
Kinetic Sensors for Ligament Balance and Kinematic Evaluation in Anatomic Bi-Cruciate Stabilized Total Knee Arthroplasty

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
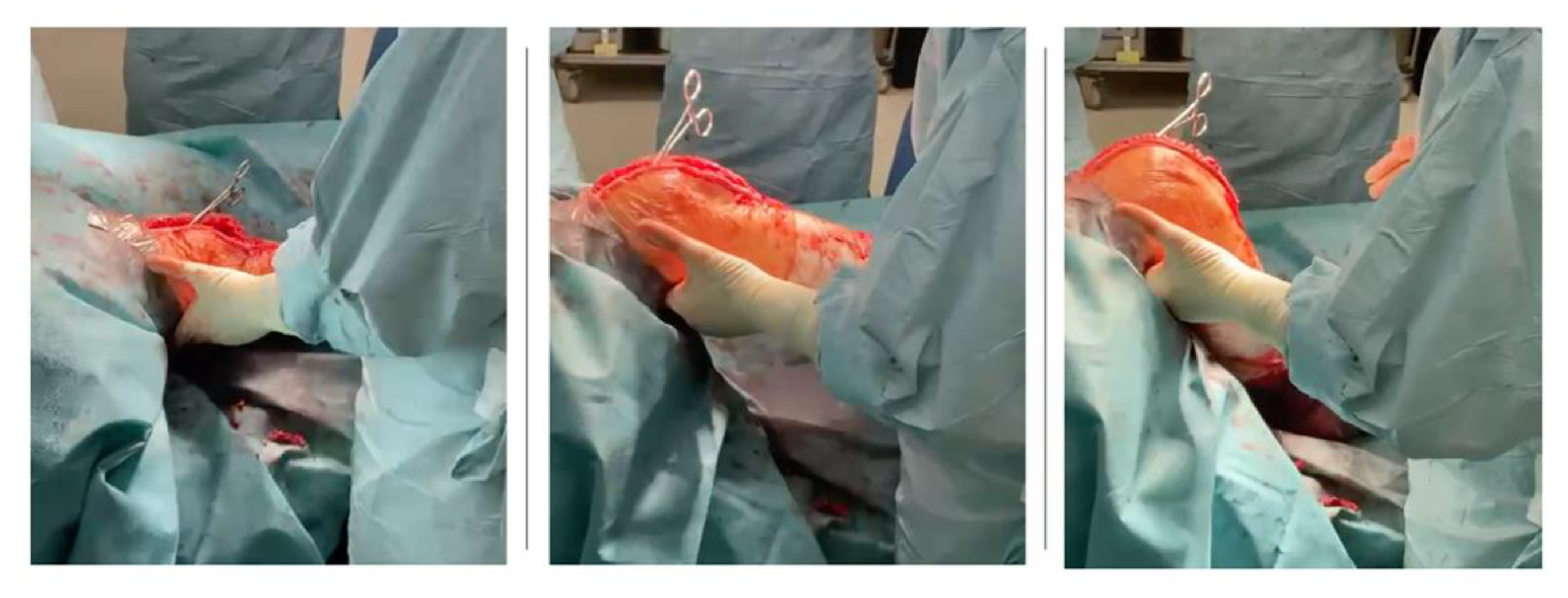
2.1. Surgical Technique
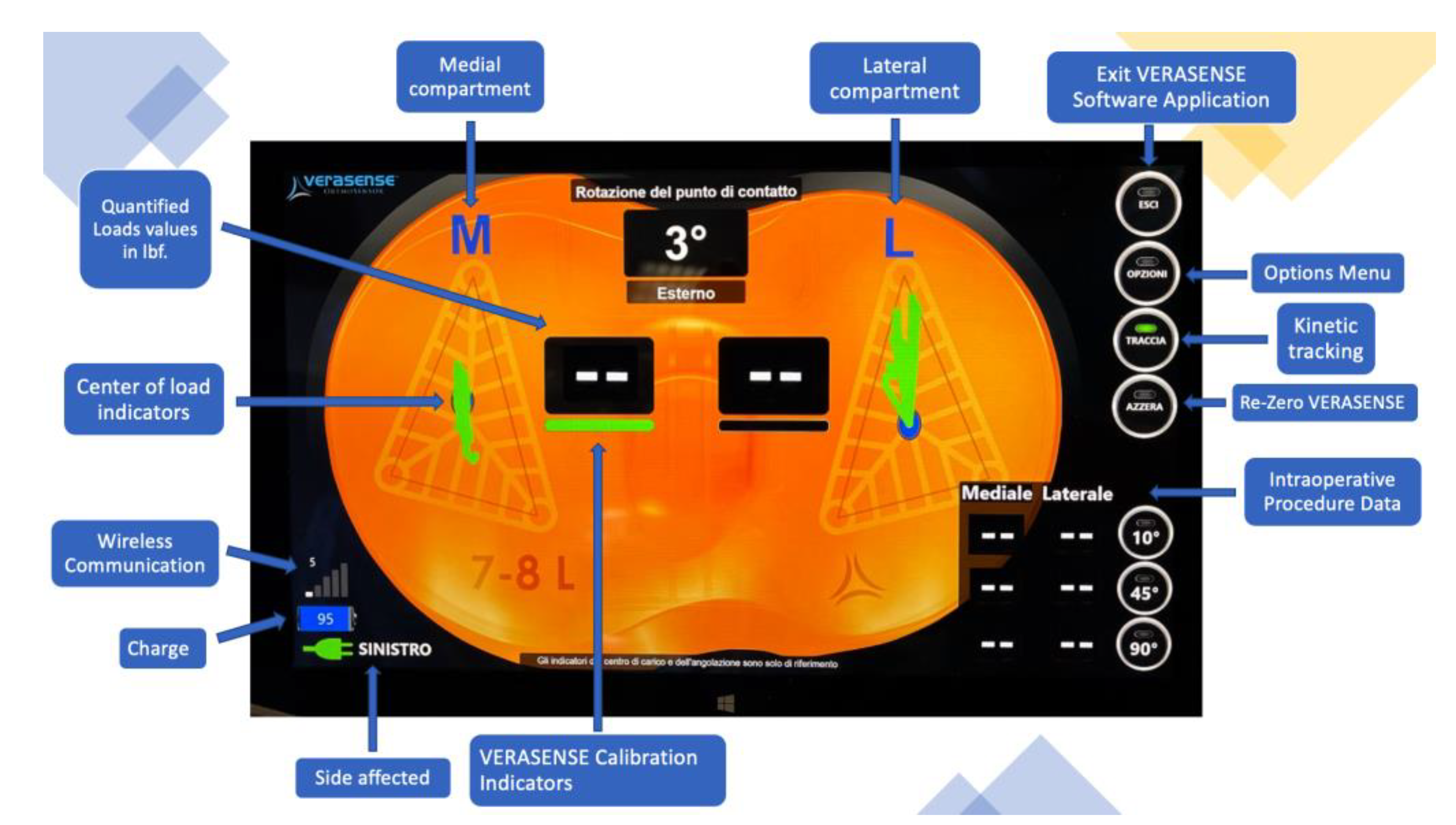
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
Epidemiological and Radiological Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamilton, D.F.; Howie, C.R.; Burnett, R.; Simpson, A.H.R.W.; Patton, J.T. Dealing with the predicted increase in demand for revision total knee arthroplasty: Challenges, risks and opportunities. Bone Jt. J. 2015, 97, 723–728. [Google Scholar] [CrossRef]
- Nemes, S.; Rolfson, O.; W-Dahl, A.; Garellick, G.; Sundberg, M.; Kärrholm, J.; Robertsson, O. Historical view and future demand for knee arthroplasty in Sweden. Acta Orthop. 2015, 86, 426–431. [Google Scholar] [CrossRef] [Green Version]
- Mulhall, K.J.; Ghomrawi, H.M.; Scully, S.; Callaghan, J.J.; Saleh, K.J. Current etiologies and modes of failure in total knee arthroplasty revision. Clin. Orthop. Relat. Res. 2006, 446, 45–50. [Google Scholar] [CrossRef]
- Matziolis, G.; Pfiel, S.; Wassilew, G.; Boenicke, H.; Perka, C. Kinematic analysis of the flexion axis for correct femoral component placement. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1504–1509. [Google Scholar] [CrossRef]
- Postler, A.; Lützner, C.; Beyer, F.; Tille, E.; Lützner, J. Analysis of Total Knee Arthroplasty revision causes. BMC Musculoskelet. Disord. 2018, 19, 55. [Google Scholar] [CrossRef] [Green Version]
- Vince, K. Mid-flexion instability after total knee arthroplasty: Woolly thinking or a real concern? Bone Jt. J. 2016, 98, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Tsukiyama, H.; Kuriyama, S.; Kobayashi, M.; Nakamura, S.; Furu, M.; Ito, H.; Matsuda, S. Medial rather than lateral knee instability correlates with inferior patient satisfaction and knee function after total knee arthroplasty. Knee 2017, 24, 1478–1484. [Google Scholar] [CrossRef]
- Azukizawa, M.; Kuriyama, S.; Nakamura, S.; Nishitani, K.; Lyman, S.; Morita, Y.; Furu, M.; Ito, H.; Matsuda, S. Intraoperative medial joint laxity in flexion decreases patient satisfaction after total knee arthroplasty. Arch. Orthop. Trauma Surg. 2018, 138, 1143–1150. [Google Scholar] [CrossRef]
- Dennis, D.A.; Komistek, R.D.; Mahfouz, M.R.; Haas, B.D.; Stiehl, J.B. Multicenter determination of in vivo kinematics after total knee arthroplasty. Clin. Orthop. Relat. Res. 2003, 416, 37–57. [Google Scholar] [CrossRef] [Green Version]
- Harwin, S.F.; Banerjee, S.; Issa, K.; Mont, M.A. Advances in total knee arthroplasty. J. Knee Surg. 2014, 27, 169–170. [Google Scholar] [CrossRef]
- Asano, H.; Hoshino, A.; Wilton, T.J. Soft-tissue tension total knee arthroplasty. J. Arthroplast. 2004, 19, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Ghirardelli, S.; Bala, A.; Peretti, G.; Antonini, G.; Indelli, P.F. Intraoperative Sensing Technology to Achieve Balance in Primary Total Knee Arthroplasty: A Review of the Literature. JBJS Rev. 2019, 7, 1–6. [Google Scholar] [CrossRef]
- Cho, K.J.; Seon, J.K.; Jang, W.Y.; Park, C.G.; Song, E.K. Objective quantification of ligament balancing using VERASENSE in measured resection and modified gap balance total knee arthroplasty. BMC Musculoskelet. Disord. 2018, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustke, K.A.; Golladay, G.J.; Roche, M.W.; Elson, L.C.; Anderson, C.R. A Targeted Approach to Ligament Balancing Using Kinetic Sensors. J. Arthroplast. 2017, 32, 2127–2132. [Google Scholar] [CrossRef]
- Gustke, K.A.; Golladay, G.J.; Roche, M.W.; Elson, L.C.; Anderson, C.R. A new method for defining balance: Promising Short-Term Clinical Outcomes of Sensor-Guided TKA. J. Arthroplast. 2014, 29, 955–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, P.S.; Meere, P.A.; Bell, C.P. Effects of surgical variables in balancing of total knee replacements using an instrumented tibial trial. Knee 2014, 21, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Bellemans, J.; Colyn, W.; Vandenneucker, H.; Victor, J. Is Neutral Mechanical Alignment Normal for All Patients? The Concept of Constitutional Varus. Clin. Orthop. Relat. Res. 2012, 470, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Liu, G.; Han, B.; Wang, Z.; Yan, Y.; Ma, J.; Wei, P. Knee Joint Biomechanics in Physiological Conditions and How Pathologies Can Affect It: A Systematic Review. Appl. Bionics Biomech. 2020, 2020, 7451683. [Google Scholar] [CrossRef] [PubMed]
- Stambough, J.B.; Edwards, P.K.; Mannen, E.M.; Barnes, C.L.; Mears, S.C. Flexion Instability After Total Knee Arthroplasty. J. Am. Acad. Orthop. Surg. 2019, 27, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Kia, M.; Wright, T.M.; Cross, M.B.; Mayman, D.J.; Pearle, A.D.; Sculco, P.K.; Westrich, G.H.; Imhauser, C.W. Femoral Component External Rotation Affects Knee Biomechanics: A Computational Model of Posterior-stabilized TKA. Clin. Orthop. Relat. Res. 2018, 476, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Risitano, S.; Indelli, P.F. Is “symmetric” gap balancing still the gold standard in primary total knee arthroplasty? Ann. Transl. Med. 2017, 5, 325. [Google Scholar] [CrossRef] [Green Version]
- Indelli, P.F.; Morello, F.; Ghirardelli, S.; Fidanza, A.; Iannotti, F.; Ferrini, A. No clinical differences at the 2-year follow-up between single radius and J-curve medial pivot total knee arthroplasty in the treatment of neutral or varus knees. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3949–3954. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, L.; Risitano, S.; Parisi, G.; Tosto, F.; Indelli, P.F.; Atzori, F.; Massè, A. Medial pivot in total knee arthroplasty: Literature review and our first experience. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2018, 11. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Cai, H.; Zhang, K. Pie-crusting technique is effective and safe to release superficial medial collateral ligament for total knee arthroplasty. J. Orthop. Transl. 2018, 13, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Wood, T.J.; Winemaker, M.J.; Williams, D.S.; Petruccelli, D.T.; Tushinski, D.M.; de Beer, J.d.V. Randomized Controlled Trial of Sensor-Guided Knee Balancing Compared to Standard Balancing Technique in Total Knee Arthroplasty. J. Arthroplast. 2021, 36, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Golladay, G.J.; Bradbury, T.L.; Gordon, A.C.; Fernandez-Madrid, I.J.; Krebs, V.E.; Patel, P.D.; Suarez, J.C.; Higuera Rueda, C.A.; Barsoum, W.K. Are Patients More Satisfied with a Balanced Total Knee Arthroplasty? J. Arthroplast. 2019, 34, S195–S200. [Google Scholar] [CrossRef] [PubMed]
- Walker, L.C.; Clement, N.D.; Ghosh, K.M.; Deehan, D.J. What is a balanced knee replacement? EFORT Open Rev. 2018, 3, 614–619. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Instability following total knee arthroplasty. HSS J. 2011, 7, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.J.; Lim, H.; Lee, N.R.; Moon, Y.-W. Diagnosis, causes and treatments of instability following total knee arthroplasty. Knee Surg. Relat. Res. 2014, 26, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Park, C.H.; Song, S.J. Sensor-assisted total knee arthroplasty: A narrative review. CiOS Clin. Orthop. Surg. 2021, 13, 1–9. [Google Scholar] [CrossRef]
- Bellemans, J.; D’Hooghe, P.; Vandenneucker, H.; Damme, G. Van; Victor, J. Soft tissue balance in total knee arthroplasty: Does stress relaxation occur perioperatively? Clin. Orthop. Relat. Res. 2006, 49–52. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Age | Side Affected | BMI | HKA | JLCA | Balancing Procedure Performed | Type of Balancing Procedure Performed | |
|---|---|---|---|---|---|---|---|---|---|
| Soft tissues | Bone cuts | ||||||||
| 1 | F | 79 | R | 23.56 | +12 | 5 | YES | YES | YES |
| 2 | F | 77 | R | 23.88 | 0 | 1 | NO | NO | NO |
| 3 | F | 82 | L | 23.88 | +2 | 1 | NO | NO | NO |
| 4 | M | 72 | L | 24.76 | +2 | 1 | NO | NO | NO |
| 5 | F | 88 | R | 24.89 | 0 | 4 | YES | YES | YES |
| 6 | F | 86 | R | 25.39 | −1 | 1 | NO | YES | NO |
| 7 | F | 77 | L | 25.89 | +4 | 3 | YES | NO | YES |
| 8 | F | 72 | L | 26.04 | −2 | 1 | NO | NO | NO |
| 9 | F | 82 | R | 26.67 | −1 | 1 | NO | NO | NO |
| 10 | M | 68 | L | 27.76 | +10 | 2 | YES | NO | YES |
| 11 | M | 80 | R | 28.04 | +9 | 1 | NO | NO | NO |
| 12 | M | 77 | R | 28.3 | +1 | 0 | NO | NO | NO |
| 13 | F | 76 | R | 28.89 | +9 | 0 | NO | NO | NO |
| 14 | F | 70 | R | 29.09 | +7 | 3 | NO | NO | NO |
| 15 | F | 76 | L | 29.41 | +11 | 2 | NO | NO | NO |
| 16 | F | 86 | R | 30.1 | +10 | 2 | YES | NO | YES |
| 17 | M | 75 | L | 30.45 | +11 | 4 | YES | YES | YES |
| 18 | F | 76 | R | 30.86 | −2 | 1 | YES | YES | YES |
| 19 | F | 70 | L | 31.14 | +13 | 1 | YES | YES | NO |
| 20 | F | 72 | L | 31.56 | +15 | 1 | NO | NO | NO |
| 21 | F | 77 | R | 32.87 | +8 | 1 | NO | NO | NO |
| Prognostic Factors | Values | N° | % | Balance Procedure Performed | Balance Procedure not Performed | χ2 | OR | p Value |
|---|---|---|---|---|---|---|---|---|
| Sex | F | 16 | 76.19% | 6 | 10 | |||
| M | 5 | 23.81% | 2 | 3 | 0.01 | 1.11 | 0.920 | |
| Age | <75 y.o. | 7 | 33.33% | 3 | 4 | |||
| ≥75 y.o. | 14 | 66.67% | 5 | 9 | 0.10 | 0.74 | 0.751 | |
| BMI | <30 | 15 | 71.43% | 4 | 11 | |||
| ≥30 | 6 | 28.57% | 4 | 2 | 2.91 | 5.5 | 0.088 | |
| HKA | <+10 degrees | 14 | 66.67% | 3 | 11 | |||
| ≥+10 degrees | 7 | 33.33% | 5 | 2 | 4.95 | 9.17 | 0.026 | |
| JLCA | <2 degrees | 13 | 61.90% | 2 | 11 | |||
| ≥2 degrees | 8 | 38.09% | 6 | 2 | 7.46 | 16.50 | 0.006 | |
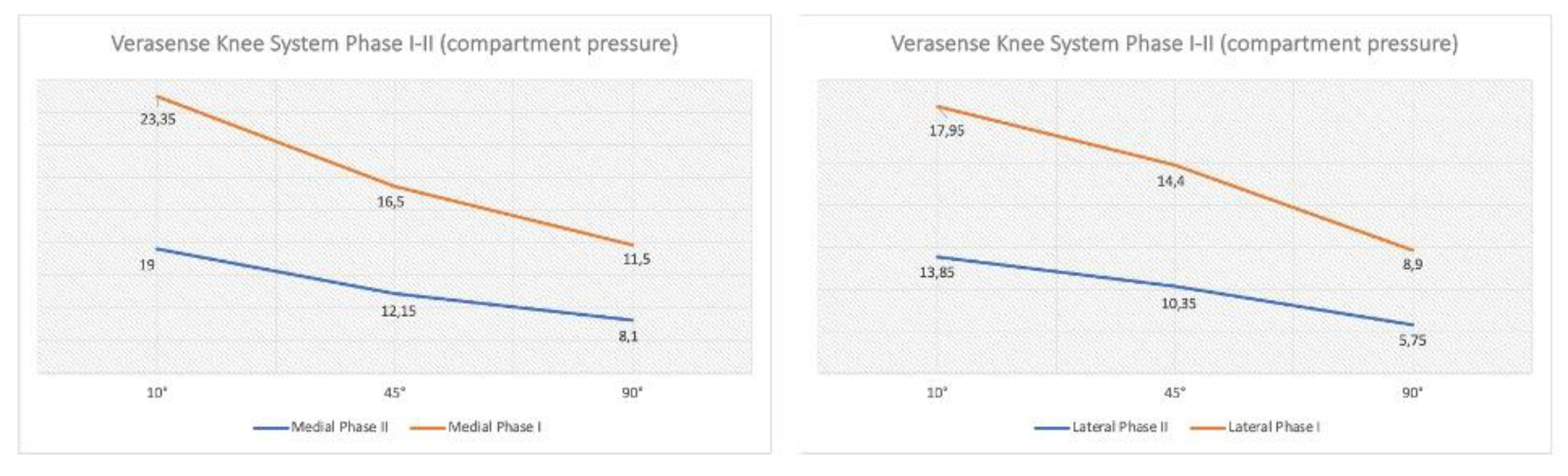
| Phase I | Phase II | p-Value | |
|---|---|---|---|
| Medial compartment | |||
| 10° | 24.38 ± 14.50 | 19.57 ± 7.81 | 0.188 |
| 45° | 17.43 ± 10.97 | 12.67 ± 5.91 | 0.088 |
| 90° | 12.05 ± 9.31 | 8.19 ± 4.73 | 0.098 |
| Lateral compartment | |||
| 10° | 18.10 ± 6.69 | 14.05 ± 5.41 | 0.037 |
| 45° | 14.33 ± 6.26 | 10.29 ± 3.44 | 0.013 |
| 90° | 8.86 ± 4.33 | 5.57 ± 3.50 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabatini, L.; Bosco, F.; Barberis, L.; Camazzola, D.; Bistolfi, A.; Risitano, S.; Massè, A.; Indelli, P.F. Kinetic Sensors for Ligament Balance and Kinematic Evaluation in Anatomic Bi-Cruciate Stabilized Total Knee Arthroplasty. Sensors 2021, 21, 5427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165427
Sabatini L, Bosco F, Barberis L, Camazzola D, Bistolfi A, Risitano S, Massè A, Indelli PF. Kinetic Sensors for Ligament Balance and Kinematic Evaluation in Anatomic Bi-Cruciate Stabilized Total Knee Arthroplasty. Sensors. 2021; 21(16):5427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165427
Chicago/Turabian StyleSabatini, Luigi, Francesco Bosco, Luca Barberis, Daniele Camazzola, Alessandro Bistolfi, Salvatore Risitano, Alessandro Massè, and Pier Francesco Indelli. 2021. "Kinetic Sensors for Ligament Balance and Kinematic Evaluation in Anatomic Bi-Cruciate Stabilized Total Knee Arthroplasty" Sensors 21, no. 16: 5427. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165427