
Design and Experimental Characterization of L-CADEL v2, an Assistive Device for Elbow Motion

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Requirements
- Comfort: User comfort can be a requirement that gives constraints that are often not considered for the functional medical purposes of a motion assistance device. The comfort in wearing and utilizing the device requires considerations not only in design and functional problems but also in man-machine interactions and the psychological effects on the user.
- Home use: The solution of a portable device that can be used at home is a problem both for the design and for the operation of a motion assistive device that must be managed directly by a user in an environment, such as the home environment, that is not designed for medical devices. Therefore, it may require particular attention both in terms of sizing and functionality, as well as interactivity with a user, also bearing in mind additional requirements on medical and environmental health and hygiene.
- Wearability: Wearability is linked both to comfort and to the possibility of home use. It is also an important aspect for user acceptance, requiring not only comfort and transportability but also aspects of interaction with the patient’s arm and the ease of application and use of the device. These problems certainly influence the design and operation of the device, also requesting specific sensors to define an optimal solution.
- Self-user operation: Autonomy in managing the device for motion assistance is a fundamental aspect for determining a device that can be managed directly by a patient, considering both learning and handling the functionality of the system, as well as its regulation and monitoring during motion exercise. This aspect also includes device quality in terms of training and ease of device management.
- Human-machine interactions: The interactions between the limb and the device determine problems and characteristics of the solution for motion assistance that can be understood, not only as requirements and constraints, but also as indications for the design and functionality of the device at adequate levels, both in terms of movements and actions between the device and the user’s limb.
- Interfaces: The interfaces that can be required for system operation are not only at the level of movement adjustment for the exercise by the user but also for motion and clinical monitoring. Interfaces that can facilitate the understanding of the device by a user and its management, such as the supervision of the system via smartphone, are desirable.
- Auto-regulation: The regulation and, therefore, the control of the functionality of the device in the exercise of motion assistance requires supervision algorithms that can be independent of the user’s reaction. Indeed, it is required that the device can have self-regulation to ensure a certain level of autonomous operation for the user’s personal safety.
- Safety: User safety is an essential aspect in these motion assistive devices, where a machine interacts with the human body. Thus, the need to ensure high-reliability levels imposes design choices and controlled functional procedures in every aspect of risk, which, however, must also be shared with risk awareness by users and medical operators.
- Motion definition: The definition of the motion characteristics in the exercise of motor assistance requires clinical medical knowledge of a patient by a medical operator and the possibility of applying this exercise adequately with the device available. The definition of motion exercise requires synergy and integration of the device’s motion skills with the physiotherapy requests that are identified by a medical operator specifically for a user-patient.
- Portability: Portability is a specific requirement of these motion assistive devices that make them very suitable to the needs of patients and to the possibility for physiotherapists to adapt motion assistance with specific patient requirements. This portability feature, however, requires considerable attention in terms of lightness in the device, as well as its easy functionality, easy adaptability to patient anatomy, and operation management by a patient himself with few elements supporting the device.
- Exercise regulation: Exercise regulation is a very important aspect of motion assistance that must be manageable both by a user and by a medical operator supervising a medical therapy. Therefore, regulation and control of the movement exercise and of the sensors that are connected to it must be accessible both for a patient and for monitoring and remote control by a medical supervisor. Therefore, both autonomy and control open to contextual and temporary needs of the patient and medical supervisor are required.
- Patient-operator interaction: A way of interacting between the patient and medical operator during the motion-assisted exercise must be provided so that they can both react to the real-time reactions to the exercise and make necessary adjustments, as well as obtain data on the achieved results.
- Medical interfaces: Medical interfaces are indispensable aids for a motion assistance device with regard to clinical and medical parameters during and in response to motion exercise. Such medical interfaces, in terms of both sensors and systems, as well as a visualization interaction, can be useful complements, and they must be integrated into the structure and functionality of the device.
- Medical monitoring: Medical monitoring can be considered indispensable not only for the supervision and evaluation of the effectiveness of the motion exercise but also for the possibility of giving timely indications to a patient-user during and in anticipation of an exercise. Medical monitoring systems can be composed of the same sensors as the medical interfaces but can also include special devices that can allow remote monitoring with video transmission.
- Safety: Aspects of safety, including medical ones, are certainly to be considered as a priority in the applications of devices for motion assistance, and from a medical point of view, they also require non-technical considerations that can continuously identify new problems and new solutions in terms of both technical and medical devices.
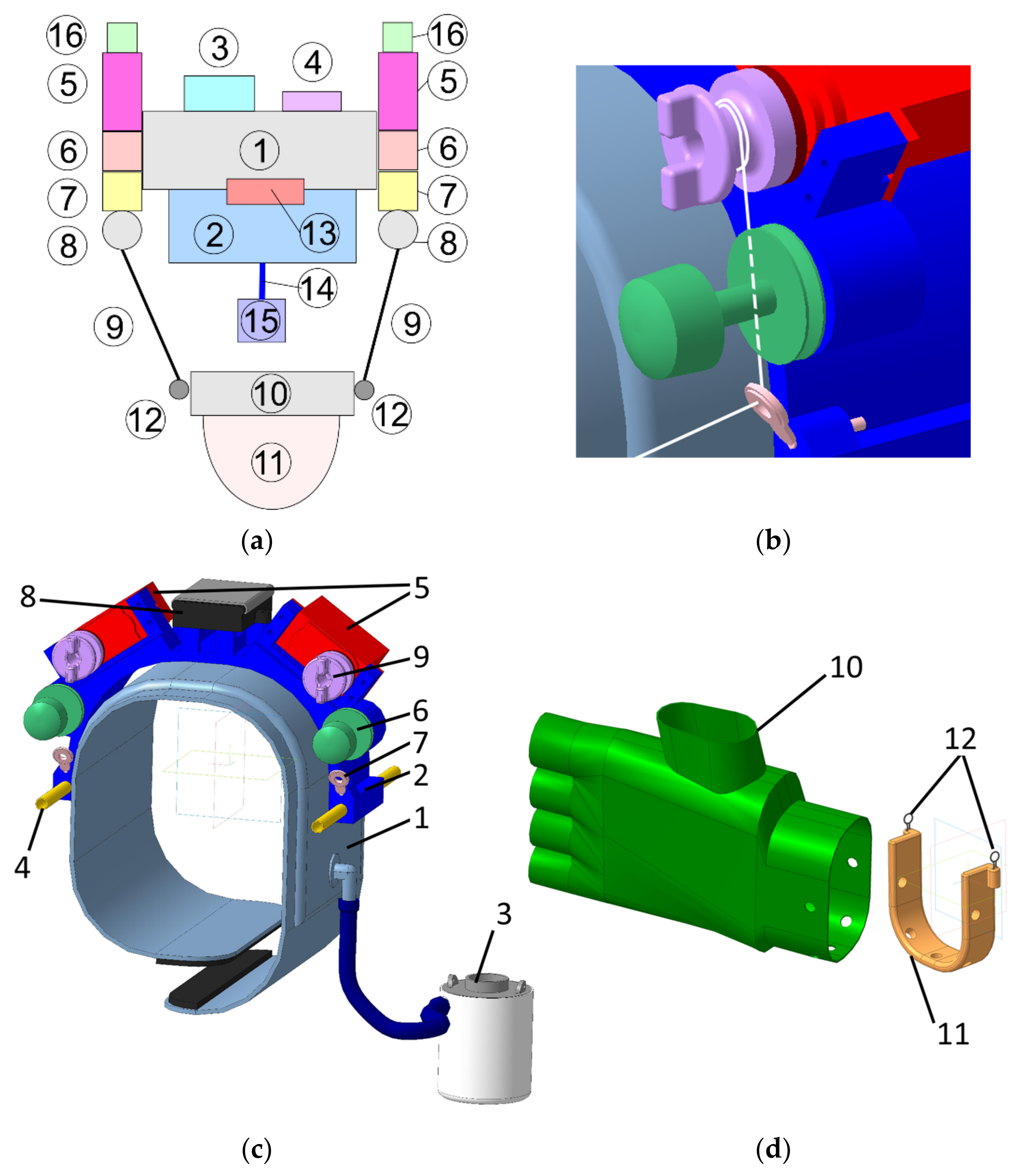
3. Conceptual Design
4. Results and Discussion
5. Conclusions
6. Patents
- Giuseppe Carbone, Marco Ceccarelli, Cable-based system for motion assistance, Patent no. IT. 102016000038975-06/11/2018, Italy.
- Marco Ceccarelli, Lucia Ferrara, Victor Petuya, Device for elbow rehabilitation, Patent no. IT. 102017000083887–29/10/2019, Italy
- Marco Ceccarelli, Matteo Russo, Device for motion assistance of ankle, n. 102020000002863, 13/02/2020, Italy, patent pending.
- Marco Ceccarelli, Matteo Bottin, Giulio Rosati, Portable cable-driven exoskeleton for elbow motion assistance, n. 102020000004885, 9/3/2020, Italy, patent pending.
- Marco Ceccarelli, Matteo Russo, Monica Urizar Arana, Mykhailo Riabtsev, Axel Fort, Mohamed Amine Laribi, Portable device for motion assistance of the elbow, n. 102021000013229, 20/5/2021, Italy, patent pending.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
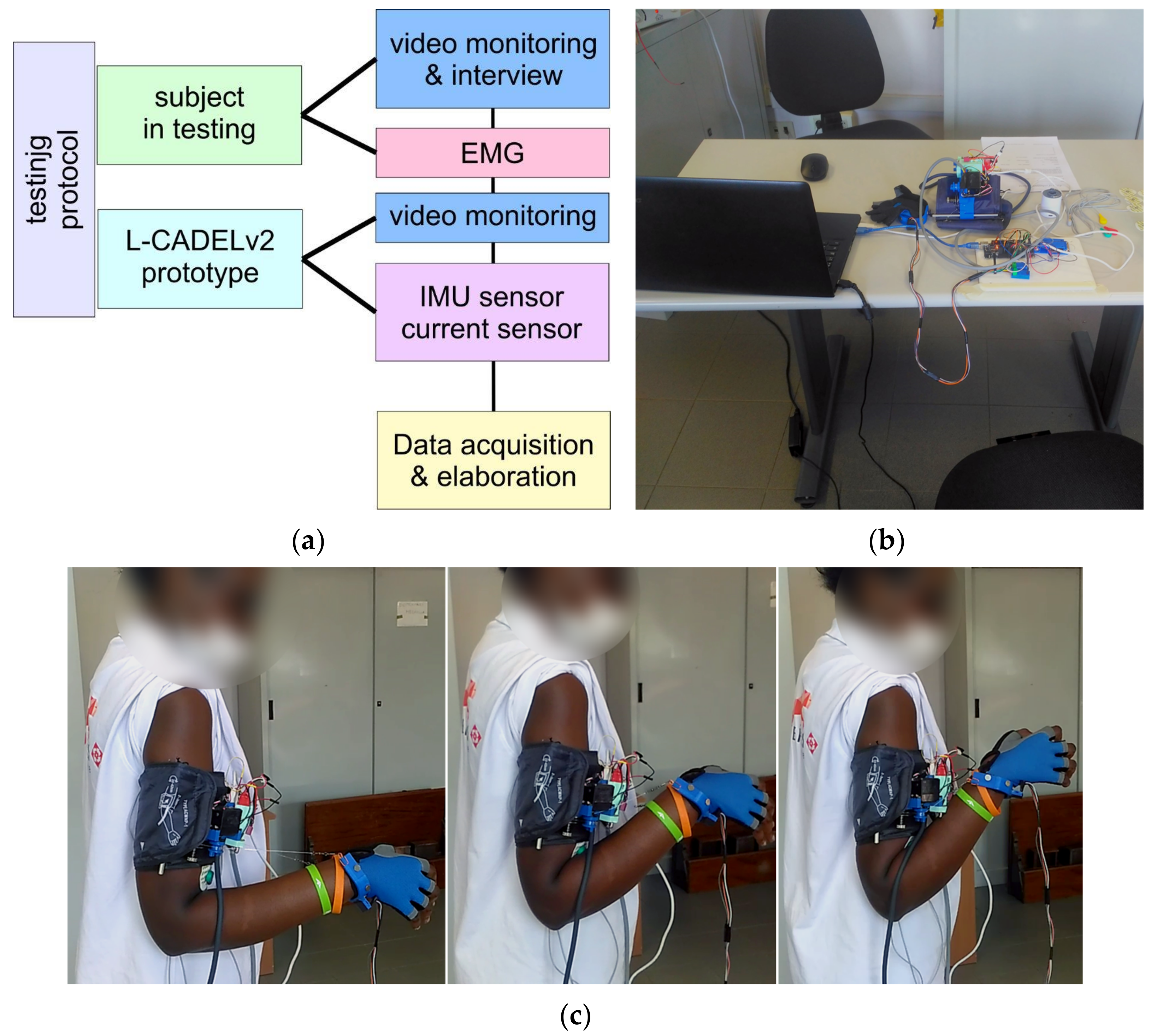
Appendix A. Protocol for Experimental Activity
- A test operator sets up the test configuration and system (with/without additional load).
- A test operator switches on the system (device, PC, data logging program).
- A test operator checks the sensors, the servomotors, and Arduino.
- A test operator informs the volunteer of the test and records the filled-in form.
- A test operator asks the volunteer to sit on a chair with a specific testing configuration.
- A test operator provides the volunteer with the alcohol solution for the skin treatment.
- A test operator asks the volunteer to wipe the skin of the shoulder with the alcohol solution.
- A test operator asks the volunteer to put the pads for the EMG sensor electrodes on his/her arm.
- A test operator asks the volunteer to connect the electrodes of the EMG sensor to the pads.
- A test operator asks the volunteer to wear the upper module.
- A test operator pumps the inflatable cuff.
- A test operator asks the volunteer to wear the lower module.
- A test operator asks the volunteer to connect the modules with the cables.
- A test operator turns on the power of the prototype.
- A test operator asks the volunteer to stand up and adjust the cables, so the angle between his/her arm and forearm will be 90°.
- A test operator asks the volunteer to adjust the cable tension so that the cables would support the weight of the forearm.
- A test operator starts collecting data.
- A test operator starts the experiment.
- A test operator finishes collecting data after three full cycles of the motions.
- A test operator switches off the system.
- A test operator asks the volunteer to take off the prototype.
- A test operator provides the volunteer with the comments questionnaire.
- A test operator undertakes post processes, and checks acquired data.
References
- Ring, D.; Jupiter, J.B. Current concepts review-fracture-dislocation of the elbow. JBJS 1998, 80, 566–580. [Google Scholar] [CrossRef]
- Ellenbecker, T.S. Rehabilitation of shoulder and elbow injuries in tennis players. Clin. Sports Med. 1995, 14, 87–110. [Google Scholar] [CrossRef]
- Wilk, K.E.; Andrews, J.R. Rehabilitation of elbow injuries. In Rehabilitation of Sports Injuries; Springer: Berlin, Germany, 2001; pp. 73–93. [Google Scholar]
- Wilk, K.E.; Arrigo, C.A. Rehabilitation of Elbow Injuries: Nonoperative and Operative. Clin. Sports Med. 2020, 39, 687–715. [Google Scholar] [CrossRef] [PubMed]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, R.M.; Van der Loos, H.M.; Lum, P.S.; Burgar, C. Robotic stroke therapy assistant. Robotica 2003, 21, 33. [Google Scholar] [CrossRef] [Green Version]
- Reinkensmeyer, D.J.; Pang, C.T.; Nessler, J.A.; Painter, C.C. Web-based telerehabilitation for the upper extremity after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 102–108. [Google Scholar] [CrossRef]
- Pang, Z.; Wang, T.; Wang, Z.; Yu, J.; Sun, Z.; Liu, S. Design and analysis of a wearable upper limb rehabilitation robot with characteristics of tension mechanism. Appl. Sci. 2020, 10, 2101. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Ceccarelli, M.; Zhang, W.; Huang, Q. Design and Performance of BIT Lexochair, a Robotic Leg-Exoskeleton Assistive Wheelchair. Int. J. Phys. Med. Rehabil. 2020, 9, 1000581. [Google Scholar]
- Cui, X.; Wang, B.; Lu, H.; Chen, J. Design and Passive Training Control of Elbow Rehabilitation Robot. Electronics 2021, 10, 1147. [Google Scholar] [CrossRef]
- Krebs, H.I.; Volpe, B.T.; Williams, D.; Celestino, J.; Charles, S.K.; Lynch, D.; Hogan, N. Robot-aided neurorehabilitation: A robot for wrist rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Beer, R.; Mayhew, D.; Bredfeldt, C.; Bachrach, B. Technical evaluation of the MACARM: A cable robot for upper limb neurorehabilitation. In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008. [Google Scholar]
- Zhang, J.; Li, X.; Liu, J.; Chen, W. Design and analysis of a compliant elbow-joint for arm rehabilitation robot. In Proceedings of the 2018 13th IEEE Conference on Industrial Electronics and Applications (ICIEA), Wuhan, China, 31 May–2 June 2018; pp. 2321–2326. [Google Scholar]
- Zhang, Q.; Sun, D.; Qian, W.; Xiao, X.; Guo, Z. Modeling and control of a cable-driven rotary series elastic actuator for an upper limb rehabilitation robot. Front. Neurorobot. 2020, 14, 13. [Google Scholar] [CrossRef]
- Rodríguez-León, J.F.; Chaparro-Rico, B.D.; Russo, M.; Cafolla, D. An Autotuning Cable-Driven Device for Home Rehabilitation. J. Healthc. Eng. 2021, 2021, 6680762. [Google Scholar] [CrossRef]
- Liu, Y.; Guo, S.; Hirata, H.; Ishihara, H.; Tamiya, T. Development of a powered variable-stiffness exoskeleton device for elbow rehabilitation. Biomed. Microdevices 2018, 20, 64. [Google Scholar] [CrossRef] [PubMed]
- Tiboni, M.; Borboni, A.; Faglia, R.; Pellegrini, N. Robotics rehabilitation of the elbow based on surface electromyography signals. Adv. Mech. Eng. 2018, 10, 1687814018754590. [Google Scholar] [CrossRef]
- Zhang, S.; Fu, Q.; Guo, S.; Fu, Y. A telepresence system for therapist-in-the-loop training for elbow joint rehabilitation. Appl. Sci. 2019, 9, 1710. [Google Scholar] [CrossRef] [Green Version]
- Copaci, D.; Martín, F.; Moreno, L.; Blanco, D. SMA based elbow exoskeleton for rehabilitation therapy and patient evaluation. IEEE Access 2019, 7, 31473–31484. [Google Scholar] [CrossRef]
- Cafolla, D.; Russo, M.; Carbone, G. Design and validation of an inherently-safe cable-driven assisting device. Int. J. Mech. Control 2018, 19, 23–32. [Google Scholar]
- Ceccarelli, M.; Romdhane, L. Design issues for human-machine platform interface in cable-based parallel manipulators for physiotherapy applications. J. Zhejiang Univ. Sci. A 2010, 11, 231–239. [Google Scholar] [CrossRef]
- Li, Z.; Chen, W.; Zhang, J.; Bai, S. Design and control of a 4-DOF cable-driven arm rehabilitation robot (CARR-4). In Proceedings of the 2017 IEEE International Conference on Cybernetics and Intelligent Systems (CIS) and IEEE Conference on Robotics, Automation and Mechatronics (RAM), Ningbo, China, 19–21 November 2017; pp. 581–586. [Google Scholar]
- Russo, M.; Ceccarelli, M. Analysis of a Wearable Robotic System for Ankle Rehabilitation. Machines 2020, 8, 48. [Google Scholar] [CrossRef]
- Ceccarelli, M.; Ferrara, L.; Petuya, V. Design of a cable-driven device for elbow rehabilitation and exercise. In Interdisciplinary Applications of Kinematics; Springer: Cham, Switzerland, 2019; pp. 61–68. [Google Scholar]
- Kozisek, A.; Ceccarelli, M.; Laribi, M.A.; Ferrara, L. Experimental Characterization of a Cable-Driven Device for Elbow Motion Assistance. In International Workshop on Medical and Service Robots; Springer: Cham, Switzerland, 2020; pp. 71–78. [Google Scholar]
- Zuccon, G.; Bottin, M.; Ceccarelli, M.; Rosati, G. Design and Performance of an Elbow Assisting Mechanism. Machines 2020, 8, 68. [Google Scholar] [CrossRef]
- Laribi, M.A.; Ceccarelli, M. Design and Experimental Characterization of a Cable-Driven Elbow Assisting Device. J. Med. Devices 2021, 15, 014503. [Google Scholar] [CrossRef]
- Ceccarelli, M. Problems and issues for service robots in new applications. Int. J. Soc. Robot. 2011, 3, 299–312. [Google Scholar] [CrossRef]
- Ceccarelli, M. Service Robots and Robotics: Design and Application; IGI Global: Pennsylvania, PA, USA, 2012. [Google Scholar]
- Rudhe, C.; Albisser, U.; Starkey, M.L.; Curt, A.; Bolliger, M. Reliability of movement workspace measurements in a passive arm orthosis used in spinal cord injury rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Kwakkel, G.; Kollen, B.J.; Krebs, H.I. Effects of robot-assisted therapy on upper limb recovery after stroke: A systematic review. Neurorehabilit. Neural Repair 2008, 22, 111–121. [Google Scholar] [CrossRef]
- Nef, T.; Mihelj, M.; Riener, R. ARMin: A robot for patient-cooperative arm therapy. Med. Biol. Eng. Comput. 2007, 45, 887–900. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Agrawal, S.K. Design of a cable-driven arm exoskeleton (CAREX) for neural rehabilitation. IEEE Trans. Robot. 2012, 28, 922–931. [Google Scholar] [CrossRef]
- Van Delden, A.L.E.Q.; Peper, C.L.E.; Kwakkel, G.; Beek, P.J. A systematic review of bilateral upper limb training devices for poststroke rehabilitation. Stroke Res. Treat. 2012, 2012, 972069. [Google Scholar] [CrossRef] [PubMed]
- Frisoli, A.; Bergamasco, M.; Carboncini, M.C.; Rossi, B. Robotic assisted rehabilitation in virtual reality with the L-EXOS. Stud Health Technol. Inf. 2009, 145, 40–54. [Google Scholar]
- Ren, Y.; Park, H.S.; Zhang, L.Q. Developing a whole-arm exoskeleton robot with hand opening and closing mechanism for upper limb stroke rehabilitation. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 761–765. [Google Scholar]
- Ball, S.J.; Brown, I.E.; Scott, S.H. MEDARM: A rehabilitation robot with 5DOF at the shoulder complex. In Proceedings of the 2007 IEEE/ASME international conference on Advanced intelligent mechatronics, Zurich, Switzerland, 4–7 September 2007; pp. 1–6. [Google Scholar]
- Carignan, C.; Tang, J.; Roderick, S. Development of an exoskeleton haptic interface for virtual task training. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MI, USA, 11–15 October 2009; pp. 3697–3702. [Google Scholar]
- Gopura, R.A.R.C.; Kiguchi, K.; Li, Y. SUEFUL-7: A 7DOF upper-limb exoskeleton robot with muscle-model-oriented EMG-based control. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MI, USA, 11–15 October 2009; pp. 1126–1131. [Google Scholar]
- Rosati, G.; Gallina, P.; Masiero, S.; Rossi, A. Design of a new 5 d.o.f. wire-based robot for rehabilitation. In Proceedings of the 2005 IEEE 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 430–433. [Google Scholar]
- Parallax Continuous Rotation Servo Datasheet. Available online: https://www.parallax.com/product/parallax-continuous-rotation-servo/ (accessed on 18 June 2021).
- Arduino Nano Datasheet. Available online: https://store.arduino.cc/arduino-nano (accessed on 18 June 2021).
- Inertial Measurement Unit GY-BMI160 Datasheet. Available online: https://www.bosch-sensortec.com/media/boschsensortec/downloads/datasheets/bst-bmi160-ds000.pdf (accessed on 26 June 2021).
- MyoWare Muscle Sensor Datasheet. Available online: https://cdn.sparkfun.com/assets/a/3/a/f/a/AT-04-001.pdf (accessed on 26 June 2021).
- Arduino Mega Datasheet. Available online: https://store.arduino.cc/arduino-mega-2560-rev3 (accessed on 18 June 2021).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Design | Joint | DoF | Actuators | Power Transmission |
|---|---|---|---|---|
| ARMin [33] | shoulder, elbow, wrist | 7 | DC Brushed Motors, Maxon series RE | cable, gear |
| CAREX [34] | shoulder, elbow | 4 | Brushless Motors, Maxon EC 45 | cable |
| EXO-7 [35] | shoulder, elbow, wrist | 7 | DC Brushed Motors, Maxon | cable |
| L-EXOS [36] | shoulder, elbow | 4 | AC Motors, VERNITRON 3730V-115 | cable, gear |
| IntelliArm [37] | shoulder, elbow, wrist, hand | 8 + (2) | Electric motors | cable, gear |
| MEDARM [38] | shoulder, elbow | 6 | Electric motors | cable, gear |
| MGA [39] | shoulder, elbow | 5 | DC Brushless Motors | gear |
| SUEFUL-7 [40] | shoulder, elbow, wrist | 7 + (1) | Harmonic Drive series RH/RHS | cable, gear |
| MariBot [41] | shoulder, elbow | 3 + (2) | Direct drive pulley-motor system | cable |
| Parameter | hU | bU | sUmax | sUmin | RU | hL | bL | sL | RL |
|---|---|---|---|---|---|---|---|---|---|
| Dimension (mm) | 99 | 144 | 50 | 30 | 50 | 60 | 60 | 20 | 20 |
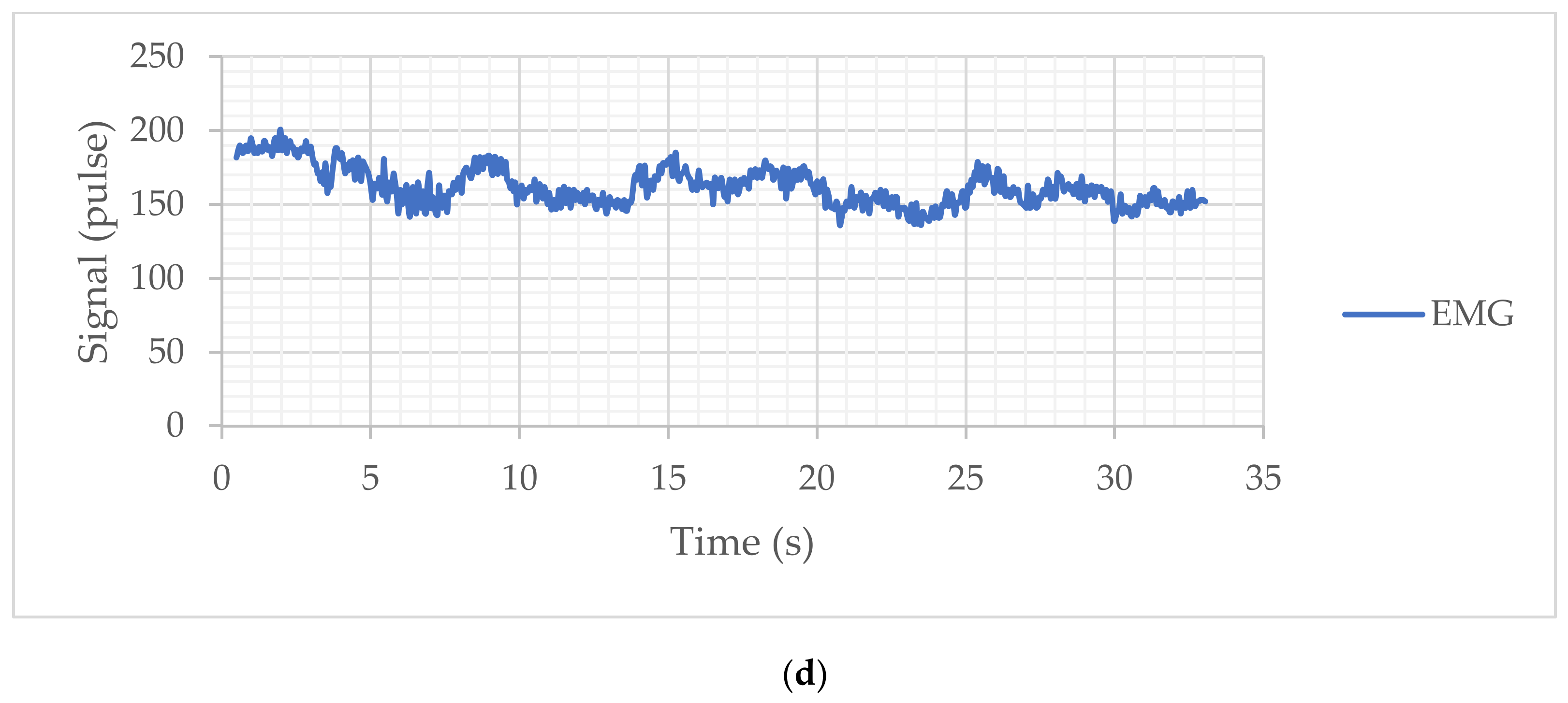
| Elbow Angle, Min–Max (deg) | Acceleration Magnitude Min–Max (m/s2) | Power Consumption (J) | EMG Response Min–Max (Pulse) | |
|---|---|---|---|---|
| Free-load | 49.19–90.79 | 0.073–0.109 | 37.68 | 67–176 |
| With load of 5N | 61.53–110.15 | 0.102–0.107 | 37.29 | 136–201 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccarelli, M.; Riabtsev, M.; Fort, A.; Russo, M.; Laribi, M.A.; Urizar, M. Design and Experimental Characterization of L-CADEL v2, an Assistive Device for Elbow Motion. Sensors 2021, 21, 5149. https://0-doi-org.brum.beds.ac.uk/10.3390/s21155149
Ceccarelli M, Riabtsev M, Fort A, Russo M, Laribi MA, Urizar M. Design and Experimental Characterization of L-CADEL v2, an Assistive Device for Elbow Motion. Sensors. 2021; 21(15):5149. https://0-doi-org.brum.beds.ac.uk/10.3390/s21155149
Chicago/Turabian StyleCeccarelli, Marco, Mykhailo Riabtsev, Axel Fort, Matteo Russo, Med Amine Laribi, and Monica Urizar. 2021. "Design and Experimental Characterization of L-CADEL v2, an Assistive Device for Elbow Motion" Sensors 21, no. 15: 5149. https://0-doi-org.brum.beds.ac.uk/10.3390/s21155149