
Vitamin D and the Kidney: Two Players, One Console

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Vitamin D in Bone Homeostasis
3. Vitamin D in Chronic Kidney Disease and End Stage Renal Disease
4. Vitamin D and CKD-MBD
5. Effect of Vitamin D Therapy
6. Vitamin D and Kidney Transplantation
7. Immunomodulatory Effects of Vitamin D
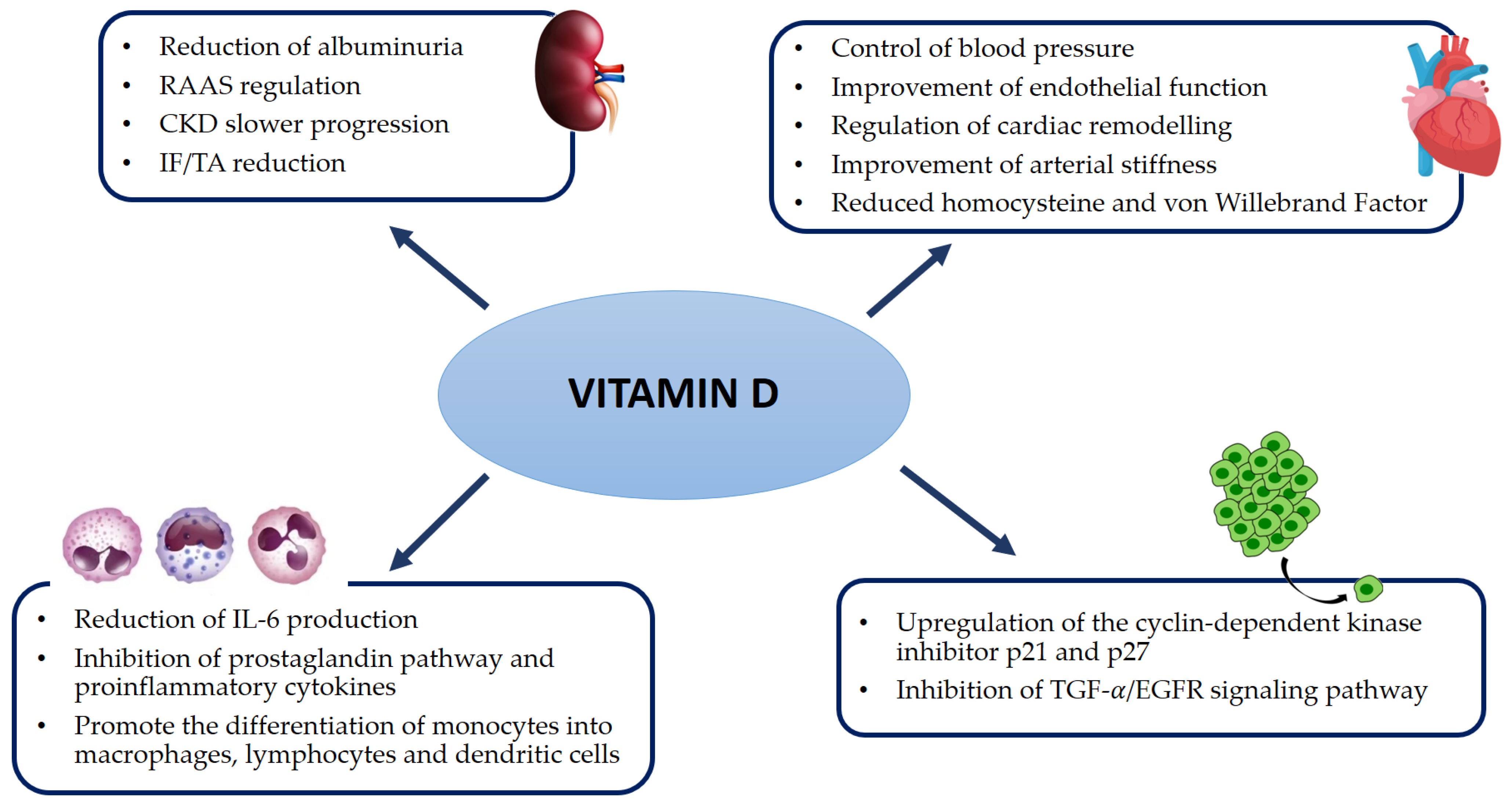
8. Pleiotropic Effects of Vitamin D
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heaney, R.P. Vitamin D in Health and Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1535–1541. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. High Prevalence of Vitamin D Inadequacy and Implications for Health. Mayo Clin. Proc. 2006, 81, 353–373. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; DeMay, M. Vitamin D and Human Health: Lessons from Vitamin D Receptor Null Mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Prosser, D.E.; Kaufmann, M. Cytochrome P450-mediated metabolism of vitamin D. J. Lipid Res. 2014, 55, 13–31. [Google Scholar] [CrossRef]
- Zierold, C.; Nehring, J.A.; Deluca, H.F. Nuclear receptor 4A2 and C/EBPβ regulate the parathyroid hormone-mediated transcriptional regulation of the 25-hydroxyvitamin D3-1α-hydroxylase. Arch. Biochem. Biophys. 2007, 460, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Perwad, F.; Azam, N.; Zhang, M.Y.; Yamashita, T.; Tenenhouse, H.S.; Portale, A.A. Dietary and Serum Phosphorus Regulate Fibroblast Growth Factor 23 Expression and 1,25-Dihydroxyvitamin D Metabolism in Mice. Endocrinology 2005, 146, 5358–5364. [Google Scholar] [CrossRef]
- Kumar, R.; Tebben, P.J.; Thompson, J.R. Vitamin D and the kidney. Arch. Biochem. Biophys. 2012, 523, 77–86. [Google Scholar] [CrossRef]
- Caudarella, R.; Vescini, F.; Buffa, A.; Sinicropi, G.; Rizzoli, E.; La Manna, G.; Stefoni, S. Bone mass loss in calcium stone disease: Focus on hypercalciuria and metabolic factors. J. Nephrol. 2003, 16, 260–266. [Google Scholar] [PubMed]
- Friedman, P.A.; Gesek, F.A. Cellular calcium transport in renal epithelia: Measurement, mechanisms, and regulation. Physiol. Rev. 1995, 75, 429–471. [Google Scholar] [CrossRef]
- Borke, J.L.; Penniston, J.T.; Kumar, R. Recent advances in calcium transport by the kidney. Semin. Nephrol. 1990, 10, 15–23. [Google Scholar] [PubMed]
- Khazai, N.; Judd, S.E.; Tangpricha, V. Calcium and vitamin D: Skeletal and extraskeletal health. Curr. Rheumatol. Rep. 2008, 10, 110–117. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Capelli, I.; Cianciolo, G.; Gasperoni, L.; Galassi, A.; Ciceri, P.; Cozzolino, M. Nutritional vitamin D in CKD: Should we measure? Should we treat? Clin. Chim. Acta 2020, 501, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Morrone, L.F.; Bolasco, P.; Camerini, C.; Cianciolo, G.; Cupisti, A.; Galassi, A.; Mazzaferro, S.; Russo, D.; Russo, L.; Cozzolino, M. Vitamin D in patients with chronic kidney disease: A position statement of the Working Group “Trace Elements and Mineral Metabolism” of the Italian Society of Nephrology. J. Nephrol. 2016, 29, 305–328. [Google Scholar] [CrossRef]
- Kogawa, M.; Findlay, D.M.; Anderson, P.H.; Ormsby, R.; Vincent, C.; Morris, H.A.; Atkins, G.J. Osteoclastic Metabolism of 25(OH)-Vitamin D3: A Potential Mechanism for Optimization of Bone Resorption. Endocrinology 2010, 151, 4613–4625. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.H.; Atkins, G.J.; Turner, A.G.; Kogawa, M.; Findlay, D.M.; Morris, H.A. Vitamin D metabolism within bone cells: Effects on bone structure and strength. Mol. Cell. Endocrinol. 2011, 347, 42–47. [Google Scholar] [CrossRef]
- Cianciolo, G.; Cappuccilli, M.; Tondolo, F.; Gasperoni, L.; Zappulo, F.; Barbuto, S.; Iacovella, F.; Conte, D.; Capelli, I.; La Manna, G. Vitamin D Effects on Bone Homeostasis and Cardiovascular System in Patients with Chronic Kidney Disease and Renal Transplant Recipients. Nutrients 2021, 13, 1453. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef]
- Lips, P.; van Schoor, N.M. The effect of vitamin D on bone and osteoporosis. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Fusaro, M.; Aghi, A.; Mereu, M.C.; Giusti, A. Fratture da fragilità nella Malattia Renale Cronica (MRC) [Fragility fracture in the Chronic Kidney Disease (CKD)]. G. Ital. Nefrol. 2017, 6, 34. [Google Scholar]
- Pazianas, M.; Miller, P.D. Osteoporosis and Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD): Back to Basics. Am. J. Kidney Dis. 2021, 78, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Felsenberg, D.; Boonen, S. The bone quality framework: Determinants of bone strength and their interrelationships, and implications for osteoporosis management. Clin. Ther. 2005, 27, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hampson, G.; Elder, G.J.; Cohen-Solal, M.; Abrahamsen, B. A review and perspective on the assessment, management and prevention of fragility fractures in patients with osteoporosis and chronic kidney disease. Endocrine 2021, 73, 509–529. [Google Scholar] [CrossRef] [PubMed]
- Peugh, J.; Khalil, A.; Chan, M.R.; Hansen, K.E. Teriparatide Treatment for Hypercalcemia Associated With Adynamic Bone Disease. JBMR Plus 2019, 3, e10176. [Google Scholar] [CrossRef]
- Kawahara, M.; Iwasaki, Y.; Sakaguchi, K.; Taguchi, T.; Nishiyama, M.; Nigawara, T.; Tsugita, M.; Kambayashi, M.; Suda, T.; Hashimoto, K. Predominant role of 25OHD in the negative regulation of PTH expression: Clinical relevance for hypovitaminosis D. Life Sci. 2008, 82, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Arcidiacono, M.V.; Yang, J.; Fernandez, E.; Dusso, A. The induction of C/EBP contributes to vitamin D inhibition of ADAM17 expression and parathyroid hyperplasia in kidney disease. Nephrol. Dial. Transplant. 2015, 30, 423–433. [Google Scholar] [CrossRef]
- Wolf, M.; Shah, A.; Gutierrez, O.; Ankers, E.; Monroy, M.; Tamez, H.; Steele, D.; Chang, Y.; Camargo, C.A., Jr.; Tonelli, M.; et al. Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int. 2007, 72, 1004–1013. [Google Scholar] [CrossRef]
- Sözen, T.; Özışık, L.; Başaran, N.Ç. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Moe, S.; Drüeke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Olgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G.; et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Mizobuchi, M.; Ogata, H.; Hatamura, I.; Saji, F.; Koiwa, F.; Kinugasa, E.; Koshikawa, S.; Akizawa, T. Activation of calcium-sensing receptor accelerates apoptosis in hyperplastic parathyroid cells. Biochem. Biophys. Res. Commun. 2007, 362, 11–16. [Google Scholar] [CrossRef]
- Aloia, J.; Dhaliwal, R.; Mikhail, M.; Shieh, A.; Stolberg, A.; Ragolia, L.; Fazzari, M.; Abrams, S.A. Free 25(OH)D and Calcium Absorption, PTH, and Markers of Bone Turnover. J. Clin. Endocrinol. Metab. 2015, 100, 4140–4145. [Google Scholar] [CrossRef]
- Shieh, A.; Ma, C.; Chun, R.F.; Wittwer-Schegg, J.; Swinkels, L.; Huijs, T.; Wang, J.; Donangelo, I.; Hewison, M.; Adams, J.S. Associations Between Change in Total and Free 25-Hydroxyvitamin D With 24,25-Dihydroxyvitamin D and Parathyroid Hormone. J. Clin. Endocrinol. Metab. 2018, 103, 3368–3375. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.; Binongo, J.N.; Ziegler, T.R.; Schlanger, L.E.; Wang, W.; Someren, J.T.; Tangpricha, V. Cholecalciferol (Vitamin D3) Therapy and Vitamin D Insufficiency in Patients with Chronic Kidney Disease: A Randomized Controlled Pilot Study. Endocr. Pract. 2008, 14, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, P.A.; Sterner, G.; Ljunggren, O.; Isaksson, E.; Elvarson, F.; Dezfoolian, H.; Linde, T. High doses of cholecalciferol alleviate the progression of hyperparathyroidism in patients with CKD Stages 3–4: Results of a 12-week double-blind, randomized, controlled study. Nephrol. Dial. Transplant. 2018, 33, 466–471. [Google Scholar] [CrossRef]
- Massart, A.; Debelle, F.D.; Racapé, J.; Gervy, C.; Husson, C.; Dhaene, M.; Wissing, K.M.; Nortier, J.L. Biochemical Parameters After Cholecalciferol Repletion in Hemodialysis: Results From the VitaDial Randomized Trial. Am. J. Kidney Dis. 2014, 64, 696–705. [Google Scholar] [CrossRef]
- Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of Daily, Weekly, and Monthly Vitamin D3 in Ethanol Dosing Protocols for Two Months in Elderly Hip Fracture Patients. J. Clin. Endocrinol. Metab. 2008, 93, 3430–3435. [Google Scholar] [CrossRef]
- Kandula, P.; Dobre, M.; Schold, J.D.; Schreiber, M.J., Jr.; Mehrotra, R.; Navaneethan, S.D. Vitamin D Supplementation in Chronic Kidney Disease: A Systematic Review and Meta-Analysis of Observational Studies and Randomized Controlled Trials. Clin. J. Am. Soc. Nephrol. 2011, 6, 50–62. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Law, J.; Coakley, K.E.; Zughaier, S.M.; Hao, L.; Shahid Salles, K.; Wasse, H.; Gutiérrez, O.M.; Ziegler, T.R.; Tangpricha, V. High-dose cholecalciferol reduces parathyroid hormone in patients with early chronic kidney disease: A pilot, randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2012, 96, 672–679. [Google Scholar] [CrossRef]
- Cupisti, A.; Egidi, M.F.; Vigo, V.; Baronti, M.E.; D’Alessandro, C.; Ghiadoni, L. Vitamin D status and cholecalciferol supplementation in chronic kidney disease patients: An Italian cohort report. Int. J. Nephrol. Renovacs. Dis. 2015, 8, 151–157. [Google Scholar] [CrossRef]
- Jean, G.; Vanel, T.; Terrat, J.C.; Chazot, C. Prevention of secondary hyperparathyroidism in hemodialysis patients: The key role of native vitamin D supplementation. Hemodial. Int. 2010, 14, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Aytac, M.B.; Deveci, M.; Bek, K.; Kayabey, O.; Ekinci, Z. Effect of cholecalciferol on local arterial stiffness and endothelial dysfunction in children with chronic kidney disease. Pediatr. Nephrol. 2016, 31, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Karakas, Y.; Sahin, G.; Urfali, F.E.; Bal, C.; Degirmenci, N.A.; Sirmagul, B. Effect of vitamin D supplementation on endothelial dysfunction in hemodialysis patients. Hemodial. Int. 2017, 21, 97–106. [Google Scholar] [CrossRef]
- Kim, M.J.; Frankel, A.H.; Donaldson, M.; Darch, S.J.; Pusey, C.D.; Hill, P.D.; Mayr, M.; Tam, F.W. Oral cholecalciferol decreases albuminuria and urinary TGF-β1 in patients with type 2 diabetic nephropathy on established renin–angiotensin–aldosterone system inhibition. Kidney Int. 2011, 80, 851–860. [Google Scholar] [CrossRef]
- Meireles, M.S.; Kamimura, M.A.; Dalboni, M.A.; Giffoni de Carvalho, J.T.; Aoike, D.T.; Cuppari, L. Effect of cholecalciferol on vitamin D-regulatory proteins in monocytes and on inflammatory markers in dialysis patients: A randomized controlled trial. Clin. Nutr. 2016, 35, 1251–1258. [Google Scholar] [CrossRef]
- Mann, M.C.; Hobbs, A.J.; Hemmelgarn, B.R.; Roberts, D.J.; Ahmed, S.B.; Rabi, D.M. Effect of oral vitamin D analogs on mortality and cardiovascular outcomes among adults with chronic kidney disease: A meta-analysis. Clin. Kidney J. 2015, 8, 41–48. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2014, CD007470. [Google Scholar] [CrossRef]
- Cianciolo, G.; Galassi, A.; Capelli, I.; Angelini, M.L.; La Manna, G.; Cozzolino, M. Vitamin D in Kidney Transplant Recipients: Mechanisms and Therapy. Am. J. Nephrol. 2016, 43, 397–407. [Google Scholar] [CrossRef]
- Obi, Y.; Hamano, T.; Ichimaro, N.; Tomida, K.; Matsui, I.; Fujii, N.; Okumi, M.; Kaimori, J.-Y.; Yazawa, K.; Kokado, Y. Vitamin D deficiency predicts decline in kidney allograft function: A prospective cohort study. J. Clin. Endocrinol. Metab. 2014, 99, 527–535. [Google Scholar] [CrossRef]
- Lee, J.R.; Dadhania, D.; August, P.; Lee, J.B.; Suthanthiran, M.; Muthukumar, T. Circulating levels of 25-hydroxyvitamin D and acute cellular rejection in kidney allograft recipients. Transplantation 2014, 98, 292–299. [Google Scholar] [CrossRef]
- Filipov, J.J.; Zlatkov, B.K.; Dimitrov, E.P.; Svinarov, D.A. Higher 25-Hydroxyvitamin D Levels Are Associated With Lower Proteinuria in Kidney Transplant Recipients. Exp. Clin. Transplant. 2016, 14, 629–633. [Google Scholar] [PubMed]
- Courbebaisse, M.; Souberbielle, J.-C.; Thervet, E. Potential Nonclassical Effects of Vitamin D in Transplant Recipients. Transplantation 2010, 89, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Courbebaisse, M.; Xu-Dubois, Y.-C.; Thervet, E.; Prié, D.; Zuber, J.; Kreis, H.; Legendre, C.; Rondeau, E.; Pallet, N. Cholecalciferol Supplementation Does Not Protect Against Renal Allograft Structural and Functional Deterioration: A Retrospective Study. Transplantation 2011, 91, 207–212. [Google Scholar] [CrossRef]
- Westenfeld, R.; Schlieper, G.; Wöltje, M.; Gawlik, A.; Brandenburg, V.; Rutkowski, P.; Floege, J.; Jahnen-Dechent, W.; Ketteler, M. Impact of sirolimus, tacrolimus and mycophenolate mofetil on osteoclastogenesis--implications for post-transplantation bone disease. Nephrol. Dial. Transplant. 2011, 26, 4115–4123. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef]
- Cantorna, M.T.; Snyder, L.; Lin, Y.-D.; Yang, L. Vitamin D and 1,25(OH)2D Regulation of T cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef]
- Bhalla, A.K.; Amento, E.P.; Clemens, T.L.; Holick, M.F.; Krane, S.M. Specific high-affinity receptors for 1,25-dihydroxyvitamin D3 in human peripheral blood mononuclear cells: Presence in monocytes and induction in T lymphocytes following activation. J. Clin. Endocrinol. Metab. 1983, 57, 1308–1310. [Google Scholar] [CrossRef]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef]
- Kim, E.W.; Teles, R.M.B.; Haile, S.; Liu, P.T.; Modlin, R.L. Vitamin D status contributes to the antimicrobial activity of macrophages against Mycobacterium leprae. PLOS Neglected Trop. Dis. 2018, 12, e0006608. [Google Scholar] [CrossRef]
- Piemonti, L.; Monti, P.; Sironi, M.; Fraticelli, P.; Leone, B.E.; Dal Cin, E.; Allavena, P.; Di Carlo, V. Vitamin D3 Affects Differentiation, Maturation, and Function of Human Monocyte-Derived Dendritic Cells. J. Immunol. 2000, 164, 4443–4451. [Google Scholar] [CrossRef]
- Chen, L.; Eapen, M.S.; Zosky, G.R. Vitamin D both facilitates and attenuates the cellular response to lipopolysaccharide. Sci. Rep. 2017, 7, 45172. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.D.; Lutz, W.H.; Phan, V.A.; Bachman, L.A.; McKean, D.J.; Kumar, R. Potent Inhibition of Dendritic Cell Differentiation and Maturation by Vitamin D Analogs. Biochem. Biophys. Res. Commun. 2000, 270, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Bartels, L.E.; Hvas, C.L.; Agnholt, J.; Dahlerup, J.F.; Agger, R. Human dendritic cell antigen presentation and chemotaxis are inhibited by intrinsic 25-hydroxy vitamin D activation. Int. Immunopharmacol. 2010, 10, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Dam, T.N.; Møller, B.; Hindkjaer, J.; Kragballe, K. The vitamin D3 analog calcipotriol suppresses the number and antigen-presenting function of Langerhans cells in normal human skin. J. Investig. Dermatol. Symp. Proc. 1996, 1, 72–77. [Google Scholar]
- Rolf, L.; Muris, A.-H.; Hupperts, R.; Damoiseaux, J. Vitamin D effects on B cell function in autoimmunity. Ann. N. Y. Acad. Sci. 2014, 1317, 84–91. [Google Scholar] [CrossRef]
- Chen, S.; Sims, G.P.; Chen, X.X.; Gu, Y.Y.; Chen, S.; Lipsky, P.E. Modulatory Effects of 1,25-Dihydroxyvitamin D3on Human B Cell Differentiation. J. Immunol. 2007, 179, 1634–1647. [Google Scholar] [CrossRef]
- Morgan, J.W.; Kouttab, N.; Ford, D.; Maizel, A.L. Vitamin D-Mediated Gene Regulation in Phenotypically Defined Human B Cell Subpopulations. Endocrinology 2000, 141, 3225–3234. [Google Scholar] [CrossRef]
- Levin, G.P.; Robinson-Cohen, C.; de Boer, I.H.; Houston, D.K.; Lohman, K.; Liu, Y.; Kritchevsky, S.B.; Cauley, J.A.; Tanaka, T.; Ferrucci, L.; et al. Genetic Variants and Associations of 25-Hydroxyvitamin D Concentrations With Major Clinical Outcomes. JAMA 2012, 308, 1898–1905. [Google Scholar] [CrossRef]
- Galassi, A.; Bellasi, A.; Auricchio, S.; Papagni, S.; Cozzolino, M. Which Vitamin D in CKD-MBD? The Time of Burning Questions. BioMed Res. Int. 2013, 2013, 864012. [Google Scholar] [CrossRef]
- Mozos, I.; Marginean, O. Links between Vitamin D Deficiency and Cardiovascular Diseases. BioMed Res. Int. 2015, 2015, 109275. [Google Scholar] [CrossRef]
- Pilz, S.; Gaksch, M.; O’Hartaigh, B.; Tomaschitz, A.; Marz, W. The role of vitamin D deficiency in cardiovascular disease: Where do we stand in 2013? Arch. Toxicol. 2013, 87, 2083–2103. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef]
- Lee, J.H.; O’Keefe, J.H.; Bell, D.; Hensrud, D.D.; Holick, M.F. Vitamin D deficiency an important, common, and easily treatable cardiovascular risk factor? J. Am. Coll. Cardiol. 2008, 52, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Weishaar, R.E.; Simpson, R.U. Vitamin D3 and cardiovascular function in rats. J. Clin. Investig. 1987, 79, 1706–1712. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Song, Y.; Manson, J.E.; Pilz, S.; Marz, W.; Michaelsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C.; et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: A meta-analysis of prospective studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-Hydroxyvitamin D and risk of myocardial infarction in men: A prospective study. Arch. Internal Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Michos, E.D.; Post, W.; Astor, B. 25-Hydroxyvitamin D Levels and the Risk of Mortality in the General Population. Arch. Int. Med. 2008, 168, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Messenger, W.; Nielson, C.M.; Li, H.; Beer, T.; Barrett-Connor, E.; Stone, K.; Shannon, J. Serum and dietary vitamin D and cardiovascular disease risk in elderly men: A prospective cohort study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 856–863. [Google Scholar] [CrossRef]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the Third National Health and Nutrition Examination Survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef]
- Chang, Q.; Hoefs, S.; van der Kemp, A.W.; Topala, C.N.; Bindels, R.J.; Hoenderop, J.G. The beta-glucuronidase klotho hydrolyzes and activates the TRPV5 channel. Science 2005, 310, 490–493. [Google Scholar] [CrossRef]
- Durup, D.; Jørgensen, H.L.; Christensen, J.; Schwarz, P.; Heegaard, A.-M.; Lind, B. A Reverse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study. J. Clin. Endocrinol. Metab. 2012, 97, 2644–2652. [Google Scholar] [CrossRef]
- Jeon, S.-M.; Shin, E.-A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Wen, X.; Liu, Y. Paricalcitol Inhibits Renal Inflammation by Promoting Vitamin D Receptor–Mediated Sequestration of NF-κB Signaling. J. Am. Soc. Nephrol. 2008, 19, 1741–1752. [Google Scholar] [CrossRef] [PubMed]
- Foltyn, V.N.; Bendikov, I.; De Miranda, J.; Panizzutti, R.; Dumin, E.; Shleper, M.; Li, P.; Toney, M.D.; Kartvelishvily, E.; Wolosker, H. Serine Racemase Modulates Intracellular D-Serine Levels through an α,β-Elimination Activity. J. Biol. Chem. 2005, 280, 1754–1763. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Law, C.S.; Grigsby, C.L.; Olsen, K.; Hong, T.-T.; Zhang, Y.; Yeghiazarians, Y.; Gardner, D.G. Cardiomyocyte-Specific Deletion of the Vitamin D Receptor Gene Results in Cardiac Hypertrophy. Circulation 2011, 124, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-H.; Fang, T.-C. The Pleiotropic Effect of Vitamin D. ISRN Nephrol. 2013, 2013, 898125. [Google Scholar] [CrossRef]
- Zittermann, A. Vitamin D in preventive medicine: Are we ignoring the evidence? Br. J. Nutr. 2003, 89, 552–572. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.-F.; Liu, S.Q.; Cao, L.-P. 1,25-Dihydroxyvitamin D3 is a negative endocrine regulator of the renin-angiotensin system. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Mohseni, H.; Hosseini, S.A.; Amani, R.; Ekrami, A.; Ahmadzadeh, A.; Latifi, S.M. Circulating 25-Hydroxy Vitamin D Relative to Vitamin D Receptor Polymorphism after Vitamin D3 Supplementation in Breast Cancer Women: A Randomized, Double-Blind Controlled Clinical Trial. Asian Pac. J. Cancer Prev. 2017, 18, 1953–1959. [Google Scholar] [CrossRef] [PubMed]
- Cantorna, M.T.; Mahon, B. Mounting Evidence for Vitamin D as an Environmental Factor Affecting Autoimmune Disease Prevalence. Exp. Biol. Med. 2004, 229, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Lavelli, V.; D’Incecco, P.; Pellegrino, L. Vitamin D Incorporation in Foods: Formulation Strategies, Stability, and Bioaccessibility as Affected by the Food Matrix. Foods 2021, 10, 1989. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Vitamin D Formulation | Dosage | Study Design | Patients | Study Length | Results |
|---|---|---|---|---|---|---|
| Kandula et al. [38] | Ergocalciferol or cholecalciferol | Observational study 4000 to 50,000 IU daily. RCTs rom 20,000 IU weekly to 25,000 IU monthly | Systematic review and meta-analysis | CKD: pre-dialysis, hemodialysis, peritoneal dialysis and KTRs | 1966 to September 2009 | No influence on Ca and P levels Reduction of PTH |
| Alvarez et al. [39] | Cholecalciferol | 50,000 IU/week for 12 weeks followed by 50,000 IU every other week for 40 weeks | Prospective | 46 early CKD (stages 2–3) | 1 year | Prevent vitamin D insufficiency Improvement of serum PTH |
| Cupisti et al. [40] | Cholecalciferol | 10,000 IU once-a-week | Cohort study | 405 CKD patients (stages 2–4) | 12 months | Reduction of PTH |
| Jean et al. [41] | Cholecalciferol and calcifediol | cholecalciferol 100,000 U/month calcifediol 10–50 μg/d | Prospective | All incident and prevalent hemodialysis patients in a single center | Three observation periods of 1-yr each | Reduction of the incidence of SHPT |
| Aytac et al. [42] | Cholecalciferol | single dose of 300,000 IU of oral cholecalciferol | Prospective | 41 CKD children and 24 healthy subjects free of any underlying cardiac or renal disease | 12 weeks | Increase in flow mediated dilatation, reduction in arterial stiffness Reduction of plasmatic Hcy and von Willebrand factor |
| Karakas et al. [43] | Cholecalciferol | 50,000 units weekly | Prospective | 44 hemodialysis patients and 24 healthy | 8 weeks | Increase in flow-mediated dilatation |
| Kim et al. [44] | Cholecalciferol | 40,000 units weekly for 8 weeks and then monthly | Prospective | 63 patients with diabetic nephropathy | 4 Months | Decrease in proteinuria in addition to ACE-i |
| Meireless et al. [45] | Cholecalciferol | 50,000 IU of cholecalciferol twice weekly | Prospective | 38 dialysis patients | 12 weeks | Upregulation of CYP27B1 and VDR expression in monocytes Lower serum IL-6 and CRP levels |
| Mann et al. [46] | Cholecalciferol, doxecalciferol, paracalcitol or alfacalcidol | 0.25 ug per day to 200,000 IU per week | Systematic review | Adults with CKD (≤60 mL/min/1.73 m2), including dialysis-dependent ESRD | 3–104 weeks | Lack of significant effects of vitamin D supplementation on mortality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zappulo, F.; Cappuccilli, M.; Cingolani, A.; Scrivo, A.; Chiocchini, A.L.C.; Nunzio, M.D.; Donadei, C.; Napoli, M.; Tondolo, F.; Cianciolo, G.; et al. Vitamin D and the Kidney: Two Players, One Console. Int. J. Mol. Sci. 2022, 23, 9135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169135
Zappulo F, Cappuccilli M, Cingolani A, Scrivo A, Chiocchini ALC, Nunzio MD, Donadei C, Napoli M, Tondolo F, Cianciolo G, et al. Vitamin D and the Kidney: Two Players, One Console. International Journal of Molecular Sciences. 2022; 23(16):9135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169135
Chicago/Turabian StyleZappulo, Fulvia, Maria Cappuccilli, Alessandra Cingolani, Anna Scrivo, Anna Laura Croci Chiocchini, Miriam Di Nunzio, Chiara Donadei, Marianna Napoli, Francesco Tondolo, Giuseppe Cianciolo, and et al. 2022. "Vitamin D and the Kidney: Two Players, One Console" International Journal of Molecular Sciences 23, no. 16: 9135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23169135