
Blood-Based Biomarkers as Prognostic Factors of Recurrent Disease after Radical Cystectomy: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Inclusion and Exclusion
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
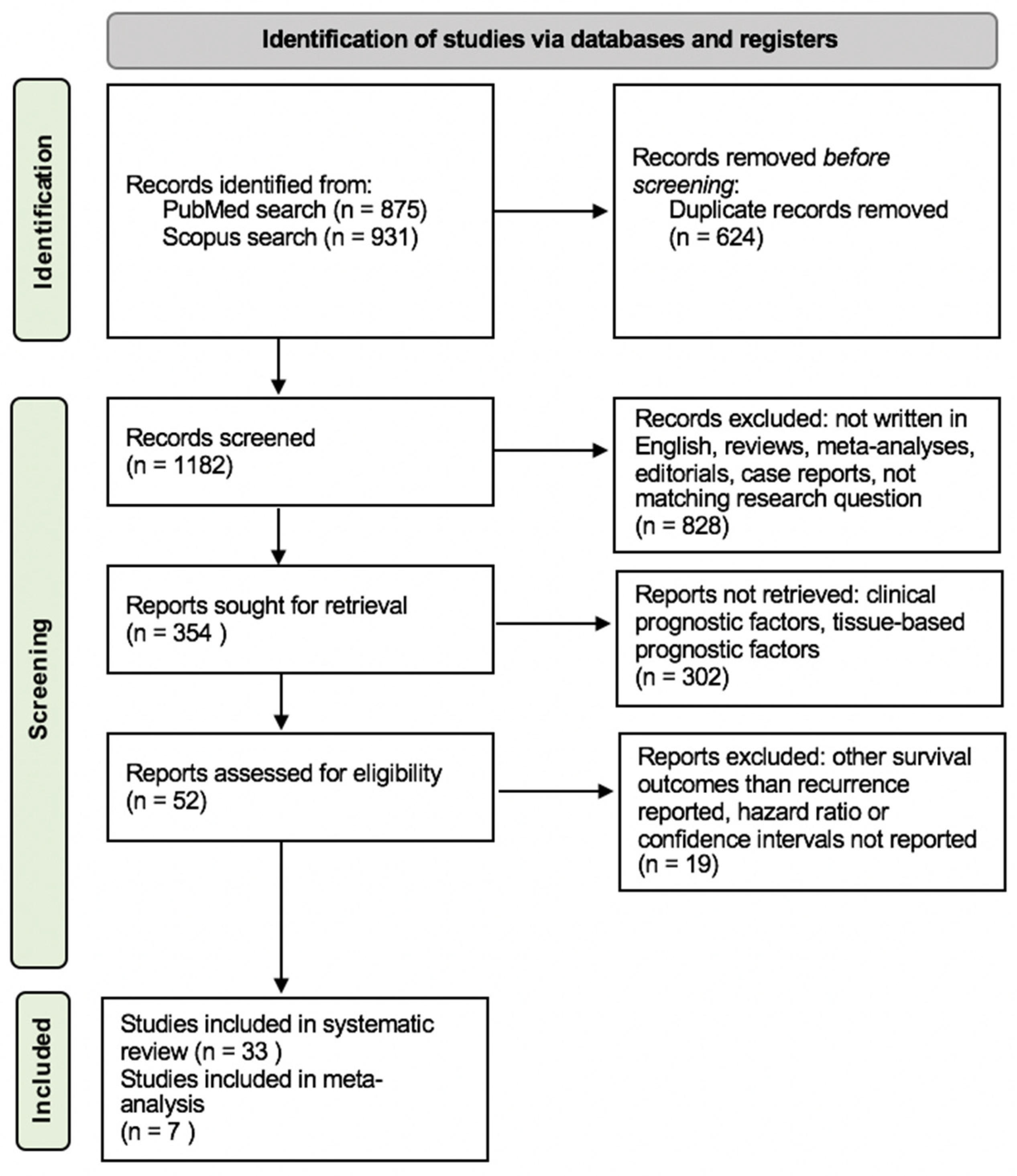
3.1. Search Results
3.2. Study Characteristics
3.3. Systematic Review of Blood-Based Biomarkers
3.3.1. Inflammatory Biomarkers
3.3.2. Serum Carbohydrate Antigen and Carcinoembryonic Antigen
3.3.3. Circulating Tumor Cells and DNA
3.3.4. Nutritional Status Biomarkers
3.3.5. Factors of Angiogenesis and Vascular Endothelial Growth
3.3.6. Other Blood-Based Biomarkers
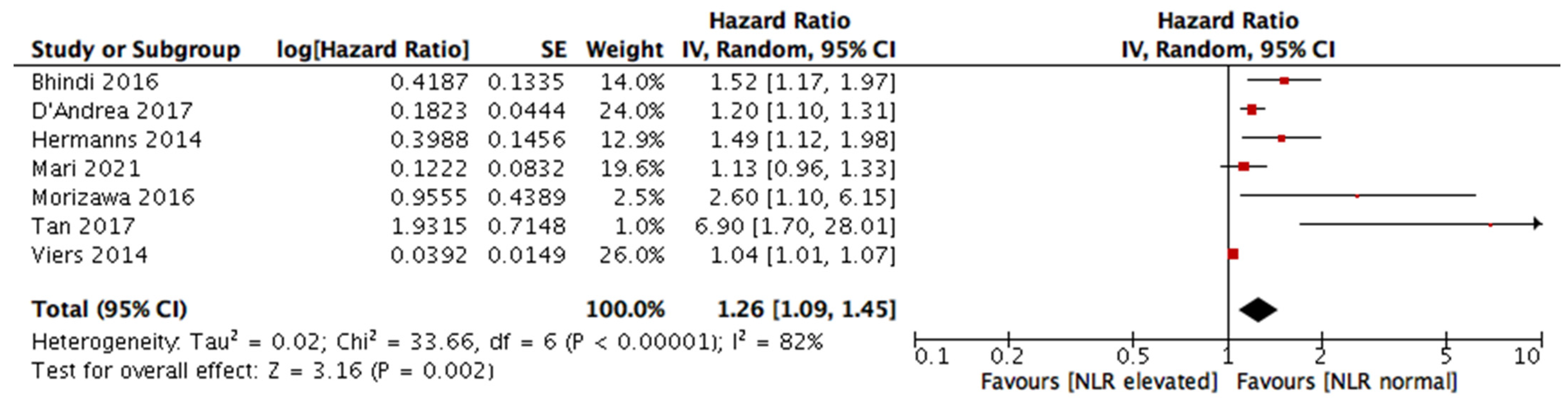
3.4. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xylinas, E.; Robinson, B.; Kluth, L.; Volkmer, B.; Hautmann, R.; Küfer, R.; Zerbib, M.; Kwon, E.; Thompson, R.; Boorjian, S.; et al. Association of T-cell co-regulatory protein expression with clinical outcomes following radical cystectomy for urothelial carcinoma of the bladder. Eur. J. Surg. Oncol. EJSO 2014, 40, 121–127. [Google Scholar] [CrossRef]
- Shariat, S.F.; Karakiewicz, P.I.; Palapattu, G.S.; Lotan, Y.; Rogers, C.G.; Amiel, G.E.; Vazina, A.; Gupta, A.; Bastian, P.J.; Sagalowsky, A.I.; et al. Outcomes of Radical Cystectomy for Transitional Cell Carcinoma of the Bladder: A Contemporary Series from the Bladder Cancer Research Consortium. J. Urol. 2006, 176 Pt 1, 2414–2422; [Google Scholar] [CrossRef] [PubMed]
- Aziz, A.; May, M.; Burger, M.; Palisaar, R.-J.; Trinh, Q.-D.; Fritsche, H.-M.; Rink, M.; Chun, F.; Martini, T.; Bolenz, C.; et al. Prediction of 90-day Mortality after Radical Cystectomy for Bladder Cancer in a Prospective European Multicenter Cohort. Eur. Urol. 2014, 66, 156–163. [Google Scholar] [CrossRef]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical Cystectomy in the Treatment of Invasive Bladder Cancer: Long-Term Results in 1054 Patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Shariat, S.F.; Ashfaq, R.; Karakiewicz, P.I.; Saeedi, O.; Sagalowsky, A.I.; Lotan, Y. Survivin expression is associated with bladder cancer presence, stage, progression, and mortality. Cancer 2007, 109, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Kluth, L.A.; Black, P.C.; Bochner, B.H.; Catto, J.; Lerner, S.P.; Stenzl, A.; Sylvester, R.; Vickers, A.J.; Xylinas, E.; Shariat, S.F. Prognostic and Prediction Tools in Bladder Cancer: A Comprehensive Review of the Literature. Eur. Urol. 2015, 68, 238–253. [Google Scholar] [CrossRef]
- Shariat, S.F.; Zlotta, A.R.; Ashfaq, R.; Sagalowsky, A.I.; Lotan, Y. Cooperative effect of cell-cycle regulators expression on bladder cancer development and biologic aggressiveness. Mod. Pathol. 2007, 20, 445–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathieu, R.; Lucca, I.; Rouprêt, M.; Briganti, A.; Shariat, S.F. The prognostic role of lymphovascular invasion in urothelial carcinoma of the bladder. Nat. Rev. Urol. 2016, 13, 471–479. [Google Scholar] [CrossRef]
- Moschini, M.; D’Andrea, D.; Korn, S.; Irmak, Y.; Soria, F.; Compérat, E.; Shariat, S.F. Characteristics and clinical significance of histological variants of bladder cancer. Nat. Rev. Urol. 2017, 14, 651–668. [Google Scholar] [CrossRef]
- Svatek, R.S.; Shariat, S.F.; Lasky, R.E.; Skinner, E.C.; Novara, G.; Lerner, S.P.; Fradet, Y.; Bastian, P.J.; Kassouf, W.; Karakiewicz, P.I.; et al. The Effectiveness of Off-Protocol Adjuvant Chemotherapy for Patients with Urothelial Carcinoma of the Urinary Bladder. Clin. Cancer Res. 2010, 16, 4461–4467. [Google Scholar] [CrossRef] [Green Version]
- Isbarn, H.; Jeldres, C.; Zini, L.; Perrotte, P.; Baillargeon-Gagne, S.; Capitanio, U.; Shariat, S.F.; Arjane, P.; Saad, F.; McCormack, M.; et al. A Population Based Assessment of Perioperative Mortality After Cystectomy for Bladder Cancer. J. Urol. 2009, 182, 70–77. [Google Scholar] [CrossRef]
- Grossmann, N.C.; Rajwa, P.; Quhal, F.; König, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Katayama, S.; Motlagh, R.S.; Fankhauser, C.D.; et al. Comparative Outcomes of Primary versus Recurrent High-risk Non–muscle-invasive and Primary versus Secondary Muscle-invasive Bladder Cancer after Radical Cystectomy: Results from a Retrospective Multicenter Study. Eur. Urol. Open Sci. 2022, 39, 14–21. [Google Scholar] [CrossRef]
- Necchi, A.; Pond, G.R.; Moschini, M.; Plimack, E.R.; Niegisch, G.; Yu, E.Y.; Bamias, A.; Agarwal, N.; Vaishampayan, U.; Theodore, C.; et al. Development of a Prediction Tool for Exclusive Locoregional Recurrence after Radical Cystectomy in Patients with Muscle-Invasive Bladder Cancer. Clin. Genitourin. Cancer 2019, 17, 7–14.e3. [Google Scholar] [CrossRef] [PubMed]
- Ru, Y.; Dancik, G.M.; Theodorescu, D. Biomarkers for prognosis and treatment selection in advanced bladder cancer patients. Curr. Opin. Urol. 2011, 21, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Shariat, S.F.; Lotan, Y.; Vickers, A.; Karakiewicz, P.I.; Schmitz-Dräger, B.J.; Goebell, P.J.; Malats, N. Statistical consideration for clinical biomarker research in bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 389–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bensalah, K.; Montorsi, F.; Shariat, S.F. Challenges of Cancer Biomarker Profiling. Eur. Urol. 2007, 52, 1601–1609. [Google Scholar] [CrossRef]
- Gakis, G. The Role of Inflammation in Bladder Cancer. Adv. Exp. Med. Biol. 2014, 816, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Nabavizadeh, R.; Bobrek, K.; Master, V.A. Risk stratification for bladder cancer: Biomarkers of inflammation and immune activation. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 706–712. [Google Scholar] [CrossRef]
- Cancer-Related Inflammation|Nature. Available online: https://www-nature-com.ez.srv.pmu.ac.at/articles/nature07205 (accessed on 10 December 2022).
- Bhindi, B.; Hermanns, T.; Wei, Y.; Yu, J.; O Richard, P.; Wettstein, M.S.; Templeton, A.; Li, K.; Sridhar, S.S.; Jewett, M.A.S.; et al. Identification of the best complete blood count-based predictors for bladder cancer outcomes in patients undergoing radical cystectomy. Br. J. Cancer 2016, 114, 207–212. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, D.; Moschini, M.; Gust, K.M.; Abufaraj, M.; Özsoy, M.; Mathieu, R.; Soria, F.; Briganti, A.; Rouprêt, M.; Karakiewicz, P.I.; et al. Lymphocyte-to-monocyte ratio and neutrophil-to-lymphocyte ratio as biomarkers for predicting lymph node metastasis and survival in patients treated with radical cystectomy. J. Surg. Oncol. 2017, 115, 455–461. [Google Scholar] [CrossRef]
- Morizawa, Y.; Miyake, M.; Shimada, K.; Hori, S.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Tanaka, N.; Konishi, N.; Fujimoto, K. Neutrophil-to-lymphocyte ratio as a detection marker of tumor recurrence in patients with muscle-invasive bladder cancer after radical cystectomy. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 257.e11–257.e17. [Google Scholar] [CrossRef]
- Riva, J.J.; Malik, K.M.P.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167–171. [Google Scholar]
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.; Cai, J.; Miranda, G.; Groshen, S.; Skinner, D.; Stein, J.P. Usefulness of CA 125 as a preoperative prognostic marker for transitional cell carcinoma of the bladder. J. Urol. 2004, 172 Pt 1, 2182–2186. [Google Scholar] [CrossRef] [PubMed]
- Kouba, E.J.; Lentz, A.; Wallen, E.M.; Pruthi, R.S. Clinical use of serum CA-125 levels in patients undergoing radical cystectomy for transitional cell carcinoma of the bladder. Urol. Oncol. Semin. Orig. Investig. 2009, 27, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Hazzaa, S.M.; Elashry, O.M.; Afifi, I.K. Clusterin as a Diagnostic and Prognostic Marker for Transitional Cell Carcinoma of the Bladder. Pathol. Oncol. Res. 2010, 16, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Chun, F.K.; Dahlem, R.; Soave, A.; Minner, S.; Hansen, J.; Stoupiec, M.; Coith, C.; Kluth, L.A.; Ahyai, S.A.; et al. Prognostic Role and HER2 Expression of Circulating Tumor Cells in Peripheral Blood of Patients Prior to Radical Cystectomy: A Prospective Study. Eur. Urol. 2012, 61, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, H.; Djaladat, H.; Cai, J.; Miranda, G.; Daneshmand, S. Precystectomy serum levels of carbohydrate antigen 19-9, carbohydrate antigen 125, and carcinoembryonic antigen: Prognostic value in invasive urothelial carcinoma of the bladder. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 648–656. [Google Scholar] [CrossRef]
- Hermanns, T.; Bhindi, B.; Wei, Y.; Yu, J.; Noon, A.; O Richard, P.; Bhatt, J.R.; Almatar, A.; Jewett, M.A.S.; E Fleshner, N.; et al. Pre-treatment neutrophil-to-lymphocyte ratio as predictor of adverse outcomes in patients undergoing radical cystectomy for urothelial carcinoma of the bladder. Br. J. Cancer 2014, 111, 444–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viers, B.; Boorjian, S.A.; Frank, I.; Tarrell, R.F.; Thapa, P.; Karnes, R.J.; Thompson, R.H.; Tollefson, M.K. Pretreatment Neutrophil-to-Lymphocyte Ratio Is Associated with Advanced Pathologic Tumor Stage and Increased Cancer-specific Mortality Among Patients with Urothelial Carcinoma of the Bladder Undergoing Radical Cystectomy. Eur. Urol. 2014, 66, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Djaladat, H.; Bruins, H.M.; Miranda, G.; Cai, J.; Skinner, E.C.; Daneshmand, S. The association of preoperative serum albumin level and American Society of Anesthesiologists (ASA) score on early complications and survival of patients undergoing radical cystectomy for urothelial bladder cancer. BJU Int. 2014, 113, 887–893. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Dai, Y.; Zhou, F.; Long, Z.; Li, Y.; Liu, B.; Xie, D.; Tang, J.; Tan, J.; Yao, K.; et al. The prognostic role of preoperative serum albumin/globulin ratio in patients with bladder urothelial carcinoma undergoing radical cystectomy. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 484.e1–484.e8. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.G.; Eu, E.; On, W.L.K.; Huang, H.H. Pretreatment neutrophil-to-lymphocyte ratio predicts worse survival outcomes and advanced tumor staging in patients undergoing radical cystectomy for bladder cancer. Asian J. Urol. 2017, 4, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Christensen, E.; Birkenkamp-Demtröder, K.; Sethi, H.; Shchegrova, S.; Salari, R.; Nordentoft, I.K.; Wu, H.-T.; Knudsen, M.; Lamy, P.; Lindskrog, S.V.; et al. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J. Clin. Oncol. 2019, 37, 1547–1557. [Google Scholar] [CrossRef]
- Yuk, H.D.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. De Ritis Ratio (Aspartate Transaminase/Alanine Transaminase) as a Significant Prognostic Factor in Patients Undergoing Radical Cystectomy with Bladder Urothelial Carcinoma: A Propensity Score-Matched Study. Dis. Markers 2019, 2019, 6702964. [Google Scholar] [CrossRef] [Green Version]
- Ninomiya, S.; Kawahara, T.; Miyoshi, Y.; Yao, M.; Uemura, H. A retrospective study on the possible systematic inflammatory response markers to predict the prognosis of patients with bladder cancer undergoing radial cystectomy. Mol. Clin. Oncol. 2020, 13, 47. [Google Scholar] [CrossRef]
- Fallah, J.; Diaz-Montero, C.M.; Rayman, P.; Wei, W.; Finke, J.H.; Kim, J.S.; Pavicic, P.G.; Lamenza, M.; Dann, P.; Company, D.; et al. Myeloid-Derived Suppressor Cells in Nonmetastatic Urothelial Carcinoma of Bladder Is Associated with Pathologic Complete Response and Overall Survival. Clin. Genitourin. Cancer 2020, 18, 500–508. [Google Scholar] [CrossRef]
- Su, S.; Liu, L.; Sun, C.; Yang, L.; Nie, Y.; Chen, Y.; Zhang, J.; Li, S. Prognostic significance of serum lactate dehydrogenase in patients undergoing radical cystectomy for bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 852.e1–852.e9. [Google Scholar] [CrossRef] [PubMed]
- Dohn, L.; Thind, P.; Salling, L.; Lindberg, H.; Oersted, S.; Christensen, I.; Laerum, O.; Illemann, M.; von der Maase, H.; Høyer-Hansen, G.; et al. Circulating Forms of Urokinase-Type Plasminogen Activator Receptor in Plasma Can Predict Recurrence and Survival in Patients with Urothelial Carcinoma of the Bladder. Cancers 2021, 13, 2377. [Google Scholar] [CrossRef]
- Schuettfort, V.M.; D’andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Motlagh, R.S.; Rink, M.; Abufaraj, M.; Karakiewicz, P.I.; et al. Impact of preoperative serum albumin-globulin ratio on disease outcome after radical cystectomy for urothelial carcinoma of the bladder. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 235.e5–235.e14. [Google Scholar] [CrossRef]
- Li, S.; Lu, S.; Liu, X.; Chen, X. Association between the Pretreatment Albumin-to-Alkaline Phosphatase Ratio and Clinical Outcomes in Patients With Bladder Cancer Treated With Radical Cystectomy: A Retrospective Cohort Study. Front. Oncol. 2021, 11, 664392. [Google Scholar] [CrossRef]
- Mari, A.; Muto, G.; Di Maida, F.; Tellini, R.; Bossa, R.; Bisegna, C.; Campi, R.; Cocci, A.; Viola, L.; Grosso, A.; et al. Oncological impact of inflammatory biomarkers in elderly patients treated with radical cystectomy for urothelial bladder cancer. Arab. J. Urol. 2021, 19, 2–8. [Google Scholar] [CrossRef]
- Schuettfort, V.M.; Pradere, B.; D’Andrea, D.; Grossmann, N.C.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Rink, M.; Karakiewicz, P.I.; et al. Prognostic Impact of Preoperative Plasma Levels of Urokinase Plasminogen Activator Proteins on Disease Outcomes after Radical Cystectomy. J. Urol. 2021, 206, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Schuettfort, V.M.; D’Andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; König, F.; Rink, M.; Abufaraj, M.; Karakiewicz, P.I.; et al. A panel of systemic inflammatory response biomarkers for outcome prediction in patients treated with radical cystectomy for urothelial carcinoma. BJU Int. 2022, 129, 182–193. [Google Scholar] [CrossRef]
- Grossmann, N.C.; Schuettfort, V.M.; Pradere, B.; Rajwa, P.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Motlagh, R.S.; Aydh, A.; et al. Impact of preoperative systemic immune-inflammation Index on oncologic outcomes in bladder cancer patients treated with radical cystectomy. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 106.e11–106.e19. [Google Scholar] [CrossRef] [PubMed]
- Laukhtina, E.; Schuettfort, V.M.; D’andrea, D.; Pradere, B.; Mori, K.; Quhal, F.; Motlagh, R.S.; Mostafaei, H.; Katayama, S.; Grossmann, N.; et al. Preoperative plasma level of endoglin as a predictor for disease outcomes after radical cystectomy for nonmetastatic urothelial carcinoma of the bladder. Mol. Carcinog. 2022, 61, 5–18. [Google Scholar] [CrossRef]
- Motlagh, R.S.; Schuettfort, V.M.; Mori, K.; Katayama, S.; Rajwa, P.; Aydh, A.; Grossmann, N.C.; Laukhtina, E.; Pradere, B.; Mostafai, H.; et al. Prognostic impact of insulin-like growth factor-I and its binding proteins, insulin-like growth factor-I binding protein-2 and -3, on adverse histopathological features and survival outcomes after radical cystectomy. Int. J. Urol. 2022, 29, 676–683. [Google Scholar] [CrossRef]
- Mori, K.; Schuettfort, V.M.; Katayama, S.; Laukhtina, E.; Pradere, B.; Quhal, F.; Motlagh, R.S.; Mostafaei, H.; Grossmann, N.C.; Rajwa, P.; et al. Prognostic Role of Preoperative Vascular Cell Adhesion Molecule-1 Plasma Levels in Urothelial Carcinoma of the Bladder Treated With Radical Cystectomy. Ann. Surg. Oncol. 2022, 29, 5307–5316. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Jiao, D.; Yao, Z.; Wang, L.; Zhao, Z. Prognostic values of preoperative neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and lymphocyte- to-monocyte ratio for patients with muscle- invasive bladder cancer undergoing radical cystectomy. Arch. Esp. Urol. 2022, 75, 287–294. [Google Scholar]
- Schuettfort, V.M.; Pradere, B.; Trinh, Q.-D.; D’Andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Motlagh, R.S.; Rink, M.; et al. Impact of preoperative plasma levels of interleukin 6 and interleukin 6 soluble receptor on disease outcomes after radical cystectomy for bladder cancer. Cancer Immunol. Immunother. 2022, 71, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Urabe, F.; Matsuzaki, J.; Ito, K.; Takamori, H.; Tsuzuki, S.; Miki, J.; Kimura, T.; Egawa, S.; Nakamura, E.; Matsui, Y.; et al. Serum microRNA as liquid biopsy biomarker for the prediction of oncological outcomes in patients with bladder cancer. Int. J. Urol. 2022, 29, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Katayama, S.; Schuettfort, V.M.; Pradere, B.; Mori, K.; Mostafaei, H.; Quhal, F.; Motlagh, R.S.; Laukhtina, E.; Grossmann, N.C.; Aydh, A.; et al. Prognostic value of hepatocyte growth factor for muscle-invasive bladder cancer. J. Cancer Res. Clin. Oncol. 2022, 148, 3091–3102. [Google Scholar] [CrossRef]
- Inflammation and Cancer: Back to Virchow?-ScienceDirect. Available online: https://www-sciencedirect-com.ez.srv.pmu.ac.at/science/article/pii/S0140673600040460?via%3Dihub?ezproxy=true (accessed on 11 December 2022).
- Fernandes, J.V.; Cobucci, R.; Jatobá, C.A.N.; Fernandes, T.; De Azevedo, J.W.V.; De Araújo, J.M.G. The Role of the Mediators of Inflammation in Cancer Development. Pathol. Oncol. Res. POR 2015, 21, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Seah, J.-A.; Leibowitz-Amit, R.; Atenafu, E.G.; Alimohamed, N.; Knox, J.J.; Joshua, A.M.; Sridhar, S.S. Neutrophil-Lymphocyte Ratio and Pathological Response to Neoadjuvant Chemotherapy in Patients with Muscle-Invasive Bladder Cancer. Clin. Genitourin. Cancer 2015, 13, e229–e233. [Google Scholar] [CrossRef]
- Song, M.; Graubard, B.I.; Rabkin, C.S.; Engels, E.A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci. Rep. 2021, 11, 464. [Google Scholar] [CrossRef]
- Guthrie, G.J.K.; Charles, K.A.; Roxburgh, C.S.D.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil–lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Lowsby, R.; Gomes, C.; Jarman, I.; Lisboa, P.; Nee, P.A.; Vardhan, M.; Eckersley, T.; Saleh, R.; Mills, H. Neutrophil to lymphocyte count ratio as an early indicator of blood stream infection in the emergency department. Emerg. Med. J. 2015, 32, 531–534. [Google Scholar] [CrossRef] [Green Version]
- Adamstein, N.H.; MacFadyen, J.G.; Rose, L.M.; Glynn, R.J.; Dey, A.K.; Libby, P.; Tabas, I.A.; Mehta, N.N.; Ridker, P.M. The neutrophil–lymphocyte ratio and incident atherosclerotic events: Analyses from five contemporary randomized trials. Eur. Heart J. 2021, 42, 896–903. [Google Scholar] [CrossRef]
- Park, J.M. Neutrophil-to-lymphocyte ratio in trauma patients. J. Trauma Acute Care Surg. 2017, 82, 225–226. [Google Scholar] [CrossRef]
- Li, W.; Hou, M.; Ding, Z.; Liu, X.; Shao, Y.; Li, X. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 686983. [Google Scholar] [CrossRef]
- Lee, M.-J.; Park, S.-D.; Kwon, S.W.; Woo, S.-I.; Lee, M.-D.; Shin, S.-H.; Kim, D.-H.; Kwan, J.; Park, K.-S. Relation between Neutrophil-to-Lymphocyte Ratio and Index of Microcirculatory Resistance in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Am. J. Cardiol. 2016, 118, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Kalemaki, D.; Tzagkarakis, E.; Lydakis, C. Pitfalls in studies of eosinopenia and neutrophil-to-lymphocyte count ratio. Infect. Dis. 2018, 50, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Ruiter, R.; Ikram, M.A.; Voortman, T.; van Eijck, C.H.J.; Stricker, B.H. Reference values for white blood-cell-based inflammatory markers in the Rotterdam Study: A population-based prospective cohort study. Sci. Rep. 2018, 8, 10566. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author | Year | Blood-Based Biomarker | Sample Size | Study Design | Survival Outcomes |
|---|---|---|---|---|---|
| Chang et al. [27] | 2004 | CA 125 | n = 287 | retrospective single-center | RFS, OS |
| Kouba et al. [28] | 2009 | CA 125 | n = 92 | prospective single-center | recurrence |
| Hazzaa et al. [29] | 2010 | clusterin | n = 26 | prospective single-center | RFS, OS |
| Rink et al. [30] | 2012 | HER2 expression of circulating tumor cells | n = 100 | prospective single-center | OS, CSS, RFS |
| Ahmadi et al. [31] | 2014 | CA 19-9, CA 125, CEA | n = 186 | prospective single-center | OS, RFS |
| Hermanns et al. [32] | 2014 | NLR | n = 424 | retrospective single-center | OS, CSS, RFS |
| Viers et al. [33] | 2014 | NLR | n = 899 | retrospective single-center | OS, CSS, RFS |
| Djaladat et al. [34] | 2014 | albumin level, ASA score | n = 1471 | retrospective single-center | RFS, OS |
| Morizawa et al. [22] | 2016 | NLR | n = 110 | retrospective single-center | OS, CSS, RFS |
| Bhindi et al. [20] | 2016 | hemoglobin, individual cell counts, NLR, MLR, LMR, PLR | n = 418 | retrospective single-center | OS, CSS, RFS |
| Liu et al. [35] | 2016 | albumin/globulin ratio | n = 296 | retrospective multicenter | RFS, CSS |
| Tan et al. [36] | 2017 | NLR | n = 84 | retrospective single-center | OS, CSS, RFS |
| D’Andrea et al. [21] | 2017 | LMR, NLR | n = 4198 | retrospective multicenter | OS, CSS, RFS |
| Christensen et al. [37] | 2019 | circulating tumor DNA | n = 68 | prospective single-center | RFS, OS |
| Yuk et al. [38] | 2019 | De Ritis ratio | n = 771 | retrospective single-center | OS, CSS, RFS |
| Ninomiya et al. [39] | 2020 | NLR, MLR, LPR, De Ritis ratio, PNI | n = 107 | retrospective single-center | OS, RFS |
| Fallah et al. [40] | 2020 | Myeloid-derived suppressor cells | n = 109 | retrospective single-center | OS, RFS |
| Su et al. [41] | 2020 | lactate dehydrogenase | n = 263 | retrospective single-center | OS, CSS, DFS |
| Dohn et al. [42] | 2021 | uPA | n = 107 | prospective single-center | OS, CSS, RFS |
| Schuettfort et al. [43] | 2021 | albumin-globulin ratio | n = 4335 | retrospective multicenter | OS, CSS, RFS |
| Li et al. [44] | 2021 | albumin-to-alkaline phosphatase ratio | n = 199 | retrospective single-center | OS, CSS, RFS |
| Mari et al. [45] | 2021 | inflammatory biomarkers | n = 255 | retrospective single-center | recurrence, CSM, OM |
| Schuettfort et al. [46] | 2021 | uPA, SuPAR, PAI-one | n = 1036 | retrospective multicenter | RFS, CSS |
| Schuettfort et al. [47] | 2022 | panel of SIR markers | n = 4199 | retrospective multicenter | CSS, RFS |
| Grossmann et al. [48] | 2022 | systemic immune-inflammation index | n = 4335 | retrospective multicenter | OS, CSS, RFS |
| Laukhtina et al. [49] | 2022 | endoglin | n = 1036 | retrospective multicenter | OS, CSS, RFS |
| Sari Motlagh et al. [50] | 2022 | IGF-I, IGFBP-2, IGFBP-3 | n = 1036 | retrospective multicenter | OS, CSS, RFS |
| Mori et al. [51] | 2022 | VCAM-1 | n = 1036 | retrospective multicenter | OS, CSS, RFS |
| Lei et al. [52] | 2022 | NLR, PLR, LMR | n = 186 | retrospective single-center | RFS |
| Schuettfort et al. [53] | 2022 | Interleukin-6 and its soluble receptor | n = 1036 | retrospective multicenter | OS, CSS, RFS |
| Urabe et al. [54] | 2022 | Serum microRNA | n = 81 | retrospective single-center | OS, PFS |
| Katayama et al. [55] | 2022 | hepatocyte growth factor | n = 565 | retrospective multicenter | OS, CSS, RFS |
| Mori et al. [51] | 2022 | VEGF plasma levels | n = 1036 | retrospective multicenter | OS, CSS, RFS |
| Author | Year | Sample Size | Age, Years, Median (Range) | Pathological Stage | Median Follow-Up (Range) | HR, Multivariate Analysis (CI) | NLR Cut-Off | p-Value |
|---|---|---|---|---|---|---|---|---|
| Viers et al. [33] | 2014 | 899 | 69 (62–76) | T ≤ 1–T4, Nx, N0–N3 | 10.9 years (8.3–13.9) | Recurrence: HR 1.04 (1.01–1.08) | NLR > 2.7 | p = 0.02 |
| Hermanns et al. [32] | 2014 | 424 | 70.1 (60.6–76.3) | T0–T4, Ta, Tis, Nx, N0, N+ | 58.4 months (21.3–94.5) | Recurrence: HR 1.49 (1.12–2.00) | NLR ≥ 3 | p = 0.007 |
| Bhindi et al. [20] | 2016 | 418 | 70 (61–76) | T0– T4, Ta, Tis, N0, N+, Nx | 40 months (14–72) | RFS: HR 1.52 (1.17–1.98) | NLR < 2.9 | p = 0.002 |
| Morizawa et al. [22] | 2016 | 110 | 72 (65–76) | T0–T4, N+ | 37.5 months (11–65) | RFS: HR 2.6 (1.1–6.0) | NLR < 2.6 | p = 0.02 |
| D’Andrea et al. [21] | 2017 | 4198 | 67 (60–73) | T0–T4, Ta, Tis; N+ | not reported | RFS: HR 1.2 (1.1–1.3) | NLR < 2.7 | p < 0.001 |
| Tan et al. [36] | 2017 | 84 | 67 (37–82) | T1–T4, N+ | 30.1 months (3.2–161.7) | Recurrence: HR 6.999 (1.712–28.606) | NLR ≥ 2.7 | p = 0.007 |
| Mari et al. [45] | 2021 | 255 | 79 (75–83) | T1–T4, Nx, N0–N3 | Not reported | Recurrence: HR 1.13 (0.96–1.32) | NLR > 3 | p = 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofner, H.; Laukhtina, E.; Hassler, M.R.; Shariat, S.F. Blood-Based Biomarkers as Prognostic Factors of Recurrent Disease after Radical Cystectomy: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 5846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065846
Ofner H, Laukhtina E, Hassler MR, Shariat SF. Blood-Based Biomarkers as Prognostic Factors of Recurrent Disease after Radical Cystectomy: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(6):5846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065846
Chicago/Turabian StyleOfner, Heidemarie, Ekaterina Laukhtina, Melanie R. Hassler, and Shahrokh F. Shariat. 2023. "Blood-Based Biomarkers as Prognostic Factors of Recurrent Disease after Radical Cystectomy: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 6: 5846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065846