
Dissecting Immunotherapy Strategies for Small Cell Lung Cancer: Antibodies, Ionizing Radiation and CAR-T
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. “First Steps” of Immunotherapy in ES-SCLC
3. The Establishment of a New First-Line Standard
4. Combining Immunotherapy and Ionizing Radiation for SCLC
4.1. Limited Stage SCLC
4.2. Extended Stage SCLC
5. Chasing Predictive Biomarkers for SCLC Immunotherapy
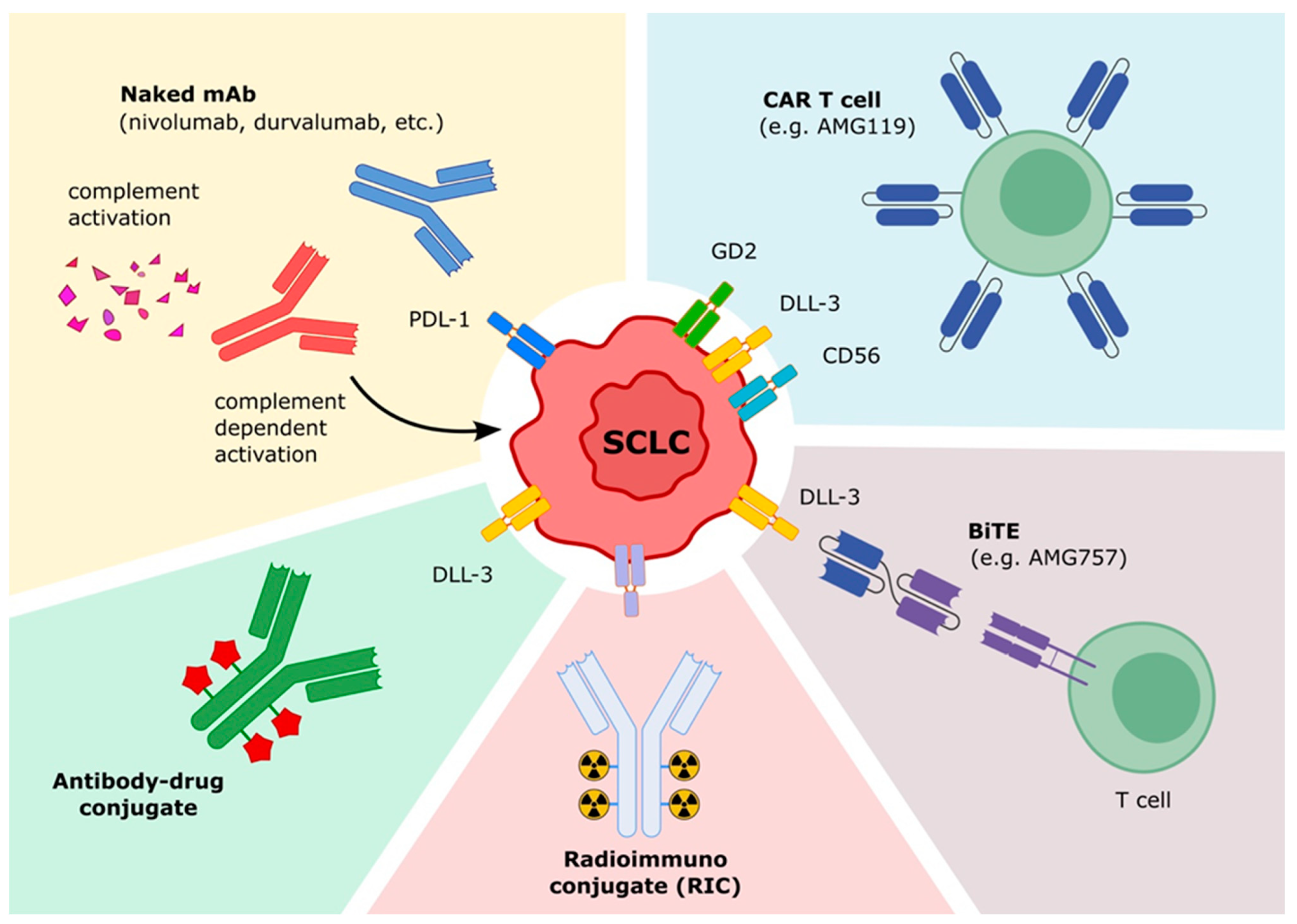
6. Future Immunotherapeutic Perspectives for SCLC
6.1. Antibody-Drug Conjugates (ADCs)
6.2. Radioimmunoconjugate
6.3. Bispecific T-Cell Engager (BiTEs®)
6.4. Bispecific Antibody
6.5. Chimeric Antigen Receptor (CAR) T Cells
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Devasia, T.; Mariotto, A.B.; Yabroff, K.R.; Jemal, A.; Kramer, J.; Siegel, R.L. Cancer treatment and survivorship statistics, 2022. CA A Cancer J. Clin. 2022, 72, 409–436. [Google Scholar] [CrossRef] [PubMed]
- Mascaux, C.; Paesmans, M.; Berghmans, T.; Branle, F.; Lafitte, J.; Lemaître, F.; Meert, A.; Vermylen, P.; Sculier, J. A systematic review of the role of etoposide and cisplatin in the chemotherapy of small cell lung cancer with methodology assessment and meta-analysis. Lung Cancer 2000, 30, 23–36. [Google Scholar] [CrossRef]
- Gozzard, P.; Woodhall, M.; Chapman, C.; Nibber, A.; Waters, P.; Vincent, A.; Lang, B.; Maddison, P. Paraneoplastic neurologic disorders in small cell lung carcinoma. Neurology 2015, 85, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Miret, M.; Horváth-Puhó, E.; Déruaz-Luyet, A.; Sørensen, H.T.; Ehrenstein, V. Potential paraneoplastic syndromes and selected autoimmune conditions in patients with non-small cell lung cancer and small cell lung cancer: A population-based cohort study. PLoS ONE 2017, 12, e0181564. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretić, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Peifer, M.; Fernandez-Cuesta, L.; Sos, M.L.; George, J.; Seidel, D.; Kasper, L.H.; Plenker, D.; Leenders, F.; Sun, R.; Zander, T.; et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 2012, 44, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.M.; Durinck, S.; Stawiski, E.W.; Poirier, J.; Modrusan, Z.; Shames, D.S.; Bergbower, E.; Guan, Y.; Shin, J.; Guillory, J.; et al. Comprehensive genomic analysis identifies SOX2 as a frequently amplified gene in small-cell lung cancer. Nat. Genet. 2012, 44, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L. Erratum: Signatures of mutational processes in human cancer (Nature (2013) 500 (415–421)). Nature 2013, 502, 258. [Google Scholar] [CrossRef] [Green Version]
- Dingemans, A.-M.; Früh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.; et al. Small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann. Oncol. 2021, 32, 839–853. [Google Scholar] [CrossRef]
- Ardizzoni, A.; Hansen, H.; Dombernowsky, P.; Gamucci, T.; Kaplan, S.; Postmus, P.; Giaccone, G.; Schaefer, B.; Wanders, J.; Verweij, J. Topotecan, a new active drug in the second-line treatment of small-cell lung cancer: A phase II study in patients with refractory and sensitive disease. The European Organization for Research and Treatment of Cancer Early Clinical Studies Group and New Drug Development Office, and the Lung Cancer Cooperative Group. J. Clin. Oncol. 1997, 15, 2090–2096. [Google Scholar] [CrossRef]
- Antonia, S.J.; López-Martin, J.A.; Bendell, J.; Ott, P.A.; Taylor, M.; Eder, J.P.; Jäger, D.; Pietanza, M.C.; Le, D.T.; de Braud, F.; et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): A multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016, 17, 883–895. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Luft, A.; Szczesna, A.; Havel, L.; Kim, S.-W.; Akerley, W.; Pietanza, M.C.; Wu, Y.-L.; Zielinski, C.; Thomas, M.; et al. Phase III Randomized Trial of Ipilimumab Plus Etoposide and Platinum Versus Placebo Plus Etoposide and Platinum in Extensive-Stage Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 3740–3748. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.V.; Reck, M.; Mansfield, A.S.; Mok, T.; Scherpereel, A.; Reinmuth, N.; Garassino, M.C.; Carpeno, J.D.C.; Califano, R.; Nishio, M. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J. Clin. Oncol. 2021, 39, 619. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H. Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.; Özgüroğlu, M.; Ji, J.; Garassino, M.; et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open 2022, 7, 100408. [Google Scholar] [CrossRef]
- Rudin, C.M.; Awad, M.M.; Navarro, A.; Gottfried, M.; Peters, S.; Csőszi, T.; Cheema, P.K.; Rodriguez-Abreu, D.; Wollner, M.; Yang, J.C.-H.; et al. Pembrolizumab or Placebo Plus Etoposide and Platinum as First-Line Therapy for Extensive-Stage Small-Cell Lung Cancer: Randomized, Double-Blind, Phase III KEYNOTE-604 Study. J. Clin. Oncol. 2020, 38, 2369–2379. [Google Scholar] [CrossRef]
- Wang, Z.; Zhao, J.; Ma, Z.; Cui, J.; Shu, Y.; Liu, Z.; Cheng, Y.; Leaw, S.J.; Wu, Y.; Ma, Y.; et al. A Phase 2 Study of Tislelizumab in Combination with Platinum-Based Chemotherapy as First-line Treatment for Advanced Lung Cancer in Chinese Patients. Lung Cancer 2020, 147, 259–268. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, C.; Yao, W.; Wang, Q.; Min, X.; Chen, G.; Xu, X.; Li, X.; Xu, F.; Fang, Y.; et al. Adebrelimab or placebo plus carboplatin and etoposide as first-line treatment for extensive-stage small-cell lung cancer (CAPSTONE-1): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 739–747. [Google Scholar] [CrossRef]
- Chung, H.C.; Piha-Paul, S.A.; Lopez-Martin, J.; Schellens, J.H.M.; Kao, S.; Miller, W.H., Jr.; Delord, J.-P.; Gao, B.; Planchard, D.; Gottfried, M.; et al. Pembrolizumab After Two or More Lines of Previous Therapy in Patients with Recurrent or Metastatic SCLC: Results From the KEYNOTE-028 and KEYNOTE-158 Studies. J. Thorac. Oncol. 2020, 15, 618–627. [Google Scholar] [CrossRef]
- Reck, M.; Vicente, D.; Ciuleanu, T.; Gettinger, S.; Peters, S.; Horn, L.; Audigier-Valette, C.; Pardo, N.; Juan-Vidal, O.; Cheng, Y.; et al. Efficacy and safety of nivolumab (nivo) monotherapy versus chemotherapy (chemo) in recurrent small cell lung cancer (SCLC): Results from CheckMate 331. Ann. Oncol. 2018, 29, x43. [Google Scholar] [CrossRef]
- Pujol, J.-L.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Uwer, L.; Hureaux, J.; Guisier, F.; Carmier, D.; Madelaine, J.; Otto, J.; et al. A Randomized Non-Comparative Phase II Study of Anti-Programmed Cell Death-Ligand 1 Atezolizumab or Chemotherapy as Second-Line Therapy in Patients with Small Cell Lung Cancer: Results From the IFCT-1603 Trial. J. Thorac. Oncol. 2019, 14, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Keam, B.; Ock, C.-Y.; Song, S.; Kim, M.; Kim, S.H.; Kim, K.H.; Kim, J.-S.; Kim, T.M.; Kim, D.-W.; et al. A phase II study of pembrolizumab and paclitaxel in patients with relapsed or refractory small-cell lung cancer. Lung Cancer 2019, 136, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.; Chiang, A.; Gilbert, J.; Gordon, M.; Conkling, P.; Thompson, D.; Marcoux, J.; Antonia, S.; Liu, B.; Shames, D.; et al. Clinical activity, safety and predictive biomarkers results from a phase Ia atezolizumab (atezo) trial in extensive-stage small cell lung cancer (ES-SCLC). Ann. Oncol. 2016, 27, vi493. [Google Scholar] [CrossRef] [Green Version]
- Goldman, J.W.; Dowlati, A.; Antonia, S.J.; Nemunaitis, J.J.; Butler, M.O.; Segal, N.H.; Smith, P.A.; Weiss, J.; Zandberg, D.P.; Xiao, F.; et al. Safety and antitumor activity of durvalumab monotherapy in patients with pretreated extensive disease small-cell lung cancer (ED-SCLC). J. Clin. Oncol. 2018, 36, 8518. [Google Scholar] [CrossRef]
- Cho, D.C.; Mahipal, A.; Dowlati, A.; Chow, W.A.; Segal, N.H.; Chung, K.Y.; Schneider, B.J.; Nemunaitis, J.J.; Razak, A.R.A.; Tsai, F.Y.-C.; et al. Safety and clinical activity of durvalumab in combination with tremelimumab in extensive disease small-cell lung cancer (ED-SCLC). J. Clin. Oncol. 2018, 36, 8517. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Park, K.; Govindan, R.; Ready, N.; Reck, M.; Peters, S.; Dakhil, S.R.; Navarro, A.; Rodríguez-Cid, J.; Schenker, M.; et al. Nivolumab and Ipilimumab as Maintenance Therapy in Extensive-Disease Small-Cell Lung Cancer: CheckMate 451. J. Clin. Oncol. 2021, 39, 1349–1359. [Google Scholar] [CrossRef]
- Gadgeel, S.M.; Pennell, N.A.; Fidler, M.J.; Halmos, B.; Bonomi, P.; Stevenson, J.; Schneider, B.; Sukari, A.; Ventimiglia, J.; Chen, W.; et al. Phase II Study of Maintenance Pembrolizumab in Patients with Extensive-Stage Small Cell Lung Cancer (SCLC). J. Thorac. Oncol. 2018, 13, 1393–1399. [Google Scholar] [CrossRef] [Green Version]
- Bondarenko, I.; Juan-Vidal, O.; Pajkos, G.; Kryzhanivska, A.; Székely, Z.P.; Vicente, D.; Vynnychenko, I.; Jones, S.; Wang, Y.; Jiang, H.; et al. Preliminary efficacy of durvalumab plus tremelimumab in platinum-refractory/resistant ED-SCLC from arm A of the phase II BALTIC study. Ann. Oncol. 2018, 29, viii596. [Google Scholar] [CrossRef]
- Fischer, R.N.; George, J.; Scheel, A.H.; Schloesser, H.A.; Vehreschild, M.; Brossart, P.; Engel-Riedel, W.; Griesinger, F.; Grohé, C.; Kambartel, K.-O.; et al. BIOLUMA: A phase II trial of nivolumab in combination with ipilimumab to evaluate efficacy and safety in lung cancer and to evaluate biomarkers predictive for response—Preliminary results from the NSCLC cohort. J. Clin. Oncol. 2019, 37, e20550. [Google Scholar] [CrossRef]
- ClinicalTrials. BIOLUMA: Biomarkers for Nivolumab and Ipilimumab and Evaluation of the Combination in Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03083691 (accessed on 15 August 2022).
- Reck, M.; Bondarenko, I.; Luft, A.; Serwatowski, P.; Barlesi, F.; Chacko, R.; Sebastian, M.; Lu, H.; Cuillerot, J.-M.; Lynch, T. Ipilimumab in combination with paclitaxel and carboplatin as first-line therapy in extensive-disease-small-cell lung cancer: Results from a randomized, double-blind, multicenter phase 2 trial. Ann. Oncol. 2013, 24, 75–83. [Google Scholar] [CrossRef]
- Goldman, J.W.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H. Durvalumab, with or without tremelimumab, plus platinum–etoposide versus platinum–etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): Updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 51–65. [Google Scholar] [CrossRef]
- Andrini, E.; Lamberti, G.; Mazzoni, F.; Riccardi, F.; Bonetti, A.; Follador, A.; Artioli, F.; Genova, C.; Barbieri, F.; Frassoldati, A.; et al. A phase II, open-label, single arm, trial of carboplatin plus etoposide with bevacizumab and atezolizumab in patients with extended-stage small-cell lung cancer (CeLEBrATE study): Background, design and rationale. Futur. Oncol. 2022, 18, 771–779. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials. Ipilimumab and Nivolumab in Recurrent Extensive Stage Small Cell Lung Cancer After Receiving Platinum-based Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT03670056 (accessed on 15 August 2022).
- ClinicalTrials. Combination Immunotherapy-Ipilimumab-Nivolumab-Dendritic Cell p53 Vac—Patients with Small Cell Lung Cancer (SCLC). Available online: https://clinicaltrials.gov/ct2/show/NCT03406715 (accessed on 15 August 2022).
- ClinicalTrials. Pembrolizumab vs Topotecan in Patients with Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02963090 (accessed on 15 August 2022).
- Morgensztern, D.; Rose, M.; Waqar, S.N.; Morris, J.; Ma, P.C.; Reid, T.; Brzezniak, C.; Zeman, K.G.; Padmanabhan, A.; Hirth, J.; et al. RRx-001 followed by platinum plus etoposide in patients with previously treated small-cell lung cancer. Br. J. Cancer 2019, 121, 211–217. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials. Chemoradiation With Durvalumab Followed by Durvalumab Maintenance for Limited Disease Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03585998 (accessed on 15 August 2022).
- ClinicalTrials. Atezolizumab After Concurrent Chemo-radiotherapy Versus Chemo-radiotherapy Alone in Limited Disease Small-cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT0540420 (accessed on 15 August 2022).
- ClinicalTrials. Chemoradiotherapy With or Without Sintilimab in Limited-stage SCLC. Available online: https://clinicaltrials.gov/ct2/show/NCT04189094 (accessed on 15 August 2022).
- ClinicalTrials. Testing the Addition of a New Immunotherapy Drug, Atezolizumab (MPDL3280A), to the Usual Chemoradiation (CRT) Therapy Treatment for Limited Stage Small Cell Lung Cancer (LS-SCLC). Available online: https://clinicaltrials.gov/ct2/show/NCT03811002 (accessed on 15 August 2022).
- Rimner, A.; Lai, W.-C.V.; Califano, R.; Jabbour, S.K.; Rudin, C.M.; Faivre-Finn, C.; Cho, B.C.; Kato, T.; Yu, J.; Chafin, W.; et al. Rationale and Design of the Phase 3 KEYLYNK-013 Study of Pembrolizumab with Concurrent Chemoradiotherapy Followed by Pembrolizumab With or Without Olaparib for Limited-Stage Small-Cell Lung Cancer. Clin. Lung Cancer 2022, 23, e325–e329. [Google Scholar] [CrossRef]
- ClinicalTrials. Study of Durvalumab + Tremelimumab, Durvalumab, and Placebo in Limited Stage Small-Cell Lung Cancer in Patients Who Have Not Progressed Following Concurrent Chemoradiation Therapy. Available online: https://clinicaltrials.gov/ct2/show/NCT03703297 (accessed on 15 August 2022).
- ClinicalTrials. Pembrolizumab and Concurrent Chemoradiotherapy or Radiation Therapy in Treating Patients with Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02402920. (accessed on 15 August 2022).
- ClinicalTrials. Immunotherapy in Combination with Chemoradiation in Patients With Advanced Solid Tumors. Available online: https://clinicaltrials.gov/ct2/show/NCT03509012 (accessed on 15 August 2022).
- Perez, B.A.; Kim, S.; Wang, M.; Karimi, A.M.; Powell, C.; Li, J.; Dilling, T.J.; Chiappori, A.; Latifi, K.; Rose, T.; et al. Prospective Single-Arm Phase 1 and 2 Study: Ipilimumab and Nivolumab with Thoracic Radiation Therapy After Platinum Chemotherapy in Extensive-Stage Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2020, 109, 425–435. [Google Scholar] [CrossRef]
- ClinicalTrials. Sequential Hypofractionated Radiotherapy Followed by Anti-PD-L1 Atezolizumab for SCLC. Available online: https://clinicaltrials.gov/ct2/show/NCT03262454. (accessed on 15 August 2022).
- ClinicalTrials. Radiotherapy and Durvalumab/Durvalumab Combo (Tremelimumab/Olaparid) for Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03923270 (accessed on 15 August 2022).
- ClinicalTrials. NCT04402788. Testing the Addition of Radiation Therapy to the Usual Immune Therapy Treatment (Atezolizumab) for Extensive Stage Small Cell Lung Cancer, RAPTOR Trial. Available online: https://clinicaltrials.gov/ct2/show/NCT04402788 (accessed on 15 August 2022).
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.-X. Irradiation and anti–PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Investig. 2014, 124, 687–695. [Google Scholar] [CrossRef]
- Blanquicett, C.; Saif, M.W.; Buchsbaum, D.J.; Eloubeidi, M.; Vickers, S.M.; Chhieng, D.C.; Carpenter, M.D.; Sellers, J.C.; Russo, S.; Diasio, R.B.; et al. Antitumor Efficacy of Capecitabine and Celecoxib in Irradiated and Lead-Shielded, Contralateral Human BxPC-3 Pancreatic Cancer Xenografts: Clinical Implications of Abscopal Effects. Clin. Cancer Res. 2005, 11, 8773–8781. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Barsoumian, H.B.; Yang, L.; Younes, A.I.; Verma, V.; Hu, Y.; Menon, H.; Wasley, M.; Masropour, F.; Mosaffa, S.; et al. SHP-2 and PD-L1 Inhibition Combined with Radiotherapy Enhances Systemic Antitumor Effects in an Anti–PD-1–Resistant Model of Non–Small Cell Lung Cancer. Cancer Immunol. Res. 2020, 8, 883–894. [Google Scholar] [CrossRef] [Green Version]
- Ostrand-Rosenberg, S.; Horn, L.A.; Ciavattone, N.G. Radiotherapy Both Promotes and Inhibits Myeloid-Derived Suppressor Cell Function: Novel Strategies for Preventing the Tumor-Protective Effects of Radiotherapy. Front. Oncol. 2019, 9, 215. [Google Scholar] [CrossRef]
- Rodríguez-Ruiz, M.E.; Vanpouille-Box, C.; Melero, I.; Formenti, S.C.; Demaria, S. Immunological Mechanisms Responsible for Radiation-Induced Abscopal Effect. Trends Immunol. 2018, 39, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Iori, F.; Bruni, A.; Cozzi, S.; Ciammella, P.; Di Pressa, F.; Boldrini, L.; Greco, C.; Nardone, V.; Salvestrini, V.; Desideri, I.; et al. Can Radiotherapy Empower the Host Immune System to Counterattack Neoplastic Cells? A Systematic Review on Tumor Microenvironment Radiomodulation. Curr. Oncol. 2022, 29, 4612–4624. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Apetoh, L.; Ghiringhelli, F.; André, F.; Tesniere, A.; Kroemer, G. The anticancer immune response: Indispensable for therapeutic success? J. Clin. Investig. 2008, 118, 1991–2001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, A.; Schoenfeld, J.D. Immunotherapy and radiotherapy for metastatic cancers. Ann. Palliat. Med. 2019, 8, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Karam, I.; Jiang, S.Y.; Khaira, M.; Lee, C.W.; Schellenberg, D. Outcomes of Small Cell Lung Cancer Patients Treated with Cisplatin-Etoposide Versus Carboplatin-Etoposide. Am. J. Clin. Oncol. 2015, 38, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Turrisi, A.T.; Kim, K.; Blum, R.; Sause, W.T.; Livingston, R.B.; Komaki, R.; Wagner, H.; Aisner, S.; Johnson, D.H. Twice-Daily Compared with Once-Daily Thoracic Radiotherapy in Limited Small-Cell Lung Cancer Treated Concurrently with Cisplatin and Etoposide. N. Engl. J. Med. 1999, 340, 265–271. [Google Scholar] [CrossRef]
- Slotman, B. What is the optimal radiotherapy schedule for limited stage small cell lung cancer? Lung Cancer 2017, 105, 52–53. [Google Scholar] [CrossRef] [Green Version]
- Faivre-Finn, C.; Snee, M.; Ashcroft, L.; Appel, W.; Barlesi, F.; Bhatnagar, A.; Bezjak, A.; Cardenal, F.; Fournel, P.; Harden, S.; et al. Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): An open-label, phase 3, randomised, superiority trial. Lancet Oncol. 2017, 18, 1116–1125. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials. Radiation Therapy Regimens in Treating Patients with Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide. Available online: https://clinicaltrials.gov/ct2/show/NCT00632853 (accessed on 15 August 2022).
- ClinicalTrials. Two Schedules of Hyperfractionated Thoracic Radiotherapy in Limited Disease Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02041845 (accessed on 15 August 2022).
- Levy, A.; Hendriks, L.E.; Le Péchoux, C.; Falk, S.; Besse, B.; Novello, S.; Dingemans, A.-M.C.; Hasan, B.; Reck, M.; Berghmans, T.; et al. Current management of limited-stage SCLC and CONVERT trial impact: Results of the EORTC Lung Cancer Group survey. Lung Cancer 2019, 136, 145–147. [Google Scholar] [CrossRef]
- Mamesaya, N.; Wakuda, K.; Omae, K.; Miyawaki, E.; Kotake, M.; Fujiwara, T.; Kawamura, T.; Kobayashi, H.; Nakashima, K.; Omori, S.; et al. Efficacy of prophylactic cranial irradiation in patients with limited-disease small-cell lung cancer who were confirmed to have no brain metastasis via magnetic resonance imaging after initial chemoradiotherapy. Oncotarget 2018, 9, 17664–17674. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senan, S.; Okamoto, I.; Lee, G.-W.; Chen, Y.; Niho, S.; Mak, G.; Yao, W.; Shire, N.; Jiang, H.; Cho, B.C. Design and Rationale for a Phase III, Randomized, Placebo-controlled Trial of Durvalumab with or Without Tremelimumab After Concurrent Chemoradiotherapy for Patients With Limited-stage Small-cell Lung Cancer: The ADRIATIC Study. Clin. Lung Cancer 2020, 21, e84–e88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.; Pujol, J.-L.; Dafni, U.; Dómine, M.; Popat, S.; Reck, M.; Andrade, J.; Becker, A.; Moro-Sibilot, D.; Curioni-Fontecedro, A.; et al. Consolidation nivolumab and ipilimumab versus observation in limited-disease small-cell lung cancer after chemo-radiotherapy—Results from the randomised phase II ETOP/IFCT 4-12 STIMULI trial. Ann. Oncol. 2021, 33, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, J.L.; McCoy, F.; Scullin, P.; Fennell, D.A. New Advances in the Second-Line Treatment of Small Cell Lung Cancer. Oncol. 2009, 14, 986–994. [Google Scholar] [CrossRef]
- Slotman, B.J.; van Tinteren, H.; Praag, J.O.; Knegjens, J.L.; El Sharouni, S.Y.; Hatton, M.; Keijser, A.; Faivre-Finn, C.; Senan, S. Use of thoracic radiotherapy for extensive stage small-cell lung cancer: A phase 3 randomised controlled trial. Lancet 2015, 385, 36–42. [Google Scholar] [CrossRef]
- Gore, E.M.; Hu, C.; Sun, A.Y.; Grimm, D.F.; Ramalingam, S.S.; Dunlap, N.E.; Higgins, K.A.; Werner-Wasik, M.; Allen, A.M.; Iyengar, P.; et al. Randomized Phase II Study Comparing Prophylactic Cranial Irradiation Alone to Prophylactic Cranial Irradiation and Consolidative Extracranial Irradiation for Extensive-Disease Small Cell Lung Cancer (ED SCLC): NRG Oncology RTOG 0937. J. Thorac. Oncol. 2017, 12, 1561–1570. [Google Scholar] [CrossRef] [Green Version]
- Jeremic, B.; Shibamoto, Y.; Nikolic, N.; Milicic, B.; Milisavljevic, S.; Dagovic, A.; Aleksandrovic, J.; Radosavljevic-Asic, G. Role of Radiation Therapy in the Combined-Modality Treatment of Patients with Extensive Disease Small-Cell Lung Cancer: A Randomized Study. J. Clin. Oncol. 1999, 17, 2092. [Google Scholar] [CrossRef]
- Seto, T.; Shukuya, T.; Yamanaka, T. Chemotherapy developments for lung cancer. J. Thorac. Oncol. 2015, 10, S173–S260. [Google Scholar]
- Slotman, B.J.; van Tinteren, H. Which patients with extensive stage small-cell lung cancer should and should not receive thoracic radiotherapy? Transl. Lung Cancer Res. 2015, 4, 292. [Google Scholar]
- Welsh, J.W.; Heymach, J.V.; Chen, D.; Verma, V.; Cushman, T.R.; Hess, K.R.; Shroff, G.; Tang, C.; Skoulidis, F.; Jeter, M.; et al. Phase I Trial of Pembrolizumab and Radiation Therapy after Induction Chemotherapy for Extensive-Stage Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 15, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Pakkala, S.; Higgins, K.; Chen, Z.; Sica, G.; Steuer, C.; Zhang, C.; Zhang, G.; Wang, S.; Hossain, M.S.; Nazha, B.; et al. Durvalumab and tremelimumab with or without stereotactic body radiation therapy in relapsed small cell lung cancer: A randomized phase II study. J. Immunother. Cancer 2020, 8, e001302. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials. Ipilimumab + Nivolumab w/Thoracic Radiotherapy for Extensive-Stage Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03043599 (accessed on 15 August 2022).
- Sen, T.; Rodriguez, B.L.; Chen, L.; Della Corte, C.M.; Morikawa, N.; Fujimoto, J.; Cristea, S.; Nguyen, T.; Diao, L.; Li, L.; et al. Targeting DNA Damage Response Promotes Antitumor Immunity through STING-Mediated T-cell Activation in Small Cell Lung Cancer. Cancer Discov. 2019, 9, 646–661. [Google Scholar] [CrossRef] [PubMed]
- Laird, J.H.; Lok, B.H.; Ma, J.; Bell, A.; de Stanchina, E.; Poirier, J.T.; Rudin, C.M. Talazoparib Is a Potent Radiosensitizer in Small Cell Lung Cancer Cell Lines and Xenografts. Clin. Cancer Res. 2018, 24, 5143–5152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, M.; Saito, K.; Shiraishi, K.; Maeda, D.; Suzuki, H.; Minamiya, Y.; Kono, K.; Kohno, T.; Goto, A. Identification of candidate responders for anti-PD-L1/PD-1 immunotherapy, Rova-T therapy, or EZH2 inhibitory therapy in small-cell lung cancer. Mol. Clin. Oncol. 2018, 8, 310–314. [Google Scholar] [CrossRef] [Green Version]
- Hellmann, M.D.; Callahan, M.K.; Awad, M.M.; Calvo, E.; Ascierto, P.A.; Atmaca, A.; Rizvi, N.A.; Hirsch, F.R.; Selvaggi, G.; Szustakowski, J.D.; et al. Tumor Mutational Burden and Efficacy of Nivolumab Monotherapy and in Combination with Ipilimumab in Small-Cell Lung Cancer. Cancer Cell 2018, 33, 853–861.e4. [Google Scholar] [CrossRef] [Green Version]
- Ricciuti, B.; Kravets, S.; Dahlberg, S.E.; Umeton, R.; Albayrak, A.; Subegdjo, S.J.; Johnson, B.E.; Nishino, M.; Sholl, L.M.; Awad, M.M. Use of targeted next generation sequencing to characterize tumor mutational burden and efficacy of immune checkpoint inhibition in small cell lung cancer. J. Immunother. Cancer 2019, 7, 87. [Google Scholar] [CrossRef]
- Sacdalan, D.B.; Lucero, J.A.; Sacdalan, D.L. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: A review and meta-analysis. Onco Targets Ther. 2018, 11, 955. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, Y.; Chen, P.; Xu, W.; Wu, Y.; Che, G. Prognostic value of the pretreatment systemic immune-inflammation index (SII) in patients with non-small cell lung cancer: A meta-analysis. Ann. Transl. Med. 2019, 7, 433. [Google Scholar] [CrossRef]
- Xiong, Q.; Huang, Z.; Xin, L.; Qin, B.; Zhao, X.; Zhang, J.; Shi, W.; Yang, B.; Zhang, G.; Hu, Y. Post-treatment neutrophil-to-lymphocyte ratio (NLR) predicts response to anti-PD-1/PD-L1 antibody in SCLC patients at early phase. Cancer Immunol. Immunother. 2021, 70, 713–720. [Google Scholar] [CrossRef]
- Hardy-Werbin, M.; Rocha, P.; Arpi, O.; Taus, Á.; Nonell, L.; Durán, X.; Villanueva, X.; Joseph-Pietras, D.; Nolan, L.; Danson, S.; et al. Serum cytokine levels as predictive biomarkers of benefit from ipilimumab in small cell lung cancer. OncoImmunology 2019, 8, e1593810. [Google Scholar] [CrossRef] [Green Version]
- Herbreteau, G.; Langlais, A.; Greillier, L.; Audigier-Valette, C.; Uwer, L.; Hureaux, J.; Moro-Sibilot, D.; Guisier, F.; Carmier, D.; Madelaine, J.; et al. Circulating Tumor DNA as a Prognostic Determinant in Small Cell Lung Cancer Patients Receiving Atezolizumab. J. Clin. Med. 2020, 9, 3861. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Hodkinson, P.; McLaren, F.; MacKinnon, A.; Wallace, W.; Howie, S.; Sethi, T. Small cell lung cancer tumour cells induce regulatory T lymphocytes, and patient survival correlates negatively with FOXP3+ cells in tumour infiltrate. Int. J. Cancer 2012, 131, E928–E937. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Hodkinson, P.; McLaren, F.; Mackean, M.J.; Williams, L.; Howie, S.; Wallace, W.A.; Sethi, T. Histologic Assessment of Tumor-Associated CD45+ Cell Numbers Is an Independent Predictor of Prognosis in Small Cell Lung Cancer. Chest 2013, 143, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, L.; Pavan, A.; Dieci, M.; Di Liso, E.; Schiavon, M.; Comacchio, G.M.; Attili, I.; Pasello, G.; Calabrese, F.; Rea, F.; et al. The role of immune microenvironment in small-cell lung cancer: Distribution of PD-L1 expression and prognostic role of FOXP3-positive tumour infiltrating lymphocytes. Eur. J. Cancer 2018, 101, 191–200. [Google Scholar] [CrossRef]
- Muppa, P.; Terra, S.B.S.P.; Sharma, A.; Mansfield, A.S.; Aubry, M.-C.; Bhinge, K.; Asiedu, M.K.; de Andrade, M.; Janaki, N.; Murphy, S.J.; et al. Immune Cell Infiltration May Be a Key Determinant of Long-Term Survival in Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 14, 1286–1295. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Sun, Y.; Sun, T.; Tang, R. Comprehensive Bioinformatics Analysis Identifies Tumor Microenvironment and Immune-related Genes in Small Cell Lung Cancer. Comb. Chem. High Throughput Screen. 2020, 23, 381–391. [Google Scholar] [CrossRef]
- Zhao, X.W.; van Beek, E.M.; Schornagel, K.; Van der Maaden, H.; Van Houdt, M.; Otten, M.A.; Finetti, P.; Van Egmond, M.; Matozaki, T.; Kraal, G. CD47–signal regulatory protein-α (SIRPα) interactions form a barrier for antibody-mediated tumor cell destruction. Proc. Natl. Acad. Sci. USA 2011, 108, 18342–18347. [Google Scholar] [CrossRef] [Green Version]
- Tseng, D.; Volkmer, J.-P.; Willingham, S.B.; Contreras-Trujillo, H.; Fathman, J.W.; Fernhoff, N.B.; Seita, J.; Inlay, M.A.; Weiskopf, K.; Miyanishi, M.; et al. Anti-CD47 antibody–mediated phagocytosis of cancer by macrophages primes an effective antitumor T-cell response. Proc. Natl. Acad. Sci. USA 2013, 110, 11103–11108. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Pu, Y.; Cron, K.R.; Deng, L.; Kline, J.; Frazier, W.A.; Xu, H.; Peng, H.; Fu, Y.-X.; Xu, M.M. CD47 blockade triggers T cell–mediated destruction of immunogenic tumors. Nat. Med. 2015, 21, 1209–1215. [Google Scholar] [CrossRef] [Green Version]
- Weiskopf, K.; Jahchan, N.S.; Schnorr, P.; Cristea, S.; Ring, A.; Maute, R.L.; Volkmer, A.K.; Volkmer, J.-P.; Liu, J.; Lim, J.S.; et al. CD47-blocking immunotherapies stimulate macrophage-mediated destruction of small-cell lung cancer. J. Clin. Investig. 2016, 126, 2610–2620. [Google Scholar] [CrossRef]
- Horta, Z.P.; Goldberg, J.L.; Sondel, P.M. Anti-GD2 mAbs and next-generation mAb-based agents for cancer therapy. Immunotherapy 2016, 8, 1097–1117. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.; Goetsch, L.; Dumontet, C.; Corvaïa, N. Strategies and challenges for the next generation of antibody–drug conjugates. Nat. Rev. Drug Discov. 2017, 16, 315–337. [Google Scholar] [CrossRef]
- Drago, J.Z.; Modi, S.; Chandarlapaty, S. Unlocking the potential of antibody–drug conjugates for cancer therapy. Nat. Rev. Clin. Oncol. 2021, 18, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Saunders, L.R.; Bankovich, A.J.; Anderson, W.C.; Aujay, M.A.; Bheddah, S.; Black, K.; Desai, R.; Escarpe, P.A.; Hampl, J.; Laysang, A.; et al. A DLL3-targeted antibody-drug conjugate eradicates high-grade pulmonary neuroendocrine tumor-initiating cells in vivo. Sci. Transl. Med. 2015, 7, 302ra136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, D.H.; Giffin, M.J.; Bailis, J.M.; Smit, M.-A.D.; Carbone, D.P.; He, K. DLL3: An emerging target in small cell lung cancer. J. Hematol. Oncol. 2019, 12, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudin, C.M.; Pietanza, M.C.; Bauer, T.M.; Ready, N.; Morgensztern, D.; Glisson, B.S.; Byers, L.A.; Johnson, M.L.; Burris, H.A., III; Robert, F. Rovalpituzumab tesirine, a DLL3-targeted antibody-drug conjugate, in recurrent small-cell lung cancer: A first-in-human, first-in-class, open-label, phase 1 study. Lancet Oncol. 2017, 18, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Blackhall, F.; Jao, K.; Greillier, L.; Cho, B.C.; Penkov, K.; Reguart, N.; Majem, M.; Nackaerts, K.; Syrigos, K.; Hansen, K.; et al. Efficacy and Safety of Rovalpituzumab Tesirine Compared with Topotecan as Second-Line Therapy in DLL3-High SCLC: Results From the Phase 3 TAHOE Study. J. Thorac. Oncol. 2021, 16, 1547–1558. [Google Scholar] [CrossRef]
- Hann, C.L.; Burns, T.F.; Dowlati, A.; Morgensztern, D.; Ward, P.J.; Koch, M.M.; Chen, C.; Ludwig, C.; Patel, M.; Nimeiri, H.; et al. A Phase 1 Study Evaluating Rovalpituzumab Tesirine in Frontline Treatment of Patients with Extensive-Stage SCLC. J. Thorac. Oncol. 2021, 16, 1582–1588. [Google Scholar] [CrossRef]
- Johnson, M.L.; Zvirbule, Z.; Laktionov, K.; Helland, A.; Cho, B.C.; Gutierrez, V.; Colinet, B.; Lena, H.; Wolf, M.; Gottfried, M.; et al. Rovalpituzumab Tesirine as a Maintenance Therapy After First-Line Platinum-Based Chemotherapy in Patients with Extensive-Stage–SCLC: Results from the Phase 3 MERU Study. J. Thorac. Oncol. 2021, 16, 1570–1581. [Google Scholar] [CrossRef]
- Malhotra, J.; Nikolinakos, P.; Leal, T.; Lehman, J.; Morgensztern, D.; Patel, J.D.; Wrangle, J.M.; Curigliano, G.; Greillier, L.; Johnson, M.L.; et al. A Phase 1–2 Study of Rovalpituzumab Tesirine in Combination with Nivolumab Plus or Minus Ipilimumab in Patients With Previously Treated Extensive-Stage SCLC. J. Thorac. Oncol. 2021, 16, 1559–1569. [Google Scholar] [CrossRef]
- Calvo, E.; Spira, A.; de Miguel, M.; Kondo, S.; Gazzah, A.; Millward, M.; Prenen, H.; Rottey, S.; Warburton, L.; Alanko, T.; et al. Safety, pharmacokinetics, and efficacy of budigalimab with rovalpituzumab tesirine in patients with small cell lung cancer. Cancer Treat. Res. Commun. 2021, 28, 100405. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Cassier, P.A.; Lin, C.-C.; Alanko, T.; Peltola, K.J.; Gazzah, A.; Shiah, H.-S.; Calvo, E.; Cervantes, A.; Roda, D.; et al. First-in-human phase 1 study of budigalimab, an anti-PD-1 inhibitor, in patients with non-small cell lung cancer and head and neck squamous cell carcinoma. Cancer Immunol. Immunother. 2021, 71, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Smaglo, B.G.; Aldeghaither, D.; Weiner, L.M. The development of immunoconjugates for targeted cancer therapy. Nat. Rev. Clin. Oncol. 2014, 11, 637–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parakh, S.; Lee, S.T.; Gan, H.K.; Scott, A.M. Radiolabeled Antibodies for Cancer Imaging and Therapy. Cancers 2022, 14, 1454. [Google Scholar] [CrossRef] [PubMed]
- Giffin, M.J.; Lobenhofer, E.K.; Cooke, K.; Raum, T.; Stevens, J.; Beltran, P.J.; Coxon, A.; Hughes, P.E. Abstract 3632: BiTE® antibody constructs for the treatment of SCLC. Cancer Res. 2017, 77, 3632. [Google Scholar] [CrossRef]
- Klinger, M.; Benjamin, J.; Kischel, R.; Stienen, S.; Zugmaier, G. Harnessing T cells to fight cancer with BiTE® antibody constructs–past developments and future directions. Immunol. Rev. 2016, 270, 193–208. [Google Scholar] [CrossRef]
- Choi, B.D.; Cai, M.; Bigner, D.D.; Mehta, A.I.; Kuan, C.-T.; Sampson, J.H. Bispecific antibodies engage T cells for antitumor immunotherapy. Expert Opin. Biol. Ther. 2011, 11, 843–853. [Google Scholar] [CrossRef]
- Zhou, S.; Liu, M.; Ren, F.; Meng, X.; Yu, J. The landscape of bispecific T cell engager in cancer treatment. Biomark. Res. 2021, 9, 38. [Google Scholar] [CrossRef]
- ClinicalTrials. Study Evaluating Safety, Tolerability and PK of AMG 757 in Adults with Small Cell Lung Cancer. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03319940 (accessed on 15 August 2022).
- Cooke, K.; Estrada, J.; Zhan, J.; Werner, J.; Lee, F.; Shetty, A.; Smit, M.-A.D.; Salvati, M.; Bailis, J. 627 The DLL3-targeted half-life extended bispecific T cell engager (HLE BiTE®) immune-oncology therapy AMG 757 has potent antitumor activity in neuroendocrine cancer. J. Immunother. Cancer 2020, 8, A663. [Google Scholar] [CrossRef]
- ClinicalTrials. Safety and Clinical Activity of Nivatrotamab in Relapsed/Recurrent Metastatic Small-cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT04750239 (accessed on 15 August 2022).
- Nazha, B.; Inal, C.; Owonikoko, T.K. Disialoganglioside GD2 Expression in Solid Tumors and Role as a Target for Cancer Therapy. Front. Oncol. 2020, 10, 1000. [Google Scholar] [CrossRef]
- Yoshida, S.; Fukumoto, S.; Kawaguchi, H.; Sato, S.; Ueda, R.; Furukawa, K. Ganglioside G(D2) in small cell lung cancer cell lines: Enhancement of cell proliferation and mediation of apoptosis. Cancer Res. 2001, 61, 4244–4252. [Google Scholar] [PubMed]
- Chen, L.-C.; Brown, A.B.; Cheung, I.Y.; Cheung, N.-K.V.; Kris, M.G.; Krug, L.M. Analysis of GD2/GM2 synthase mRNA as a biomarker for small cell lung cancer. Lung Cancer 2010, 67, 216–220. [Google Scholar] [CrossRef] [PubMed]
- D’Aloia, M.M.; Zizzari, I.G.; Sacchetti, B.; Pierelli, L.; Alimandi, M. CAR-T cells: The long and winding road to solid tumors. Cell Death Dis. 2018, 9, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, D.L.; Levine, B.L.; Kalos, M.; Bagg, A.; June, C.H. Chimeric Antigen Receptor–Modified T Cells in Chronic Lymphoid Leukemia. N. Engl. J. Med. 2011, 365, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Maude, S.L.; Frey, N.; Shaw, P.A.; Aplenc, R.; Barrett, D.M.; Bunin, N.J.; Chew, A.; Gonzalez, V.E.; Zheng, Z.; Lacey, S.F.; et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 2014, 371, 1507–1517. [Google Scholar] [CrossRef] [Green Version]
- Sacchetti, B.; Botticelli, A.; Pierelli, L.; Nuti, M.; Alimandi, M. CAR-T with License to Kill Solid Tumors in Search of a Winning Strategy. Int. J. Mol. Sci. 2019, 20, 1903. [Google Scholar] [CrossRef] [Green Version]
- Crossland, D.L.; Denning, W.; Ang, S.; Olivares, S.; Mi, T.; Switzer, K.; Singh, H.; Huls, H.; Gold, K.S.; Glisson, B.S.; et al. Antitumor activity of CD56-chimeric antigen receptor T cells in neuroblastoma and SCLC models. Oncogene 2018, 37, 3686–3697. [Google Scholar] [CrossRef]
- Rudin, C.M.; Brambilla, E.; Faivre-Finn, C.; Sage, J. Small-cell lung cancer. Nat. Rev. Dis. Primers 2021, 7, 3. [Google Scholar] [CrossRef]
- Yu, J.; Wu, X.; Yan, J.; Yu, H.; Xu, L.; Chi, Z.; Sheng, X.; Si, L.; Cui, C.; Dai, J. Anti-GD2/4-1BB chimeric antigen receptor T cell therapy for the treatment of Chinese melanoma patients. J. Hematol. Oncol. 2018, 11, 1. [Google Scholar] [CrossRef]
- Charan, M.; Dravid, P.; Cam, M.; Audino, A.; Gross, A.C.; Arnold, M.A.; Roberts, R.D.; Cripe, T.P.; Pertsemlidis, A.; Houghton, P.J.; et al. GD2-directed CAR-T cells in combination with HGF-targeted neutralizing antibody (AMG102) prevent primary tumor growth and metastasis in Ewing sarcoma. Int. J. Cancer 2019, 146, 3184–3195. [Google Scholar] [CrossRef]
- Straathof, K.; Flutter, B.; Wallace, R.; Jain, N.; Loka, T.; Depani, S.; Wright, G.; Thomas, S.; Cheung, G.W.-K.; Gileadi, T.; et al. Antitumor activity without on-target off-tumor toxicity of GD2–chimeric antigen receptor T cells in patients with neuroblastoma. Sci. Transl. Med. 2020, 12, eabd6169. [Google Scholar] [CrossRef] [PubMed]
- Prapa, M.; Chiavelli, C.; Golinelli, G.; Grisendi, G.; Bestagno, M.; Di Tinco, R.; Dall’Ora, M.; Neri, G.; Candini, O.; Spano, C.; et al. GD2 CAR T cells against human glioblastoma. Npj Precis. Oncol. 2021, 5, 93. [Google Scholar] [CrossRef] [PubMed]
- Majzner, R.G.; Ramakrishna, S.; Yeom, K.W.; Patel, S.; Chinnasamy, H.; Schultz, L.M.; Richards, R.M.; Jiang, L.; Barsan, V.; Mancusi, R.; et al. GD2-CAR T cell therapy for H3K27M-mutated diffuse midline gliomas. Nature 2022, 603, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Reppel, L.; Tsahouridis, O.; Akulian, J.; Davis, I.J.; Lee, H.; Fucà, G.; Weiss, J.; Dotti, G.; Pecot, C.V.; Savoldo, B. Targeting disialoganglioside GD2 with chimeric antigen receptor-redirected T cells in lung cancer. J. Immunother. Cancer 2022, 10, e003897. [Google Scholar] [CrossRef]


{kind=link}
| Setting | Trial | Phase | No. of Patients | Treatment Arms | End Points | ORR | mPFS Months (95% CI) | mOS Months (95% CI) |
|---|---|---|---|---|---|---|---|---|
| 1st line | Reck M et al. JCO 2016 [12] | 3 | 1132 | EP + ipilimumab EP + placebo | OS (primary) PFS (secondary) | 62% ipilimumab 62% placebo | 4.6 (4.50–4.99) ipilimumab 4.4 (4.73–4.63) placebo HR 0.85 (95% CI 0.75–0.97); p = 0.0161 | 11.0 (10.45–11.33) ipilimumab 10.9 (10.02–11.50) placebo HR 0.94 (95% CI 0.81–1.09); p = 0.3775 |
| Impower133 Horn et al. NEJM 2018 [13] Liu et al. JCO 2020 [14] | 3 | 403 | EP + atezolizumab EP + placebo | OS, PFS (primary) ORR, DoR (secondary) | 60.2% atezolizumab 64.4% placebo | 5.2 (4.4–5.6) atezolizumab 4.3 (4.2–4.5) placebo HR 0.77 (95% CI 0.62–0.96); p = 0.02 | 12.3 atezolizumab 10.3 placebo HR 0.76 (95% CI 0.60–0.95); p = 0.0154 * | |
| Caspian Paz-Ares et al. Lancet 2019 [15] Pas-Arez et al. Ann Oncol 2022 [16] | 3 | 805 | EP + durvalumab EP + duvalumab + tremelimumab EP alone | OS (primary) PFS, ORR, Safety (secondary) | 68% durvalumab 58% EP alone | 5.1 (4.7–6.2) durvalumab 5.4 (4.8–6.2) EP alone HR 0.78 (95% CI 0.65–0.94) | 12.9 (11.3–14.7) durvalumab 10.5 (9.3–11.2) EP alone HR 0.71 (95% CI 0.60–0.86); p = 0.0003 * | |
| Keynote-604 Rudin CM et al. JCO 2020 [17] | 3 | 453 | EP + pembrolizumab EP + placebo | OS, PFS (primary) ORR, DoR, Safety (secondary) | 70.6%pembrolizumab 61.8% placebo | 4.5 (4,3–5,4) pembrolizumab 4.3 (4.2–4.4) placebo HR 0.75 (95% CI 0.61–0.91); p = 0.0023 | 10.8 (9.2–12.9) pembrolizumab 9.7 (8.6–10.7) placebo HR 0.80 (95% CI 0.64–0.98); p = 0.0164 | |
| Wang et al. Lung Cancer 2020 [18] | 2 | 17 | EP + tislelizumab | ORR (primary) DCR, DoR, PFS, Safety (secondary) | 77% | 6.9 (4.9–10.09) | 15.6 (11.79-NE) | |
| Capstone-1 Wang et al. Lancet Oncol 2022 [19] | 3 | 462 | CBDCA + eto + adebrelimab CDBCA + eto + placebo | OS (primary) PFS, ORR, DoR, DCR, 6 and 12 months-PFS, 12 and 24 moths-OS, Safety (Secondary) | 70.4% adebrelimab 65.9% placebo | 5.8 (5.6–6.96) adebrelimab 5.6 (5.5–5.7) placebo HR 0.67 (95% CI 0.54–0.83); p < 0.0001 | 15.3 (13.2–17.5) adebrelimab 12.8 (11.3–13.7) placebo HR 0.72 (95% CI 0.58–0.90); p = 0.0017 | |
| 2nd line and beyond | CheckMate-032 Antonia et al. Lancet Oncol 2016 [11] | 1/2 | 216 | nivo 3 mg/kg nivo 1 mg/kg + ipi 1 mg/kg nivo 1 mg/kg + ipi 3 mg/kg nivo 3 mg/kg + ipi1 mg/kg | ORR (primary) OS, PFS, DoR, Safety (secondary) | 10% nivo 3 mg/kg 33% nivo 1 mg/kg + ipi 1 mg/kg 23% nivo 1 mg/kg + ipi 3 mg/kg 19% nivo 3 mg/kg + ipi 1 mg/kg | 1.4 (1.4–1.9) nivo 3 mg/kg 2.6 (1.4–4.1) nivo 1 mg/kg + ipi 3 mg/kg 1.4 (1.3–2.2) nivo 3 mg/kg + ipi 1 mg/kg | 4.4 (3.0–9.3) nivo 3 mg/kg 7.7 (3.6–18.0) nivo 1 mg/kg + ipi 3 mg/kg 6.0 (95% CI 3.6–11.0) nivo 3 mg/kg + ipi 1 mg/kg |
| Keynote-028/Keynote-158 Pooled analysis Chung et al. JCO 2020 [20] | 1b and 2 | 83 | pembrolizumab | ORR (primary) OS, PFS, DoR (secondary) | 19.3% | 2.0 (1.9–3.4) | 7.7 (5.2–10.1) | |
| CheckMate 331 Reck M et al. Ann Oncol 2018 [21] | 3 | 569 | nivolumab chemotherapy | OS (primary) | 14% nivolumab 16% chemotherapy | 1.4 (1.4–1.5) nivolumab 3.8 (3.0–4.2) chemotherapy HR 1.41 (95% CI 1.18–1.69) | 7.5 (5.7–9.2) nivo 8.4 (7.0–10.0) chemotherapy HR 0.86 (95 CI 0.72–1.04); p = 0.11 | |
| IFCT-1603 Pujol et al. Thorac Oncol 2019 [22] | 2 | 73 | Atezolizumab chemotherapy | ORR (primary) OS, PFS (secondary) | 2.3% atezolizumab 10% chemotherapy | 1.4 (1.2–1.5) atezolizumab 4.3 (1.5–5.9) chemotherapy HR 2.26 (95 CI 1.30–3.93); p = 0.004 | 9.5 (3.2–14.4) atezolizumab 8.7 (4.1–12.7) chemotherapy HR 0.84 (95% CI 0.45–1.58); p = 0.60 | |
| Kim et al. Lung Cancer 2019 [23] | 2 | paclitaxel + pembrolizumab | ORR (primary) PFS, OS, safety, biomarkers (secondary) | 23.1% | 5.0 (2.7–6.7) | 9.1 (6.5–15.0) | ||
| Sequist et al. Ann Oncol 2016 [24] | 1 | 17 | atezolizumab | PFS, OS, safety (primary) ORR (secondary) | 6% | 1.5 (1.2–2.7) | 5.9 (4.3–20.1) | |
| Goldman et al. JCO 2018 [25] | 1/2 | 21 | durvalumab | Safety (primary) OS, PFS; ORR (secondary) | 9.5% | 1.5 (0.9–1.8) | 4.8 (1.3–10.4) | |
| Cho et al. JCO 2018 [26] | 1 | 30 | durvalumab + tremelimumab | Safety, ORR (primary) OS, PFS, DoR (secondary) | 13.3% | 1.8 (1.0–1.9) | 7.9 (3.2–15.8) | |
| Maintenance | CheckMate 451 Owonikoko et al. JCO 2021 [27] | 3 | 834 | Nivo 1 mg/kg + ipi 3 mg/kg followed by nivo 240 mg (combination) nivolumab 240 mg placebo | OS (primary) PFS, ORR, DoR (secondary) | 9.1% combination 11.5% nivolumab 4.2% placebo | 1.7 (1.5–2.6) combination 1.9 (1.6–2.6) nivolumab 1.4 (1.4–1.5) placebo HR 0.72 (95% CI 0.60–0.87) combination vs. placebo | 9.2 (8.2–10.2) combination 10.4 (9.5–12.1) nivolumab, 9.6 (8.2–11.0) placebo HR 0.92 (95% CI 0.75–1.12); p = 0.37 |
| Gadgeel et al. JTO 2018 [28] | 2 | 45 | pembrolizumab | PFS (primary) OS, RR (secondary) | 11.1% | 1.4 (1.3–2.8) | 9.6 (7.0–12) |
| Trial ID | Phase | Setting | Treatment Arms | Primary Endpoint(s) | Secondary Endpoint(s) * | |
|---|---|---|---|---|---|---|
| Sistemic Treatements | NCT04730999 (CeLEBrATE) [34] | 2 | 1st line | CBDCA + etoposide + atezolimab + bevacizumab | OS | Safety and tolerability; ORR; PFS |
| → atezolizumab + bevacizumab | ||||||
| NCT03083691 (BIOLUMA) [30] | 2 | Relapsed/ | nivolumab + ipilimumab → nivolumab | ORR | OS; PFS; DoR | |
| recurrent | ||||||
| NCT03670056 [35] | 2 | Recurrent | nivolumab + ipilimumab → nivolumab | changes in Teff/Treg | RR; DoR; PFS | |
| cells ratio | ||||||
| NCT03406715 (MCC-19163) [36] | 2 | Recurrent | nivolumab + ipilimumab + Ad.p53-DC → nivolumab | DCR | PFS; OS; IR | |
| NCT02963090 (AFT-17) [37] | 2 | Progressed/ | pembrolizumab | PFS | - | |
| relapsed | topotecan | |||||
| NCT02489903 (QUADRUPLE THREAT) [38] | 2 | ≥3rd line or 2nd platinum refractory/resistant | RRx-001 → platinum rechallenge at progression (CBDCA/CDDP + etoposide) EP alone | OS | ORR; DCR; PFS | |
| NCT02937818 (BALTIC) [29] | 2 | Platinum refractory | durvalumab + tremelimumab (Arm A) | ORR | DoR, 12-weeks DC, TTR | |
| AZD1775 + CBDCA (Arm B) | ||||||
| AZD6739 + olaparib (Arb C) | ||||||
| Radiotherapy and Immunotherapy | NCT03585998 [39] | 2 | LS-SCLC | CRT + durvalumab → durvalumab consolidation | PFS | OS; Safety |
| NCT03540420 (ACHILES) [40] | 2 | LS-SCLC after CRT (EP) | Atezolizumab | OS | PFS, best response, | |
| observation | AEs | |||||
| NCT04189094 [41] | 2 | LS-SCLC | CRT ± concurrent sintilimab | PFS | OS; ORR | |
| NCT03811002 (NRG LU005) [42] | 2/3 | LS-SCLC | CRT ± concurrent atezolizumab | OS | PFS; AEs; ORR | |
| NCT04624204 [43] | 3 | LS-SCLC | CRT ± concurrent pembolizumab → pembrolizumab ± olaparib | PFS; OS | AEs; AEs-related discontinuations; OR | |
| NCT03703297 (ADRIATIC) [44] | 3 | LS-SCLC | durvalumab durvalumab + tremelimumab Placebo | PFS; OS (durvalumab vs. placebo) | OS; ORR; PFS (durvalumab + tremelimumab) | |
| NCT02402920 [45] | 1 | LS- and ES-SCLC | CRT/RT + concurrent pembrolizumab | MTD | RR, PFS, OS | |
| NCT03509012 (CLOVER) [46] | 1 | LS- and ES-SCLC | CRT + durvalumab ± tremelimumab | DLTs/Aes | PFS; OS; ORR | |
| NCT03043599 [47] | 1/2 | ES-SCLC | Thoracic RT + ipilimumab + nivolumab | IT dose (phase I); | OS | |
| PFS(phase II) | ||||||
| NCT03262454 [48] | 2 | ES SCLC recurrent/refractory | Atezolizumab + SHRT | OS | PFS | |
| NCT03923270 [49] | 1 | ES SCLC after 1st line EP | Thoracic RT + durvalumab Thoracic RT + durvalumab + tremelimumab (75 mg) Thoracic RT + durvalumab + olaparib Thoraci RT + durvalumab + tremelimumab (300 mg) | SAEs (Phase 1); PFS (Phase 1b) | PFS; OS | |
| NCT04402788 (RAPTOR) [50] | 2/3 | consolidation after standard 1st line | RT + atezolizumab | PFS | AEs; PFS (Phase 3); PFS according to the number of visible tumors | |
| (Phase 2) | ||||||
| atezolizumab | OS (Phase 3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guaitoli, G.; Neri, G.; Cabitza, E.; Natalizio, S.; Mastrodomenico, L.; Talerico, S.; Trudu, L.; Lauro, C.; Chiavelli, C.; Baschieri, M.C.; et al. Dissecting Immunotherapy Strategies for Small Cell Lung Cancer: Antibodies, Ionizing Radiation and CAR-T. Int. J. Mol. Sci. 2022, 23, 12728. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232112728
Guaitoli G, Neri G, Cabitza E, Natalizio S, Mastrodomenico L, Talerico S, Trudu L, Lauro C, Chiavelli C, Baschieri MC, et al. Dissecting Immunotherapy Strategies for Small Cell Lung Cancer: Antibodies, Ionizing Radiation and CAR-T. International Journal of Molecular Sciences. 2022; 23(21):12728. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232112728
Chicago/Turabian StyleGuaitoli, Giorgia, Giovanni Neri, Eleonora Cabitza, Salvatore Natalizio, Luciana Mastrodomenico, Sabrina Talerico, Lucia Trudu, Chiara Lauro, Chiara Chiavelli, Maria Cristina Baschieri, and et al. 2022. "Dissecting Immunotherapy Strategies for Small Cell Lung Cancer: Antibodies, Ionizing Radiation and CAR-T" International Journal of Molecular Sciences 23, no. 21: 12728. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232112728