PIK3CA Mutations in Circulating Tumor DNA Using Next-Generation Sequencing in the Screening Process for Early Breast Cancer Diagnosis. J. Clin. Med. 2019, 8, 1183. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Hancock, B.A.; Solzak, J.P.; Brinza, D.; Scafe, C.; Miller, K.D.; Radovich, M. Next-generation sequencing of circulating tumor DNA to predict recurrence in triple-negative breast cancer patients with residual disease after neoadjuvant chemotherapy. NPJ Breast Cancer 2017, 3, 24. [Google Scholar] [CrossRef]
- Yuan, Y.; Chen, X.S.; Liu, S.Y.; Shen, K.W. Accuracy of MRI in prediction of pathologic complete remission in breast cancer after preoperative therapy: A meta-analysis. AJR Am. J. Roentgenol. 2010, 195, 260–268. [Google Scholar] [CrossRef]
- Chagpar, A.B.; Middleton, L.P.; Sahin, A.A.; Dempsey, P.; Buzdar, A.U.; Mirza, A.N.; Ames, F.C.; Babiera, G.V.; Feig, B.W.; Hunt, K.K.; et al. Accuracy of physical examination, ultrasonography, and mammography in predicting residual pathologic tumor size in patients treated with neoadjuvant chemotherapy. Ann. Surg. 2006, 243, 257–264. [Google Scholar] [CrossRef]
- McDonald, B.R.; Contente-Cuomo, T.; Sammut, S.J.; Odenheimer-Bergman, A.; Ernst, B.; Perdigones, N.; Chin, S.F.; Farooq, M.; Mejia, R.; Cronin, P.A.; et al. Personalized circulating tumor DNA analysis to detect residual disease after neoadjuvant therapy in breast cancer. Sci. Transl. Med. 2019, 11, eaax7392. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, M.; Custodio, S.; de Las Casas, M.L.; Garcia-Saenz, J.A.; de la Torre, J.C.; Bellon-Cano, J.M.; Lopez-Tarruella, S.; Vidaurreta-Lazaro, M.; de la Orden, V.; Jerez, Y.; et al. Circulating tumor cells following first chemotherapy cycle: An early and strong predictor of outcome in patients with metastatic breast cancer. Oncologist 2013, 18, 917–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidard, F.C.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Smerage, J.B.; Barlow, W.E.; Hortobagyi, G.N.; Winer, E.P.; Leyland-Jones, B.; Srkalovic, G.; Tejwani, S.; Schott, A.F.; O’Rourke, M.A.; Lew, D.L.; et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J. Clin. Oncol. 2014, 32, 3483–3489. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Pierga, J.Y.; Reuben, J.; Rademaker, A.; Davis, A.A.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; et al. The clinical use of circulating tumor cells (CTCs) enumeration for staging of metastatic breast cancer (MBC): International expert consensus paper. Crit. Rev. Oncol. Hematol. 2019, 134, 39–45. [Google Scholar] [CrossRef]
- Muller, V.; Banys-Paluchowski, M.; Friedl, T.W.P.; Fasching, P.A.; Schneeweiss, A.; Hartkopf, A.; Wallwiener, D.; Rack, B.; Meier-Stiegen, F.; Huober, J.; et al. Prognostic relevance of the HER2 status of circulating tumor cells in metastatic breast cancer patients screened for participation in the DETECT study program. ESMO Open 2021, 6, 100299. [Google Scholar] [CrossRef]
- Bidard, F.C.; Jacot, W.; Kiavue, N.; Dureau, S.; Kadi, A.; Brain, E.; Bachelot, T.; Bourgeois, H.; Goncalves, A.; Ladoire, S.; et al. Efficacy of Circulating Tumor Cell Count-Driven vs Clinician-Driven First-line Therapy Choice in Hormone Receptor-Positive, ERBB2-Negative Metastatic Breast Cancer: The STIC CTC Randomized Clinical Trial. JAMA Oncol. 2021, 7, 34–41. [Google Scholar] [CrossRef]
- Cabel, L.; Berger, F.; Cottu, P.; Loirat, D.; Rampanou, A.; Brain, E.; Cyrille, S.; Bourgeois, H.; Kiavue, N.; Deluche, E.; et al. Clinical utility of circulating tumour cell-based monitoring of late-line chemotherapy for metastatic breast cancer: The randomised CirCe01 trial. Br. J. Cancer 2021, 124, 1207–1213. [Google Scholar] [CrossRef]
- Tan, G.; Chu, C.; Gui, X.; Li, J.; Chen, Q. The prognostic value of circulating cell-free DNA in breast cancer: A meta-analysis. Medicine 2018, 97, e0197. [Google Scholar] [CrossRef]
- Shaw, J.A.; Guttery, D.S.; Hills, A.; Fernandez-Garcia, D.; Page, K.; Rosales, B.M.; Goddard, K.S.; Hastings, R.K.; Luo, J.; Ogle, O.; et al. Mutation Analysis of Cell-Free DNA and Single Circulating Tumor Cells in Metastatic Breast Cancer Patients with High Circulating Tumor Cell Counts. Clin. Cancer Res. 2017, 23, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Garcia, D.; Hills, A.; Page, K.; Hastings, R.K.; Toghill, B.; Goddard, K.S.; Ion, C.; Ogle, O.; Boydell, A.R.; Gleason, K.; et al. Plasma cell-free DNA (cfDNA) as a predictive and prognostic marker in patients with metastatic breast cancer. Breast Cancer Res. 2019, 21, 149. [Google Scholar] [CrossRef] [PubMed]
- Murtaza, M.; Dawson, S.J.; Pogrebniak, K.; Rueda, O.M.; Provenzano, E.; Grant, J.; Chin, S.F.; Tsui, D.W.Y.; Marass, F.; Gale, D.; et al. Multifocal clonal evolution characterized using circulating tumour DNA in a case of metastatic breast cancer. Nat. Commun. 2015, 6, 8760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [CrossRef] [Green Version]
- Schiff, R.; Jeselsohn, R. Is ctDNA the Road Map to the Landscape of the Clonal Mutational Evolution in Drug Resistance? Lessons from the PALOMA-3 Study and Implications for Precision Medicine. Cancer Discov. 2018, 8, 1352–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darrigues, L.; Pierga, J.Y.; Bernard-Tessier, A.; Bieche, I.; Silveira, A.B.; Michel, M.; Loirat, D.; Cottu, P.; Cabel, L.; Dubot, C.; et al. Circulating tumor DNA as a dynamic biomarker of response to palbociclib and fulvestrant in metastatic breast cancer patients. Breast Cancer Res. 2021, 23, 31. [Google Scholar] [CrossRef]
- Andre, F.; Su, F.; Solovieff, N.; Arteaga, C.L.; Hortobagyi, G.N.; Chia, S.K.; Neven, P.; Bardia, A.; Tripathy, D.; Lu, Y.S. Pooled ctDNA analysis of the MONALEESA (ML) phase III advanced breast cancer (ABC) trials. In Proceedings of the 2020 ASCO Annual Meeting I, Online, 29–31 May 2020. [Google Scholar]
- Hrebien, S.; Citi, V.; Garcia-Murillas, I.; Cutts, R.; Fenwick, K.; Kozarewa, I.; McEwen, R.; Ratnayake, J.; Maudsley, R.; Carr, T.H.; et al. Early ctDNA dynamics as a surrogate for progression-free survival in advanced breast cancer in the BEECH trial. Ann. Oncol. 2019, 30, 945–952. [Google Scholar] [CrossRef]
- Turner, N.C.; Kingston, B.; Kilburn, L.S.; Kernaghan, S.; Wardley, A.M.; Macpherson, I.R.; Baird, R.D.; Roylance, R.; Stephens, P.; Oikonomidou, O.; et al. Circulating tumour DNA analysis to direct therapy in advanced breast cancer (plasmaMATCH): A multicentre, multicohort, phase 2a, platform trial. Lancet Oncol. 2020, 21, 1296–1308. [Google Scholar] [CrossRef]
- Coombes, R.C.; Page, K.; Salari, R.; Hastings, R.K.; Armstrong, A.; Ahmed, S.; Ali, S.; Cleator, S.; Kenny, L.; Stebbing, J.; et al. Personalized Detection of Circulating Tumor DNA Antedates Breast Cancer Metastatic Recurrence. Clin. Cancer Res. 2019, 25, 4255–4263. [Google Scholar] [CrossRef] [Green Version]
- Guttery, D.S.; Page, K.; Hills, A.; Woodley, L.; Marchese, S.D.; Rghebi, B.; Hastings, R.K.; Luo, J.; Pringle, J.H.; Stebbing, J.; et al. Noninvasive detection of activating estrogen receptor 1 (ESR1) mutations in estrogen receptor-positive metastatic breast cancer. Clin. Chem. 2015, 61, 974–982. [Google Scholar] [CrossRef] [Green Version]
- Schiavon, G.; Hrebien, S.; Garcia-Murillas, I.; Cutts, R.J.; Pearson, A.; Tarazona, N.; Fenwick, K.; Kozarewa, I.; Lopez-Knowles, E.; Ribas, R.; et al. Analysis of ESR1 mutation in circulating tumor DNA demonstrates evolution during therapy for metastatic breast cancer. Sci. Transl. Med. 2015, 7, 313ra182. [Google Scholar] [CrossRef] [Green Version]
- Butler, T.M.; Johnson-Camacho, K.; Peto, M.; Wang, N.J.; Macey, T.A.; Korkola, J.E.; Koppie, T.M.; Corless, C.L.; Gray, J.W.; Spellman, P.T. Exome Sequencing of Cell-Free DNA from Metastatic Cancer Patients Identifies Clinically Actionable Mutations Distinct from Primary Disease. PLoS ONE 2015, 10, e0136407. [Google Scholar] [CrossRef] [Green Version]
- Courtney, K.D.; Corcoran, R.B.; Engelman, J.A. The PI3K pathway as drug target in human cancer. J. Clin. Oncol. 2010, 28, 1075–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, Y.; Velculescu, V.E. Oncogenic mutations of PIK3CA in human cancers. Cell Cycle 2004, 3, 1221–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wein, L.; Loi, S. Mechanisms of resistance of chemotherapy in early-stage triple negative breast cancer (TNBC). Breast 2017, 34 (Suppl. 1), S27–S30. [Google Scholar] [CrossRef]
- Burris, H.A., 3rd. Overcoming acquired resistance to anticancer therapy: Focus on the PI3K/AKT/mTOR pathway. Cancer Chemother. Pharm. 2013, 71, 829–842. [Google Scholar] [CrossRef]
- Helleday, T.; Bryant, H.E.; Schultz, N. Poly(ADP-ribose) polymerase (PARP-1) in homologous recombination and as a target for cancer therapy. Cell Cycle 2005, 4, 1176–1178. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, A.J.; Marengo, M.S.; Oltean, S.; Kemeny, G.; Bitting, R.L.; Turnbull, J.D.; Herold, C.I.; Marcom, P.K.; George, D.J.; Garcia-Blanco, M.A. Circulating tumor cells from patients with advanced prostate and breast cancer display both epithelial and mesenchymal markers. Mol. Cancer Res. 2011, 9, 997–1007. [Google Scholar] [CrossRef] [Green Version]
- Riethdorf, S.; Fritsche, H.; Muller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Coith, C.; Beck, K.; Janicke, F.; et al. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: A validation study of the CellSearch system. Clin. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Gorges, T.M.; Tinhofer, I.; Drosch, M.; Rose, L.; Zollner, T.M.; Krahn, T.; von Ahsen, O. Circulating tumour cells escape from EpCAM-based detection due to epithelial-to-mesenchymal transition. BMC Cancer 2012, 12, 178. [Google Scholar] [CrossRef] [Green Version]
- Poudineh, M.; Sargent, E.H.; Pantel, K.; Kelley, S.O. Profiling circulating tumour cells and other biomarkers of invasive cancers. Nat. Biomed. Eng 2018, 2, 72–84. [Google Scholar] [CrossRef]
- Coumans, F.A.; van Dalum, G.; Beck, M.; Terstappen, L.W. Filter characteristics influencing circulating tumor cell enrichment from whole blood. PLoS ONE 2013, 8, e61770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagrath, S.; Sequist, L.V.; Maheswaran, S.; Bell, D.W.; Irimia, D.; Ulkus, L.; Smith, M.R.; Kwak, E.L.; Digumarthy, S.; Muzikansky, A.; et al. Isolation of rare circulating tumour cells in cancer patients by microchip technology. Nature 2007, 450, 1235–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.; Bardia, A.; Wittner, B.S.; Stott, S.L.; Smas, M.E.; Ting, D.T.; Isakoff, S.J.; Ciciliano, J.C.; Wells, M.N.; Shah, A.M.; et al. Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science 2013, 339, 580–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, X.; Tao, L.; Zhang, X. A chimeric virus-based probe unambiguously detects live circulating tumor cells with high specificity and sensitivity. Mol. Ther. Methods Clin. Dev. 2021, 23, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Horimoto, Y.; Tokuda, E.; Murakami, F.; Uomori, T.; Himuro, T.; Nakai, K.; Orihata, G.; Iijima, K.; Togo, S.; Shimizu, H.; et al. Analysis of circulating tumour cell and the epithelial mesenchymal transition (EMT) status during eribulin-based treatment in 22 patients with metastatic breast cancer: A pilot study. J. Transl. Med. 2018, 16, 287. [Google Scholar] [CrossRef]
- Coumans, F.A.; Ligthart, S.T.; Uhr, J.W.; Terstappen, L.W. Challenges in the enumeration and phenotyping of CTC. Clin. Cancer Res. 2012, 18, 5711–5718. [Google Scholar] [CrossRef] [Green Version]
- Stoecklein, N.H.; Fischer, J.C.; Niederacher, D.; Terstappen, L.W. Challenges for CTC-based liquid biopsies: Low CTC frequency and diagnostic leukapheresis as a potential solution. Expert Rev. Mol. Diagn. 2016, 16, 147–164. [Google Scholar] [CrossRef]
- Tang, W.; Jiang, D.; Li, Z.; Zhu, L.; Shi, J.; Yang, J.; Xiang, N. Recent advances in microfluidic cell sorting techniques based on both physical and biochemical principles. Electrophoresis 2019, 40, 930–954. [Google Scholar] [CrossRef]
- Hyun, K.A.; Lee, T.Y.; Lee, S.H.; Jung, H.I. Two-stage microfluidic chip for selective isolation of circulating tumor cells (CTCs). Biosens. Bioelectron. 2015, 67, 86–92. [Google Scholar] [CrossRef]
- Deng, Y.; Zhang, Y.; Sun, S.; Wang, Z.; Wang, M.; Yu, B.; Czajkowsky, D.M.; Liu, B.; Li, Y.; Wei, W.; et al. An integrated microfluidic chip system for single-cell secretion profiling of rare circulating tumor cells. Sci. Rep. 2014, 4, 7499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madic, J.; Kiialainen, A.; Bidard, F.C.; Birzele, F.; Ramey, G.; Leroy, Q.; Rio Frio, T.; Vaucher, I.; Raynal, V.; Bernard, V.; et al. Circulating tumor DNA and circulating tumor cells in metastatic triple negative breast cancer patients. Int. J. Cancer 2015, 136, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Swennenhuis, J.F.; Reumers, J.; Thys, K.; Aerssens, J.; Terstappen, L.W. Efficiency of whole genome amplification of single circulating tumor cells enriched by CellSearch and sorted by FACS. Genome Med. 2013, 5, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorges, T.M.; Kuske, A.; Rock, K.; Mauermann, O.; Muller, V.; Peine, S.; Verpoort, K.; Novosadova, V.; Kubista, M.; Riethdorf, S.; et al. Accession of Tumor Heterogeneity by Multiplex Transcriptome Profiling of Single Circulating Tumor Cells. Clin. Chem. 2016, 62, 1504–1515. [Google Scholar] [CrossRef]
- Heitzer, E.; Auer, M.; Gasch, C.; Pichler, M.; Ulz, P.; Hoffmann, E.M.; Lax, S.; Waldispuehl-Geigl, J.; Mauermann, O.; Lackner, C.; et al. Complex tumor genomes inferred from single circulating tumor cells by array-CGH and next-generation sequencing. Cancer Res. 2013, 73, 2965–2975. [Google Scholar] [CrossRef] [Green Version]
- Kwan, T.T.; Bardia, A.; Spring, L.M.; Giobbie-Hurder, A.; Kalinich, M.; Dubash, T.; Sundaresan, T.; Hong, X.; LiCausi, J.A.; Ho, U.; et al. A Digital RNA Signature of Circulating Tumor Cells Predicting Early Therapeutic Response in Localized and Metastatic Breast Cancer. Cancer Discov. 2018, 8, 1286–1299. [Google Scholar] [CrossRef] [Green Version]
- Ramskold, D.; Luo, S.; Wang, Y.C.; Li, R.; Deng, Q.; Faridani, O.R.; Daniels, G.A.; Khrebtukova, I.; Loring, J.F.; Laurent, L.C.; et al. Full-length mRNA-Seq from single-cell levels of RNA and individual circulating tumor cells. Nat. Biotechnol. 2012, 30, 777–782. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.; Bardelli, A. Lesion-Directed Therapies and Monitoring Tumor Evolution Using Liquid Biopsies. Cold Spring Harb. Perspect. Med. 2017, 7, a029587. [Google Scholar] [CrossRef] [Green Version]
- Mazel, M.; Jacot, W.; Pantel, K.; Bartkowiak, K.; Topart, D.; Cayrefourcq, L.; Rossille, D.; Maudelonde, T.; Fest, T.; Alix-Panabieres, C. Frequent expression of PD-L1 on circulating breast cancer cells. Mol. Oncol. 2015, 9, 1773–1782. [Google Scholar] [CrossRef] [Green Version]
- Powell, A.A.; Talasaz, A.H.; Zhang, H.; Coram, M.A.; Reddy, A.; Deng, G.; Telli, M.L.; Advani, R.H.; Carlson, R.W.; Mollick, J.A.; et al. Single cell profiling of circulating tumor cells: Transcriptional heterogeneity and diversity from breast cancer cell lines. PLoS ONE 2012, 7, e33788. [Google Scholar] [CrossRef] [Green Version]
- Bortolini Silveira, A.; Bidard, F.C.; Tanguy, M.L.; Girard, E.; Tredan, O.; Dubot, C.; Jacot, W.; Goncalves, A.; Debled, M.; Levy, C.; et al. Multimodal liquid biopsy for early monitoring and outcome prediction of chemotherapy in metastatic breast cancer. NPJ Breast Cancer 2021, 7, 115. [Google Scholar] [CrossRef]
- Keup, C.; Suryaprakash, V.; Hauch, S.; Storbeck, M.; Hahn, P.; Sprenger-Haussels, M.; Kolberg, H.C.; Tewes, M.; Hoffmann, O.; Kimmig, R.; et al. Integrative statistical analyses of multiple liquid biopsy analytes in metastatic breast cancer. Genome Med. 2021, 13, 85. [Google Scholar] [CrossRef] [PubMed]
- Radovich, M.; Jiang, G.; Hancock, B.A.; Chitambar, C.; Nanda, R.; Falkson, C.; Lynce, F.C.; Gallagher, C.; Isaacs, C.; Blaya, M.; et al. Association of Circulating Tumor DNA and Circulating Tumor Cells After Neoadjuvant Chemotherapy with Disease Recurrence in Patients With Triple-Negative Breast Cancer: Preplanned Secondary Analysis of the BRE12-158 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Mujoo, K.; Lucci, A. Therapeutics of Oxidative Stress and Stemness in Breast Cancer. In Handbook of Oxidative Stress in Cancer: Mechanistic Aspects; Chakraborti, S., Ray, B.K., Roychowdhury, S., Eds.; Springer: Singapore, 2020; pp. 1–12. [Google Scholar] [CrossRef]
- Singh, B.; Sarli, V.N.; Lucci, A. Inhibition of resistant triple-negative breast cancer cells with low-dose 6-mercaptopurine and 5-azacitidine. Oncotarget 2021, 12, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Sarli, V.N.; Washburn, L.J.; Raythatha, M.R.; Lucci, A. A usable model of “decathlon winner” cancer cells in triple-negative breast cancer: Survival of resistant cancer cells in quiescence. Oncotarget 2018, 9, 11071–11082. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors [Reference] | Study Design | Method | Findings |
|---|---|---|---|
| Riethdorf, S., et al., 2010 [32] | CTCs before and after neoadjuvant chemotherapy | CellSearch | 1 or more CTC detected in 21.6% patients before NACT. 1 or more CTC detected in 10.6% patients after NACT. No correlation between CTC detection and clinicopathological features. No association between CTC levels and treatment response. |
| Xenidis, N., et al., 2009 [33] | CK-19 mRNA-positive CTCs before and after adjuvant chemotherapy | RT-PCR | CK-19 mRNA+ CTCs detected in 41% patients before adjuvant chemotherapy. CK-19 mRNA+ CTCs detected in 32.7% patients after adjuvant chemotherapy. CK-19 mRNA+ CTCs associated with more than 3 involved axillary lymph nodes. CK-19 mRNA+ CTCs post-adjuvant chemotherapy associated with chemotherapy-resistant residual disease. CK-19 mRNA+ CTCs post-adjuvant chemotherapy associated with decreased DFS and OS. |
| Sandri, M.T., et al., 2010 [34] | CTCs before and after surgery | CellSearch | CTCs detected in 30% of patients before and after surgery.CTCs detected pre-surgery associated with positive vascular invasion. |
| Serrano, M.J., et al., 2012 [35] | CTCs before and after neoadjuvant chemotherapy | Ficoll gradient Immunomagnetic cell separation CK 7, 8, 18, 19, anti-CK FITC | CTCs detected in 71% patients pre-NACT. CTCs detected in 54% patients post-NACT. CTCs detected pre- and post-NACT associated with increased risk of recurrence. |
| Pierga, J.Y., et al., 2008 [36] | CTCs in patients with large operable or locally advanced breast cancer before and after neoadjuvant chemotherapy | CellSearch | CTCs detected in 23% patients pre-NACT. CTCs detected in 17% patients post-NACT. No association between CTC and primary tumor response. CTCs independently associated with early relapse. |
| Bidard, F.C., et al., 2013 [37] | CTCs before and after NACT | CellSearch | CTCs detected pre-NACT associated with disease metastatic free survival (DMFS)and OS. CTCs detected post-NACT had no impact. CTCs independently associated with significantly worse outcome during first 3 years of follow-up. |
| Lucci, A., et al., 2012 [38] | CTCs at time of surgery in chemonaive early stage breast cancer | CellSearch | CTCs detected in 24% of patients at surgery. CTCs associated with decreased PFS and OS. |
| Hall, C., et al., 2015 [39] | CTCs after NACT in TNBC | CellSearch | CTCs detected in 30% of patients after NACT. CTCs associated with decreased RFS and OS. |
| Rack, B., et al., 2014 [40] | CTCs before and after adjuvant chemotherapy | CellSearch | CTCs detected in 21.5% of patients pre-adjuvant chemotherapy. CTCs detected in 22.1% of patients post-adjuvant chemotherapy. CTCs before and after adjuvant therapy independently associated with decreased disease-free survival and overall survival. |
| Pierga, J.Y., et al., 2015 [41] | CTCs in HER2+ IBC before, during, after NACT | CellSearch | CTCs at baseline independently associated with 3-year disease free survival. No CTC detected at baseline = 81% DFS. 1 or more CTC detected at baseline = 43% DFS. |
| Pierga, J.Y., et al., 2017 [42] | CTCs in HER2+ IBC before, during, after NACT (pooled analysis) | CellSearch | CTCs detected in 39% of patients at baseline. CTCs detected in 9% of patients after 4 cycles of chemotherapy. No correlation between CTC and pCR. CTCs detected as baseline associated with decreased 3-year DFS and OS. |
| Sparano, J., et al., 2018 [43] | CTCs at 5-years after diagnosis in ER+, HER2- | CellSearch | CTCs detected in 5.1% of patients 5 years after diagnosis.CTCs independently associated with increased risk of recurrence 5 years after diagnosis. |
| Goodman, C.R., et al., 2018 [44] | CTCs and radiotherapy in early stage breast cancer | CellSearch | At least 1 CTC and treated with radiotherapy associated with increased RFS, DFS, and OS. |
| Trapp, E., et al., 2019 [45] | CTCs before and 2 years after adjuvant chemotherapy | CellSearch | CTCs detected in 18.2% of patients 2 years after chemotherapy. CTCs detected 2 years after chemotherapy associated with decreased OS and DFS. |
| Rossi, T., et al., 2020 [46] | Copy number alterations of CTCs pre-surgery, 1-month post-surgery, and 6-months post-surgery | OncoQuick DEPArray | CTCs presented different levels of copy number alterations based on timepoint and cancer subtype. CTCs 6 months post-surgery shared copy number alterations with primary tumor. |
| Authors [Reference] | Study Design | Method | Findings |
|---|---|---|---|
| Beaver, J.A., et al., 2014 [47] | PIK3CA in pre- and post-surgery plasma samples | ddPCR | ctDNA detectable in plasma. Of 15 PIK3CA mutations detected in tumors, 14 were detected in pre-surgery plasma. No mutations detected in wild-type PIK3CA plasma. Sensitivity: 93.3%, specificity: 100% |
| Riva, F., et al., 2017 [48] | ctDNA in TNBC before NACT, after 1 cycle, pre-surgery, post-surgery | ddPCR | ctDNA detected in 75% of patients at baseline. ctDNA decreased during NACT. Minimal decrease in ctDNA level during NACT associated with shorter DFS and OS. |
| Phallen, J., et al., 2017 [49] | ctDNA at primary diagnosis | TEC-Seq | ctDNA detected in 56% stage I-III BC patients. ctDNA detected had high concordance with alterations detected in tumor tissue. |
| Cohen, J.D., et al., 2018 [50] | ctDNA at primary diagnosis | QIASymphony CancerSEEK | 33% sensitivity in breast cancer. |
| Garcia-Murillas, I., et al., 2019 [51] | ctDNA before, during, and after NACT | ddPCR | ctDNA detected at baseline associated with RFS. ctDNA detected during follow-up associated with increased risk of relapse. |
| Garcia-Murillas, I., et al., 2015 [52] | ctDNA after NACT | ddPCR | ctDNA detected at post-surgical time point or during follow-ups increased risk of relapse. Serial ctDNA predicted relapse with median lead time of 7.9 months over clinical relapse. |
| Rothe, F., et al., 2019 [54] | ctDNA before, at week 2, and after NACT in HER2+ patients | ddPCR | ctDNA detected in 41% of patients at baseline. ctDNA detected in 20% of patients at week 2. ctDNA detected in 5% of patients post-NACT. ctDNA detected at baseline associated with decreased pCR. |
| Zhang, X., et al., 2019 [55] | ctDNA before and after adjuvant chemotherapy | AmpliSeq | ctDNA detected after surgery associated with increased lymph node metasis. ctDNA positivity decreased after chemotherapy in TNBC and HER2+. ctDNA positivity persistent after chemotherapy in ER+. |
| Rodriguez, B.J., et al., 2019 [56] | TP53 and PIK3CA in plasma and tissue at diagnosis | SafeSEQ | Matched plasma and tumor mutations detected in 27.6% of patients at diagnosis. Four ctDNA mutations identified in plasma but not in tumor tissue. Clinicopathological features significantly associated with ctDNA detection. |
| Chen, Y.H., et al., 2017 [57] | ctDNA in patients with residual disease after NACT | Oncomine Research Panel | Mutations identified in tumor tissue of 33/38 patients. ctDNA detected in 4/33 patients. All 4 patients relapsed (100% specificity). 13 patients in total relapsed (31% sensitivity). ctDNA detected in patients with residual disease associated with decreased DFS. |
| McDonald, B.R., et al., 2019 [60] | ctDNA before, during, and after NACT | TARDIS | ctDNA detected in 100% of patients before treatment. ctDNA concentrations decreased during treatment and were lower overall for patients who achieved pCR. |
| Authors [Reference] | Study Design | Method | Findings |
|---|---|---|---|
| Martin, M., et al., 2013 [62] | CTCs at baseline and before second cycle of chemotherapy | CellSearch | n = 99. Detection of CTCs before the second cycle of chemotherapy is an early and powerful predictor of treatment outcome. Patients with 0–4 CTCs had a significantly better OS, PFS, and clinical benefit rate than patients with ≥5 CTCs |
| Bidard, F.C., et al., 2014 [63] | CTCs before, during, and after treatment | CellSearch | n = 911. Patients with ≥5 CTCs before treatment had a decreased PFS and OS compared to patients with <5 CTCs. An increase in CTCs 3–5 weeks and 6–8 weeks after treatment correlated with shorter PFS and OS. |
| Smerage, J.B., et al., 2014 [64] | CTCs before treatment and 21 days into treatment | CellSearch | n = 595. After 21 days of treatment, patients with increased CTCs compared to baseline were randomly assigned to receive either initial therapy or an alternate therapy. Switching cytotoxic therapies based on an increase in CTCs did not result in a longer OS compared to patients with persistently elevated CTCs. |
| Cristofanilli, M., et al., 2019 [65] | CTCs for stratification of patients | CellSearch | n = 2436. Patients who had ≥5 CTCs were classified as Stage IV aggressive, while patients with 1–4 CTCs were classified as stage IV indolent. The stage IV indolent group had a longer median OS across all disease subtypes. |
| Muller, V., et al., 2021 [66] | CTCs at baseline with HER2 phenotype staining | CellSearch | n = 1933. Detection of one of more CTCs with strong HER2 staining was associated with a shorter OS compared to patients with negative-to-moderate HER2 staining. CTC status independently predicted OS. |
| Bidard, F.C., et al., 2021 [67] | CTC-driven treatment vs. clinician-driven treatment | CellSearch | n = 78. Median PFS was slightly longer in the CTC-driven treatment arm than in the clinician-driven treatment arm. |
| Cabel, L., et al., 2021 [68] | CTC-based monitoring after first-line therapy | CellSearch | n = 207. This study failed to demonstrate the clinical utility of CTC monitoring in metastatic breast cancer due to limited accrual and compliance. |
| Authors [Reference] | Study Design | Method | Findings |
|---|---|---|---|
| Tan, G., et al., 2018 [69] | Meta-analysis of 10 different studies | n = 1127. There was a strong association between cfDNA and OS, DFS, and RFS. Subgroup analyses confirmed the role of cfDNA as a strong prognostic marker regardless of cfDNA analyses, sampling time, sample source, detection method, tumor stage, sample size, or area. | |
| Shaw, J.A., et al., 2017 [70] | Comparison of cfDNA profiles to isolated CTCs | NGS and ddPCR | n = 5. Total cfDNA levels were significantly associated with OS. In all 5 patients, cfDNA profiles matched the mutations found in matched, isolated CTCs (apart from two additional mutations that may have been acquired with disease progression). |
| Fernandez-Garcia, D., et al., 2019 [71] | ctDNA with CTCs | qPCR | n = 94. Level of total cfDNA is a strong predictor of OS, PFS, and disease relapse (when comparing responders to non-responders). Combining CTC and cfDNA levels is a stronger biomarker for OS than the combination of CA15-3 and AP. |
| Murtaza, M., et al., 2015 [72] | cfDNA throughout treatment plan to evaluate clonal evolution | ddPCR and Whole Exome Sequencing | n = 1. Changes in serial collections of cfDNA throughout treatment correlate with different treatment responses between sites of metastatic disease, allowing cfDNA to provide real-time information of multifocal clonal evolution. |
| Darrigues, L., et al., 2021 [75] | cfDNA before, during, after treatment and at disease progression | ddPCR | n = 61. Serial analyses of cfDNA is an effective tool to measure treatment response to palbociclib and fulvestrant in ER+ metastatic breast cancer. Early variations in levels of cfDNA is a prognostic factor of PFS. |
| Fabrice Andre, F.S., et al., 2020 [76] | ctDNA at baseline | NGS | n = 1053. Genetic alterations from ctDNA can serve as potential biomarkers of response or resistance in metastatic breast cancer. |
| Hrebien, S., et al., 2019 [77] | ctDNA levels at baseline and early treatment | ddCPR | n = 59. Early changes in ctDNA dynamics were a strong indicator for PFS |
| Turner, N.C., et al., 2020 [78] | ctDNA before treatment | ddPCR and targeted sequencing | n = 1034. Concordance between ddPCR and targeted sequencing of ctDNA was 96–99%, and sensitivity of ddPCR ctDNA mutations identified in tissue sequencing was 98%. Three of the four treatment arms met or exceeded target response rate, demonstrating that ctDNA testing offers accurate and rapid genotyping that can allow the selection of mutation-directed treatments for metastatic breast cancer patients. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Addanki, S.; Meas, S.; Sarli, V.N.; Singh, B.; Lucci, A. Applications of Circulating Tumor Cells and Circulating Tumor DNA in Precision Oncology for Breast Cancers. Int. J. Mol. Sci. 2022, 23, 7843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23147843
Addanki S, Meas S, Sarli VN, Singh B, Lucci A. Applications of Circulating Tumor Cells and Circulating Tumor DNA in Precision Oncology for Breast Cancers. International Journal of Molecular Sciences. 2022; 23(14):7843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23147843
Chicago/Turabian StyleAddanki, Sridevi, Salyna Meas, Vanessa Nicole Sarli, Balraj Singh, and Anthony Lucci. 2022. "Applications of Circulating Tumor Cells and Circulating Tumor DNA in Precision Oncology for Breast Cancers" International Journal of Molecular Sciences 23, no. 14: 7843. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23147843