
Novel Technique to Measure Pulse Wave Velocity in Brain Vessels Using a Fast Simultaneous Multi-Slice Excitation Magnetic Resonance Sequence


Abstract
:1. Introduction
2. Materials and Methods
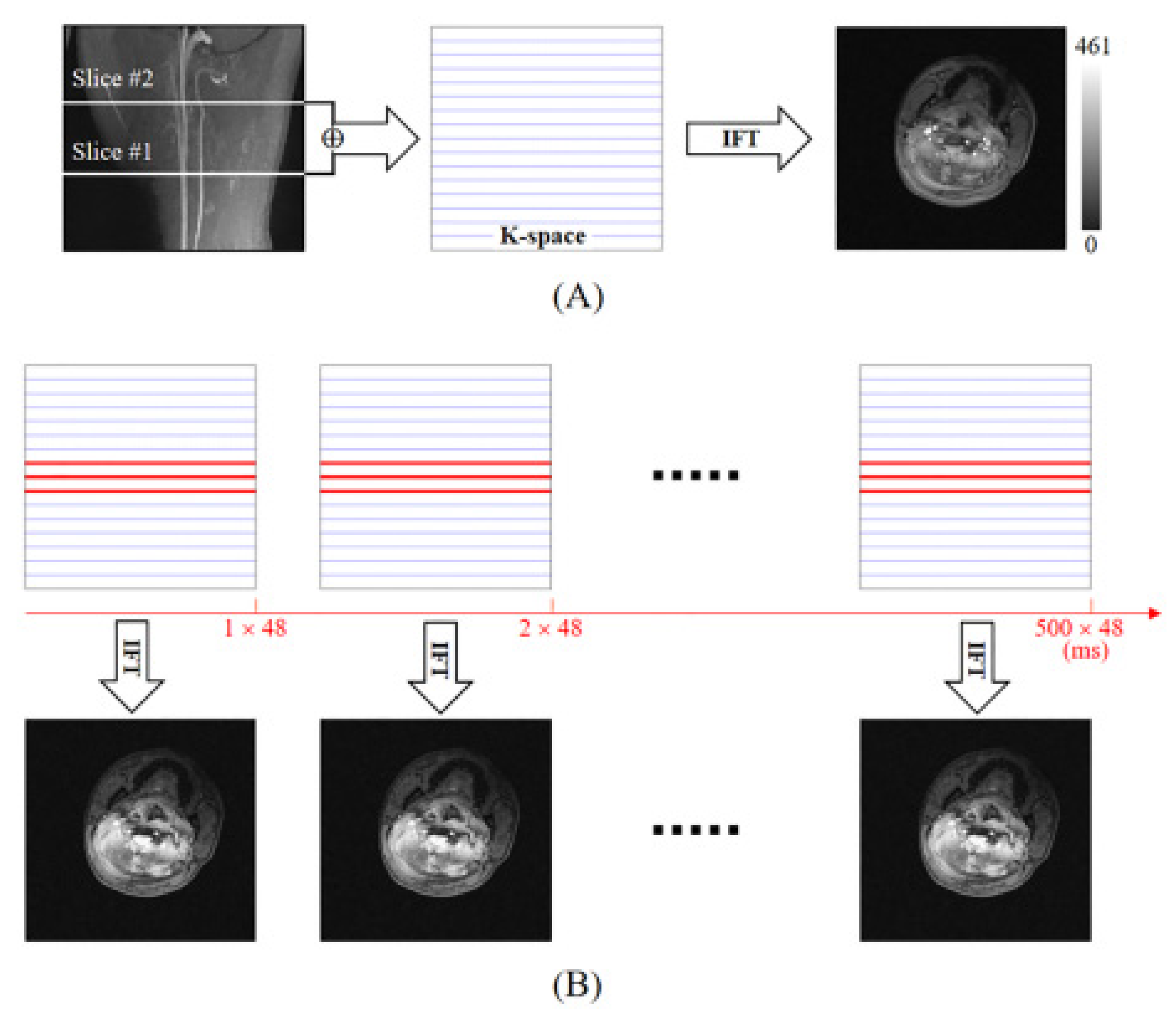
2.1. Method of SMS-K
2.2. Phantom MRI Experimental Protocols
2.3. Human MRI Experimental Protocols
2.4. Human Heart-Finger PWV Experiment Protocols
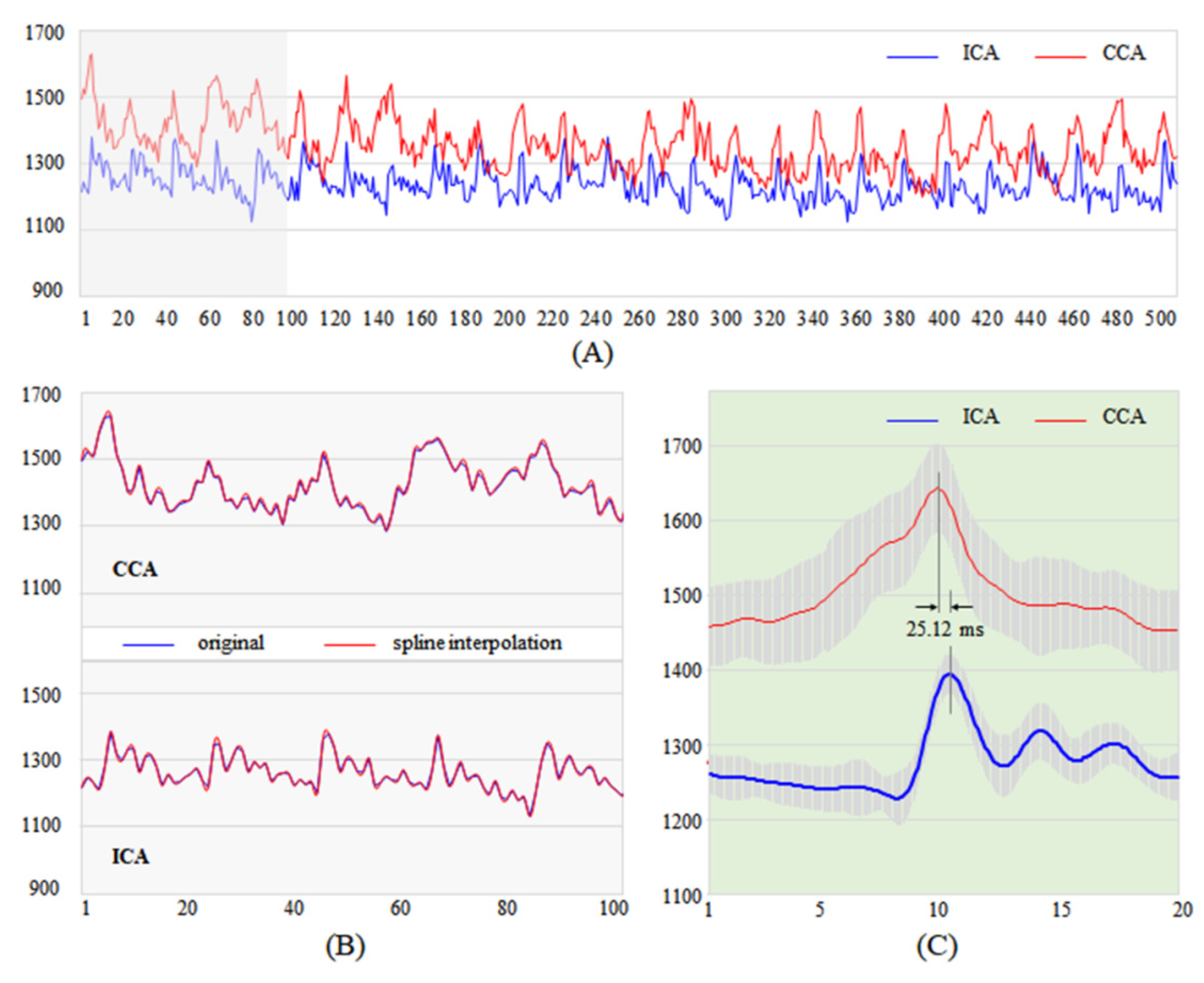
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murphy, S.J.X.; Werring, D.J. Stroke: Causes and Clinical Features. Medicine (Abingdon) 2020, 48, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.-L.; Dong, Y.; Xu, W.; Huang, Y.-Y.; Wang, H.-F.; Zhang, T.-S.; Sun, L.; Tan, L.; Dong, Q.; Yu, J.-T. Role of Blood Pressure Management in Stroke Prevention: A Systematic Review and Network Meta-Analysis of 93 Randomized Controlled Trials. J. Stroke 2021, 23, 1–11. [Google Scholar] [CrossRef]
- Baek, J.H.; Kim, K.; Lee, Y.-B.; Park, K.-H.; Park, H.-M.; Shin, D.-J.; Sung, Y.H.; Shin, D.H.; Bang, O.Y. Predicting Stroke Outcome Using Clinical- versus Imaging-Based Scoring System. J. Stroke Cerebrovasc. Dis. 2015, 24, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Whangbo, T. Evaluating a Deep-Learning System for Automatically Calculating the Stroke ASPECT Score. In Proceedings of the 2018 International Conference on Information and Communication Technology Convergence (ICTC), Jeju, Korea, 17–19 October 2018; pp. 564–567. [Google Scholar]
- Lee, K.R.; Bae, J.H.; Hwang, I.C.; Kim, K.K.; Suh, H.S.; Ko, K.D. Effect of Influenza Vaccination on Risk of Stroke: A Systematic Review and Meta-Analysis. NED 2017, 48, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.R.; Hwang, I.C.; Lee, Y.J.; Ham, E.B.; Park, D.K.; Kim, S. Stroke Risk among Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Clinics (Sao Paulo) 2018, 73, e177. [Google Scholar] [CrossRef] [PubMed]
- Fekadu, G.; Chelkeba, L.; Kebede, A. Risk Factors, Clinical Presentations and Predictors of Stroke among Adult Patients Admitted to Stroke Unit of Jimma University Medical Center, South West Ethiopia: Prospective Observational Study. BMC Neurol. 2019, 19, 187. [Google Scholar] [CrossRef]
- Moczulska, B.; Kubiak, M.; Bryczkowska, A.; Malinowska, E. Pulse wave velocity as an early marker of diastolic heart failure in patients with hypertension. Pol. Merkur. Lekarski 2017, 42, 142–144. [Google Scholar]
- Shirwany, N.A.; Zou, M. Arterial Stiffness: A Brief Review. Acta Pharmacol. Sin. 2010, 31, 1267–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, S.S.; Gustin, W.; Wong, N.D.; Larson, M.G.; Weber, M.A.; Kannel, W.B.; Levy, D. Hemodynamic Patterns of Age-Related Changes in Blood Pressure. The Framingham Heart Study. Circulation 1997, 96, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated Aortic Pulse Wave Velocity, a Marker of Arterial Stiffness, Predicts Cardiovascular Events in Well-Functioning Older Adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.U.; Pfeffer, M.A.; Glynn, R.J.; Mitchell, G.F.; Taylor, J.O.; Hennekens, C.H. Increased Pulse Pressure and Risk of Heart Failure in the Elderly. JAMA 1999, 281, 634–639. [Google Scholar] [CrossRef]
- Pereira, T.; Correia, C.; Cardoso, J. Novel Methods for Pulse Wave Velocity Measurement. J. Med. Biol. Eng. 2015, 35, 555–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janić, M.; Lunder, M.; Šabovič, M. Arterial Stiffness and Cardiovascular Therapy. Biomed. Res. Int. 2014, 2014, 621437. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Huang, C.; Wong, K.S.; Chen, X.; Gao, Q. A New Method for Cerebral Arterial Stiffness by Measuring Pulse Wave Velocity Using Transcranial Doppler. J. Atheroscler Thromb. 2016, 23, 1004–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wentland, A.L.; Grist, T.M.; Wieben, O. Review of MRI-Based Measurements of Pulse Wave Velocity: A Biomarker of Arterial Stiffness. Cardiovasc. Diagn. Ther. 2014, 4, 193–206. [Google Scholar] [CrossRef]
- Wen, B.; Tian, S.; Cheng, J.; Li, Y.; Zhang, H.; Xue, K.; Zhang, Z.; Fan, Y.; Wu, B. Test-Retest Multisite Reproducibility of Neurovascular 4D Flow MRI. J. Magn. Reson. Imaging 2019, 49, 1543–1552. [Google Scholar] [CrossRef]
- Rivera-Rivera, L.A.; Cody, K.A.; Eisenmenger, L.; Cary, P.; Rowley, H.A.; Carlsson, C.M.; Johnson, S.C.; Johnson, K.M. Assessment of Vascular Stiffness in the Internal Carotid Artery Proximal to the Carotid Canal in Alzheimer’s Disease Using Pulse Wave Velocity from Low Rank Reconstructed 4D Flow MRI. J. Cereb. Blood Flow Metab. 2021, 41, 298–311. [Google Scholar] [CrossRef]
- Rivera-Rivera, L.A.; Schubert, T.; Turski, P.; Johnson, K.M.; Berman, S.E.; Rowley, H.A.; Carlsson, C.M.; Johnson, S.C.; Wieben, O. Changes in Intracranial Venous Blood Flow and Pulsatility in Alzheimer’s Disease: A 4D Flow MRI Study. J. Cereb. Blood Flow Metab. 2017, 37, 2149–2158. [Google Scholar] [CrossRef]
- Barth, M.; Breuer, F.; Koopmans, P.J.; Norris, D.G.; Poser, B.A. Simultaneous Multislice (SMS) Imaging Techniques. Magn. Reson. Med. 2016, 75, 63–81. [Google Scholar] [CrossRef]
- Glover, G.H. Phase-Offset Multiplanar (POMP) Volume Imaging: A New Technique. J. Magn. Reson. Imaging 1991, 1, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Pollock, S.; Whelan, B.; Keall, P.; Kim, T. Dynamic Keyhole: A Novel Method to Improve MR Images in the Presence of Respiratory Motion for Real-Time MRI. Med. Phys. 2014, 41, 072304. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Park, J.C.; Gach, H.M.; Chun, J.; Mutic, S. Technical Note: Real-Time 3D MRI in the Presence of Motion for MRI-Guided Radiotherapy: 3D Dynamic Keyhole Imaging with Super-Resolution. Med. Phys. 2019, 46, 4631–4638. [Google Scholar] [CrossRef] [PubMed]
- MRIcron Installation Page. Available online: https://people.cas.sc.edu/rorden/mricron/install.html (accessed on 11 September 2021).
- MATLAB—Mathworks. Available online: https://www.mathworks.com/products/get-matlab.html (accessed on 18 September 2021).
- Kröner, E.S.J.; van der Geest, R.J.; Scholte, A.J.H.A.; Kroft, L.J.M.; van den Boogaard, P.J.; Hendriksen, D.; Lamb, H.J.; Siebelink, H.-M.J.; Mulder, B.J.M.; Groenink, M.; et al. Evaluation of Sampling Density on the Accuracy of Aortic Pulse Wave Velocity from Velocity-Encoded MRI in Patients with Marfan Syndrome. J. Magn. Reson. Imaging 2012, 36, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Heidari Pahlavian, S.; Cen, S.Y.; Bi, X.; Wang, D.J.J.; Chui, H.C.; Yan, L. Assessment of Carotid Stiffness by Measuring Carotid Pulse Wave Velocity Using a Single-Slice Oblique-Sagittal Phase-Contrast MRI. Magn. Reson. Med. 2021, 86, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Smith, M.G.; Waye, K.P. Effects of Train Noise and Vibration on Human Heart Rate during Sleep: An Experimental Study. BMJ Open 2013, 3, e002655. [Google Scholar] [CrossRef] [Green Version]
- Van Velzen, M.H.N.; Stolker, R.J.; Loeve, A.J.; Niehof, S.P.; Mik, E.G. Comparison between Pulse Wave Velocities Measured Using Complior and Measured Using Biopac. J. Clin. Monit. Comput. 2019, 33, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Baek, H.J. A Comparative Study of Brachial–Ankle Pulse Wave Velocity and Heart–Finger Pulse Wave Velocity in Korean Adults. Sensors 2020, 20, 2073. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phantom | Human | |
|---|---|---|
| MRI (Coil Channel) | 3 T (12 ch.) | 3 T (12 ch.) |
| Scanning Sequence | 2D GRE | 2D GRE |
| TR (ms) | 20 | 16 |
| TE (ms) | 4 | 4.14 |
| FA (°) | 9 | 18 |
| Resolution (mm3) | 1.0 × 1.0 × 5.0 | 0.5 × 0.5 × 3.0 |
| Matrix size | 256 × 256 | 256 × 256 |
| Bandwidth (Hz/Px) | 320 | 315 |
| Sections | Transit Time (ms) | PWV (m/s) |
|---|---|---|
| 1 | 32.0 | 1.88 |
| 2 | 29.6 | 2.03 |
| 3 | 28.0 | 2.14 |
| 4 | 16.8 | 3.57 |
| 5 | 19.2 | 3.13 |
| Mean ± SD | 25.12 ± 6.71 | 2.55 ± 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-Y.; Lee, Y.-B.; Kang, C.-K. Novel Technique to Measure Pulse Wave Velocity in Brain Vessels Using a Fast Simultaneous Multi-Slice Excitation Magnetic Resonance Sequence. Sensors 2021, 21, 6352. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196352
Jung J-Y, Lee Y-B, Kang C-K. Novel Technique to Measure Pulse Wave Velocity in Brain Vessels Using a Fast Simultaneous Multi-Slice Excitation Magnetic Resonance Sequence. Sensors. 2021; 21(19):6352. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196352
Chicago/Turabian StyleJung, Ju-Yeon, Yeong-Bae Lee, and Chang-Ki Kang. 2021. "Novel Technique to Measure Pulse Wave Velocity in Brain Vessels Using a Fast Simultaneous Multi-Slice Excitation Magnetic Resonance Sequence" Sensors 21, no. 19: 6352. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196352