A Novel Fetal Movement Simulator for the Performance Evaluation of Vibration Sensors for Wearable Fetal Movement Monitors

 , , ,
, , ,
Abstract
:1. Introduction
2. Design of the Fetal Movement Simulator
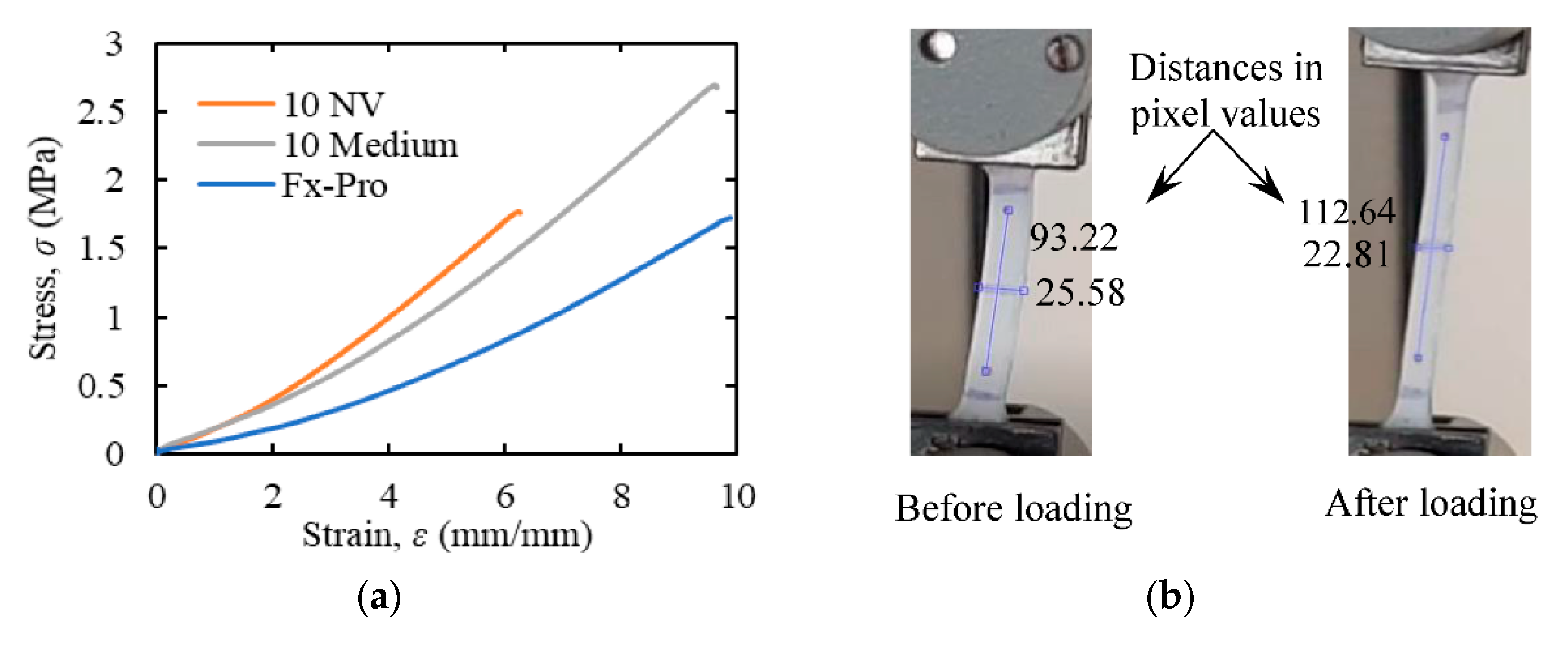
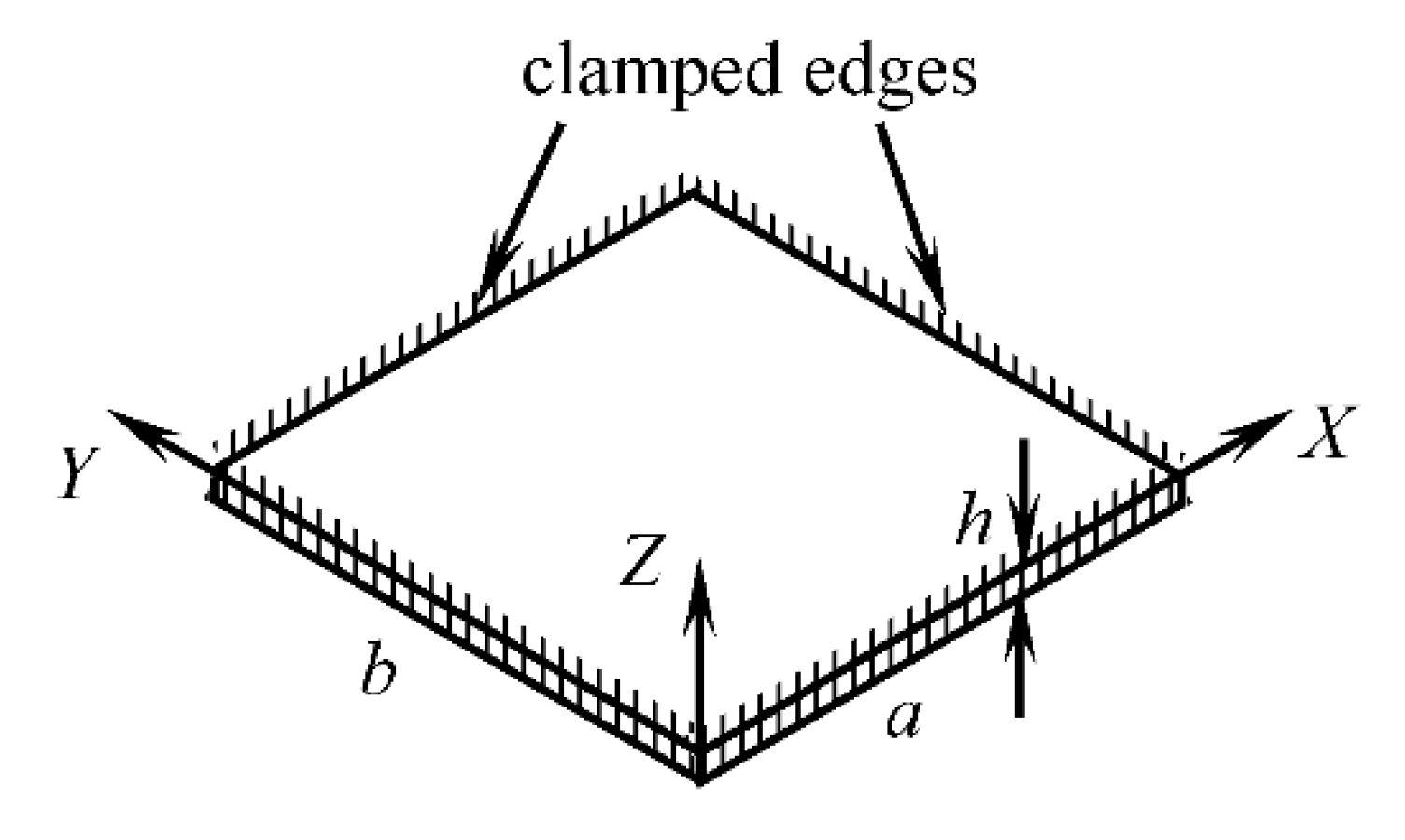
2.1. Design of the Maternal Abdomen Model
| fn = natural frequency of vibration (Hz) | flexure rigidity (Pa·m3) |
| A, B = radii of curvature (m) | E = modulus of elasticity (Pa) |
| a, b = length of sides (m) | µ = Poisson’s ratio |
| h = membrane thickness (m) | ρ = density (kg/m3) |
| fnd = natural frequency of free damped vibration (Hz) |
| ∧ = 36.112 (square membrane, 1st mode of vibration) |
| k = coefficient of damping (N·s/m). |
2.2. Design of the Support Structure and Stretching Mechanism
| normal strains along X and Y axes, respectively |
| normal stresses along X and Y axes, respectively (Pa). |
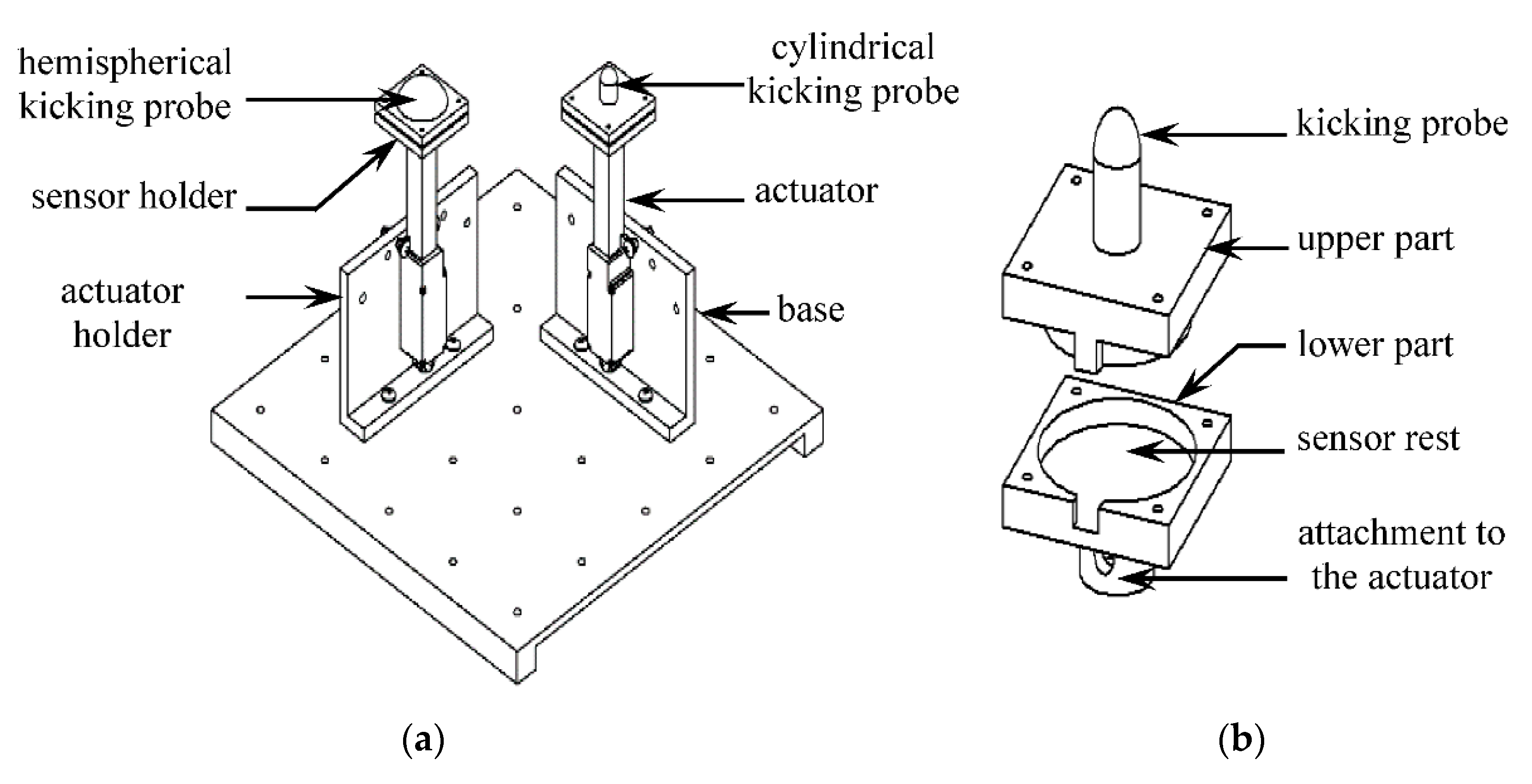
2.3. Design of the Kicking Mechanism
2.4. Data Acquisition System
2.5. Software for the Simulator
3. Characteristics of the Simulator
4. Testing of the Sensors on the Simulator
4.1. Selection of the Sensors
4.2. Processing of Sensor Data
- A noise estimate, e, was determined by taking the average of the absolute value of sensor response (Vi) for a window of time w (=2 s) during a period when no kick action was going on.where Fs is the frequency of data sampling. The time window was taken at a period sufficiently away (= 6 s) from the previous kick action to ensure the complete decay of oscillation due to the previous kick.
- The signal due to kick, S, was defined as the part of sensor response that exceeds the threshold level h = me, where m is a multiplier evaluated from trial and error:m = 5 was found to generate the most suitable threshold value for the majority of the cases, and this value was, therefore, used for all the datasets. Figure 10 demonstrates the application of this algorithm in the case of acoustic sensor response due to a simulated kick.
- The rest of the data were considered as noise N:
- Energy, E, of the signal and the noise were calculated aswhere W = S for signal and W = N for noise.
- Finally, the SNR was calculated aswhere nS and nN are the number of elements in the signal and the noise data, respectively. The noise power was assumed to be constant throughout the whole sensor response. It was, therefore, subtracted from the overall signal power to determine the power due to the kick action alone.
5. Results and Discussion
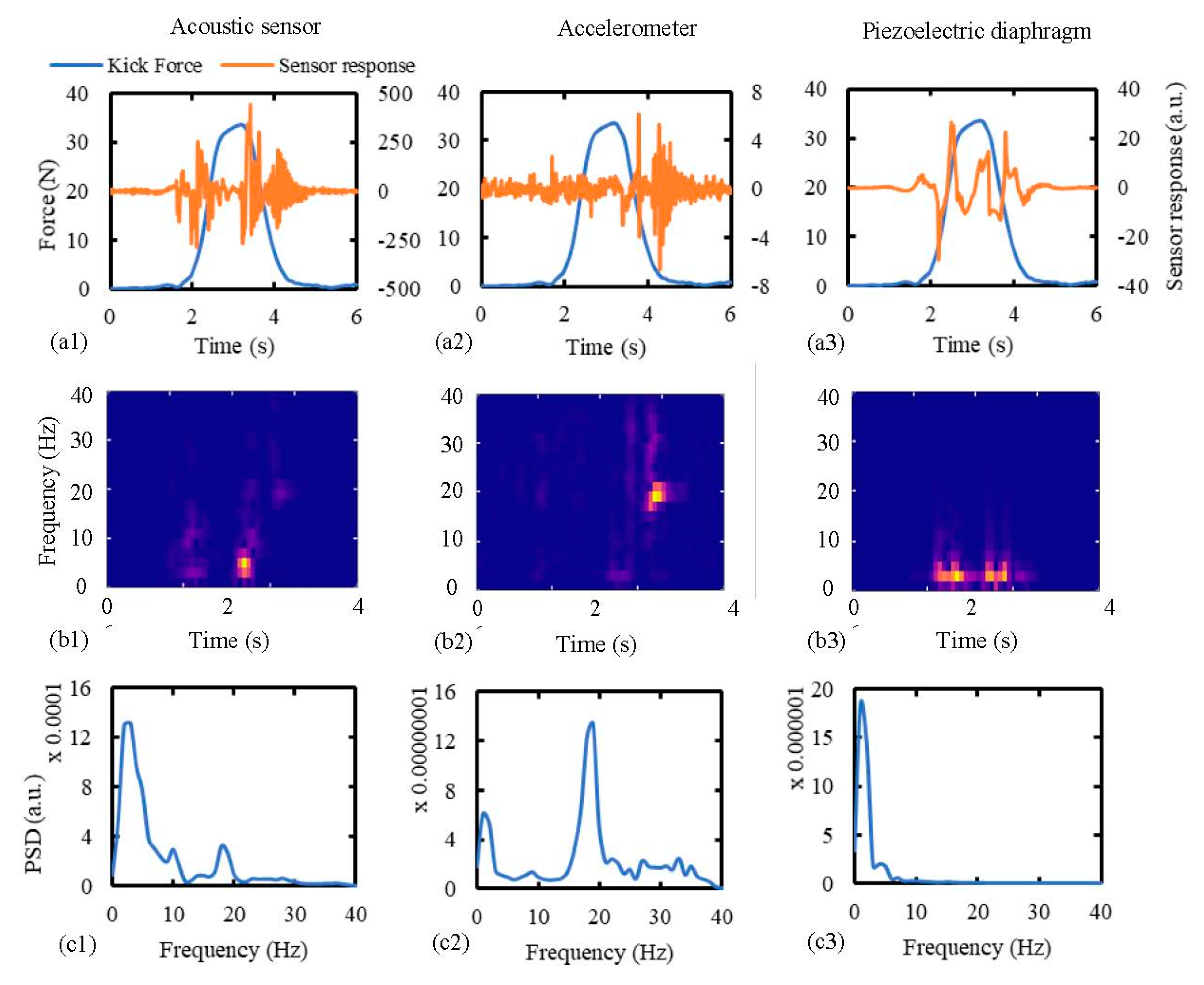
5.1. Comparative Responses from Different Sensors
5.2. Effect of Wall Displacement and Kick Distance on the Sensor Response
5.3. The Input Thresholds for the Sensors
5.4. Summary of Results
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Accessibility
References
- Olesen, A.G.; Svare, J.A. Decreased fetal movements: Background, assessment, and clinical management. Acta Obstet. Gyn. Scan. 2004, 83, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Bekedam, D.J.; Visser, G.H.A.; Devries, J.J.; Prechtl, H.F.R. Motor Behavior in the Growth Retarded Fetus. Early Hum. Dev. 1985, 12, 155–165. [Google Scholar] [CrossRef]
- Sival, D.A.; Visser, G.H.A.; Prechtl, H.F.R. The Effect of Intrauterine Growth-Retardation on the Quality of General Movements in the Human Fetus. Early Hum. Dev. 1992, 28, 119–132. [Google Scholar] [CrossRef]
- Velazquez, M.D.; Rayburn, W.F. Antenatal evaluation of the fetus using fetal movement monitoring. Clin. Obstet. Gynecol. 2002, 45, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Richardson, B.S.; Patrick, J.E.; Abduljabbar, H. Cerebral oxidative metabolism in the fetal lamb: Relationship to electrocortical state. Am. J. Obstet. Gynecol. 1985, 153, 426–431. [Google Scholar] [CrossRef]
- Richardson, B.S.; Carmichael, L.; Homan, J.; Patrick, J.E. Electrocortical activity, electroocular activity, and breathing movements in fetal sheep with prolonged and graded hypoxemia. Am. J. Obstet. Gynecol. 1992, 167, 553–558. [Google Scholar] [CrossRef]
- Pearson, J.F.; Weaver, J.B. Fetal activity and fetal wellbeing: An evaluation. Br. Med. J. 1976, 1, 1305–1307. [Google Scholar] [CrossRef] [Green Version]
- Linde, A.; Pettersson, K.; Radestad, I. Women’s Experiences of Fetal Movements before the Confirmation of Fetal DeathContractions Misinterpreted as Fetal Movement. Birth-Iss. Perinat. Care 2015, 42, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Dutton, P.J.; Warrander, L.K.; Roberts, S.A.; Bernatavicius, G.; Byrd, L.M.; Gaze, D.; Kroll, J.; Jones, R.L.; Sibley, C.P.; Froen, J.F.; et al. Predictors of poor perinatal outcome following maternal perception of reduced fetal movements--a prospective cohort study. PLoS ONE 2012, 7, e39784. [Google Scholar] [CrossRef] [Green Version]
- Efkarpidis, S.; Alexopoulos, E.; Kean, L.; Liu, D.; Fay, T. Case-control study of factors associated with intrauterine fetal deaths. MedGenMed 2004, 6, 53. [Google Scholar]
- Norman, J.E.; Heazell, A.E.P.; Rodriguez, A.; Weir, C.J.; Stock, S.J.E.; Calderwood, C.J.; Cunningham Burley, S.; Froen, J.F.; Geary, M.; Breathnach, F.; et al. Awareness of fetal movements and care package to reduce fetal mortality (AFFIRM): A stepped wedge, cluster-randomised trial. Lancet 2018, 392, 1629–1638. [Google Scholar] [CrossRef] [Green Version]
- Froen, J.F.; Heazell, A.E.P.; Tveit, J.V.H.; Saastad, E.; Fretts, R.C.; Flenady, V. Fetal movement assessment. Semin. Perinatol. 2008, 32, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Hertogs, K.; Roberts, A.B.; Cooper, D.; Griffin, D.R.; Campbell, S. Maternal perception of fetal motor activity. Br. Med. J. 1979, 2, 1183–1185. [Google Scholar] [CrossRef] [Green Version]
- Hijazi, Z.R.; Callan, S.E.; East, C.E. Maternal perception of foetal movement compared with movement detected by real-time ultrasound: An exploratory study. Aust. N. Z. J. Obstet. Gyn. 2010, 50, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Boashash, B.; Khlif, M.S.; Ben-Jabeur, T.; East, C.E.; Colditz, P.B. Passive detection of accelerometer-recorded fetal movements using a time-frequency signal processing approach. Digit. Signal. Process. 2014, 25, 134–155. [Google Scholar] [CrossRef]
- Grant, A.; Elbourne, D.; Valentin, L.; Alexander, S. Routine formal fetal movement counting and risk of antepartum late death in normally formed singletons. Lancet 1989, 2, 345–349. [Google Scholar] [CrossRef]
- National Institute for Clinical Excellence. National Collaborating Centre for Women’s and Children’s Health. Antenatal Care: Routine Care for the Healthy Pregnant Woman, 2nd ed.; Welsh, A., Ed.; RCOG Press: London, UK, 2008. [Google Scholar]
- de Vries, J.I.P.; Fong, B.F. Normal fetal motility: An overview. Ultrasound Obst. Gyn. 2006, 27, 701–711. [Google Scholar] [CrossRef]
- Andonotopo, W.; Kurjak, A. The assessment of fetal behavior of growth restricted fetuses by 4D sonography. J. Perinat. Med. 2006, 34, 471–478. [Google Scholar] [CrossRef]
- Hayat, T.T.A.; Nihat, A.; Martinez-Biarge, M.; McGuinness, A.; Allsop, J.M.; Hajnal, J.V.; Rutherford, M.A. Optimization and Initial Experience of a Multisection Balanced Steady-State Free Precession Cine Sequence for the Assessment of Fetal Behavior in Utero. Am. J. Neuroradiol. 2011, 32, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Rayburn, W.; Zuspan, F.; Motley, M.E.; Donaldson, M. An Alternative to Antepartum Fetal Heart-Rate Testing. Am. J. Obstet. Gynecol. 1980, 138, 223–226. [Google Scholar] [CrossRef]
- Thomas, G.; Mostefa, M.; Boualem, B.; Ian, C.; Stephen, W.; Miguel, F.; Susan, C.; Christine, E.; Paul, C. Detecting fetal movements using non-invasive accelerometers: A preliminary analysis. In Proceedings of the 10th International Conference on Information Science, Signal Processing and their Applications (ISSPA 2010), Kuala Lumpur, Malaysia, 10–13 May 2010; pp. 508–511. [Google Scholar]
- Ryo, E.; Nishihara, K.; Matsumoto, S.; Kamata, H. A new method for long-term home monitoring of fetal movement by pregnant women themselves. Med Eng. Phys. 2012, 34, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Mesbah, M.; Khlif, M.S.; East, C.; Smeathers, J.; Colditz, P.; Boashash, B. Accelerometer-based fetal movement detection. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 7877–7880. [Google Scholar]
- Altini, M.; Mullan, P.; Rooijakkers, M.; Gradl, S.; Penders, J.; Geusens, N.; Grieten, L.; Eskofier, B. Detection of fetal kicks using body-worn accelerometers during pregnancy: Trade-offs between sensors number and positioning. In Proceedings of the IEEE Eng Med Bio, Orlando, FL, USA, 16–20 August 2016; pp. 5319–5322. [Google Scholar]
- Lai, J.; Woodward, R.; Alexandrov, Y.; Ain Munnee, Q.; Lees, C.C.; Vaidyanathan, R.; Nowlan, N.C. Performance of a wearable acoustic system for fetal movement discrimination. PLoS ONE 2018, 13, e0195728. [Google Scholar] [CrossRef] [Green Version]
- Sazali, A.R.; Al-Ashwal, R. Fetal Movement Simulator for Fetal Monitoring System Testing. In Proceedings of the IEEE Embs Conf Bio, Sarawak, Malaysia, 3–6 December 2018; pp. 544–547. [Google Scholar]
- Palmer, P.J. The Natural Frequency of Vibration of Curved Rectangular Plates. Aeronaut. Q. 1954, 5, 101–110. [Google Scholar] [CrossRef]
- Helmig, R.; Oxlund, H.; Petersen, L.K.; Uldbjerg, N. Different Biomechanical Properties of Human Fetal Membranes Obtained before and after Delivery. Eur. J. Obstet. Gyn. Reprod. Biol. 1993, 48, 183–189. [Google Scholar] [CrossRef]
- Verbruggen, S.W.; Kainz, B.; Shelmerdine, S.C.; Hajnal, J.V.; Rutherford, M.A.; Arthurs, O.J.; Phillips, A.T.M.; Nowlan, N.C. Stresses and strains on the human fetal skeleton during development. J. R. Soc. Interface 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Verbruggen, S.W.; Loo, J.H.; Hayat, T.T.; Hajnal, J.V.; Rutherford, M.A.; Phillips, A.T.; Nowlan, N.C. Modeling the biomechanics of fetal movements. Biomech. Model. Mechanobiol. 2016, 15, 995–1004. [Google Scholar] [CrossRef] [Green Version]
- Pearsall, G.W.; Roberts, V.L. Passive Mechanical-Properties of Uterine Muscle (Myometrium) Tested Invitro. J. Biomech. 1978, 11, 167. [Google Scholar] [CrossRef]
- Acar, B.S.; van Lopik, D. Computational pregnant occupant model, ‘Expecting‘, for crash simulations. Proc. Inst. Mech. Eng. Part D J. Automob. Eng. 2009, 223, 891–902. [Google Scholar] [CrossRef] [Green Version]
- Sokolowski, P.; Saison, F.; Giles, W.; McGrath, S.; Smith, D.; Smith, J.; Smith, R. Human uterine wall tension trajectories and the onset of parturition. PLoS ONE 2010, 5, e11037. [Google Scholar] [CrossRef] [Green Version]
- Verbruggen, S.W.; Oyen, M.L.; Phillips, A.T.; Nowlan, N.C. Function and failure of the fetal membrane: Modelling the mechanics of the chorion and amnion. PLoS ONE 2017, 12, e0171588. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Alijani, A.; Frank, T.; Hanna, G.; Cuschieri, A. Elasticity of the living abdominal wall in laparoscopic surgery. J. Biomech. 2006, 39, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Schneider, U.; Pedroni, E.; Lomax, A. The calibration of CT Hounsfield units for radiotherapy treatment planning. Phys. Med. Biol. 1996, 41, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Van Hollebeke, R.B.; Cushman, M.; Schlueter, E.F.; Allison, M.A. Abdominal Muscle Density Is Inversely Related to Adiposity Inflammatory Mediators. Med. Sci. Sports Exerc. 2018, 50, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Stanišić, M.M. Free vibration of a rectangular plate with damping considered. Q. Appl. Math. 1955, 12, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Tekscan Inc. FlexiForce A401 Sensor. Available online: https://www.tekscan.com/products-solutions/force-sensors/a401 (accessed on 12 September 2020).
- SparkFun Electronics. Sparkfun Triple Axis Accelerometer Breakout-ADXL335. Available online: https://www.sparkfun.com/products/9269 (accessed on 12 September 2020).
- MMC Ltd. Piezoelectric Sound Components. Available online: https://www.sparkfun.com/products/10293 (accessed on 12 September 2020).
- Posatskiy, A.O.; Chau, T. Design and evaluation of a novel microphone-based mechanomyography sensor with cylindrical and conical acoustic chambers. Med Eng. Phys. 2012, 34, 1184–1190. [Google Scholar] [CrossRef]
- Woodward, R.B.; Shefelbine, S.J.; Vaidyanathan, R. Pervasive Monitoring of Motion and Muscle Activation: Inertial and Mechanomyography Fusion. IEEE-ASME Trans. Mechatron. 2017, 22, 2022–2033. [Google Scholar] [CrossRef]
- Actuonix Motion Devices Inc. L16-R Miniature Linear Servos for RC & Arduino. Available online: https://www.actuonix.com/L16-R-Miniature-Linear-Servo-For-RC-p/l16-r.htm (accessed on 12 September 2020).















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Material Properties, Mean (Min–Max) | Geometrical Properties, Mean (Min–Max) | |||
|---|---|---|---|---|---|
| Young’s Modulus, (kPa) | Poisson’s Ratio | Density (Kg/m3) | Thickness (mm) | Radius (mm) | |
| Fetal membrane [29,30,31] | 7100 (3200–13,700) | 0.40 | -- | 0.19 (0.14–0.28) | -- |
| Uterine wall (30 week gestational age) [30,31,32,33,34,35] | 586 | 0.40 | 1052 | 6.90 (5.0–10.50) | 99 (89–117) |
| Abdominal wall [36,37,38] | 21 (13.6–28.4) | 0.50 | 973.61 (970.13–976.75) | 31.40 (7.80–63.0) | -- |
| Total (mean) | -- | -- | -- | 38.49 (12.94–73.78) | -- |
| Weighted average | 151.37 (132–224) | 0.48 | 982.86 (980.02–985.42) | -- | -- |
| Material | Modulus of Elasticity, E100% (KPa) | Poisson’s Ratio, µ | Density, ρ (Kg/m3) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Sample 1 | Sample 2 | Sample 3 | Median | Sample 1 | Sample 2 | Sample 3 | Median | ||
| Dragon Skin FX-Pro | 81.3 | 90.9 | 148.3 | 90.9 | 0.47 | 0.51 | 0.52 | 0.51 | 1120 |
| Dragon Skin 10 NV | 207.4 | 185.5 | 189.4 | 185.5 | 0.45 | 0.49 | 0.48 | 0.48 | 1030 |
| Dragon Skin 10 Medium | 189.4 | 182.7 | 196.1 | 189.4 | 0.41 | 0.46 | 0.46 | 0.46 | 1210 |
| Property | Gestational Age (Week) | ||
|---|---|---|---|
| 20 | 25 | 30 | |
| Maximum uterine wall tensile stress, mean (range) (KPa) [34] | 11.9 (5.8–19.5) | 16.3 (9.5–24.2) | 22.8 (14.2–33.3) |
| Elongation necessary to apply the stress, mean (range) (mm) | 0.033 a (0.017–0.059) a | 0.046 a (0.017–0.059) a | 0.0639 a (0.043–0.1) a |
| Kick Mode | Description |
|---|---|
| Single | Only one actuator operates in this mode. |
| Dual: Simultaneous | Two actuators operate simultaneously in this mode. The number of kicks for both the actuators must be equal, and they will start simultaneously at the beginning of each kick. |
| Dual: Consecutive | Actuators run consecutively one after another. |
| Dual: Random | Actuators start randomly based on the respective user-defined kick profile. |
| Property | Value |
|---|---|
| Natural frequency obtained from the accelerometer, (mean ± SD) (Hz) | 18.70 ± 0.10 |
| Natural frequency obtained from the acoustic sensor, (mean ± SD) (Hz) | 18.75 ± 0.17 |
| Damping ratio, ζ | 0.80 |
| Time constant, τ (ms) | 6.40 |
| Kicking Entity | Uterine Wall Displacement, (Mean ± SD) (mm) | Kick Duration, (Mean ± SD) (s) | Kick Reaction, (Mean ± SD) (N) |
|---|---|---|---|
| 20-week old fetus [30] | 11.78 ± 4.72 | 2.65 ± 0.35 | 28.85 ± 1.88 |
| 30-week old fetus [30] | 11.52 ± 1.47 | 2.95 ± 0.74 | 46.64 ± 5.30 |
| Cylindrical probe, 10 mm diameter | 10 | 1.63 | 14.84 ± 1.76 |
| 15 | 2.45 | 33.15 ± 3.92 | |
| Hemispherical probe, 30 mm diameter | 10 | 1.69 | 26.01 ± 1.66 |
| 15 | 2.53 | 44.20 ± 2.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghosh, A.K.; Burniston, S.F.; Krentzel, D.; Roy, A.; Sheikh, A.S.; Siddiq, T.; Trinh, P.M.P.; Velazquez, M.M.; Vielle, H.-T.; Nowlan, N.C.; et al. A Novel Fetal Movement Simulator for the Performance Evaluation of Vibration Sensors for Wearable Fetal Movement Monitors. Sensors 2020, 20, 6020. https://0-doi-org.brum.beds.ac.uk/10.3390/s20216020
Ghosh AK, Burniston SF, Krentzel D, Roy A, Sheikh AS, Siddiq T, Trinh PMP, Velazquez MM, Vielle H-T, Nowlan NC, et al. A Novel Fetal Movement Simulator for the Performance Evaluation of Vibration Sensors for Wearable Fetal Movement Monitors. Sensors. 2020; 20(21):6020. https://0-doi-org.brum.beds.ac.uk/10.3390/s20216020
Chicago/Turabian StyleGhosh, Abhishek Kumar, Sonny F. Burniston, Daniel Krentzel, Abhishek Roy, Adil Shoaib Sheikh, Talha Siddiq, Paula Mai Phuong Trinh, Marta Mambrilla Velazquez, Hei-Ting Vielle, Niamh C. Nowlan, and et al. 2020. "A Novel Fetal Movement Simulator for the Performance Evaluation of Vibration Sensors for Wearable Fetal Movement Monitors" Sensors 20, no. 21: 6020. https://0-doi-org.brum.beds.ac.uk/10.3390/s20216020