
A Comparative Evaluation of Inertial Sensors for Gait and Jump Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Tested Wearable Sensors
2.1. XSENS “MTw Awinda”
- Accelerometer range m/s2;
- Gyroscope range degree/s.
2.2. Letsense “WIVA”
- Battery: V;
- Autonomy: 12–14 h;
- Communication interface: Bluetooth 4 Low Energy;
- Dimensions: mm;
- Weight: 50 g;
- Frequency: up to 1000 Hz;
- Output frequency: 100 Hz;
- Usage temperature: 0 C to 60 C;
- Accelerometer sensitivity: m/s2;
- Gyroscope sensitivity: 300 degree/s.
2.3. BTS “G-Walk”
- Accelerometer range , , , m/s2;
- Gyroscope range , , degree/s.
3. Tests in Physical Medicine and Rehabilitation
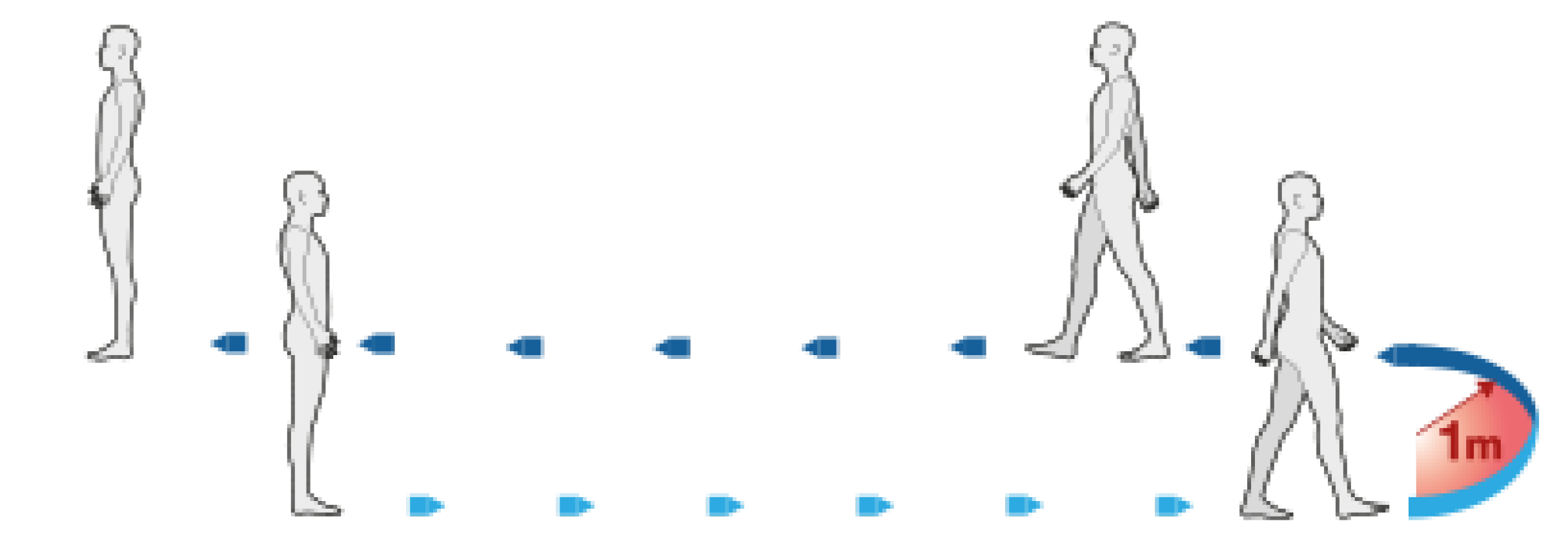
3.1. The 10 m Walk Test
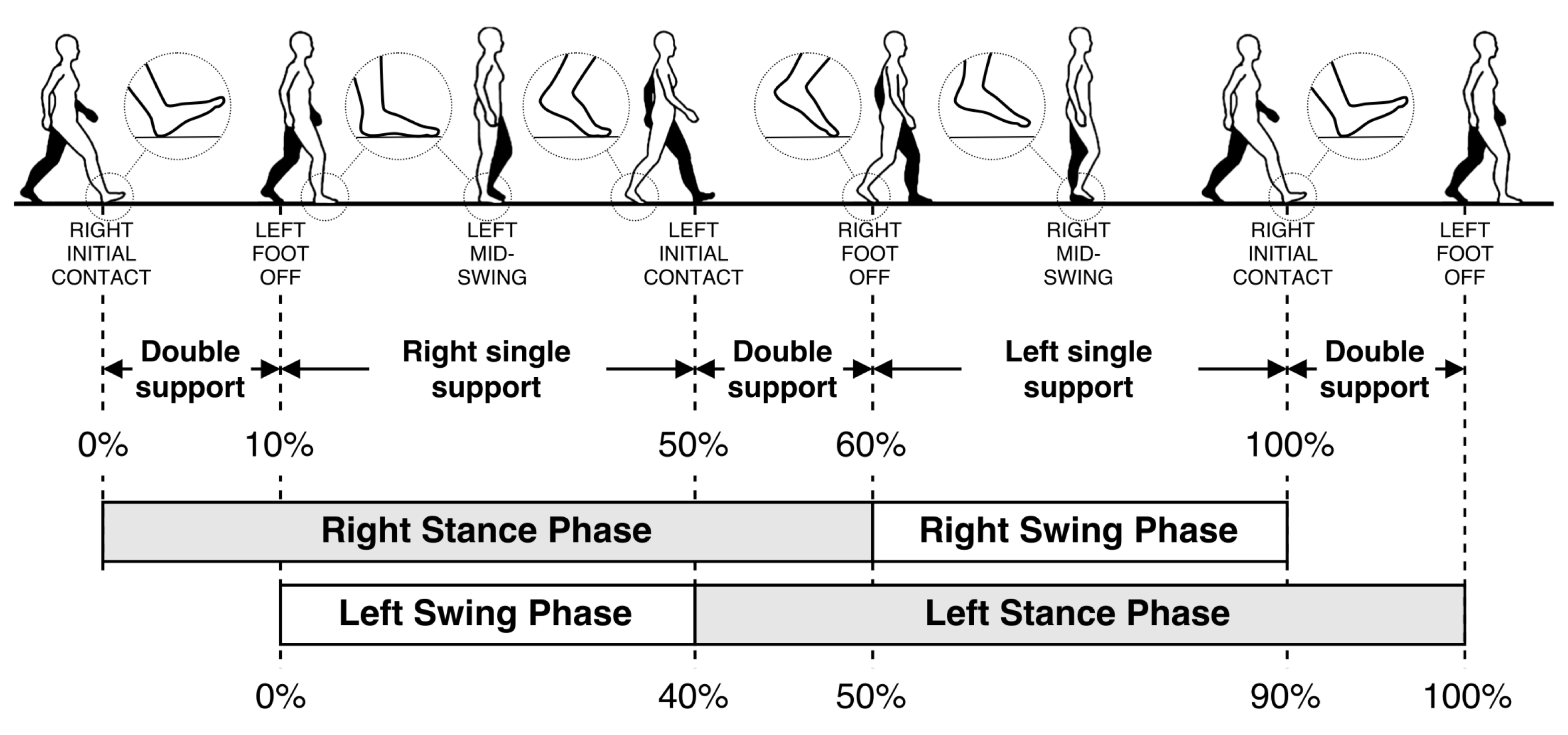
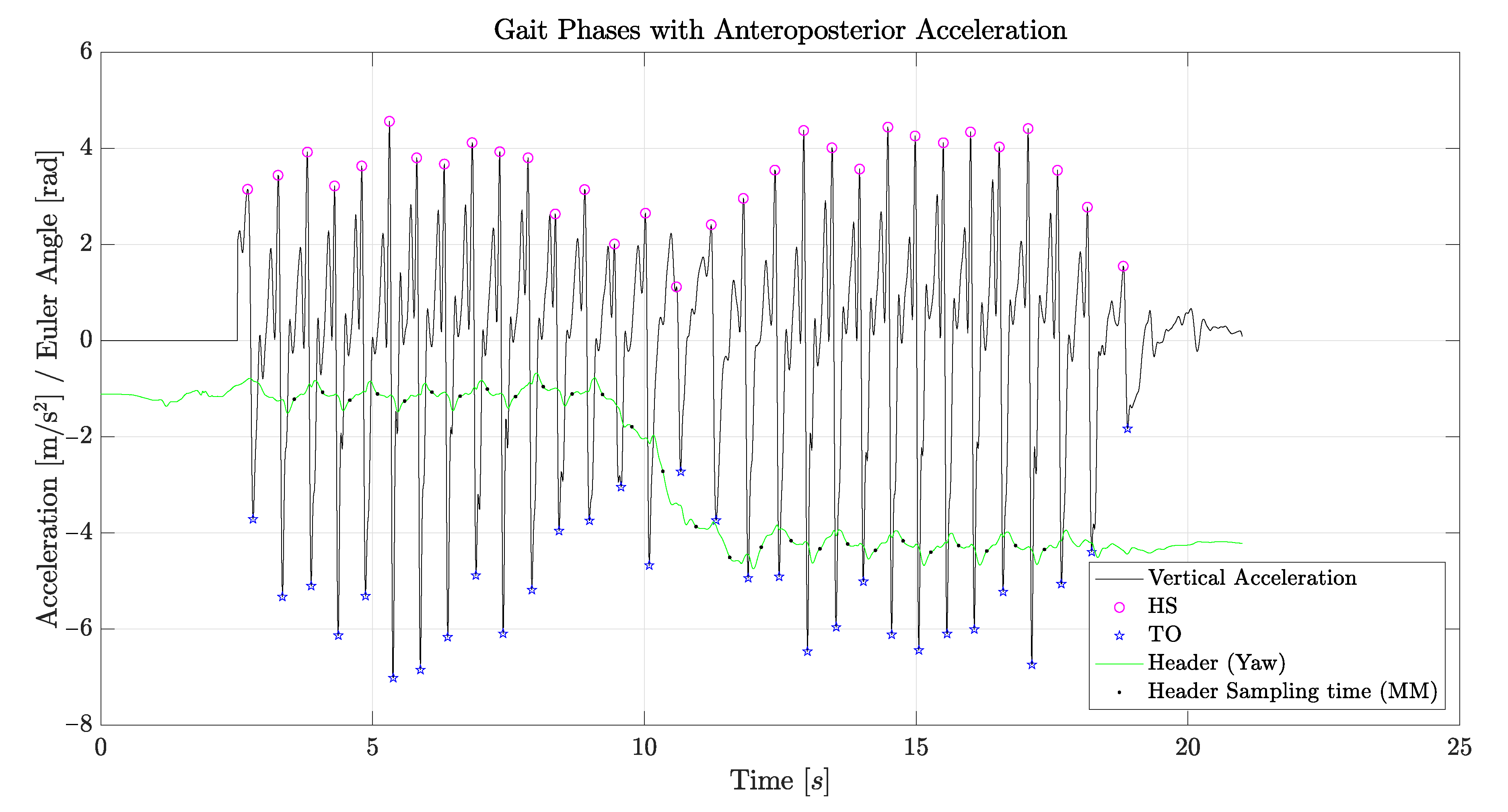
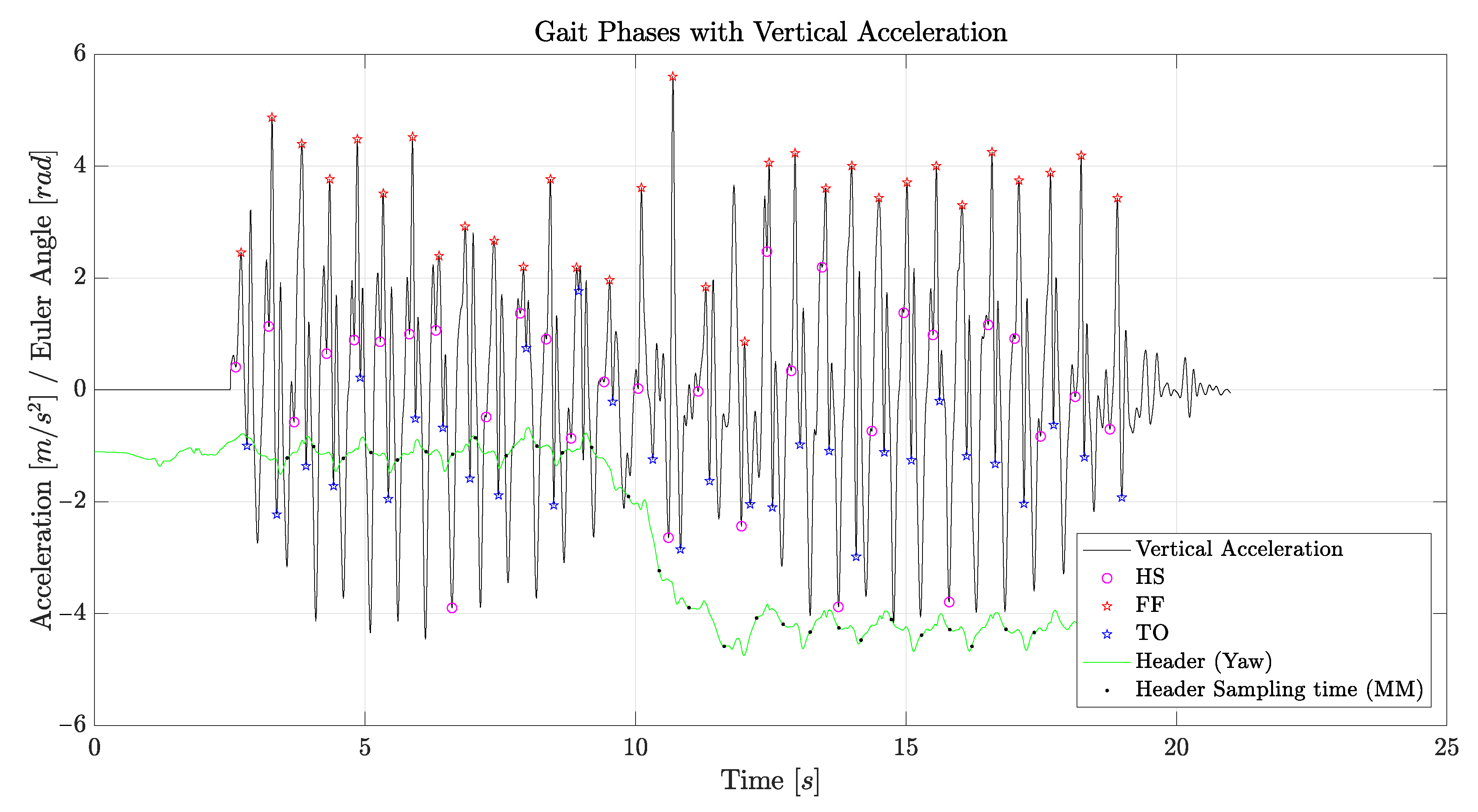
- Initial contact (IC): This phase, also called heel strike (HS) in standard notation, comprises the moment when the foot touches the floor. The joint postures presented at this time determine the limb’s loading response pattern;
- Loading response: This phase, also called foot flat (FF) in standard notation, is the initial double-stance (DS) period. The phase begins with initial floor contact and continues until the other foot is lifted for swing;
- Midstance (MM): This phase is the first half of the single-limb support interval. Here, the limb advances over the stationary foot through ankle dorsiflexion, while the knee and hip extend. Midstance begins when the other foot is lifted and continues until body weight is aligned over the forefoot;
- Terminal stance: This phase, also called heal off (HO) in standard notation, completes the single-limb support (SS). The stance begins with the heel rising and continues until the other foot strikes the ground. Throughout this phase, body weight moves ahead of the forefoot;
- Pre-swing: this final phase, also called toe off (TO) in standard notation, is the second double-stance interval in the gait cycle. Pre-swing begins with the initial contact of the opposite limb and ends with the ipsilateral toe off. The objective of this phase is to position the limb for swing;
- Initial swing: This phase is approximately one-third of the swing period, beginning with a lift of the foot from the floor and ending when the swinging foot is opposite the stance foot. In this phase, the foot is lifted, and the limb is advanced by hip flexion and increased knee flexion;
- Midswing: this phase begins as the swinging limb is opposite the stance limb and ends when the swinging limb is forward and the tibia is vertical;
- Terminal swing: This final phase of swing begins with a vertical tibia and ends when the foot strikes the floor.
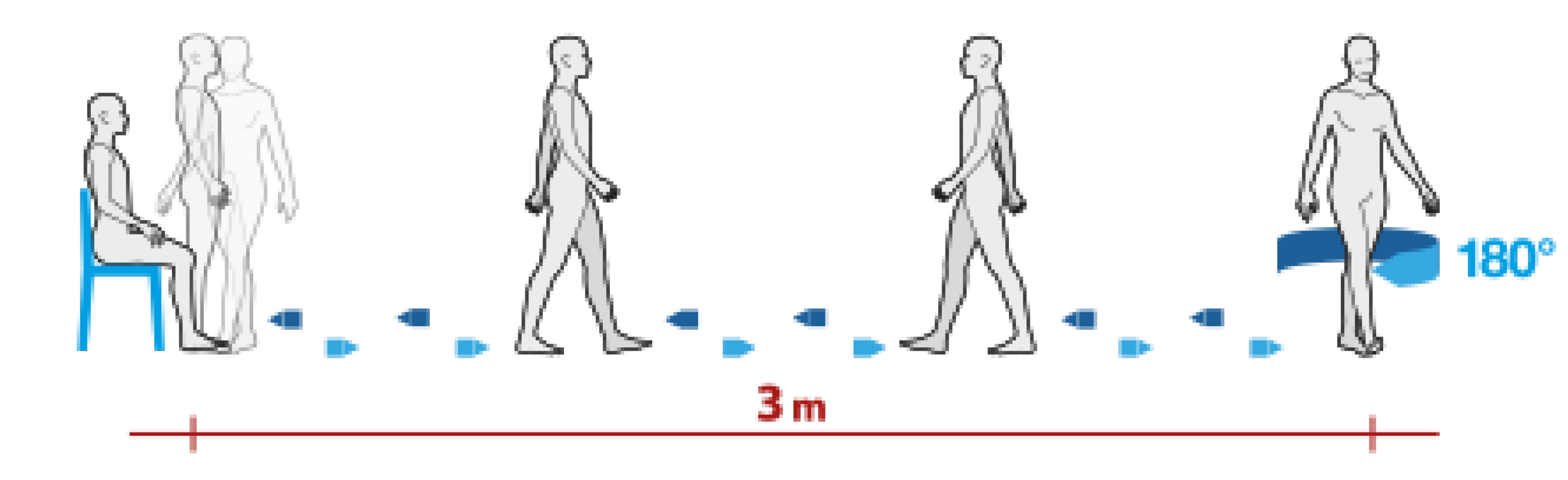
3.2. The Timed Up and Go Test
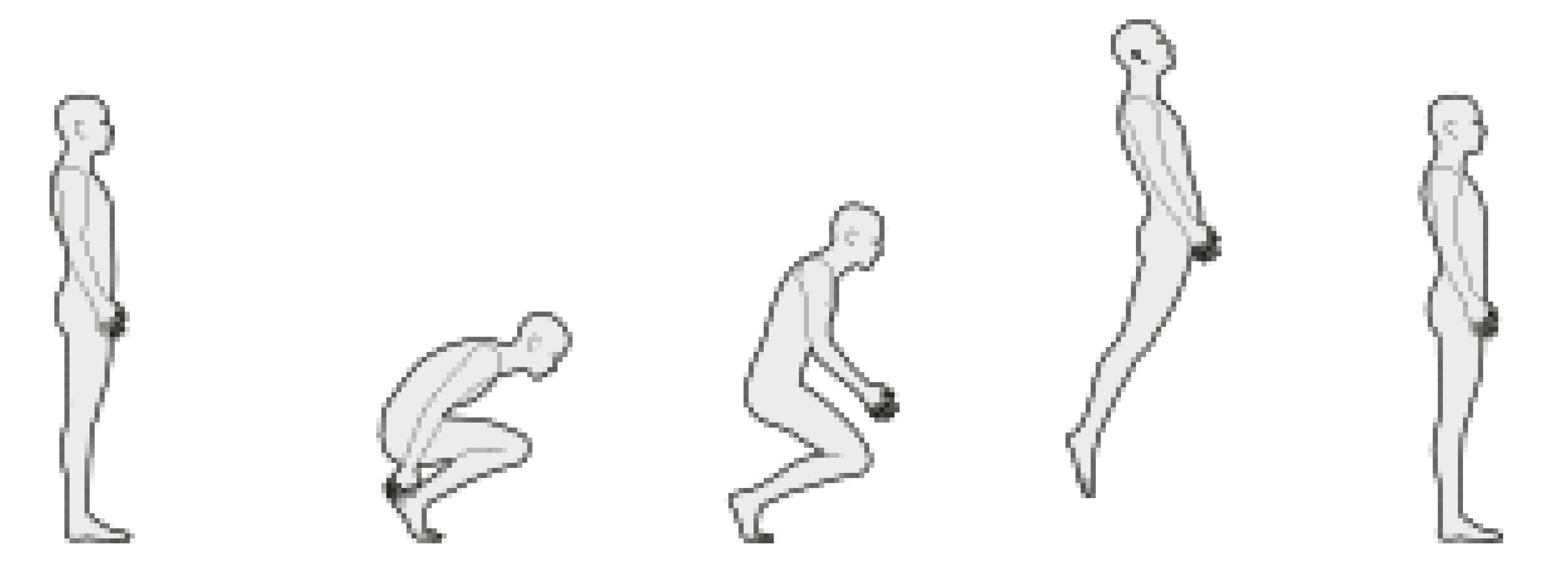
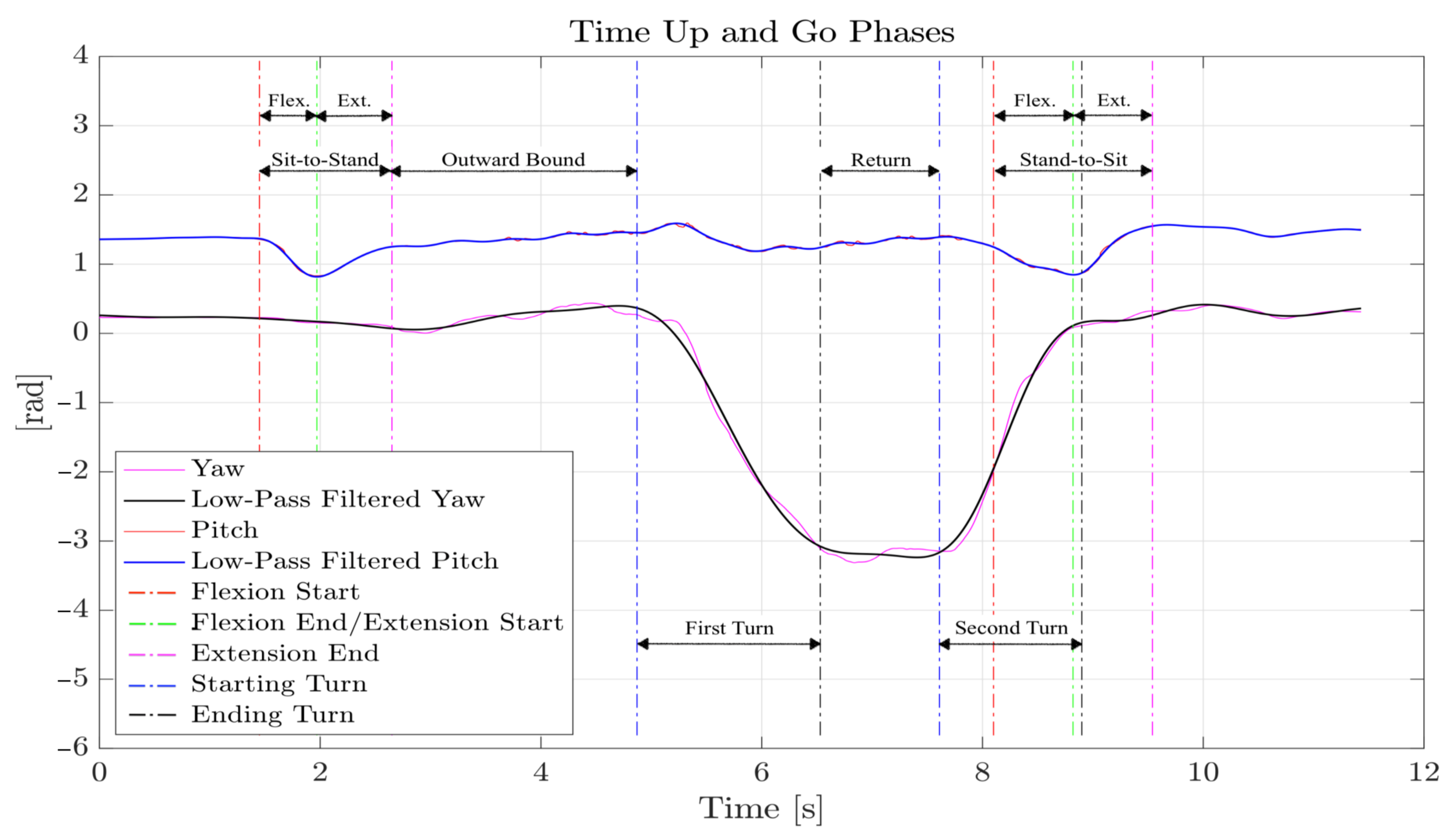
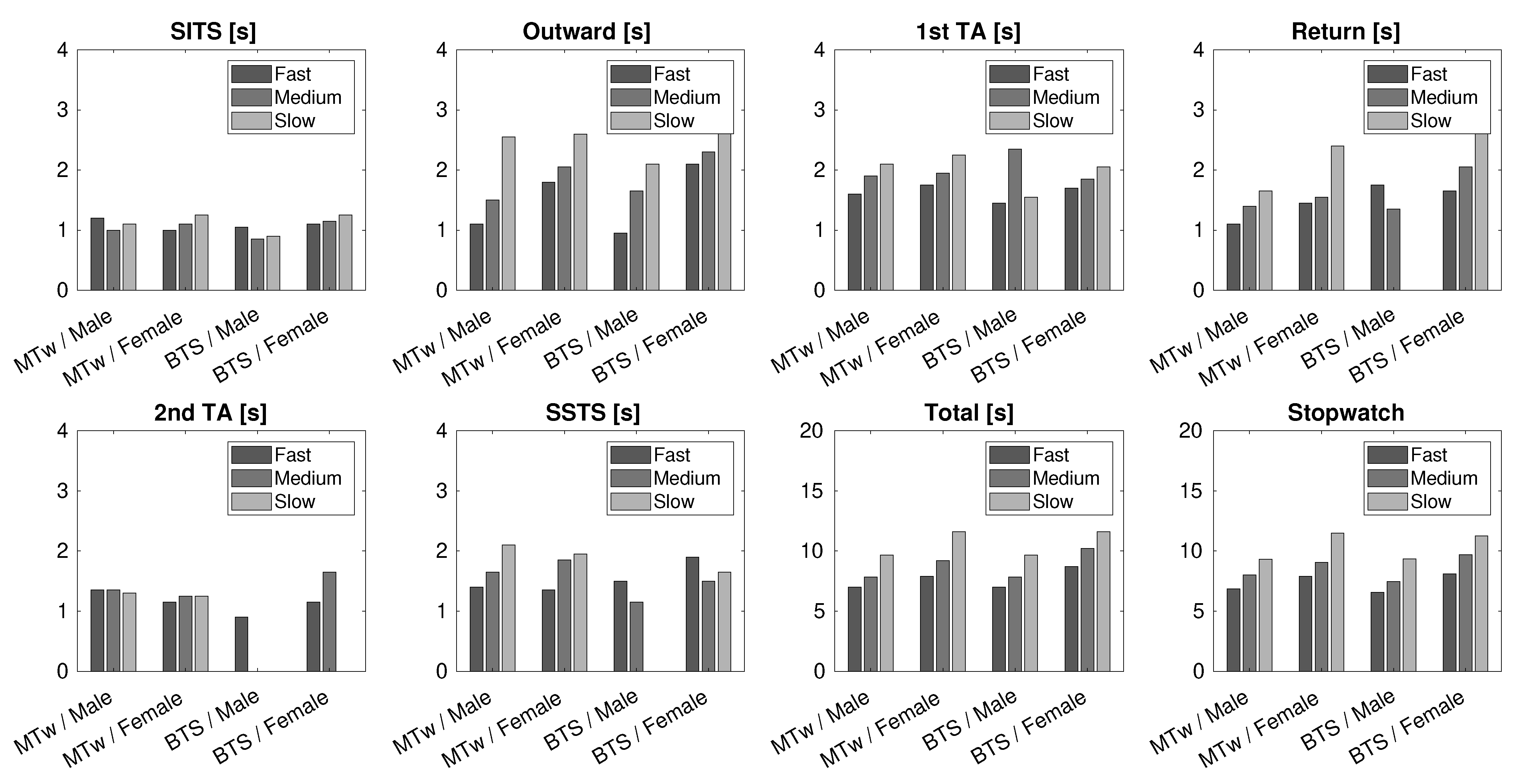
- Sit-to-stand time (SITS): the time taken by the subject to stand up from a sitting position. This phase is further divided in two parts: in the first part (flexion phase), the subject prepares himself or herself to stand up by carrying out a forward flexion of the torso; in the second part (extension phase), the subject stands up by extending the torso, which returns to the vertical position;
- Outward and return journey times: the time taken by the subject to walk from the chair to the cone in a straight line (outward) and vice versa (return);
- Turn-around time (TA): There are two different TA times: the first is the time it takes the subject to walk around the cone; the second is the time it takes the subject to turn around before sitting down again;
- Stand-to-sit time (SSTS): the time taken by the subject to sit down from a standing position. This phase is also divided in two parts: in the first part (flexion phase), the subject prepares himself or herself to sit down by carrying out a forward flexion of the torso; in the second part (extension phase), the subject sits down by extending the torso and returning to the vertical position.
3.3. A Control Test
3.4. The Counter-Movement Jump Test
3.5. The Muscle Stiffness Test
4. Data Analysis and Methods
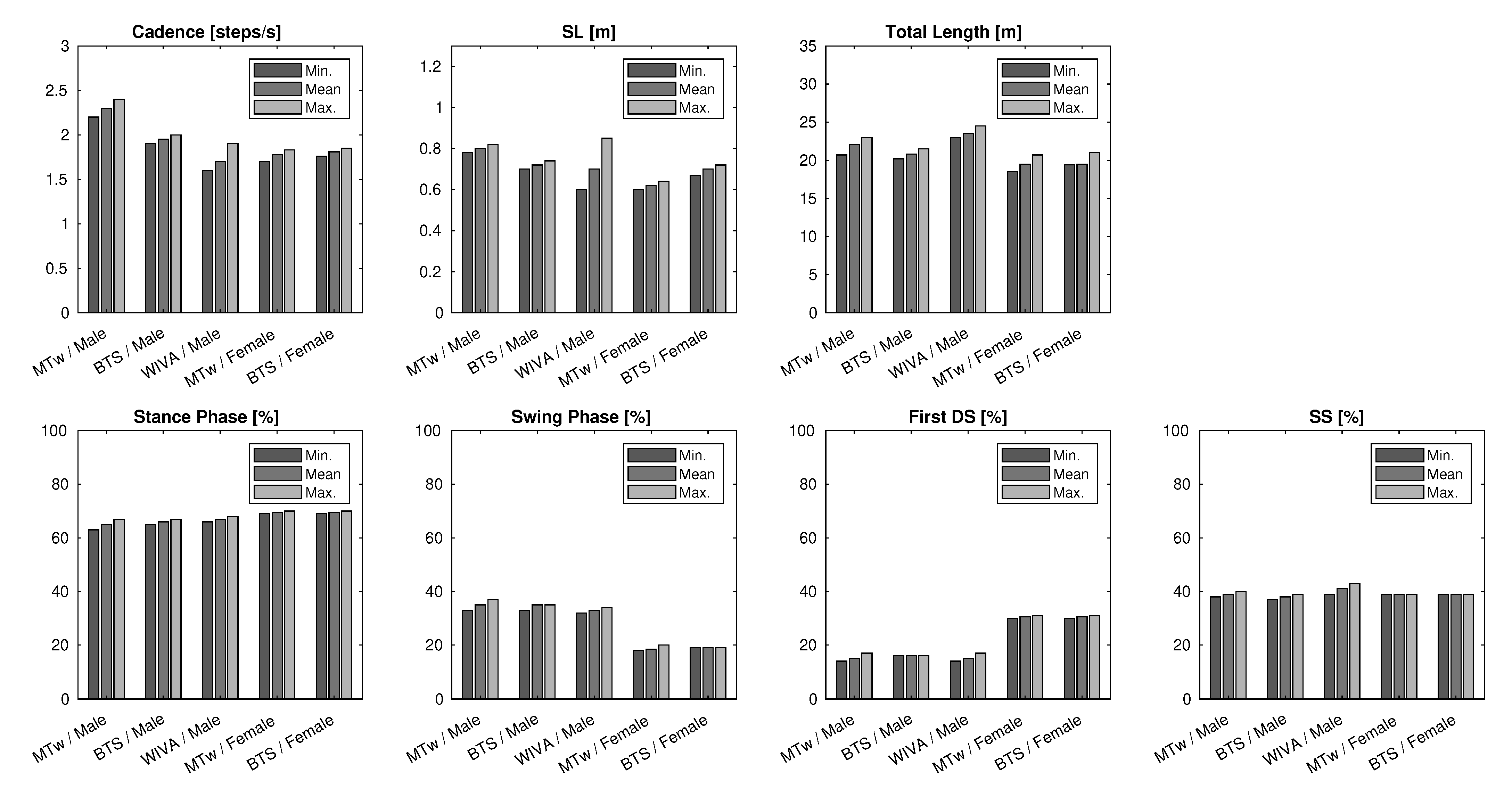
4.1. 10 m Walk
4.2. Timed Up and Go
4.3. Control Test
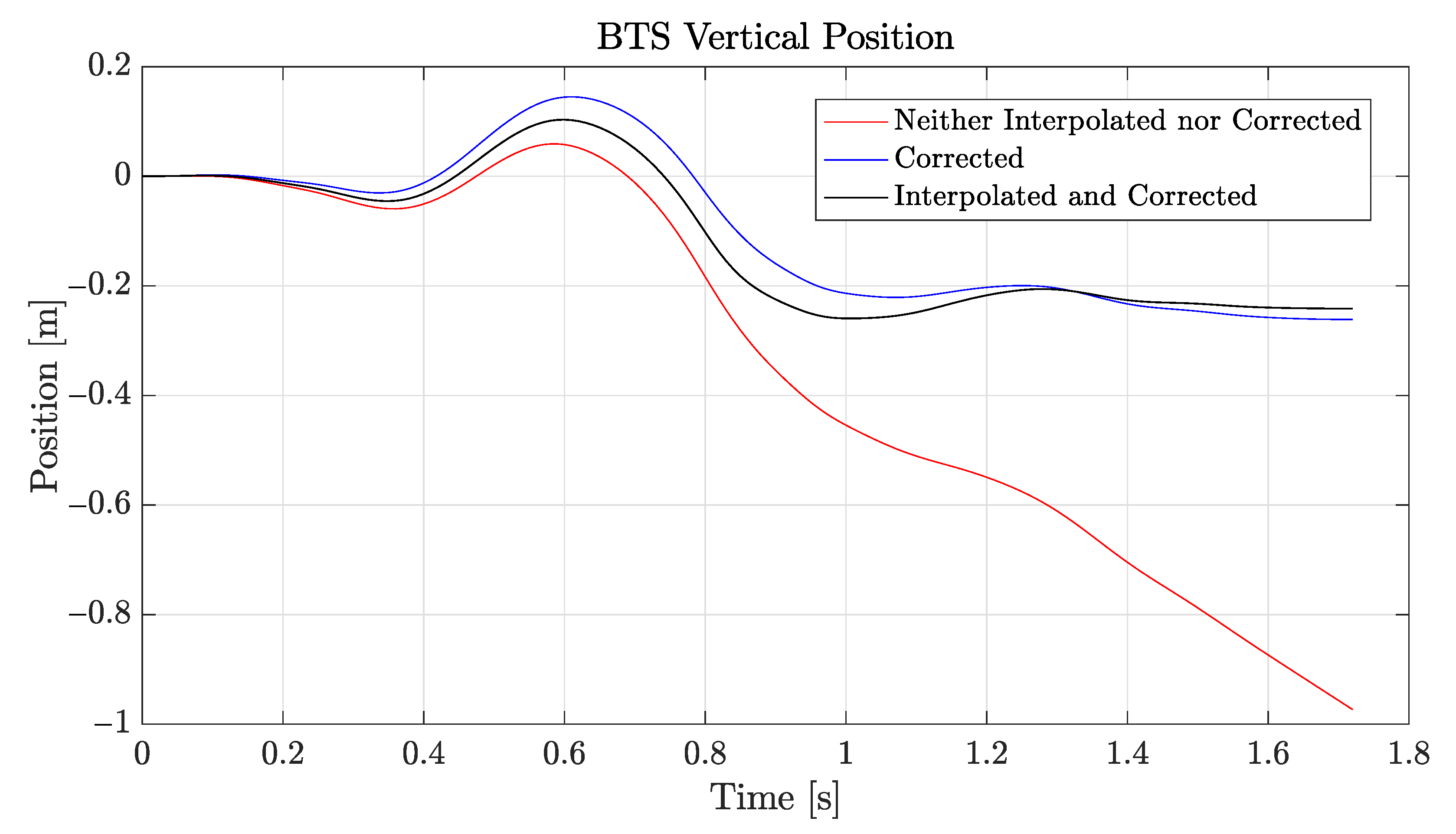
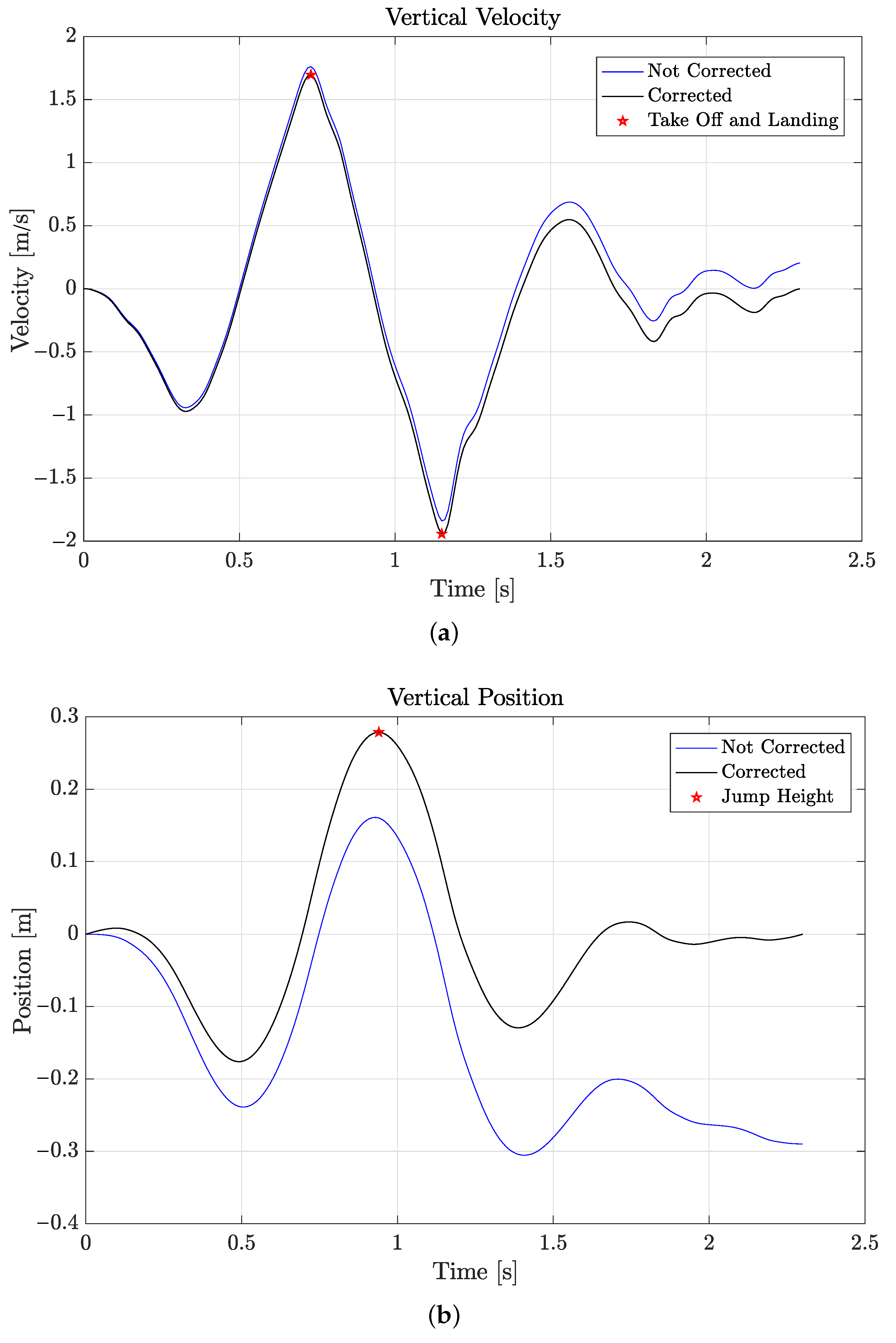
4.4. Counter-Movement Jump
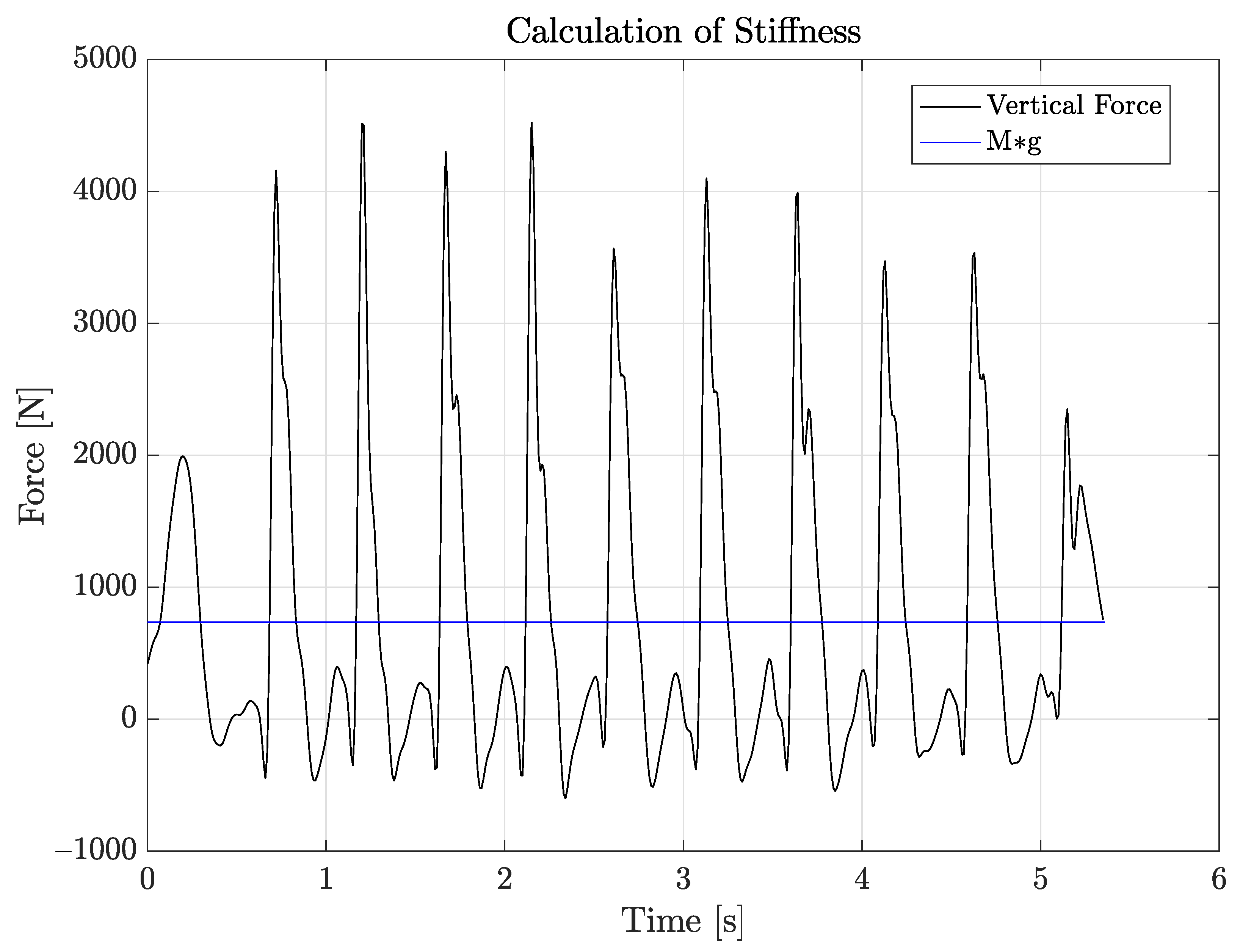
4.5. Stiffness
5. Results
5.1. 10 m Walk
5.2. Timed up and Go
5.3. Counter-Movement Jump
5.4. Stiffness
5.5. General Discussion
5.6. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| IMU | Inertial measurement unit |
| IMMU | Inertial-magnetic measurement unit |
| SDI | Strap-down integration |
| CMJ | Counter-movement jump |
| SL | Step length |
| IPM | Inverted pendulum model |
| SITS | Sit-to-stand time |
| SSTS | Stand-to-sit time |
| TA | Turn-around time |
| TOF | Time of flight |
| TUG | Timed Up and Go |
References
- Simon, S. Quantification of human motion: Gait analysis-benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Charlton, J.; Tse, C.; Esculier, J.; Graffos, A.; Krowchuk, N.; Thatcher, D.; Hunt, M. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Prasanth, H.; Caban, M.; Keller, U.; Courtine, G.; Ijspeert, A.; Vallery, H.; von Zitzewitz, J. Wearable Sensor-Based Real-Time Gait Detection: A Systematic Review. Sensors 2021, 21, 2727. [Google Scholar] [CrossRef] [PubMed]
- XSENS Technologies. MTw Awinda User Manual; XSENS: Enschede, The Netherlands, 2018. [Google Scholar]
- Kok, M.; Hol, J.D.; Schön, T.B. Using Inertial Sensors for Position and Orientation Estimation. Found. Trends Signal Process. 2017, 11, 1–153. [Google Scholar] [CrossRef] [Green Version]
- Paulich, M.; Schepers, M.; Rudigkeit, N.; Bellusci, G. XSENS MTw Awinda: Miniature Wireless Inertial-Magnetic Motion Tracker for Highly Accurate 3D Kinematic Applications; XSENS Technologies White Paper; XSENS: Enschede, The Netherlands, 2018. [Google Scholar]
- Wu, G.; Cavanagh, P. ISB recommendations for standardization in the reporting of kinematic data. J. Biomech. 1995, 28, 1257–1261. [Google Scholar] [CrossRef]
- BTS Bioengineering. BTS G-Sensor2 Hardware Manual; BTS S.p.A.: Milan, Italy, 2018. [Google Scholar]
- Tunca, C.; Pehlivan, N.; Arnrich, B.; Salur, G. Inertial Sensor-Based Robust Gait Analysis in Non-Hospital Settings for Neurological Disorders. Sensors 2017, 17, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsiadlo, D.; Richardson, S. The Timed Up and Go: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprint, G.; Cook, D.J.; Weeks, D.L. Toward Automating Clinical Assessments: A Survey of the Timed Up and Go. IEEE Rev. Biomed. Eng. 2015, 8, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Herman, T.; Plotnik, M.; Brozgol, M.; Maidan, I.; Giladi, N.; Gurevich, T.; Hausdorff, J.M. Can an accelerometer enhance the utility of the Timed up and Go Test when evaluating patients with Parkinson’s disease? Med. Eng. Phys. 2010, 32, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Beyea, J.; McGibbon, C.A.; Sexton, A.; Noble, J.; O’Connell, C. Convergent Validity of a Wearable Sensor System for Measuring Sub-Task Performance during the Timed up and Go Test. Sensors 2017, 17, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandelwal, S.; Wickström, N. Novel methodology for estimating Initial Contact events from accelerometers positioned at different body locations. Gait Posture 2018, 59, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Tietsch, M.; Muaremi, A.; Clay, I.; Kluge, F.; Hoefling, H.; Ullrich, M.; Küderle, A.; Eskofier, B.M.; Müller, A. Robust Step Detection from Different Waist-Worn Sensor Positions: Implications for Clinical Studies. Digit. Biomark 2020, 4 (Suppl. 1), 50–58. [Google Scholar] [CrossRef] [PubMed]
- Strozzi, N. Pedestrian Inertial Navigation. Ph.D. Thesis, University of Parma, Parma, Italy, 2018. [Google Scholar]
- Alvarez, D.; Gonzalez, R.C.; Lopez, A.; Alvarez, J.C. Comparison of Step Length Estimators from Wearable Accelerometer Devices. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 31 August–3 September 2006; pp. 5964–5967. [Google Scholar]
- Zijlstra, W.; Hof, A. Displacement of the pelvis during human walking: Experimental data and model predictions. Gait Posture 1997, 6, 249–262. [Google Scholar] [CrossRef]
- Gonzalez, R.C.; Alvarez, D.; Lopez, A.M.; Alvarez, J.C. Modified Pendulum Model for Mean Step Length Estimation. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007; pp. 1371–1374. [Google Scholar]
- McGinnis, R.S.; Cain, S.M.; Davidson, S.P.; Vitali, R.V.; Perkins, N.C.; McLean, S.G. Quantifying the effects of load carriage and fatigue under load on sacral kinematics during countermovement vertical jump with IMU-based method. Sport. Eng. 2016, 19, 21–34. [Google Scholar] [CrossRef]
- Setuain, I.; Martinikorena, J.; Izal, M.; Ramirez, A.; Gomez, M.; Adrian, J.; Izquierdo, M. Vertical jumping biomechanical evaluation through the use of an inertial sensor-based technology. J. Sport. Sci. 2015, 4, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Farley, C.; Blickhan, R.; Saito, J.M.; Taylor, C.R. Hopping frequency in humans: A test of how springs set stride frequency in bouncing gaits. J. Appl. Physiol. 1991, 71, 2127–2132. [Google Scholar] [CrossRef] [PubMed]
- Korff, T.; Horne, S.; Cullen, S.; Blazevich, A. Development of lower limb stiffness and its contribution to maximum vertical jumping power during adolescence. J. Exp. Biol. 2009, 212, 3737–3742. [Google Scholar] [CrossRef] [PubMed] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Sensors | Maximum Frequency |
|---|---|
| 1 up to 5 | 120 Hz |
| 6 up to 9 | 100 Hz |
| 10 | 80 Hz |
| 11 up to 20 | 60 Hz |
| Platform Height (m) | WIVA | BTS | MTw | Platform Height (m) | BTS | MTw |
|---|---|---|---|---|---|---|
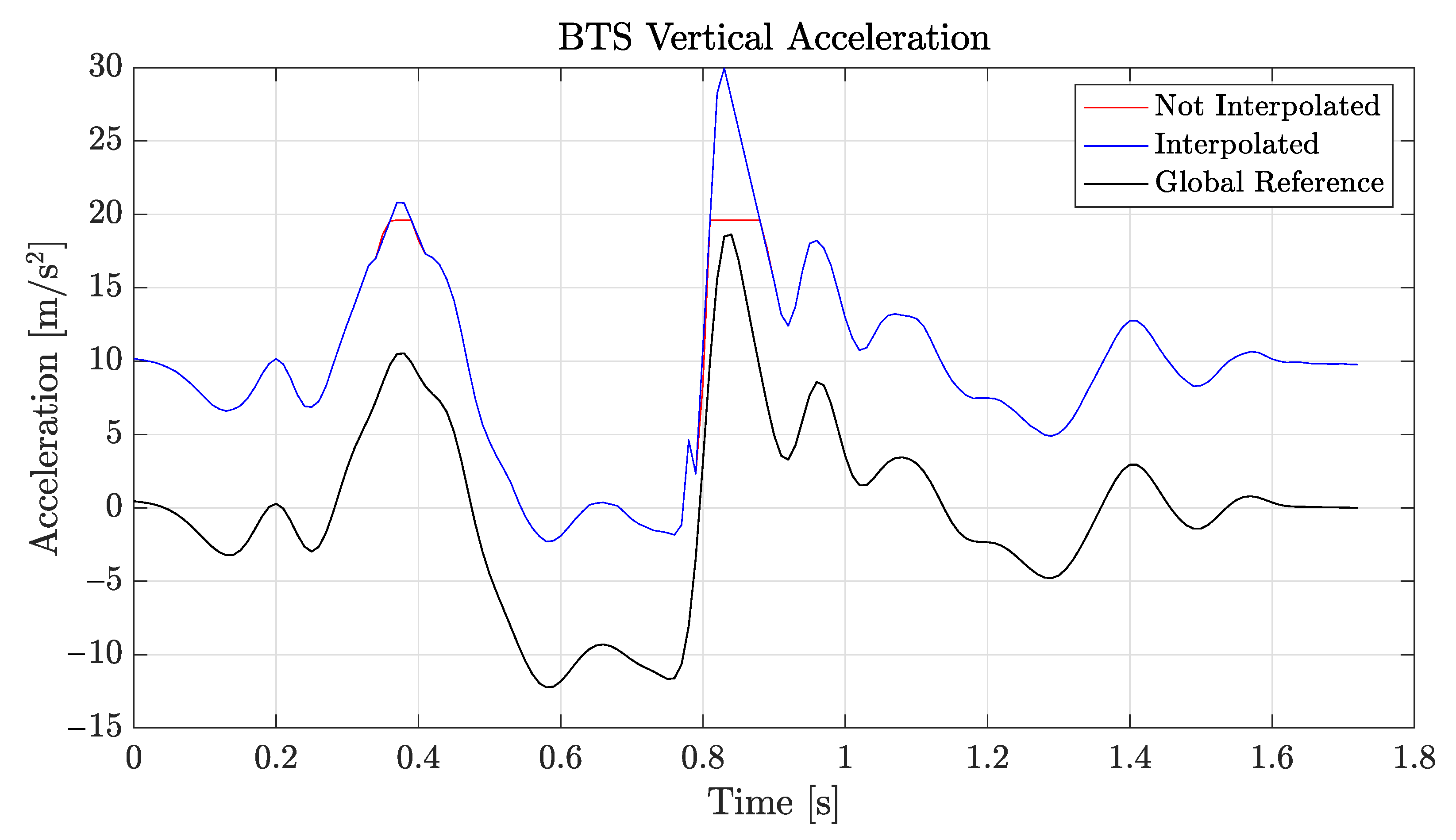
| No interpolation | 4.2 | 6.8 | 0.38 | No interpolation | 9.3 | 0.25 |
| Interpolation | 0.25 | 0.22 | 0.195 | Interpolation | 0.16 | 0.205 |
| Corrected | 0.145 | 0.213 | 0.195 | Corrected | 0.168 | 0.205 |
| Male | MTw | Video | Height |
|---|---|---|---|
| I Test | 0.39 s | 0.42 s | 0.29 |
| II Test | 0.39 s | 0.42 s | 0.22 |
| III Test | 0.43 s | 0.44 s | 0.25 |
| Female | BTS | Video | Height |
| I Test | 0.42 s | 0.42 s | 0.37 |
| II Test | 0.40 s | 0.42 s | 0.40 |
| III Test | 0.44 s | 0.44 s | 0.44 |
| Male | BTS | Video | Height |
| I Test | 0.37 s | 0.37 s | 0.31 |
| II Test | 0.39 s | 0.39 s | 0.15 |
| III Test | 0.41 s | 0.44 s | 0.31 |
| Female | BTS | Video | Height |
| I Test | 0.42 s | 0.44 s | 0.27 |
| II Test | 0.41 s | 0.42 s | 0.23 |
| III Test | 0.42 s | 0.42 s | 0.39 |
| Male | WIVA | Video | Height |
| I Test | 0.43 s | 0.41 s | 0.44 |
| II Test | 0.42 s | 0.40 s | 0.45 |
| III Test | 0.41 s | 0.40 s | 0.35 |
| Male Stiffness | MTw | BTS |
|---|---|---|
| k Minimum | 44.56 kN | 33.58 kN |
| k Mean | 44.75 kN | 40.88 kN |
| k Maximum | 55.75 kN | 54.83 kN |
| w Minimum | 1.38 s | 1.5 s−1 |
| w Mean | 1.66 s | 1.72 s−1 |
| w Maximum | 2.01 s | 2.01 s−1 |
| k Minimum | 22.84 kN | 25.61 kN |
| k Mean | 28.83 kN | 35.69 kN |
| k Maximum | 37.76 kN | 74.02 kN |
| w Minimum | 1.75 s | 1.25 s−1 |
| w Mean | 2.04 s | 1.88 s−1 |
| w Maximum | 2.26 s | 2.13 s−1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrenacci, I.; Boccaccini, R.; Bolzoni, A.; Colavolpe, G.; Costantino, C.; Federico, M.; Ugolini, A.; Vannucci, A. A Comparative Evaluation of Inertial Sensors for Gait and Jump Analysis. Sensors 2021, 21, 5990. https://0-doi-org.brum.beds.ac.uk/10.3390/s21185990
Andrenacci I, Boccaccini R, Bolzoni A, Colavolpe G, Costantino C, Federico M, Ugolini A, Vannucci A. A Comparative Evaluation of Inertial Sensors for Gait and Jump Analysis. Sensors. 2021; 21(18):5990. https://0-doi-org.brum.beds.ac.uk/10.3390/s21185990
Chicago/Turabian StyleAndrenacci, Isaia, Riccardo Boccaccini, Alice Bolzoni, Giulio Colavolpe, Cosimo Costantino, Michelangelo Federico, Alessandro Ugolini, and Armando Vannucci. 2021. "A Comparative Evaluation of Inertial Sensors for Gait and Jump Analysis" Sensors 21, no. 18: 5990. https://0-doi-org.brum.beds.ac.uk/10.3390/s21185990