Near-Infrared Spectroscopy for Monitoring Sternocleidomastoid Muscular Oxygenation during Isometric Flexion for Patients with Mild Nonspecific Neck Pain: A Pilot Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
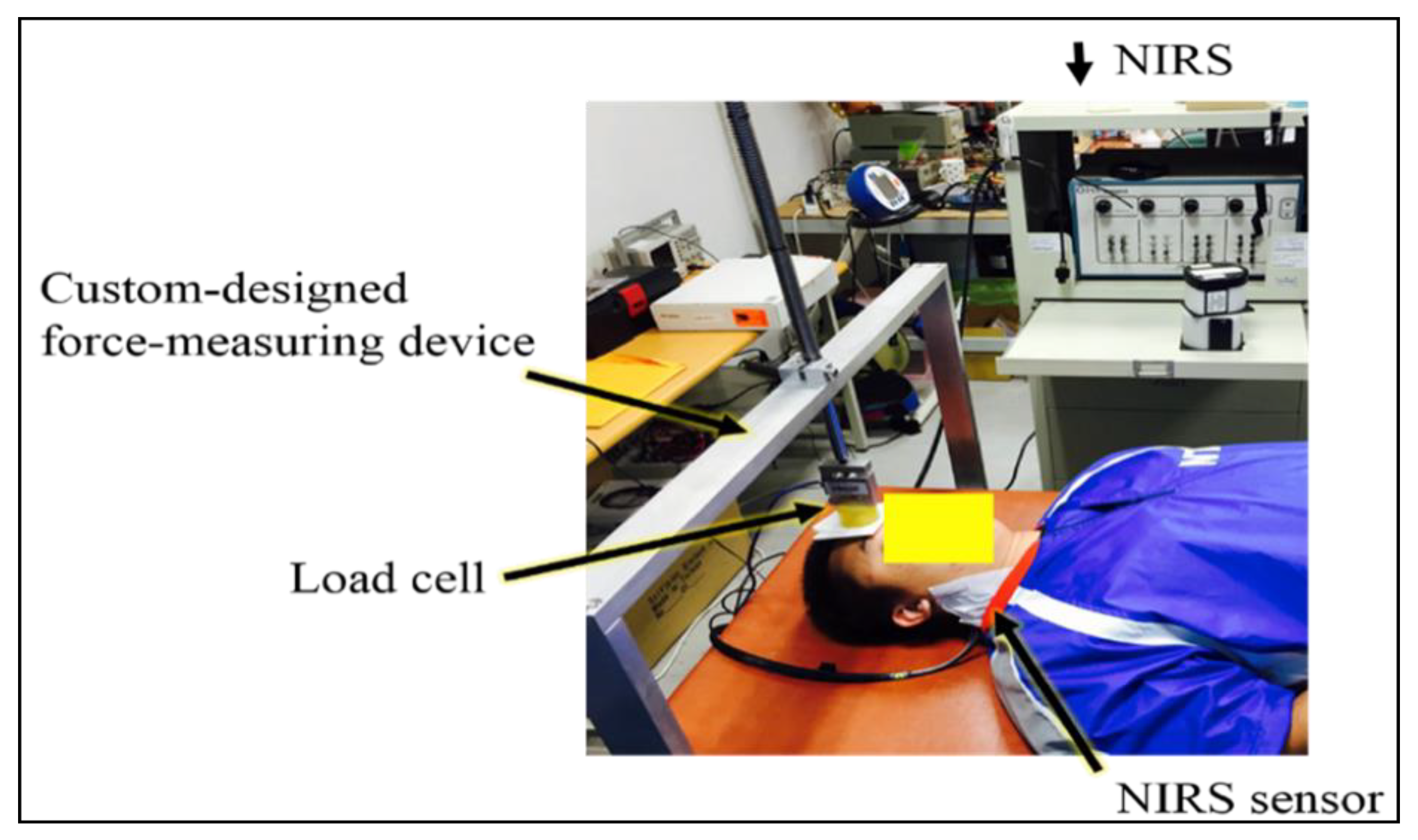
2.2. Evaluation of Muscular Oxygenation Variables Using Near-Infrared Spectroscopy
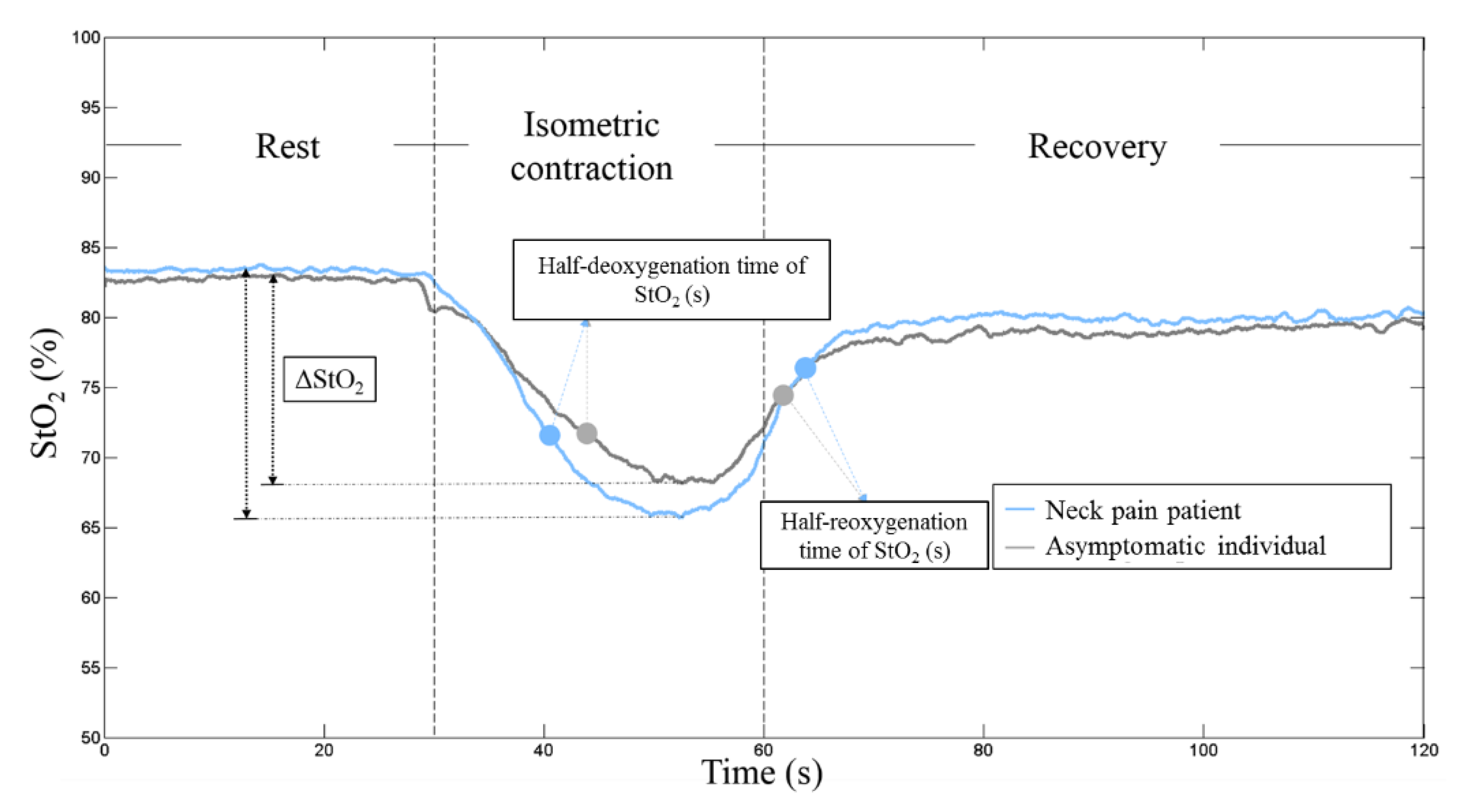
2.3. Data Analysis of the Features of Sternocleidomastoid Muscular Oxygenation
2.4. Statistical Analysis
3. Results
3.1. Muscular Oxygenation Variables of Interest
3.2. Frequency Spectrum of Muscular Oxygenation Oscillations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Childs, J.D.; Cleland, J.A.; Elliott, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitman, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W. American Physical Therapy Association. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Cote, P.; Cassidy, J.D.; Carroll, L. The Saskatchewan health and back pain survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila. PA 1976) 1998, 23, 1689–1698. [Google Scholar] [CrossRef] [PubMed]
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [Green Version]
- Picavet, H.S.; Schouten, J.S. Musculoskeletal pain in the Netherlands: Prevalences, consequences and risk groups, the DMC(3)-study. Pain 2003, 102, 167–178. [Google Scholar] [CrossRef]
- Jordan, A.; Mehlsen, J.; Ostergaard, K. A comparison of physical characteristics between patients seeking treatment for neck pain and age-matched healthy people. J. Manip. Physiol. Ther. 1997, 20, 468–475. [Google Scholar]
- Binder, A. The diagnosis and treatment of nonspecific neck pain and whiplash. Eur. Medicophys. 2007, 43, 79–89. [Google Scholar]
- Binder, A.I. Cervical spondylosis and neck pain. BMJ 2007, 334, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Ariens, G.A.; Van Mechelen, W.; Bongers, P.M.; Bouter, L.M.; Van der Wal, G. Psychosocial risk factors for neck pain: A systematic review. Am. J. Ind. Med. 2001, 39, 180–193. [Google Scholar] [CrossRef]
- Korhonen, T.; Ketola, R.; Toivonen, R.; Luukkonen, R.; Häkkänen, M.; Viikari-Juntura, E. Work related and individual predictors for incident neck pain among office employees working with video display units. Occup. Environ. Med. 2003, 60, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Palmer, K.T.; Smedley, J. Work relatedness of chronic neck pain with physical findings—A systematic review. Scand. J. Work Environ. Health 2007, 33, 165–191. [Google Scholar] [CrossRef]
- Barton, P.M.; Hayes, K.C. Neck flexor muscle strength, efficiency, and relaxation times in normal subjects and subjects with unilateral neck pain and headache. Arch. Phys. Med. Rehabil. 1996, 77, 680–687. [Google Scholar] [CrossRef]
- Petersen, S.M.; Domino, N.A.; Cook, C.E. Scapulothoracic muscle strength in individuals with neck pain. J. Back Musculoskelet. Rehabil. 2016, 29, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodhouse, A.; Vasseljen, O. Altered motor control patterns in whiplash and chronic neck pain. BMC Musculoskelet. Disord. 2008, 9, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolfsson, T.; Bjorklund, M.; Djupsjobacka, M. Range of motion in the upper and lower cervical spine in people with chronic neck pain. Man. Ther. 2012, 17, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Nicholson, L.L.; Adams, R.D. Cervical range of motion associations with subclinical neck pain. Spine (Phila. PA 1976) 2004, 29, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.Y.; Lee, S.Y.; Lin, C.F.; Yang, C.H.; Hou, Y.Y.; Wu, W.L.; Lin, H.T. Three-dimensional characteristics of neck movements in subjects with mechanical neck disorder. J. Back Musculoskelet. Rehabil. 2012, 25, 47–53. [Google Scholar] [CrossRef]
- Hagen, K.B.; Harms-Ringdahl, K.; Enger, N.O.; Hedenstad, R.; Morten, H. Relationship between subjective neck disorders and cervical spine mobility and motion-related pain in male machine operators. Spine (Phila. PA 1976) 1997, 22, 1501–1507. [Google Scholar] [CrossRef]
- Johnston, V.; Jull, G.; Souvlis, T.; Jimmieson, N.L. Neck movement and muscle activity characteristics in female office workers with neck pain. Spine (Phila. PA 1976) 2008, 33, 555–563. [Google Scholar] [CrossRef]
- Yang, C.C.; Su, F.C.; Guo, L.Y. A new concept for quantifying the complicated kinematics of the cervical spine and its application in evaluating the impairment of clients with mechanical neck disorders. Sensors (Basel) 2012, 12, 17463–17475. [Google Scholar] [CrossRef]
- Yang, C.C.; Su, F.C.; Guo, L.Y. Comparison of neck movement smoothness between patients with mechanical neck disorder and healthy volunteers using the spectral entropy method. Eur. Spine J. 2014, 23, 1743–1748. [Google Scholar] [CrossRef]
- Falla, D.; Bilenkij, G.; Jull, G. Patients with chronic neck pain demonstrate altered patterns of muscle activation during performance of a functional upper limb task. Spine (Phila. PA 1976) 2004, 29, 1436–1440. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cools, A.; Bostyn, E.; Delemarre, J.; Lemahieu, T.; Cagnie, B. Analysis of scapular muscle EMG activity in patients with idiopathic neck pain: A systematic review. J. Electromyogr. Kinesiol. 2015, 25, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Ostensvik, T.; Veiersted, K.B.; Nilsen, P. Association between numbers of long periods with sustained low-level trapezius muscle activity and neck pain. Ergonomics 2009, 52, 1556–1567. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Farina, D. Neuromuscular adaptation in experimental and clinical neck pain. J. Electromyogr. Kinesiol. 2008, 18, 255–261. [Google Scholar] [CrossRef]
- Jull, G.; Falla, D. Does increased superficial neck flexor activity in the craniocervical flexion test reflect reduced deep flexor activity in people with neck pain? Man. Ther. 2016, 25, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Falla, D.L.; Jull, G.A.; Hodges, P.W. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine (Phila. PA 1976) 2004, 29, 2108–2114. [Google Scholar] [CrossRef]
- Yip, C.H.; Chiu, T.T.; Poon, A.T. The relationship between head posture and severity and disability of patients with neck pain. Man. Ther. 2008, 13, 148–154. [Google Scholar] [CrossRef]
- Borisut, S.; Vongsirinavarat, M.; Vachalathiti, R.; Sakulsriprasert, P. Effects of strength and endurance training of superficial and deep neck muscles on muscle activities and pain levels of females with chronic neck pain. J. Phys. Ther. Sci. 2013, 25, 1157–1162. [Google Scholar] [CrossRef] [Green Version]
- Falla, D.; Rainoldi, A.; Merletti, R.; Jull, G. Myoelectric manifestations of sternocleidomastoid and anterior scalene muscle fatigue in chronic neck pain patients. Clin. Neurophysiol. 2003, 114, 488–495. [Google Scholar] [CrossRef]
- Yang, C.C.; Su, F.C.; Yang, P.C.; Lin, H.T.; Guo, L.Y. Characteristics of the motor units during sternocleidomastoid isometric flexion among patients with mechanical neck disorder and asymptomatic individuals. PLoS ONE 2016, 11, e0167737. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Jull, G.; Edwards, S.; Koh, K.; Rainoldi, A. Neuromuscular efficiency of the sternocleidomastoid and anterior scalene muscles in patients with chronic neck pain. Disabil. Rehabil. 2004, 26, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Jull, G.; Rainoldi, A.; Merletti, R. Neck flexor muscle fatigue is side specific in patients with unilateral neck pain. Eur. J. Pain 2004, 8, 71–77. [Google Scholar] [CrossRef]
- Crenshaw, A.G.; Elcadi, G.H.; Hellstrom, F.; Mathiassen, S.E. Reliability of near-infrared spectroscopy for measuring forearm and shoulder oxygenation in healthy males and females. Eur. J. Appl. Physiol. 2012, 112, 2703–2715. [Google Scholar] [CrossRef] [PubMed]
- Muthalib, M.; Millet, G.Y.; Quaresima, V.; Nosaka, K. Reliability of near-infrared spectroscopy for measuring biceps brachii oxygenation during sustained and repeated isometric contractions. J. Biomed. Opt. 2010, 15, 017008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakudo, A. Near-infrared spectroscopy for medical applications: Current status and future perspectives. Clin. Chim. Acta 2016, 455, 181–188. [Google Scholar] [CrossRef]
- Scheeren, T.W.; Schober, P.; Schwarte, L.A. Monitoring tissue oxygenation by near infrared spectroscopy (NIRS): Background and current applications. J. Clin. Monit. Comput. 2012, 26, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Vogiatzis, I.; Habazettl, H.; Louvaris, Z.; Andrianopoulos, V.; Wagner, H.; Zakynthinos, S.; Wagner, P.D. A method for assessing heterogeneity of blood flow and metabolism in exercising normal human muscle by near-infrared spectroscopy. J. Appl. Physiol. (1985) 2015, 118, 783–793. [Google Scholar] [CrossRef]
- Louvaris, Z.; Habazettl, H.; Asimakos, A.; Wagner, H.; Zakynthinos, S.; Wagner, P.D.; Vogiatzis, I. Heterogeneity of blood flow and metabolism during exercise in patients with chronic obstructive pulmonary disease. Respir. Physiol. Neurobiol. 2017, 237, 42–50. [Google Scholar] [CrossRef]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016, 21, 091313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, M.; Muthalib, M.; Quaresima, V. The use of near-infrared spectroscopy in understanding skeletal muscle physiology: Recent developments. Philos. Trans. A Math. Phys. Eng. Sci. 2011, 369, 4577–4590. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, R.; Fukuda, M.; Kawasaki, S.; Kasai, K.; Mimura, M.; Pu, S.; Noda, T.; Niwa, S.; Okazaki, Y.; Joint Project for Psychiatric Application of Near-Infrared Spectroscopy (JPSY-NIRS) Group. Neuroimaging-aided differential diagnosis of the depressive state. Neuroimage 2014, 85, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Caliandro, P.; Mirabella, M.; Padua, L.; Simbolotti, C.; Fino, C.D.; Iacovelli, C.; Sancricca, C.; Rossini, P.M. Idiopathic inflammatory myopathies evaluated by near-infrared spectroscopy. Muscle Nerve 2015, 51, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.; Dat, M.; Cooper, C.E. Underwater near-infrared spectroscopy measurements of muscle oxygenation: Laboratory validation and preliminary observations in swimmers and triathletes. J. Biomed. Opt. 2014, 19, 127002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanada, A.; Okita, K.; Yonezawa, K.; Ohtsubo, M.; Kohya, T.; Murakami, T.; Nishijima, H.; Tamura, M.; Kitabatake, A. Dissociation between muscle metabolism and oxygen kinetics during recovery from exercise in patients with chronic heart failure. Heart 2000, 83, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Larsson, B.; Søgaard, K.; Rosendal, L. Work related neck-shoulder pain: A review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract. Res. Clin. Rheumatol. 2007, 21, 447–463. [Google Scholar] [CrossRef]
- Elcadi, G.H.; Forsman, M.; Hallman, D.M.; Aasa, U.; Fahlstrom, M.; Crenshaw, A.G. Oxygenation and hemodynamics do not underlie early muscle fatigue for patients with work-related muscle pain. PLoS ONE 2014, 9, e95582. [Google Scholar] [CrossRef] [Green Version]
- Shiro, Y.; Arai, Y.C.; Matsubara, T.; Isogai, S.; Ushida, T. Effect of muscle load tasks with maximal isometric contractions on oxygenation of the trapezius muscle and sympathetic nervous activity in females with chronic neck and shoulder pain. BMC Musculoskelet. Disord. 2012, 13, 146. [Google Scholar] [CrossRef] [Green Version]
- Sjøgaard, G.; Rosendal, L.; Kristiansen, J.; Blangsted, A.K.; Skotte, J.; Larsson, B.; Gerdle, B.; Saltin, B.; Søgaard, K. Muscle oxygenation and glycolysis in females with trapezius myalgia during stress and repetitive work using microdialysis and NIRS. Eur. J. Appl. Physiol. 2010, 108, 657–669. [Google Scholar] [CrossRef]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Franceschini, M.A.; Fantini, S.; Paunescu, L.A.; Maier, J.S.; Gratton, E. Influence of a superficial layer in the quantitative spectroscopic study of strongly scattering media. Appl. Opt. 1998, 37, 7447–7458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, M.; Mottola, L.; Quaresima, V. Principles, techniques, and limitations of near infrared spectroscopy. Can. J. Appl. Physiol. 2004, 29, 463–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Zwaard, S.; Jaspers, R.T.; Blokland, I.J.; Achterberg, C.; Visser, J.M.; Den Uil, A.R.; Hofmijster, M.J.; Levels, K.; Noordhof, D.A.; De Haan, A.; et al. Oxygenation threshold derived from near-infrared spectroscopy: Reliability and its relationship with the first ventilatory threshold. PLoS ONE 2016, 11, e0162914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Beekvelt, M.C.; Borghuis, M.S.; Van Engelen, B.G.; Wevers, R.A.; Colier, W.N. Adipose tissue thickness affects in vivo quantitative near-IR spectroscopy in human skeletal muscle. Clin. Sci. Lond. Engl. 1979 2001, 101, 21–28. [Google Scholar]
- Lin, T.Y.; Lin, L.L.; Ho, T.C.; Chen, J.J. Investigating the adaptation of muscle oxygenation to resistance training for elders and young men using near-infrared spectroscopy. Eur. J. Appl. Physiol. 2014, 114, 187–196. [Google Scholar] [CrossRef]
- Jimbo, S.; Atsuta, Y.; Kobayashi, T.; Matsuno, T. Effects of dry needling at tender points for neck pain (Japanese: Katakori): Near-infrared spectroscopy for monitoring muscular oxygenation of the trapezius. J. Orthop. Sci. 2008, 13, 101–106. [Google Scholar] [CrossRef]
- Ryan, T.E.; Erickson, M.L.; Brizendine, J.T.; Young, H.J.; McCully, K.K. Noninvasive evaluation of skeletal muscle mitochondrial capacity with near-infrared spectroscopy: Correcting for blood volume changes. J. Appl. Physiol. (1985) 2012, 113, 175–183. [Google Scholar] [CrossRef]
- Kent-Braun, J.A.; Miller, R.G.; Weiner, M.W. Human skeletal muscle metabolism in health and disease: Utility of magnetic resonance spectroscopy. Exerc. Sport Sci. Rev. 1995, 23, 305–347. [Google Scholar] [CrossRef]
- Hamaoka, T.; McCully, K.K.; Niwayama, M.; Chance, B. The use of muscle near-infrared spectroscopy in sport, health and medical sciences: Recent developments. Philos. Trans. A Math. Phys. Eng. Sci. 2011, 369, 4591–4604. [Google Scholar] [CrossRef] [Green Version]
- Kell, R.T.; Bhambhani, Y. Relationship between erector spinae static endurance and muscle oxygenation-blood volume changes in healthy and low back pain subjects. Eur. J. Appl. Physiol. 2006, 96, 241–248. [Google Scholar] [CrossRef]
- Olivier, N.; Thevenon, A.; Berthoin, S.; Prieur, F. An exercise therapy program can increase oxygenation and blood volume of the erector spinae muscle during exercise in chronic low back pain patients. Arch. Phys. Med. Rehabil. 2013, 94, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Felici, F.; Quaresima, V.; Fattorini, L.; Sbriccoli, P.; Filligoi, G.C.; Ferrari, M. Biceps brachii myoelectric and oxygenation changes during static and sinusoidal isometric exercises. J. Electromyogr. Kinesiol. 2009, 19, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- Moritani, T.; Sherman, W.M.; Shibata, M.; Matsumoto, T.; Shinohara, M. Oxygen availability and motor unit activity in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1992, 64, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Coza, A.; Nigg, B.M.; Dunn, J.F. Effects of vibrations on gastrocnemius medialis tissue oxygenation. Med. Sci. Sports Exerc. 2011, 43, 509–515. [Google Scholar] [CrossRef]
- Larsson, S.E.; Zhang, Q.; Larsson, R.; Cai, H.; Oberg, P.A. Single-fibre laser Doppler flowmetry and electromyography for evaluating microcirculation in forearm muscle during static and continuous handgrip contractions. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 73, 219–224. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, M.; Chen, G.; Luo, S.; Li, J. Wavelet analysis of lumbar muscle oxygenation signals during whole-body vibration: Implications for the development of localized muscle fatigue. Eur. J. Appl. Physiol. 2012, 112, 3109–3117. [Google Scholar] [CrossRef]
- Nilsson, H.; Aalkjaer, C. Vasomotion: Mechanisms and physiological importance. Mol. Interv. 2013, 3, 79–89. [Google Scholar] [CrossRef]
- Shiogaia, Y.; Stefanovskaab, A.; McClintock, P.V.E. Nonlinear dynamics of cardiovascular ageing. Phys. Rep. 2010, 488, 51–110. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neck Pain Patients | Asymptomatic Individuals | p-Values | |
|---|---|---|---|
| Age (years) | 23.6 ± 4.2 | 24.0 ± 5.1 | 0.756 |
| Gender | 5 males, 5 females | 6 males, 4 females | 0.581 |
| Height (m) | 168.5 ± 7.5 | 165.1 ± 8.0 | 0.302 |
| Weight (kg) | 65.5 ± 15.8 | 61.5 ± 11.3 | 0.550 |
| BMI (m2/kg) | 22.9 ± 4.9 | 22.5 ± 3.7 | 0.943 |
| Skinfold thickness (mm) | 0.6 ± 0.2 | 0.5 ± 0.2 | 0.334 |
| NDI score | 9.2 ± 4.0 | 2.1 ± 0.5 | 0.008 |
| Neck Pain Patients | Asymptomatic Individuals | p-Values | |
|---|---|---|---|
| Baseline StO2 (%) | 83.57 ± 2.81 | 84.97 ± 3.22 | 0.353 |
| ΔStO2 (%) | 16.18 ± 5.58 | 15.41 ± 7.61 | 0.912 |
| Half-deoxygenation time of StO2 (s) | 10.43 ± 1.79 | 13.82 ± 1.42 | <0.001 |
| Half-reoxygenation time of StO2 (s) | 7.66 ± 2.96 | 6.20 ± 2.50 | 0.393 |
| Median frequency (Hz) | 0.35 ± 0.10 | 0.29 ± 0.17 | 0.436 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.-C.; Yang, P.-C.; Chen, J.-J.J.; Lai, Y.-H.; Hu, C.-H.; Chang, Y.; Tu, S.J.; Guo, L.-Y. Near-Infrared Spectroscopy for Monitoring Sternocleidomastoid Muscular Oxygenation during Isometric Flexion for Patients with Mild Nonspecific Neck Pain: A Pilot Study. Sensors 2020, 20, 2197. https://0-doi-org.brum.beds.ac.uk/10.3390/s20082197
Yang C-C, Yang P-C, Chen J-JJ, Lai Y-H, Hu C-H, Chang Y, Tu SJ, Guo L-Y. Near-Infrared Spectroscopy for Monitoring Sternocleidomastoid Muscular Oxygenation during Isometric Flexion for Patients with Mild Nonspecific Neck Pain: A Pilot Study. Sensors. 2020; 20(8):2197. https://0-doi-org.brum.beds.ac.uk/10.3390/s20082197
Chicago/Turabian StyleYang, Chia-Chi, Po-Ching Yang, Jia-Jin J. Chen, Yi-Horng Lai, Chia-Han Hu, Yung Chang, Shihfan Jack Tu, and Lan-Yuen Guo. 2020. "Near-Infrared Spectroscopy for Monitoring Sternocleidomastoid Muscular Oxygenation during Isometric Flexion for Patients with Mild Nonspecific Neck Pain: A Pilot Study" Sensors 20, no. 8: 2197. https://0-doi-org.brum.beds.ac.uk/10.3390/s20082197