

The Correlation between Peripheral Blood Index and Immune Cell Expansion in Vietnamese Elderly Lung Cancer Patients

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. The Peripheral Blood Indexes
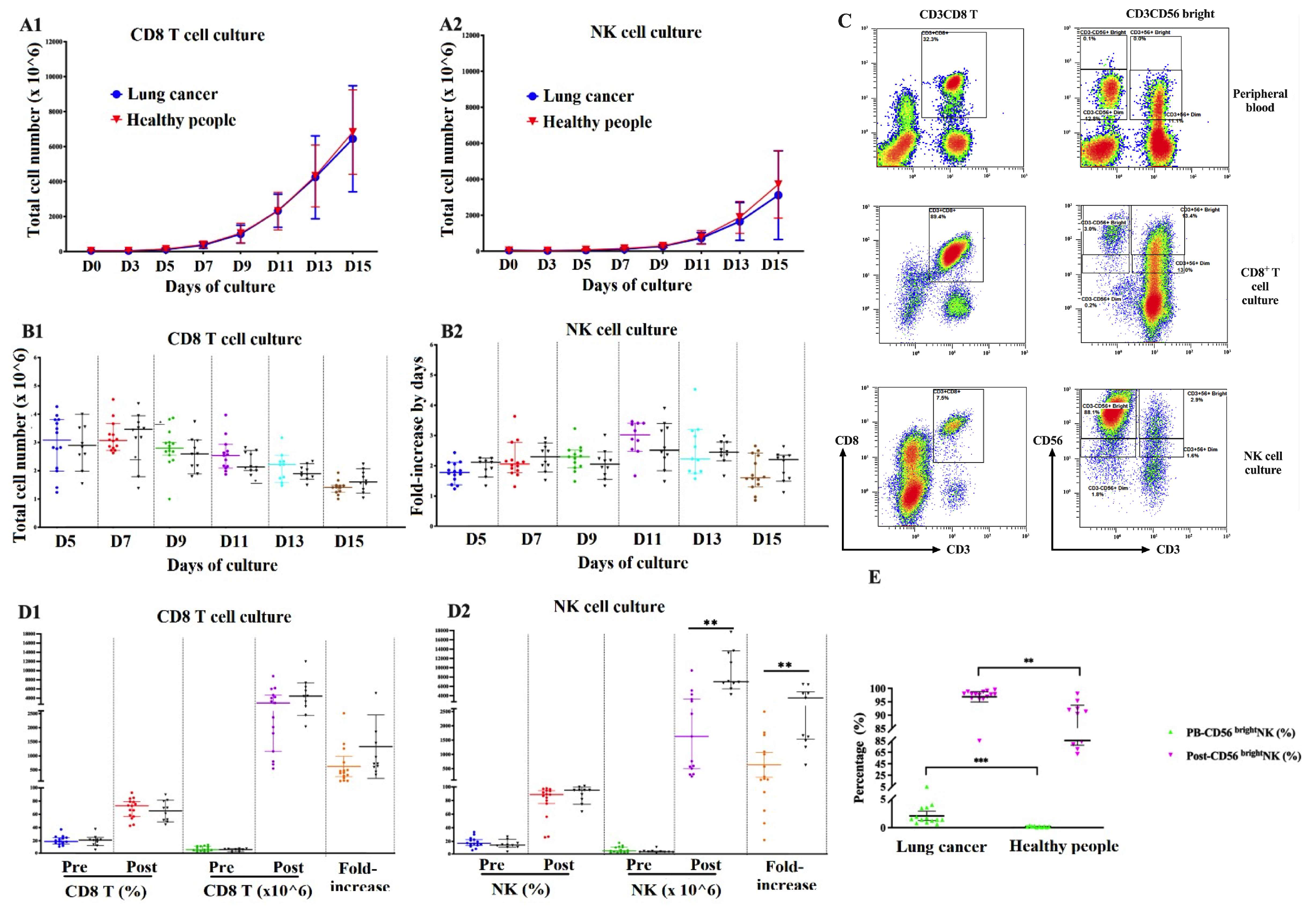
2.3. Immune Cell Expansion Capacity
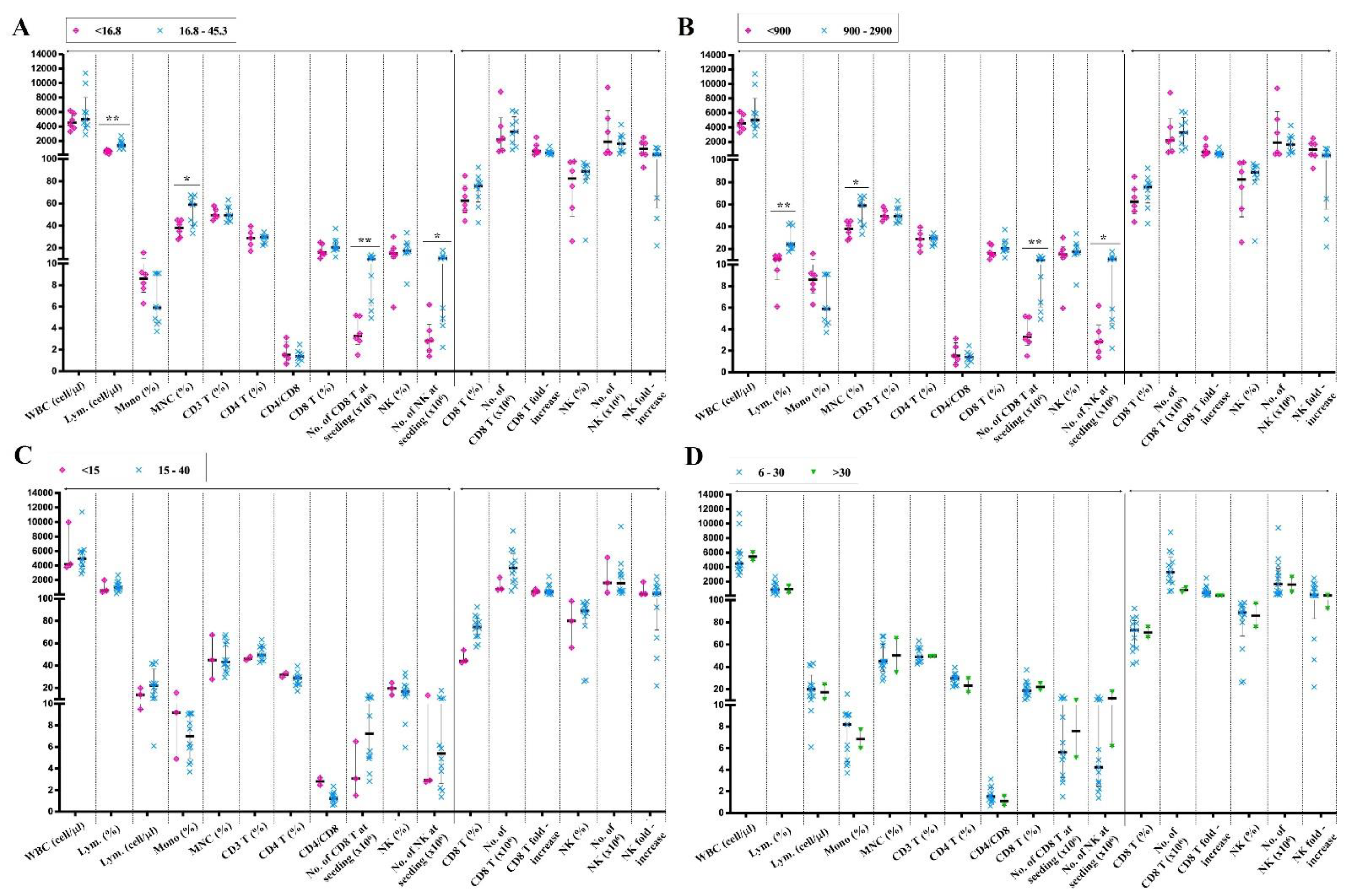
2.4. The Immune Cell Expansion in Out-of-Range Samples
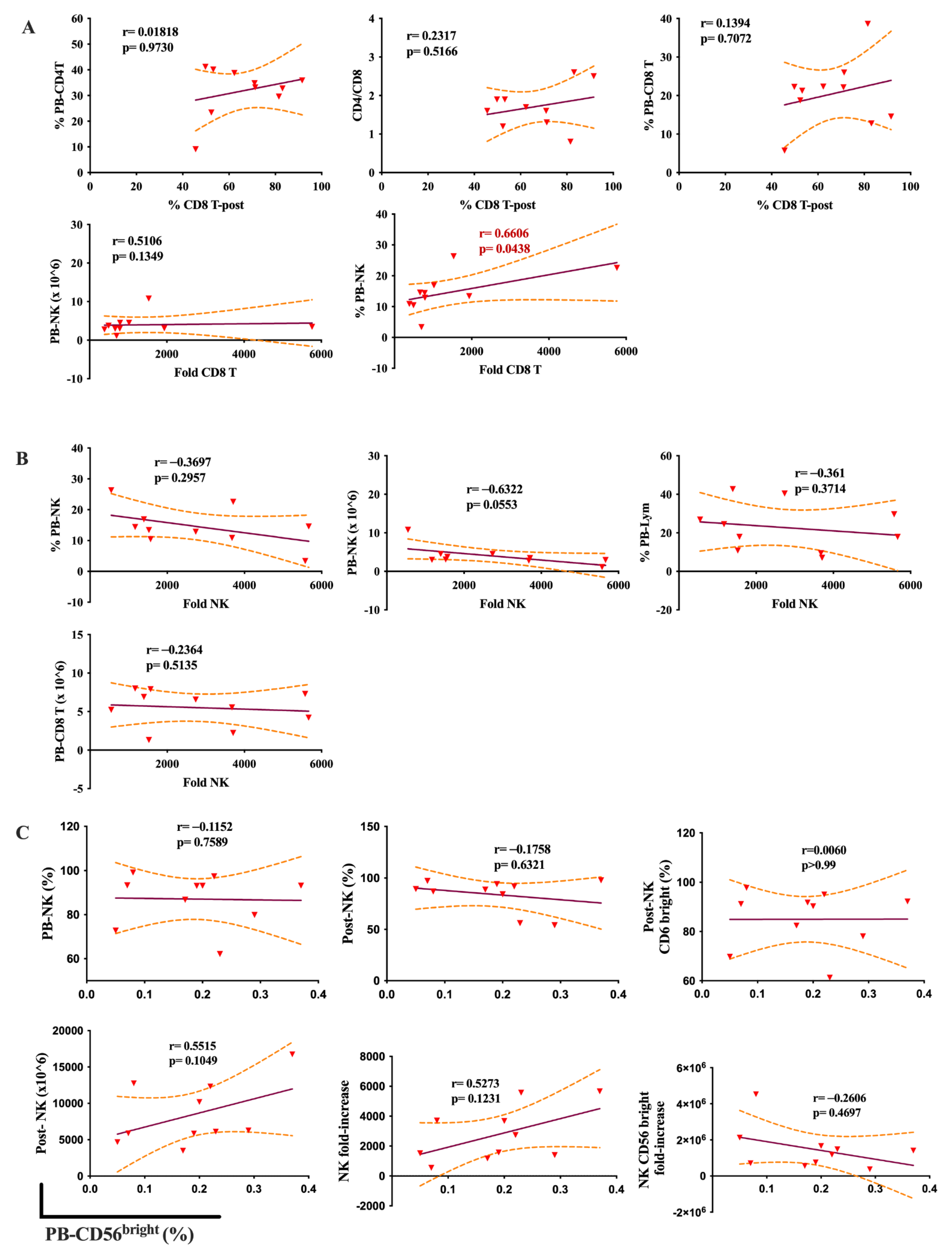
2.5. The Relationship between the PB Indices and the Immune Cell Expansion
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Data Collection
4.3. Immune Cell Expansion
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversannce, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Shin, M.H.; Kim, J.; Lim, S.A.; Kim, J.; Kim, S.-J.; Lee, K.-M. NK Cell-Based Immunotherapies in Cancer. Immune Netw. 2020, 20, e14. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Park, Y.; Ahn, J.W.; Sim, J.; Kang, S.J.; Hwang, S.; Chun, J.; Choi, H.; Kim, S.H.; Chun, D.H.; et al. Autologous adoptive immune-cell therapy elicited a durable response with enhanced immune reaction signatures in patients with recurrent glioblastoma: An open-label, phase I/IIa trial. PLoS ONE 2021, 16, e0247293. [Google Scholar] [CrossRef]
- Terunuma, H.; Deng, X.; Nishino, N.; Watanabe, K. NK cell-based autologous immune enhancement therapy (AIET) for cancer. J. Stem Cells Regen. Med. 2013, 9, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, R.; Terunuma, H.; Balamurugan, M.; Dedeepiya, V.D.; Sumana, P.; Senthilkumar, R.; Rajmohan, M.; Karthick, R.; Preethy, S.; Abraham, S.J.K. Cell-based immunotherapy in stage IIIA inflammatory breast cancer with declining innate immunity following successive chemotherapies: A case report. Mol. Clin. Oncol. 2017, 7, 493–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, T.; Okayama, T.; Sakamoto, N.; Ideno, M.; Oka, K.; Enoki, T.; Mineno, J.; Yoshida, N.; Katada, K.; Kamada, K.; et al. Phase I clinical trial of adoptive transfer of expanded natural killer cells in combination with IgG1 antibody in patients with gastric or colorectal cancer. Int. J. Cancer 2018, 142, 2599–2609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, C.L.; McCormick, S.; Gill, N.; Kugathasan, K.; Santosuosso, M.; Donaldson, N.; Heinrichs, D.E.; Ashkar, A.; Xing, Z. NK cells play a critical protective role in host defense against acute extracellular Staphylococcus aureus bacterial infection in the lung. J. Immunol. 2008, 180, 5558–5568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.; Tramsen, L.; Hanisch, M.; Latgé, J.-P.; Huenecke, S.; Koehl, U.; Lehrnbecher, T. Human natural killer cells exhibit direct activity against aspergillus fumigatus hyphae, but not against resting conidia. J. Infect. Dis. 2011, 203, 430–435. [Google Scholar] [CrossRef] [Green Version]
- Sagiv, A.; Biran, A.; Yon, M.; Simon, J.; Lowe, S.W.; Krizhanovsky, V. Granule exocytosis mediates immune surveillance of senescent cells. Oncogene 2013, 32, 1971–1977. [Google Scholar] [CrossRef] [Green Version]
- Thorén, F.B.; Riise, R.E.; Ousbäck, J.; Della Chiesa, M.; Alsterholm, M.; Marcenaro, E.; Pesce, S.; Prato, C.; Cantoni, C.; Bylund, J.; et al. Human NK Cells induce neutrophil apoptosis via an NKp46- and Fas-dependent mechanism. J. Immunol. 2012, 188, 1668–1674. [Google Scholar] [CrossRef] [Green Version]
- Waggoner, S.N.; Cornberg, M.; Selin, L.K.; Welsh, R.M. Natural killer cells act as rheostats modulating antiviral T cells. Nature 2011, 481, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Matsuyama, S.; Miyake, S.; Suga, K.; Nakachi, K. Natural cytotoxic activity of peripheral-blood lymphocytes and cancer incidence: An 11-year follow-up study of a general population. Lancet 2000, 356, 1795–1799. [Google Scholar] [CrossRef] [PubMed]
- Kishton, R.J.; Sukumar, M.; Restifo, N.P. Metabolic regulation of T cell longevity and function in tumor immunotherapy. Cell Metab. 2017, 26, 94–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Cheever, M.A.; Higano, C.S. PROVENGE (Sipuleucel-T) in prostate cancer: The first FDA-approved therapeutic cancer vaccine. Clin. Cancer Res. 2011, 17, 3520–3526. [Google Scholar] [CrossRef] [Green Version]
- Gounder, S.S.; Abdullah, B.J.J.; Radzuanb, N.; Zain, F.; Sait, N.B.M.; Chua, C.; Subramani, B. Effect of aging on NK cell population and their proliferation at ex vivo culture condition. Anal Cell Pathol. 2018, 2018, 7871814. [Google Scholar] [CrossRef] [Green Version]
- Lutz, C.T.; Karapetyan, A.; Al-Attar, A.; Shelton, B.J.; Holt, K.J.; Tucker, J.H.; Presnell, S.R. Human NK cells proliferate and die in vivo more rapidly than T cells in healthy young and elderly adults. J. Immunol. 2011, 186, 4590–4598. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Gross, D.; Elbaum, P.; Murasko, D.M. Aging affects initiation and continuation of T cell proliferation. Mech. Ageing Dev. 2007, 128, 332–339. [Google Scholar] [CrossRef]
- Li, M.; Yao, D.; Zeng, X.; Kasakovski, D.; Zhang, Y.; Chen, S.; Zha, X.; Li, Y.; Xu, L. Age related human T cell subset evolution and senescence. Immun. Ageing 2019, 16, 24. [Google Scholar] [CrossRef] [Green Version]
- Xia, A.; Zhang, Y.; Xu, J.; Yin, T.; Lu, X.J. T Cell Dysfunction in Cancer Immunity and Immunotherapy. Front. Immunol. 2019, 10, 1719. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, D.M.; Guerrero, M.E.; Maldonado, B.M.; Vollbracht, C.; Herrera, S.A. Total lymphocyte count in cancer patients with lymphopenia treated with intravenous vitamin C: Results of an observational study. Transl. Med. Commun. 2017, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Caligiuri, M.A. Human natural killer cells. Blood 2008, 112, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Fauriat, C.; Long, E.O.; Ljunggren, H.G.; Bryceson, Y.T. Regulation of human NK-cell cytokine and chemokine production by target cell recognition. Blood 2010, 115, 2167–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauernhofer, T.; Kuss, I.; Henderson, B.; Baum, A.S.; Whiteside, T.L. Preferential apoptosis of CD56dim natural killer cell subset in patients with cancer. Eur. J. Immunol. 2003, 33, 119–124. [Google Scholar] [CrossRef]
- Chan, A.; Hong, D.L.; Atzberger, A.; Kollnberger, S.; Filer, A.D.; Buckley, C.D.; McMichael, A.; Enver, T.; Bowness, P. CD56bright human NK cells differentiate into CD56dim cells: Role of contact with peripheral fibroblasts. J. Immunol. 2007, 179, 89–94. [Google Scholar] [CrossRef] [Green Version]
- De Jonge, K.; Ebering, A.; Nassiri, S.; Maby-El Hajjami, H.; Ouertatani-Sakouhi, H.; Baumgaertner, P.; Speiser, D.E. Circulating CD56(bright) NK cells inversely correlate with survival of melanoma patients. Sci. Rep. 2019, 9, 4487. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, N.; Ji, N.; Hurez, V.; Curiel, T.J.; Montgomery, M.O.; Braun, A.J.; Nicolas, M.; Aguilera, M.; Kaushik, D.; Liu, Q.; et al. Intratumoral CD56(bright) natural killer cells are associated with improved survival in bladder cancer. Oncotarget 2018, 9, 36492–36502. [Google Scholar] [CrossRef] [Green Version]
- Koo, K.C.; Shim, D.H.; Yang, C.M.; Lee, S.B.; Kim, S.M.; Shin, T.Y.; Kim, K.H.; Yoon, H.G.; Rha, K.H.; Lee, J.M.; et al. Reduction of the CD16(-)CD56bright NK cell subset precedes NK cell dysfunction in prostate cancer. PLoS ONE 2013, 8, e78049. [Google Scholar] [CrossRef] [Green Version]
- Rana, A.P.; Kaur, M.; Zonunsanga, B.; Puri, A.; Kuka, A.S. Preoperative peripheral blood count in breast carcinoma: Predictor of prognosis or a routine test. Int. J. Breast Cancer 2015, 2015, 964392. [Google Scholar] [CrossRef] [Green Version]
- An, N.; Wang, H.; Jia, W.; Jing, W.; Liu, C.; Zhu, H.; Yu, J. The prognostic role of circulating CD8(+) T cell proliferation in patients with untreated extensive stage small cell lung cancer. J. Transl. Med. 2019, 17, 402. [Google Scholar] [CrossRef] [Green Version]
- Araujo, B.d.L.V.; Hansen, M.; Spanggaard, I.; Rohrberg, K.; Reker Hadrup, S.; Lassen, U.; Svane, I.M. Immune cell profiling of peripheral blood as signature for a response during checkpoint inhibition across cancer types. Front. Oncol. 2021, 11, 558248. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Marquez, M.A.; Thelen, M.; Reinke, S.; Keller, D.; Wennhold, K.; Lehmann, J.; Veldman, J.; Borchmann, S.; Rosenwald, A.; Sasse, S.; et al. Reverted exhaustion phenotype of circulating lymphocytes as immune correlate of anti-PD1 first-line treatment in Hodgkin lymphoma. Leukemia 2021, 36, 760–771. [Google Scholar] [CrossRef] [PubMed]
- Pawelec, G. Immunosenescence and cancer. Biogerontology 2017, 18, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Witkowski, J.M.; Kotb, R.; Hirokawa, K.; Pawelec, G. Immunosenescence and cancer. Crit. Rev. Oncog. 2013, 18, 489–513. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liu, S.; Zhang, B.; Qiao, L.; Zhang, Y. T Cell Dysfunction and Exhaustion in Cancer. Front Cell Dev. Biol. 2020, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, S.M.; Lee, J.; Bae, S.J.; Baik, S.J.; Ji, J.; Kim, D.; Ahn, S.G.; Jeong, J. Body mass index and absolute lymphocyte count predict disease-free survival in Korean breast cancer patients. Br. J. Cancer 2021, 125, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Ellsworth, S.; Campian, J.; Wild, A.T.; Herman, J.M.; Laheru, D.; Brock, M.; Balmanoukian, A.; Ye, X. Survival in patients with severe lymphopenia following treatment with radiation and chemotherapy for newly diagnosed solid tumors. J. Natl. Compr. Canc. Netw. 2015, 13, 1225–1231. [Google Scholar] [CrossRef] [Green Version]
- Wild, A.T.; Ye, X.; Ellsworth, S.G.; Smith, J.A.; Narang, A.K.; Garg, T.; Campian, J.; Laheru, D.A.; Zheng, L.; Wolfgang, C.L.; et al. The Association between chemoradiation-related lymphopenia and clinical outcomes in patients with locally advanced pancreatic adenocarcinoma. Am. J. Clin. Oncol. 2015, 38, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Campian, J.L.; Sarai, G.; Ye, X.; Marur, S.; Grossman, S.A. Association between severe treatment-related lymphopenia and progression-free survival in patients with newly diagnosed squamous cell head and neck cancer. Head Neck 2014, 36, 1747–1753. [Google Scholar] [CrossRef] [Green Version]
- Afghahi, A.; Purington, N.; Han, S.S.; Desai, M.; Pierson, E.; Mathur, M.B.; Seto, T.; Thompson, C.A.; Rigdon, J.; Telli, M.L.; et al. Higher absolute lymphocyte counts predict lower mortality from early-stage triple-negative breast cancer. Clin. Cancer Res. 2018, 24, 2851–2858. [Google Scholar] [CrossRef] [Green Version]
- Lee, O.H.; Min, S.-Y. Decrease of peripheral blood lymphocyte count predicts response to neoadjuvant chemotherapy in breast cancer patients. Korean J. Clin. Oncol. 2020, 16, 79–88. [Google Scholar] [CrossRef]
- Wesselius, L.J.; Wheaton, D.L.; Manahan-Wahl, L.J.; Sherard, S.L.; Taylor, S.A.; Abdou, N.A. Lymphocyte subsets in lung cancer. Chest 1987, 91, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Luo, H.; Liang, S.; Chen, J.; Liu, A.; Niu, L.; Jiang, Y. Pembrolizumab plus allogeneic NK cells in advanced non-small cell lung cancer patients. J. Clin. Invest. 2020, 130, 2560–2569. [Google Scholar] [CrossRef] [PubMed]
- Iliopoulou, E.G.; Kountourakis, P.; Karamouzis, M.V.; Doufexis, D.; Ardavanis, A.; Baxevanis, C.N.; Rigatos, G.; Papamichail, M.; Perez, S.A. A phase I trial of adoptive transfer of allogeneic natural killer cells in patients with advanced non-small cell lung cancer. Cancer Immunol. Immunother. 2010, 59, 1781–1789. [Google Scholar] [CrossRef]
- Becker, P.S.; Suck, G.; Nowakowska, P.; Ullrich, E.; Seifried, E.; Bader, P.; Tonn, T.; Seidl, C. Selection and expansion of natural killer cells for NK cell-based immunotherapy. Cancer Immunol. Immunother. 2016, 65, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Deng, X.; Terunuma, H.; Terunuma, A.; Takane, T.; Nieda, M. Ex vivo-expanded natural killer cells kill cancer cells more effectively than ex vivo-expanded γδ T cells or αβ T cells. Int. Immunopharmacol. 2014, 22, 486–491. [Google Scholar] [CrossRef]
- Li, L.; Li, W.; Wang, C.; Yan, X.; Wang, Y.; Niu, C.; Zhang, X.; Li, M.; Tian, H.; Yao, C.; et al. Adoptive transfer of natural killer cells in combination with chemotherapy improves outcomes of patients with locally advanced colon carcinoma. Cytotherapy 2018, 20, 134–148. [Google Scholar] [CrossRef]
- Chidrawar, S.M.; Khan, N.; Chan, Y.L.; Nayak, L.; Moss, P.A. Ageing is associated with a decline in peripheral blood CD56bright NK cells. Immun. Ageing 2006, 3, 10. [Google Scholar] [CrossRef] [Green Version]
- Nelson, A.; Lukacs, J.D.; Johnston, B. The Current landscape of NKT cell immunotherapy and the hills ahead. Cancers 2021, 13, 5174. [Google Scholar] [CrossRef]
- Shissler, S.C.; Bollino, D.R.; Tiper, I.V.; Bates, J.P.; Derakhshandeh, R.; Webb, T.J. Immunotherapeutic strategies targeting natural killer T cell responses in cancer. Immunogenetics 2016, 68, 623–638. [Google Scholar] [CrossRef] [Green Version]
- Liem, N.T.; Van Phong, N.; Kien, N.T.; Anh, B.V.; Huyen, T.L.; Thao, C.T.; Tu, N.D.; Hiep, D.T.; Hoai Thu, D.T.; Nhung, H.T.M. Phase I clinical trial using autologous ex vivo expanded NK cells and cytotoxic T lymphocytes for cancer treatment in Vietnam. Int. J. Mol. Sci. 2019, 20, 3166. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age Mean (SD) Median [Min; Max] * | Stage | Metastatic Site | Pretreatment | Duration of AIET after Surgery or the 1st Chemotherapy (Months) Mean (SD) Median [Min; Max] | Estimated Survival Prior to AIET (Months) Mean (SD) Median [Min; Max] * |
|---|---|---|---|---|---|---|---|
| 59.0 (12.4) 60.0 [32.2; 82.1] | 16.2 (15.0) 12.0 [2; 48] | 12.0 (4.64) 12.0 [3.0; 20.0] | |||||
| PT 1 | F | 59.96 | IV | M1 m (pleural) | Surgical/Chemo | 48 | 12 |
| PT 2 | F | 58.52 | III | M0 | Chemo | 24 | 15 |
| PT 3 | M | 57.56 | IV | M0 | Chemo | 3 | 16 |
| PT 4 | F | 61.64 | III | M0 | Surgical/Chemo | 24 | 20 |
| PT 5 | F | 52.47 | III | M0 | Surgical/Chemo | 12 | 18 |
| PT 6 | F | 59.95 | IV | M1 m (bone) | Chemo | 48 | 14 |
| PT 7 | F | 59.27 | IV | M0 | Chemo/Radiation | 2 | 16 |
| PT 8 | F | 40.0 | IV | M1 m (brain) | Chemo/Radiation | 13 | 8 |
| PT 9 | F | 51.63 | IV | M1 m (brain) | Surgical/Chemo | 24 | 12 |
| PT 10 | F | 32.24 | IV | M1 m | Surgical/Chemo | 6 | 10 |
| PT 11 | M | 65.76 | IV | M1 m (liver) | Chemo | 4 | 12 |
| PT 12 | F | 82.12 | IV | M1 m (liver) | Chemo/Radiation | 12 | 3 |
| PT 13 | M | 78.10 | III | M0 | Chemo/Radiation | 6 | 8 |
| PT 14 | F | 63.74 | IV | M1 m (bone) | Surgical/Chemo | 4 | 6 |
| PT 15 | M | 61.52 | IV | M1 m (brain) | Surgical/Chemo | 13 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, H.-P.; Bui, V.A.; Hoang, A.-X.T.; Van Nguyen, P.; Nguyen, D.-T.; Mai, H.T.; Le, H.-A.; Nguyen, T.-L.; Hoang, N.T.M.; Nguyen, L.T.; et al. The Correlation between Peripheral Blood Index and Immune Cell Expansion in Vietnamese Elderly Lung Cancer Patients. Int. J. Mol. Sci. 2023, 24, 4284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054284
Nguyen H-P, Bui VA, Hoang A-XT, Van Nguyen P, Nguyen D-T, Mai HT, Le H-A, Nguyen T-L, Hoang NTM, Nguyen LT, et al. The Correlation between Peripheral Blood Index and Immune Cell Expansion in Vietnamese Elderly Lung Cancer Patients. International Journal of Molecular Sciences. 2023; 24(5):4284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054284
Chicago/Turabian StyleNguyen, Hoang-Phuong, Viet Anh Bui, Ai-Xuan Thi Hoang, Phong Van Nguyen, Dac-Tu Nguyen, Hien Thi Mai, Hai-Anh Le, Thanh-Luan Nguyen, Nhung Thi My Hoang, Liem Thanh Nguyen, and et al. 2023. "The Correlation between Peripheral Blood Index and Immune Cell Expansion in Vietnamese Elderly Lung Cancer Patients" International Journal of Molecular Sciences 24, no. 5: 4284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054284