
A Novel Hybrid Approach Based on Deep CNN Features to Detect Knee Osteoarthritis

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Literature Review
- To propose a novel robust algorithm that can carry out early detection of KOA according to the KL grading. The proposed algorithm uses X-ray images for training and testing the results. The hybrid features descriptors extract features, that is, CNN with HOG and CNN with LBP. Three multi-classifiers are used to classify disease according to the KL grading system (I, II, III, IV), such as KNN, RF, and SVM;
- Cross-validation has been used, using 420 images to evaluate the performance of the proposed technique, and results show 97% accuracy for overall detection and classification;
- A five-fold validation is used, such as (50,50), (25,75), (30,70), (40,60), (20,80); here, an individual set represents the train and test data respectively for each Grade and the last set is for a healthy class. Our proposed technique gives an accuracy of 98% for all grade classifications;
- We analyzed the performance of individual grade detection during cross-validation, revealing the following facts for the classification: The algorithm obtained 98% accuracy for Grade I, 97% accuracy for Grade II, 98.5% accuracy for Grade III and Grade IV;
- Due to the algorithm’s robustness, it can be used for other disease detection and classification, acquiring significant results.
3. Proposed Framework
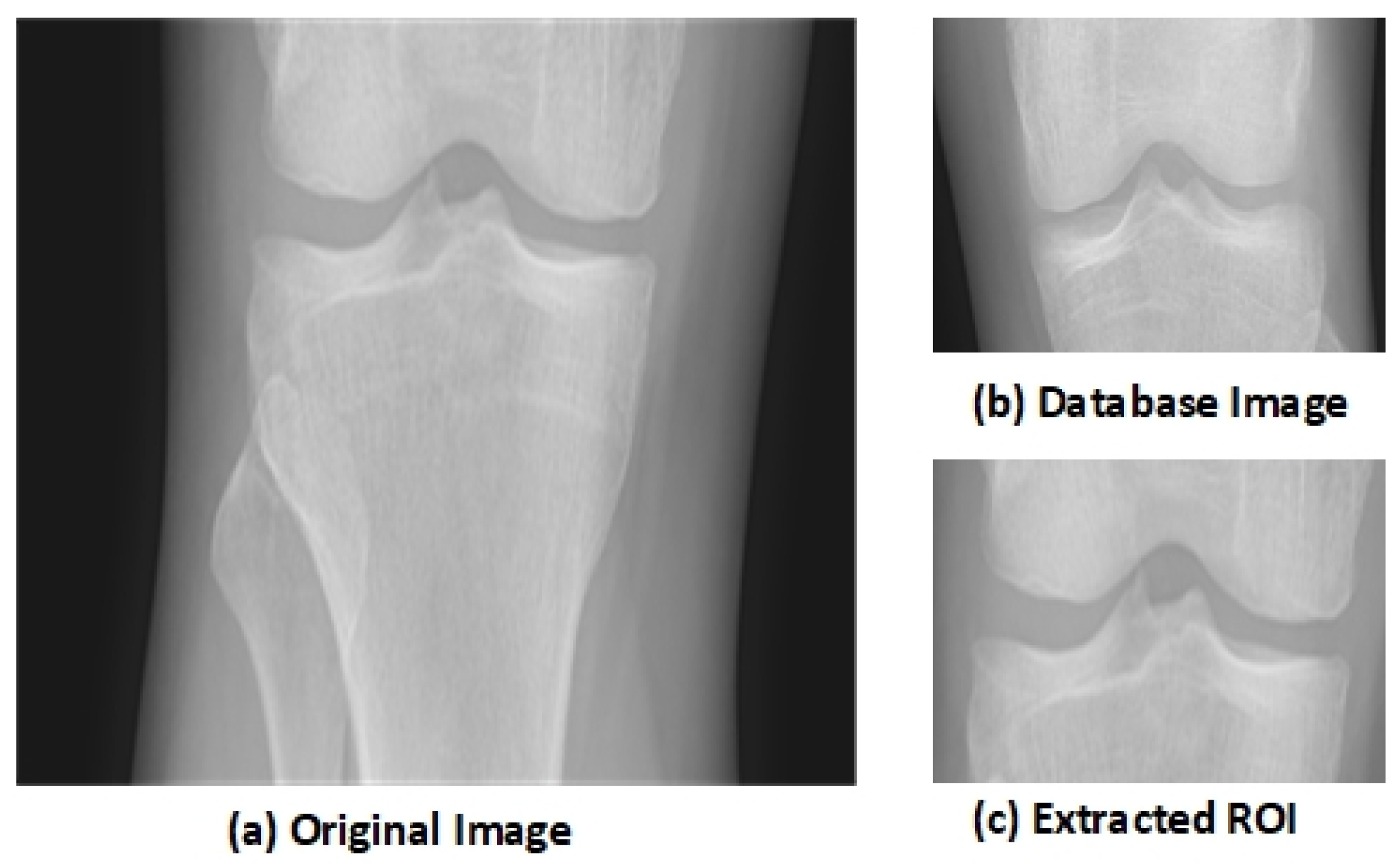
3.1. Pre-Processing
3.2. Region of Interest (ROI) and Segmentation
3.3. Deep Learning
3.4. Feature Extraction
3.5. Convolutional Neural Network as Feature Descriptor
3.6. Histogram of Oriented Gradient
3.7. Local Binary Pattern
| Algorithm 1 Pseudo code for proposed framework. |
Input: Output: Begin data(i) ← 1....k While(data(i)!= eof) { Preprocessing of the Images (change format, downscaling, negative of the image) CNNF← 2DCNN Features Extraction HOGF ← Histogram of Oriented Gradient Feature Extraction LBPF ← Local Binary Pattern Feature Extraction FV ← (CNNF HOGF LBPF) FV1 ← (CNNF+HOGF CNNF+LBPF) CL ← AssignClassLabels (Grades I...IV, Healthy) Classification ← ( SVM (FV1, CL, testImages) KNN (FV1, CL, testImages) RF (FV1, CL, testmages) ) For j=1...n { if (Classification(j))← 1 print Grade-I else if(Classification(j))← 2 print Grade-II else if(Classification(j))← 3 print Grade-III else if(Classification(j))← 4 print Grade-IV else if(Classification(j))← Healthy print KOA not detected } End |
3.8. Classification
4. Experimental Evaluation
4.1. Dataset
4.2. Results
4.3. Evaluation Metrics
4.4. Comparison with State-of-the-Art
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hodgson, R.; O’connor, P.; Moots, R. MRI of rheumatoid arthritis—Image quantitation for the assessment of disease activity, progression and response to therapy. Rheumatology 2008, 47, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Saleem, M.; Farid, M.S.; Saleem, S.; Khan, M.H. X-ray image analysis for automated knee osteoarthritis detection. Signal Image Video Process. 2020, 14, 1079–1087. [Google Scholar] [CrossRef]
- Abedin, J.; Antony, J.; McGuinness, K.; Moran, K.; O’Connor, N.E.; Rebholz-Schuhmann, D.; Newell, J. Predicting knee osteoarthritis severity: Comparative modeling based on patient’s data and plain X-ray images. Sci. Rep. 2019, 9, 5761. [Google Scholar] [CrossRef] [PubMed]
- Hendren, L.; Beeson, P. A review of the differences between normal and osteoarthritis articular cartilage in human knee and ankle joints. Foot 2009, 19, 171–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamir, L.; Ling, S.M.; Scott, W.W.; Bos, A.; Orlov, N.; Macura, T.J.; Eckley, D.M.; Ferrucci, L.; Goldberg, I.G. Knee x-ray image analysis method for automated detection of osteoarthritis. IEEE Trans. Biomed. Eng. 2008, 56, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Brahim, A.; Jennane, R.; Riad, R.; Janvier, T.; Khedher, L.; Toumi, H.; Lespessailles, E. A decision support tool for early detection of knee OsteoArthritis using X-ray imaging and machine learning: Data from the OsteoArthritis Initiative. Comput. Med. Imaging Graph. 2019, 73, 11–18. [Google Scholar] [CrossRef]
- Emrani, P.S.; Katz, J.N.; Kessler, C.L.; Reichmann, W.M.; Wright, E.A.; McAlindon, T.E.; Losina, E. Joint space narrowing and Kellgren–Lawrence progression in knee osteoarthritis: An analytic literature synthesis. Osteoarthr. Cartil. 2008, 16, 873–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mengko, T.L.; Wachjudi, R.G.; Suksmono, A.B.; Danudirdjo, D. Automated detection of unimpaired joint space for knee osteoarthritis assessment. In Proceedings of the 7th International Workshop on Enterprise Networking and Computing in Healthcare Industry, 2005 (HEALTHCOM 2005), Busan, Korea, 23–25 June 2005; pp. 400–403. [Google Scholar]
- Iqbal, M.N.; Haidri, F.R.; Motiani, B.; Mannan, A. Frequency of factors associated with knee osteoarthritis. JPMA-J. Pak. Med. Assoc. 2011, 61, 786. [Google Scholar]
- Porcheret, M.; Jordan, K.; Jinks, C.P. Croft in collaboration with the Primary Care Rheumatology Society. Primary care treatment of knee pain—A survey in older adults. Rheumatology 2007, 46, 1694–1700. [Google Scholar] [CrossRef] [Green Version]
- Swamy, M.M.; Holi, M. Knee joint cartilage visualization and quantification in normal and osteoarthritis. In Proceedings of the 2010 International Conference on Systems in Medicine and Biology, Kharagpur, India, 16–18 December 2010; pp. 138–142. [Google Scholar]
- Dodin, P.; Pelletier, J.P.; Martel-Pelletier, J.; Abram, F. Automatic human knee cartilage segmentation from 3-D magnetic resonance images. IEEE Trans. Biomed. Eng. 2010, 57, 2699–2711. [Google Scholar] [CrossRef] [Green Version]
- Hani, A.F.M.; Malik, A.S.; Kumar, D.; Kamil, R.; Razak, R.; Kiflie, A. Features and modalities for assessing early knee osteoarthritis. In Proceedings of the 2011 International Conference on Electrical Engineering and Informatics, Bandung, Indonesia, 17–19 July 2011; pp. 1–6. [Google Scholar]
- Ababneh, S.Y.; Gurcan, M.N. An automated content-based segmentation framework: Application to MR images of knee for osteoarthritis research. In Proceedings of the 2010 IEEE International Conference on Electro/Information Technology, Normal, IL, USA, 20–22 May 2010; pp. 1–4. [Google Scholar]
- Tiulpin, A.; Thevenot, J.; Rahtu, E.; Lehenkari, P.; Saarakkala, S. Automatic knee osteoarthritis diagnosis from plain radiographs: A deep learning-based approach. Sci. Rep. 2018, 8, 1727. [Google Scholar] [CrossRef] [PubMed]
- Antony, J.; McGuinness, K.; Moran, K.; O’Connor, N.E. Automatic detection of knee joints and quantification of knee osteoarthritis severity using convolutional neural networks. In International Conference on Machine Learning and Data Mining in Pattern Recognition; Springer: Berlin/Heidelberg, Germany, 2017; pp. 376–390. [Google Scholar]
- Antony, J.; McGuinness, K.; O’Connor, N.E.; Moran, K. Quantifying radiographic knee osteoarthritis severity using deep convolutional neural networks. In Proceedings of the 2016 23rd International Conference on Pattern Recognition (ICPR), Cancun, Mexico, 4–8 December 2016; pp. 1195–1200. [Google Scholar]
- Mansour, R.F. Deep-learning-based automatic computer-aided diagnosis system for diabetic retinopathy. Biomed. Eng. Lett. 2018, 8, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Haas, J.; Rabus, B. Uncertainty Estimation for Deep Learning-Based Segmentation of Roads in Synthetic Aperture Radar Imagery. Remote Sens. 2021, 13, 1472. [Google Scholar] [CrossRef]
- Rostami, M.; Kolouri, S.; Eaton, E.; Kim, K. Sar image classification using few-shot cross-domain transfer learning. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Long Beach, CA, USA, 16–17 June 2019. [Google Scholar]
- Li, L. Deep residual autoencoder with multiscaling for semantic segmentation of land-use images. Remote Sens. 2019, 11, 2142. [Google Scholar] [CrossRef] [Green Version]
- Hauptmann, A.; Arridge, S.; Lucka, F.; Muthurangu, V.; Steeden, J.A. Real-time cardiovascular MR with spatio-temporal artifact suppression using deep learning–proof of concept in congenital heart disease. Magn. Reson. Med. 2019, 81, 1143–1156. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Han, X.; Ma, S.; Lin, T.; Gong, J. Monitoring ecosystem service change in the City of Shenzhen by the use of high-resolution remotely sensed imagery and deep learning. Land Degrad. Dev. 2019, 30, 1490–1501. [Google Scholar] [CrossRef]
- McBride, J.; Zhang, S.; Wortley, M.; Paquette, M.; Klipple, G.; Byrd, E.; Baumgartner, L.; Zhao, X. Neural network analysis of gait biomechanical data for classification of knee osteoarthritis. In Proceedings of the 2011 Biomedical Sciences and Engineering Conference: Image Informatics and Analytics in Biomedicine, Knoxville, TN, USA, 15–17 March 2011; pp. 1–4. [Google Scholar]
- Guess, T.M.; Thiagarajan, G.; Kia, M.; Mishra, M. A subject specific multibody model of the knee with menisci. Med. Eng. Phys. 2010, 32, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Guess, T.M.; Liu, H.; Bhashyam, S.; Thiagarajan, G. A multibody knee model with discrete cartilage prediction of tibio-femoral contact mechanics. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 256–270. [Google Scholar] [CrossRef]
- Cashman, P.M.; Kitney, R.I.; Gariba, M.A.; Carter, M.E. Automated techniques for visualization and mapping of articular cartilage in MR images of the osteoarthritic knee: A base technique for the assessment of microdamage and submicro damage. IEEE Trans. Nanobiosci. 2002, 99, 42–51. [Google Scholar] [CrossRef]
- Yin, Y.; Zhang, X.; Williams, R.; Wu, X.; Anderson, D.D.; Sonka, M. LOGISMOS—layered optimal graph image segmentation of multiple objects and surfaces: Cartilage segmentation in the knee joint. IEEE Trans. Med. Imaging 2010, 29, 2023–2037. [Google Scholar] [CrossRef] [PubMed]
- Toyoshima, T.; Nagamune, K.; Araki, D.; Matsumoto, T.; Kubo, S.; Matsushita, T.; Kuroda, R.; Kurosaka, M. A development of navigation system with image segmentation in mosaicplasty of the knee. In Proceedings of the 2012 IEEE International Conference on Fuzzy Systems, Brisbane, QLD, Australia, 10–15 June 2012; pp. 1–6. [Google Scholar]
- Tiderius, C.J.; Olsson, L.E.; Leander, P.; Ekberg, O.; Dahlberg, L. Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) in early knee osteoarthritis. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2003, 49, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Zahurul, S.; Zahidul, S.; Jidin, R. An adept edge detection algorithm for human knee osteoarthritis images. In Proceedings of the 2010 International Conference on Signal Acquisition and Processing, Bangalore, India, 9–10 February 2010; pp. 375–379. [Google Scholar]
- Tamez-Pena, J.G.; Farber, J.; Gonzalez, P.C.; Schreyer, E.; Schneider, E.; Totterman, S. Unsupervised segmentation and quantification of anatomical knee features: Data from the Osteoarthritis Initiative. IEEE Trans. Biomed. Eng. 2012, 59, 1177–1186. [Google Scholar] [CrossRef]
- Ababneh, S.Y.; Gurcan, M.N. An efficient graph-cut segmentation for knee bone osteoarthritis medical images. In Proceedings of the 2010 IEEE International Conference on Electro/Information Technology, Normal, IL, USA, 20–22 May 2010; pp. 1–4. [Google Scholar]
- Stehling, C.; Baum, T.; Mueller-Hoecker, C.; Liebl, H.; Carballido-Gamio, J.; Joseph, G.; Majumdar, S.; Link, T. A novel fast knee cartilage segmentation technique for T2 measurements at MR imaging–data from the Osteoarthritis Initiative. Osteoarthr. Cartil. 2011, 19, 984–989. [Google Scholar] [CrossRef] [Green Version]
- Shan, L.; Zach, C.; Niethammer, M. Automatic three-label bone segmentation from knee MR images. In Proceedings of the 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Rotterdam, The Netherlands, 14–17 April 2010; pp. 1325–1328. [Google Scholar]
- Shamir, L.; Ling, S.M.; Scott, W.; Hochberg, M.; Ferrucci, L.; Goldberg, I.G. Early detection of radiographic knee osteoarthritis using computer-aided analysis. Osteoarthr. Cartil. 2009, 17, 1307–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutherford, D.J.; Baker, M. Knee moment outcomes using inverse dynamics and the cross product function in moderate knee osteoarthritis gait: A comparison study. J. Biomech. 2018, 78, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, A.; Stewart, C.; Postans, N.; Biggs, P.; Whatling, G.; Holt, C.; Roberts, A. Abnormal loading and functional deficits are present in both limbs before and after unilateral knee arthroplasty. Gait Posture 2017, 55, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Liu, Y.; Yan, S.; Cao, G.; Wang, S.; Lester, D.K.; Zhang, K. Clinical gait evaluation of patients with knee osteoarthritis. Gait Posture 2017, 58, 319–324. [Google Scholar] [CrossRef]
- Phinyomark, A.; Osis, S.T.; Hettinga, B.A.; Kobsar, D.; Ferber, R. Gender differences in gait kinematics for patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2016, 17, 157. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, H.; Hagino, H.; Sageshima, H.; Osaki, M.; Tanishima, S.; Tanimura, C. Diagnosis of knee osteoarthritis and gait variability increases risk of falling for osteoporotic older adults: The GAINA study. Osteoporos. Sarcopenia 2015, 1, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Farrokhi, S.; O’Connell, M.; Gil, A.B.; Sparto, P.J.; Fitzgerald, G.K. Altered gait characteristics in individuals with knee osteoarthritis and self-reported knee instability. J. Orthop. Sport. Phys. Ther. 2015, 45, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Favre, J.; Erhart-Hledik, J.C.; Andriacchi, T.P. Age-related differences in sagittal-plane knee function at heel-strike of walking are increased in osteoarthritic patients. Osteoarthr. Cartil. 2014, 22, 464–471. [Google Scholar] [CrossRef] [Green Version]
- Asay, J.L.; Boyer, K.A.; Andriacchi, T.P. Repeatability of gait analysis for measuring knee osteoarthritis pain in patients with severe chronic pain. J. Orthop. Res. 2013, 31, 1007–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henriksen, M.; Aaboe, J.; Bliddal, H. The relationship between pain and dynamic knee joint loading in knee osteoarthritis varies with radiographic disease severity. A cross sectional study. Knee 2012, 19, 392–398. [Google Scholar] [CrossRef]
- Gornale, S.S.; Patravali, P.U.; Marathe, K.S.; Hiremath, P.S. Determination of osteoarthritis using histogram of oriented gradients and multiclass SVM. Int. J. Image Graph. Signal Process. 2017, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Gornale, S.S.; Patravali, P.U.; Hiremath, P.S. Automatic Detection and Classification of Knee Osteoarthritis Using Hu’s Invariant Moments. Front. Robot. AI 2020, 7, 591827. [Google Scholar] [CrossRef] [PubMed]
- Shivanand Gornale, P.P. Digital Knee X-ray Images. Available online: http://0-dx-doi-org.brum.beds.ac.uk/10.17632/t9ndx37v5h.1#folder-18a3659a-1fa2-4340-b7bb-526fb81006f6 (accessed on 23 June 2020).
- Caselles, V.; Kimmel, R.; Sapiro, G. Geodesic active contours. Int. J. Comput. Vis. 1997, 22, 61–79. [Google Scholar] [CrossRef]
- Sainath, T.N.; Mohamed, A.R.; Kingsbury, B.; Ramabhadran, B. Deep convolutional neural networks for LVCSR. In Proceedings of the 2013 IEEE International Conference on Acoustics, Speech and Signal Processing, Vancouver, BC, Canada, 26–31 May 2013; pp. 8614–8618. [Google Scholar]
- Song, Q.; Zhao, L.; Luo, X.; Dou, X. Using deep learning for classification of lung nodules on computed tomography images. J. Healthc. Eng. 2017, 2017, 9314740. [Google Scholar] [CrossRef] [Green Version]
- Mary, N.A.B.; Dharma, D. Coral reef image classification employing improved LDP for feature extraction. J. Vis. Commun. Image Represent. 2017, 49, 225–242. [Google Scholar] [CrossRef]
- Gornale, S.S.; Patravali, P.U.; Manza, R.R. Detection of osteoarthritis using knee X-ray image analyses: A machine vision based approach. Int. J. Comput. Appl 2016, 145, 0975–8887. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards real-time object detection with region proposal networks. IEEE Trans. Pattern Anal. Mach. Intell. 2016, 39, 1137–1149. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.; Gao, L.; Shi, X.; Allen, K.; Yang, L. Fully automatic knee osteoarthritis severity grading using deep neural networks with a novel ordinal loss. Comput. Med. Imaging Graph. 2019, 75, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Wahyuningrum, R.T.; Anifah, L.; Purnama, I.K.E.; Purnomo, M.H. A New approach to classify knee osteoarthritis severity from radiographic images based on CNN-LSTM method. In Proceedings of the 2019 IEEE 10th International Conference on Awareness Science and Technology (iCAST), Morioka, Japan, 23–25 October 2019; pp. 1–6. [Google Scholar]
- Gong, R.; Hase, K.; Goto, H.; Yoshioka, K.; Ota, S. Knee osteoarthritis detection based on the combination of empirical mode decomposition and wavelet analysis. J. Biomech. Sci. Eng. 2020, 15, 20-00017. [Google Scholar] [CrossRef] [Green Version]
- Tiulpin, A.; Saarakkala, S. Automatic grading of individual knee osteoarthritis features in plain radiographs using deep convolutional neural networks. Diagnostics 2020, 10, 932. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Dataset | Accuracy | Findings | Contributions |
|---|---|---|---|---|
| [37] | 74 Moderate Knee Osteoarthritis Patients Images | 95% | Cross Function and Inverse Dynamics Computed the Knee Moments Outcome efficiently | Only moderate cases were used |
| [38] | 20 KOA and 20 Healthy Knee | 95% | Optimized results obtained by Focused Rehabilitation | Patients had only single joint disease |
| [39] | 23 KOA Images and 12 Healthy Images | 95% | Results were optimized using IDEEA3 for KOA Anlaysis | Five parameters were considered for measurement of KOA patients to record space |
| [40] | 45 Healthy (18 Males and 25 Females) 100 KOA Patients (45 Males and 55 Females) | 98% | Gender is Key Factor in Analysis of KOA | Considered only knee joint kinematics |
| [41] | 91 KOA Patients (22 Males and 29 Females) | 97% | KOA patients have greater risk of falling | Selection bias probability |
| [42] | 17 KOA Patients, SRKI and 36 KOA, NSRKI | 95% | SRKI cause changes in joints position | Considered KOA patients who were in medical care |
| [43] | 110 KOA Patients (29 youngers, 27 Health Control, 28 Moderate, 26 Severe) | 93% | Enhanced KAM was seen in KOA patients | Cross Validation to check the impact of undiagnosed KOA in healthy people |
| [44] | 43 KOA Patients | 94% | Gait trail was considered in which only KAM was reappearing | Number of participants was small |
| [45] | 137 KOA Patients | 96% | Positive correlation among severe pain and KAM impulse | Study design was cross-sectional |
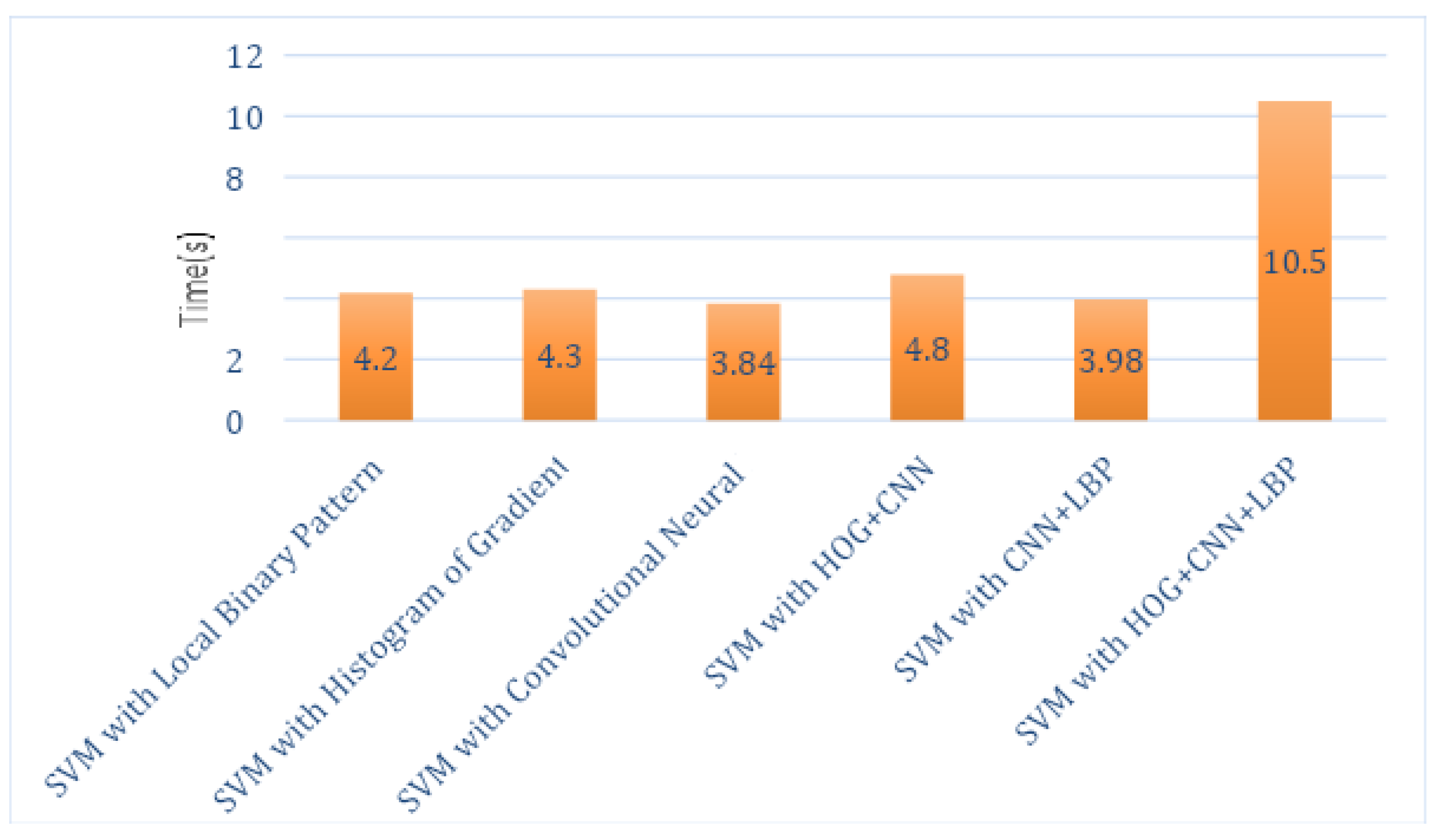
| Classifier Name | Time in Seconds |
|---|---|
| SVM with Local Binary Pattern | 4.2 s |
| SVM with Histogram of Oriented Gradients | 4.3 s |
| SVM with Convolutional Neural Network | 3.84 s |
| SVM with HOG + CNN | 4.8 s |
| SVM with CNN + LBP | 3.98 s |
| SVM with HOG + CNN + LBP | 10.5 s |
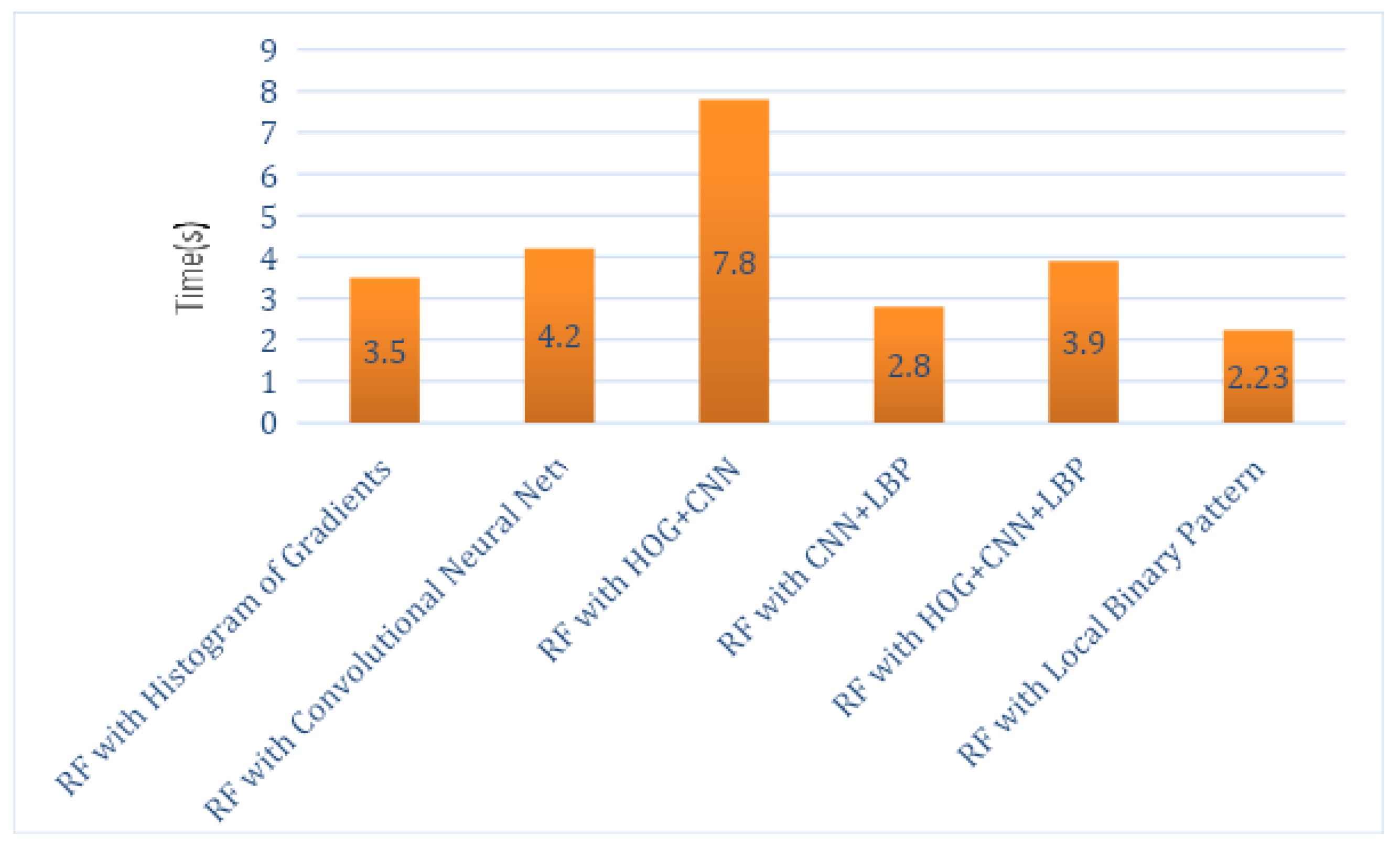
| Classifier Name | Time in Seconds |
|---|---|
| RF with Histogram of Oriented Gradients | 3.5 s |
| RF with Convolutional Neural Network | 4.2 s |
| RF with HOG + CNN | 7.8 s |
| RF with CNN + LBP | 2.8 s |
| RF with HOG + CNN + LBP | 3.9 s |
| RF with Local Binary Pattern | 2.23 s |
| Classifier Name | Time in Seconds |
|---|---|
| KNN with Histogram of Oriented Gradients | 3.3 s |
| KNN with Convolutional Neural Network | 4.3 s |
| KNN with HOG + CNN | 7.8 s |
| KNN with CNN + LBP | 2.4 s |
| KNN with HOG + CNN + LBP | 3.8 s |
| KNN with Local Binary Pattern | 2.3 s |
| SVM_LBP | SVM_HOG | SVM_CNN | SVM_HOG_CNN | SVM_LBP_CNN | |
|---|---|---|---|---|---|
| P N | P N | P N | P N | P N | |
| P | 360 37 | 342 45 | 328 43 | 348 17 | 356 35 |
| N | 8 15 | 13 20 | 24 25 | 17 38 | 14 15 |
| RF_LBP | RF_HOG | RF_CNN | RF_HOG_CNN | RF_LBP_CNN | |
|---|---|---|---|---|---|
| P N | P N | P N | P N | P N | |
| P | 355 40 | 332 50 | 345 13 | 357 20 | 353 36 |
| N | 9 16 | 15 23 | 16 46 | 20 23 | 15 16 |
| KNN_LBP | KNN_HOG | KNN_CNN | KNN_HOG_CNN | KNN_LBP_CNN | |
|---|---|---|---|---|---|
| P N | P N | P N | P N | P N | |
| P | 350 40 | 345 43 | 330 40 | 383 8 | 351 35 |
| N | 13 17 | 13 19 | 22 28 | 4 25 | 16 18 |
| Method | Average | Standard Deviation | Precision | Recall | Accuracy |
|---|---|---|---|---|---|
| SVM_LBP | 0.5342 | 0.0581 | 97.82% | 90.68% | 89.28% |
| SVM_HOG | 0.4993 | 0.0631 | 96.33% | 88.37% | 86.19% |
| SVM_CNN | 0.5521 | 0.0913 | 93.18% | 88.40% | 81.66% |
| SVM_HOG_CNN | 0.5330 | 0.0632 | 95.34% | 95.34% | 91.90% |
| SVM_LBP_CNN | 0.4783 | 0.0634 | 96.21% | 91.04% | 88.33% |
| RF_LBP | 0.5432 | 0.0599 | 97.52% | 89.87% | 88.33% |
| RF_HOG | 0.4231 | 0.0653 | 95.67% | 86.91% | 84.52% |
| RF_CNN | 0.4323 | 0.0685 | 95.56% | 96.36% | 93.09% |
| RF_HOG_CNN | 0.4345 | 0.0654 | 94.69% | 94.69% | 90.47% |
| RF_LBP_CNN | 0.4594 | 0.0601 | 95.92% | 90.74% | 87.85% |
| KNN_LBP | 0.4534 | 0.0610 | 96.41% | 89.74% | 87.38% |
| KNN_HOG | 0.4958 | 0.0611 | 96.36% | 88.91% | 88.66% |
| KNN_CNN | 0.4789 | 0.0672 | 93.75% | 89.18% | 85.23% |
| KNN_HOG_CNN | 0.5412 | 0.0580 | 98.96% | 97.95% | 97.14% |
| KNN_LBP_CNN | 0.4345 | 0.0632 | 95.64% | 90.93% | 87.85% |
| Method | Recall | Precision | Accuracy | Data Set |
|---|---|---|---|---|
| CNN [16] | 62 | 58 | 61.78 | OAI and MOST |
| DeepCNN [58] | - | - | 66.68 | OAI and MOST |
| Siamese CNNs [15] | - | - | 67.49 | OAI and MOST |
| VGG-19 [55] | - | - | 69.70 | OAI |
| CNN-LSTM [56] | - | - | 75.28 | OAI |
| Faster R-CNN [54] | - | - | 74.30 | - |
| LASVM [57] | - | - | 86.67 | VAG Signals |
| RF [53] | 60.49 | 67.12 | 72.95 | Hospital Images |
| The Proposed Algorithm | 97.95 | 98.96 | 97.14 | Mendeley Dataset IV |
| Grade | Accuracy (%) |
|---|---|
| I | 91 |
| II | 98 |
| III | 99.5 |
| IV | 99.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahum, R.; Rehman, S.U.; Meraj, T.; Rauf, H.T.; Irtaza , A.; El-Sherbeeny, A.M.; El-Meligy , M.A. A Novel Hybrid Approach Based on Deep CNN Features to Detect Knee Osteoarthritis. Sensors 2021, 21, 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186189
Mahum R, Rehman SU, Meraj T, Rauf HT, Irtaza A, El-Sherbeeny AM, El-Meligy MA. A Novel Hybrid Approach Based on Deep CNN Features to Detect Knee Osteoarthritis. Sensors. 2021; 21(18):6189. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186189
Chicago/Turabian StyleMahum, Rabbia, Saeed Ur Rehman, Talha Meraj, Hafiz Tayyab Rauf, Aun Irtaza , Ahmed M. El-Sherbeeny, and Mohammed A. El-Meligy . 2021. "A Novel Hybrid Approach Based on Deep CNN Features to Detect Knee Osteoarthritis" Sensors 21, no. 18: 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186189