
The Potential Effect of Lidocaine, Ropivacaine, Levobupivacaine and Morphine on Breast Cancer Pre-Clinical Models: A Systematic Review

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Results


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors Year | Type of Study | Drug Concentration | Outcome | Observations |
|---|---|---|---|---|
| Lidocaine | ||||
| Liu et al. [28] 2021 | In vitro MDA-MB-231 AU565 T47D MDA-MB-468 MCF-7 BT474 BT-20 | 0.3–3 mM | ↓ |
|
| Lin et al. [29] 2021 | In vitro MCF-7 | 0.01–0.2 mmol/L | ↓ |
|
| Freeman et al. [26] 2019 | In vivo Female BALB/c with 4T1 tumour cells | 1.5–2 mg/kg/h | ↓ |
|
| Chamaraux-Tran et al. [30] 2018 | In vitro MCF-10A MCF-7 MDA-MB-231 SKBr3 HER2+ | 0.1–10 mM | ↓ |
|
| In vivo SCID female mice inoculated with MDA-MB-231 cells | 100 mg/kg | ↓ |
| |
| Li et al. [31] 2018 | In vitro MCF-10A | 10–100 μM | = |
|
| 0.3–10 mM | = | |||
| MCF-7 | 10–100 μM | = | ||
| 0.3–10 mM | ↓ | |||
| MDA-MB-231 | 10–100 μM | = | ||
| 0.3–10 mM | ↓ | |||
| Agostino et al. [32] 2018 | In vitro MDA-MB-231 | 0.001–100 μM | ↓ |
|
| Jiang et al. [33] 2016 | In vitro MDA-MB-231 | 0.01–0.1 μM | = |
|
| 1–10 mM | ↓ | |||
| Chang et al. [34] 2014 | In vitro MCF-10A | 2–32 mM | = |
|
| MCF-7 | 1–16 mM | ↓ | ||
| In vivo Female BALB/c nude mice inoculated with MCF-7 cells | 21.3 mM | ↓ | ||
| Lirk et al. [23] 2014 | In vitro BT-20 MCF-7 | 10–100 μM | ↓ |
|
| Lirk et al. [35] 2012 | In vitro BT-20 MCF-7 | 0.01–0.1 mM | = |
|
| 1 mM | ↓ | |||
| Ropivacaine | ||||
| Zhao et al. [36] 2021 | In vitro MDA-MB-231 MDA-MB-468 MCF-10A SKBr3 HER2+ MCF7 BT474 | 1 mmol/L | ↓ |
|
| In vivo Balb/c nude mice injected with MDA-MB-231 cells | 40 μmol/Kg | ↓ |
| |
| Castelli et al. [37] 2019 | In vitro MDA-MB-231 | 5–1000 μM | ↓ |
|
| Li et al. [31] 2018 | In vitro MCF-10A | 3.5–35 μM | = |
|
| 0.3–10 mM | = | |||
| MCF-7 | 3.5–35 μM | = | ||
| 0.3–10 mM | ↓ | |||
| MDA-MB-231 | 3.5–35 μM | ↓ | ||
| 0.3–10 mM | ↓ | |||
| Gong et al. [25] 2018 | In vitro MDA-MB-468 SKBr3 HER2+ | 0.1–1 mM | ↓ |
|
| Lirk et al. [23] 2014 | In vitro BT-20 MCF-7 | 3–30 μM | = |
|
| Levobupivacaine | ||||
| Kwakye et al. [38] 2020 | In vitro MCF-7 MDA-MB-231 | 1–3 mM | ↓ |
|
| Castelli et al. [37] 2019 | In vitro MDA-MB-231 | 5–1000 μM | ↓ |
|
| Li et al. [31] 2018 | In vitro MCF-10A | 2.5–25 μM | = |
|
| 0.3–10 mM | = | |||
| MCF-7 | 2.5–25 μM | = | ||
| 0.3–10 mM | ↓ | |||
| MDA-MB-231 | 2.5–25 μM | = | ||
| 0.3–10 mM | ↓ | |||
| Morphine | ||||
| Cheng et al. [39] 2019 | In vitro MDA-MB-231 | 10 μmol/mL | ↑ |
|
| In vivo BALB/c-nu specific-pathogen-free mice with MDA-MB-231 cells | 10 mg/kg | ↑ | ||
| Chen et al. [40] 2017 | In vitro MCF-7 | 0.01–10 μM | ↓ |
|
| Bimonte et al. [41] 2015 | In vitro MCF-7 MDA-MB-231 | 1–100 μM | ↑ |
|
| In vivo Foxn1nu/nu mice with MDA-MB-231 | 0.714–1.43 mg/kg/day | ↑ |
| |
| Doornebal et al. [42] 2015 | In vivo Female wild-type syngeneic FVB/N mice | 10 mg/kg/12 h | = |
|
| Female MMTV-NeuT mice (BALB/c background) | 20 mg/kg/12 h | = | ||
| Niu et al. [43] 2015 | In vitro MCF-7 BT549 MCF-10A | 1–10 μM | ↑ |
|
| In vivo NOD/SCID mouse model inoculated with BT549 cells | 5–15 mg/kg | ↑ | ||
| Nguyen et al. [44] 2014 | In vivo C3TAG mice henceforth | 0.5–1.5 mg/kg/day | ↑ |
|
| Ge et al. [24] 2014 | In vitro MCF-7 | 50–1250 μM | ↓ |
|
| Ecimovic et al. [45] 2011 | In vitro MDA-MB-231 MCF-7 | 10–100 ng/mL | ↑ |
|
| Ustun et al. [46] 2010 | In vivo BALB/c bearing Ehrlich carcinoma | 0.714 mg/kg/day | ↑ |
|
3. Discussion
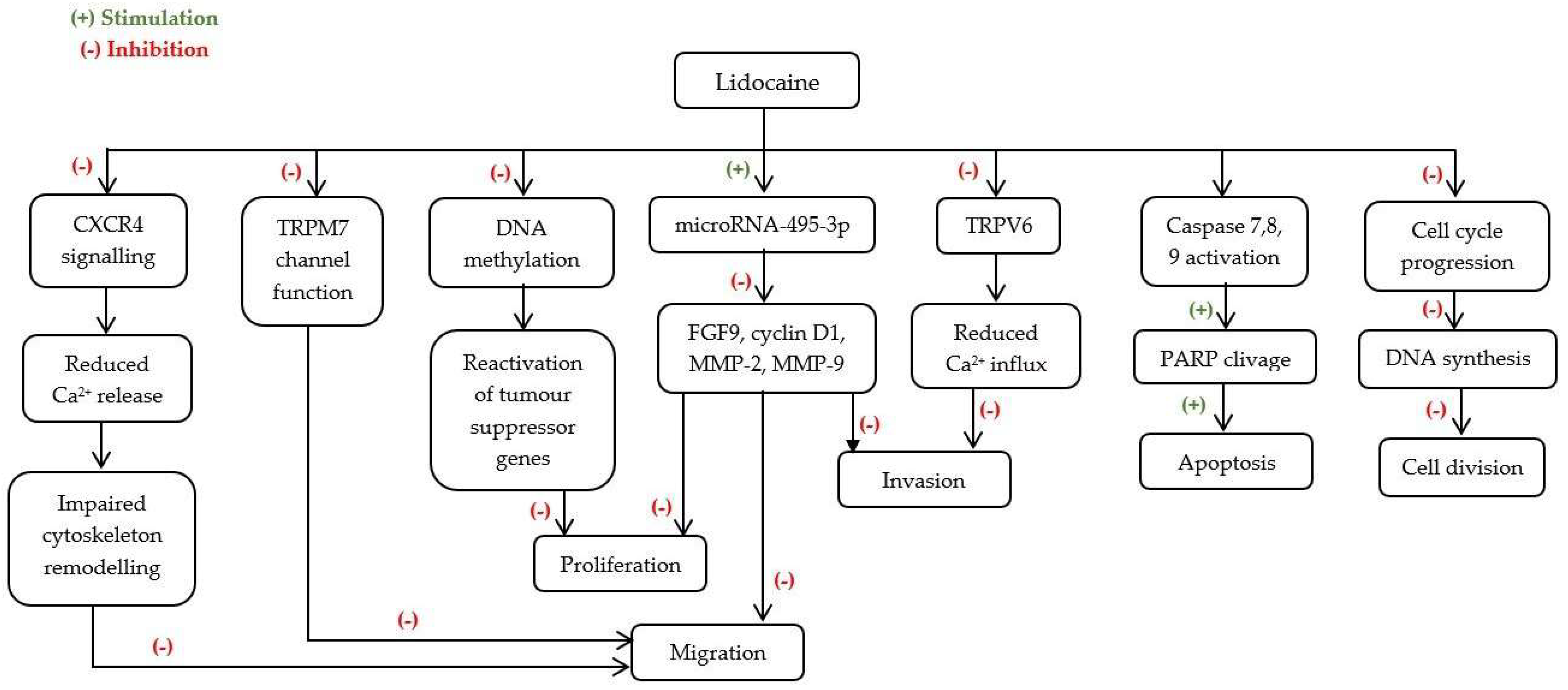
3.1. Lidocaine
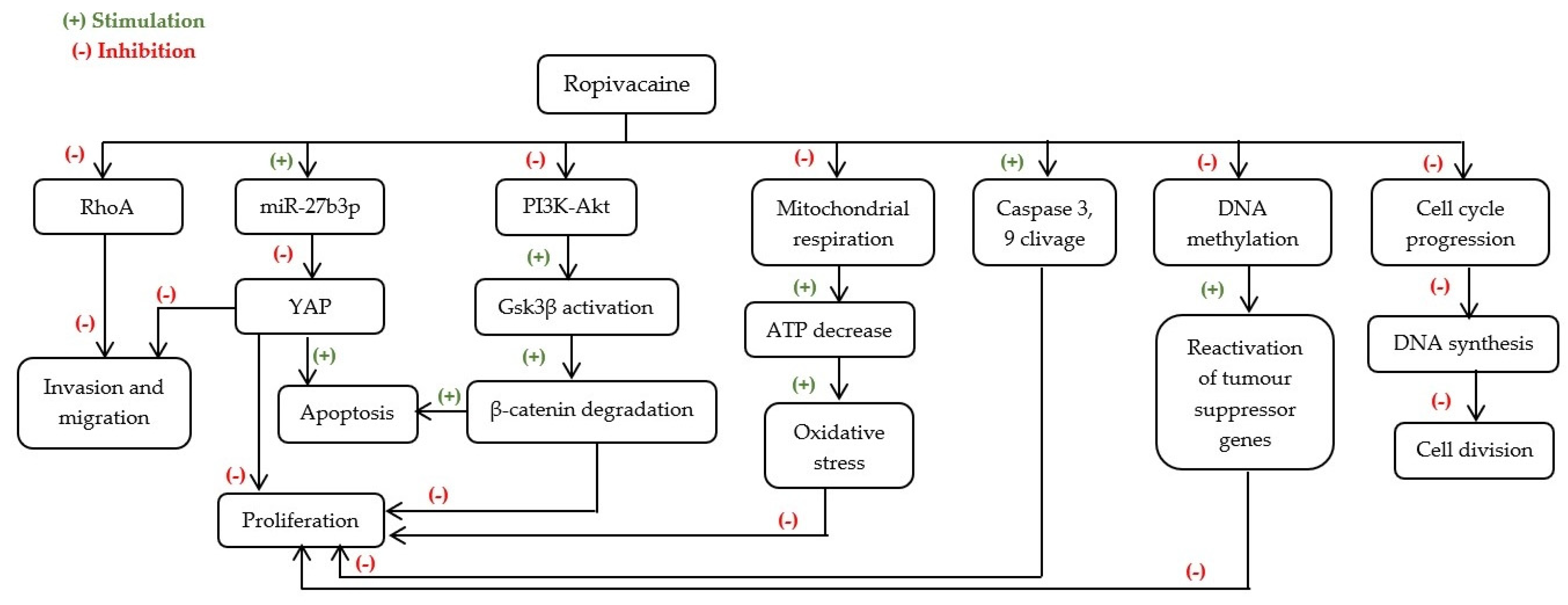
3.2. Ropivacaine
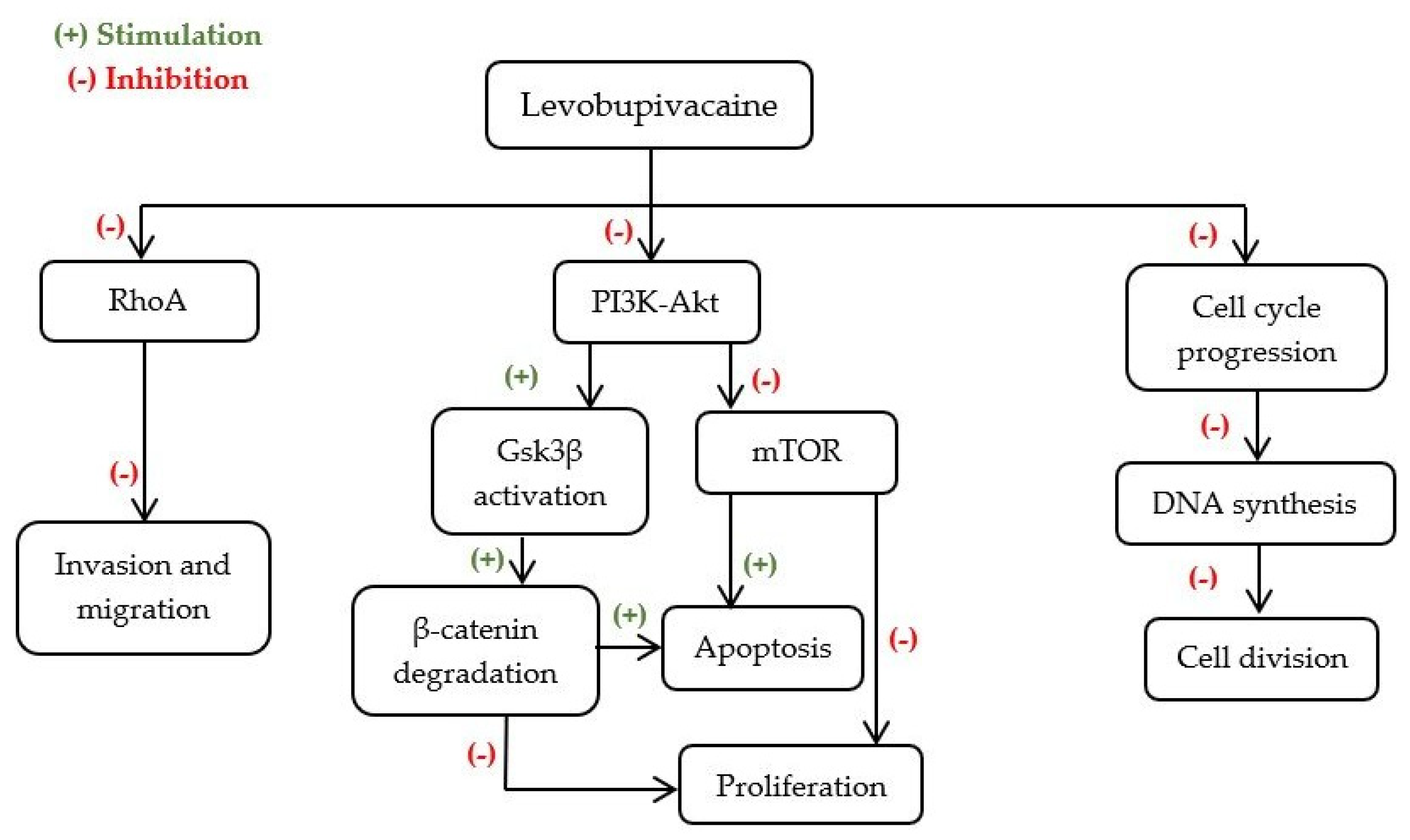
3.3. Levobupivacaine
3.4. Morphine
3.5. Limitations of This Study
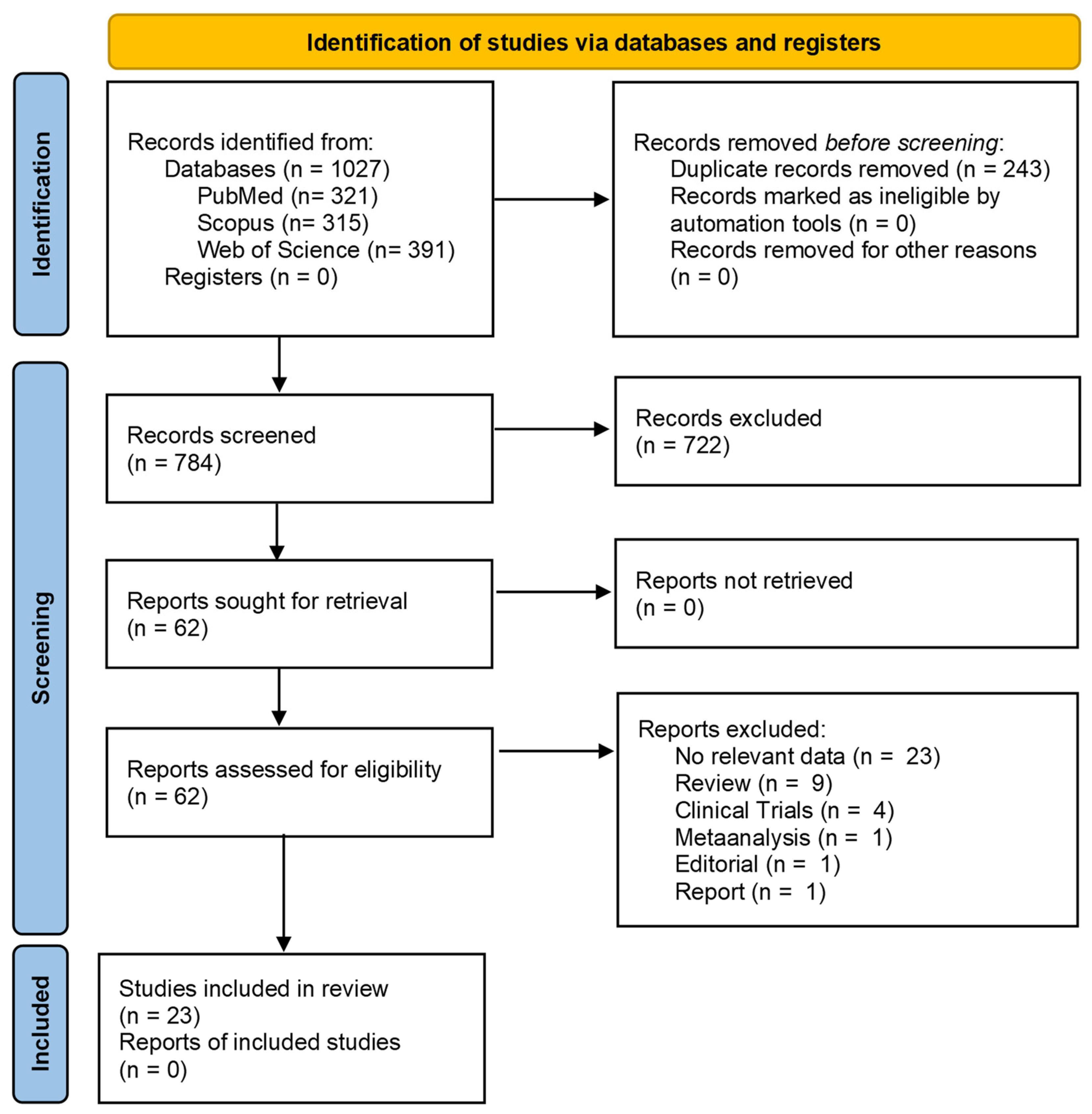
4. Materials and Methods
4.1. Search Strategy
4.2. Inclusion and Exclusion Criteria
4.3. Data Collection, Extraction and Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- 2020 Cancer Incidence and Mortality in EU-27 Countries EU Science Hub. Available online: https://ec.europa.eu/jrc/en/news/2020-cancer-incidence-and-mortality-eu-27-countries (accessed on 17 July 2021).
- Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 17 July 2021).
- Heaney, Á.; Buggy, D.J. Can anaesthetic and analgesic techniques affect cancer recurrence or metastasis? Br. J. Anaesth. 2012, 109, i17–i28. [Google Scholar] [CrossRef] [PubMed]
- Nounou, M.I.; Elamrawy, F.; Ahmed, N.; Abdelraouf, K.; Goda, S.; Syed-Sha-Qhattal, H. Breast cancer: Conventional diagnosis and treatment modalities and recent patents and technologies. Breast Cancer Basic Clin. Res. 2015, 9, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Naderi, J.; Samani, F.; Amooheidari, A.; Javanmard, S.H.; Vahabzadeh, G.; Vaseghi, G. Evaluation of effects of morphine and ionizing radiation in cancer cell lines. J. Cancer Res. Ther. 2019, 15, S144–S152. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Patel, N.; Bueno, F.R.; Hymel, B.; Vadivelu, N.; Kodumudi, G.; Urman, R.D. Effect of opiates, anesthetic techniques, and other perioperative factors on surgical cancer patients. Ochsner J. 2014, 14, 216–228. [Google Scholar]
- Wall, T.; Sherwin, A.; Ma, D.; Buggy, D.J. Influence of perioperative anaesthetic and analgesic interventions on oncological outcomes: A narrative review. Br. J. Anaesth. 2019, 123, 135–150. [Google Scholar] [CrossRef]
- Xuan, W.; Hankin, J.; Zhao, H.; Yao, S.; Ma, D. The potential benefits of the use of regional anesthesia. Int. J. Cancer 2015, 2784, 2774–2784. [Google Scholar] [CrossRef]
- Vahabi, S.; Eatemadi, A. Effects of anesthetic and analgesic techniques on cancer metastasis. Biomed. Pharmacother. 2017, 87, 1–7. [Google Scholar] [CrossRef]
- Xing, W.; Chen, D.T.; Pan, J.H.; Chen, Y.H.; Yan, Y.; Li, Q.; Zeng, W.A. Lidocaine Induces Apoptosis and Suppresses Tumor Growth in Human Hepatocellular Carcinoma Cells in Vitro and in a Xenograft Model in Vivo. Anesthesiology 2017, 126, 868–881. [Google Scholar] [CrossRef]
- Gottschalk, A.; Ford, J.; Durieux, M.E.; Tiouririne, M. The Role of the Perioperative Period in Recurrence. Anesth. Analg. 2010, 110, 1636–1643. [Google Scholar] [CrossRef]
- Xuan, W.; Zhao, H.; Hankin, J.; Chen, L.; Yao, S.; Ma, D. Local anesthetic bupivacaine induced ovarian and prostate cancer apoptotic cell death and underlying mechanisms in vitro. Nat. Publ. Group 2016, 6, 1–12. [Google Scholar] [CrossRef]
- Liston, D.R.; Davis, M. Clinically relevant concentrations of anticancer drugs: A guide for nonclinical studies. Clin. Cancer Res. 2017, 23, 3489–3498. [Google Scholar] [CrossRef]
- Baptista-Hon, D.T.; Robertson, F.M.; Robertson, G.B.; Owen, S.J.; Rogers, G.W.; Lydon, E.L.; Hales, T.G. Potent inhibition by ropivacaine of metastatic colon cancer SW620 cell invasion and NaV1.5 channel function. Br. J. Anaesth. 2014, 113, i39–i48. [Google Scholar] [CrossRef]
- Grandhi, R.K.; Lee, S.; Abd-Elsayed, A. The Relationship Between Regional Anesthesia and Cancer: A Metaanalysis. Ochsner J. 2017, 17, 345–361. [Google Scholar] [PubMed]
- Afsharimani, B.; Cabot, P.J.; Parat, M.-O. Morphine use in cancer surgery. Front. Pharmacol. 2011, 2, 46. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; David, F.; Villari, P.; Spedale, V.M.; Casuccio, A. Methadone versus morphine for postoperative pain in patients undergoing surgery for gynecological cancer: A randomized controlled clinical trial. J. Clin. Anesth. 2020, 61, 109627. [Google Scholar] [CrossRef] [PubMed]
- Morphine Sulfate Overdose. The Recovery Village Drug and Alcohol Rehab. Available online: https://www.therecoveryvillage.com/morphine-sulfate-addiction/overdose/ (accessed on 17 March 2021).
- Cox, B.; Durieux, M.E.; Marcus, M.A.E. Toxicity of local anaesthetics. Best Pract. Res. Clin. Anaesthesiol. 2003, 17, 111–136. [Google Scholar] [CrossRef]
- Townley, S.A. Book Review: Pharmacology for Anaesthesia and Intensive Care. Anaesth. Intensive Care 2008, 36, 926. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Morphine Dosage Guide with Precautions—Drugs.com. Available online: https://www.drugs.com/dosage/morphine.html (accessed on 17 March 2021).
- Lirk, P.; Hollmann, M.W.; Fleischer, M.; Weber, N.C.; Fiegl, H. Lidocaine and ropivacaine, but not bupivacaine, demethylate deoxyribonucleic acid in breast cancer cells in vitro. Br. J. Anaesth. 2014, 113, i32–i38. [Google Scholar] [CrossRef]
- Ge, Z.-H.; Wang, Z.-X.; Yu, T.-L.; Yang, N.; Sun, Y.; Hao, C.-L.; Sun, L.X. Morphine improved the antitumor effects on MCF-7 cells in combination with 5-Fluorouracil. Biomed. Pharmacother. 2014, 68, 299–305. [Google Scholar] [CrossRef]
- Gong, X.; Dan, J.; Li, F.; Wang, L. Suppression of mitochondrial respiration with local anesthetic ropivacaine targets breast cancer cells. J. Thorac. Dis. 2018, 10, 2804–2812. [Google Scholar] [CrossRef]
- Freeman, J.; Crowley, P.D.; Foley, A.G.; Gallagher, H.C.; Iwasaki, M.; Ma, D.; Buggy, D.J. Effect of Perioperative Lidocaine, Propofol and Steroids on Pulmonary Metastasis in a Murine Model of Breast Cancer Surgery. Cancers 2019, 11, 613. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Liu, H.; Dilger, J.P.; Lin, J. Lidocaine Suppresses Viability and Migration of Human Breast Cancer Cells: TRPM7 as a Target for Some Breast Cancer Cell Lines. Cancers 2021, 13, 234. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Yang, L. Study on Lidocaine Inhibiting Proliferation, Migration and Invasion of Breast Cancer Cells by Modulating the MicroRNA-495-3p/Fibroblast Growth Factor 9 Axis. Indian J. Pharm. Sci. 2021, 83, 931–938. [Google Scholar] [CrossRef]
- Chamaraux-Tran, T.-N.; Mathelin, C.; Aprahamian, M.; Joshi, G.P.; Tomasetto, C.; Diemunsch, P.; Akladios, C. Antitumor Effects of Lidocaine on Human Breast Cancer Cells: An In Vitro and In Vivo Experimental Trial. Anticancer Res. 2018, 38, 95–105. [Google Scholar] [CrossRef]
- Li, R.; Xiao, C.; Liu, H.; Huang, Y.; Dilger, J.P.; Lin, J. Effects of local anesthetics on breast cancer cell viability and migration. BMC Cancer 2018, 18, 666. [Google Scholar] [CrossRef]
- Agostino, G.D.; Saporito, A.; Cecchinato, V.; Silvestri, Y.; Borgeat, A.; Anselmi, L.; Uguccioni, M. Lidocaine inhibits cytoskeletal remodelling and human breast cancer cell migration. Br. J. Anaesth. 2018, 121, 962–968. [Google Scholar] [CrossRef]
- Jiang, Y.; Gou, H.; Zhu, J.; Tian, S.; Yu, L. Lidocaine inhibits the invasion and migration of TRPV6-expressing cancer cells by TRPV6 downregulation. Oncol. Lett. 2016, 12, 1164–1170. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Liu, C.-L.; Chen, M.-J.; Hsu, Y.-W.; Chen, S.-N.; Lin, C.-H.; Hu, M.C. Local anesthetics induce apoptosis in human breast tumor cells. Anesth. Analg. 2014, 118, 116–124. [Google Scholar] [CrossRef]
- Lirk, P.; Berger, R.; Hollmann, M.W.; Fiegl, H. Lidocaine time- and dose-dependently demethylates deoxyribonucleic acid in breast cancer cell lines in vitro. Br. J. Anaesth. 2012, 109, 200–207. [Google Scholar] [CrossRef]
- Zhao, L.; Han, S.; Hou, J.; Shi, W.; Zhao, Y.; Chen, Y. The local anesthetic ropivacaine suppresses progression of breast cancer by regulating miR-27b-3p/YAP axis. Aging 2021, 13, 16341. [Google Scholar] [CrossRef] [PubMed]
- Castelli, V.; Giordano, A.; Benedetti, E.; Ippoliti, R.; Varrassi, G.; Cimini, A. Local anesthetics counteract cell proliferation and migration of human triple—negative breast cancer and melanoma cells. J. Cell. Physiol. 2020, 235, 3474–3484. [Google Scholar] [CrossRef] [PubMed]
- Kwakye, A.K.; Kampo, S.; Lv, J.; Ramzan, M.N.; Richard, S.A.; Falagán, A.A.; Wen, Q.P. Levobupivacaine inhibits proliferation and promotes apoptosis of breast cancer cells by suppressing the PI3K/Akt/mTOR signalling pathway. BMC Res. Notes 2020, 13, 1–8. [Google Scholar] [CrossRef]
- Cheng, S.; Guo, M.; Liu, Z.; Fu, Y.; Wu, H.; Wang, C.; Cao, M. Morphine Promotes the Angiogenesis of Postoperative Recurrent Tumors and Metastasis of Dormant Breast Cancer Cells. Pharmacology 2019, 104, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Qin, Y.; Li, L.; Chen, J.; Zhang, X.; Xie, Y. Morphine can inhibit the growth of breast cancer MCF-7 cells by arresting the cell cycle and inducing apoptosis. Biol. Pharm. Bull. 2017, 40, 1686–1692. [Google Scholar] [CrossRef]
- Bimonte, S.; Barbieri, A.; Rea, D.; Palma, G.; Luciano, A.; Cuomo, A.; Izzo, F. Morphine Promotes Tumor Angiogenesis and Increases Breast Cancer Progression. BioMed Res. Int. 2015, 2015, 161508. [Google Scholar] [CrossRef]
- Doornebal, C.W.; Vrijland, K.; Hau, C.-S.; Coffelt, S.B.; Ciampricotti, M.; Jonkers, J.; Hollmann, M.W. Morphine does not facilitate breast cancer progression in two preclinical mouse models for human invasive lobular and HER2(+) breast cancer. Pain 2015, 156, 1424–1432. [Google Scholar] [CrossRef]
- Niu, D.-G.; Peng, F.; Zhang, W.; Guan, Z.; Zhao, H.-D.; Li, J.-L.; Liu, Q. Morphine promotes cancer stem cell properties, contributing to chemoresistance in breast cancer. Oncotarget 2015, 6, 3963. [Google Scholar] [CrossRef]
- Nguyen, J.; Luk, K.; Vang, D.; Soto, W.; Vincent, L.; Robiner, S.; Gupta, K. Morphine stimulates cancer progression and mast cell activation and impairs survival in transgenic mice with breast cancer. Br. J. Anaesth. 2014, 113, i4–i13. [Google Scholar] [CrossRef]
- Ecimovic, P.; Murray, D.; Doran, P.; McDonald, J.; Lambert, D.G.; Buggy, D.J. Direct effect of morphine on breast cancer cell function in vitro: Role of the NET1 gene. Br. J. Anaesth. 2011, 107, 916–923. [Google Scholar] [CrossRef]
- Ustun, F.; Durmus-Altun, G.; Altaner, S.; Tuncbilek, N.; Uzal, C.; Berkarda, S. Evaluation of morphine effect on tumour angiogenesis in mouse breast tumour model, EATC. Med. Oncol. 2010, 28, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Chamaraux-Tran, T.-N.; Piegeler, T. The Amide Local Anesthetic Lidocaine in Cancer Surgery-Potential Antimetastatic Effects and Preservation of Immune Cell Function? Narrat. Review. Front. Med. 2017, 4, 235. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Chen, L.; Zhao, H.; Wu, L.; Masters, J.; Han, C.; Ma, D. Both Bupivacaine and Levobupivacaine inhibit colon cancer cell growth but not melanoma cells in vitro. J. Anesth. 2019, 33, 17–25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cancer Pain Relief; World Health Organization: Geneva, Switzerland, 1986; pp. 1–79. Available online: https://apps.who.int/iris/handle/10665/43944 (accessed on 17 March 2021).
- Vargas-Schaffer, G. Is the WHO analgesic ladder still valid? Twenty-four years of experience. Can. Fam. Physician 2010, 56, 514–517. [Google Scholar] [CrossRef] [PubMed]




| Anaesthetic/Opioid | Injectable Concentration | Recommended Infusion Dose | Maximum Single Dose | Reference |
|---|---|---|---|---|
| Lidocaine | 5–20 mg/mL | 1.2 mg/kg/h | 4.5 mg/kg (300 mg) | [19,20] |
| Morphine | 2–10 mg/mL | 0.1–0.2 mg/kg/4 h | No maximum dose | [21,22] |
| Ropivacaine | 2.5–7.5 mg/mL | - | 3 mg/kg (200 mg) | [19,20] |
| Levobupivacaine | 2–10 mg/mL | - | 2 mg/kg (150 mg) | [19,20] |
| Database | Search Formula |
|---|---|
| Medline (via PubMed) | ((((“breast cancer”[TIAB]) OR “Breast Neoplasms”[TIAB] OR “Breast Neoplasms”[MESH]) OR “breast carcinoma”[TIAB])) AND (((((ropivacaine[TIAB]) OR ropivacaine[MESH] OR levobupivacaine[TIAB] OR levobupivacaine[MESH]) OR morphine[TIAB] OR morphine[MESH]) OR lidocaine[TIAB] OR lidocaine[MESH]) OR methadone[TIAB] OR methadone[MESH]) |
| Scopus | TITLE-ABS-KEY((“breast cancer” OR “Breast Neoplasms” OR “breast carcinoma”) AND (ropivacaine OR levobupivacaine OR morphine OR lidocaine OR methadone)) |
| Web of Science | (TS = ((“breast cancer” OR “Breast Neoplasms” OR “breast carcinoma”) AND “ropivacaine” OR “levobupivacaine” OR “morphine” OR “lidocaine” OR “methadone”))) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matos, A.C.; Marques, I.A.; Pires, A.S.; Valentim, A.; Abrantes, A.M.; Botelho, M.F. The Potential Effect of Lidocaine, Ropivacaine, Levobupivacaine and Morphine on Breast Cancer Pre-Clinical Models: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 1894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031894
Matos AC, Marques IA, Pires AS, Valentim A, Abrantes AM, Botelho MF. The Potential Effect of Lidocaine, Ropivacaine, Levobupivacaine and Morphine on Breast Cancer Pre-Clinical Models: A Systematic Review. International Journal of Molecular Sciences. 2022; 23(3):1894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031894
Chicago/Turabian StyleMatos, Ana Catarina, Inês Alexandra Marques, Ana Salomé Pires, Ana Valentim, Ana Margarida Abrantes, and Maria Filomena Botelho. 2022. "The Potential Effect of Lidocaine, Ropivacaine, Levobupivacaine and Morphine on Breast Cancer Pre-Clinical Models: A Systematic Review" International Journal of Molecular Sciences 23, no. 3: 1894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031894