
Heart and Lung Sound Measurement Using an Esophageal Stethoscope with Adaptive Noise Cancellation


Abstract
:1. Introduction
1.1. Heart and Lung Sound Recording Techniques
1.2. Sound-Absorbing Materials
1.3. Adaptive Noise Cancellation
2. Materials and Methods
2.1. Microphone Case
2.2. Microphone
2.3. Processing Unit
2.4. System Software
3. Results
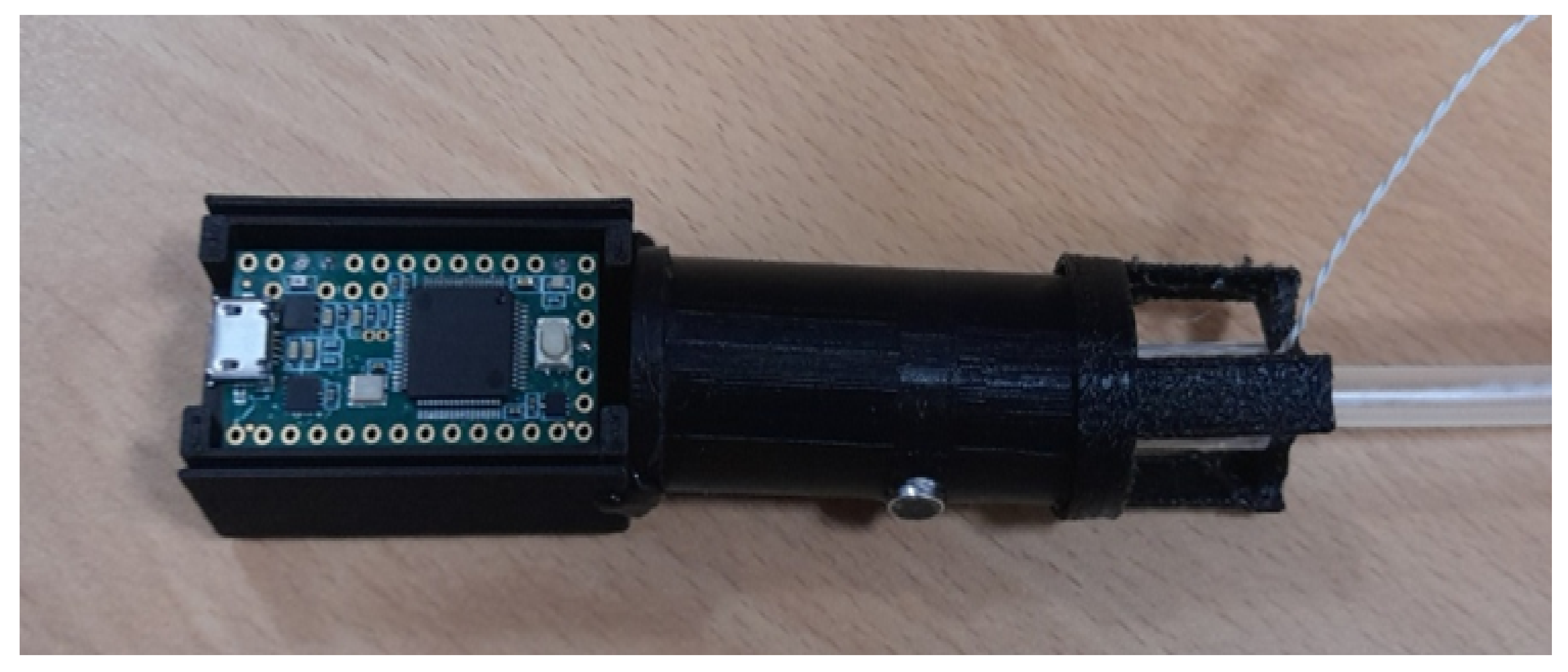
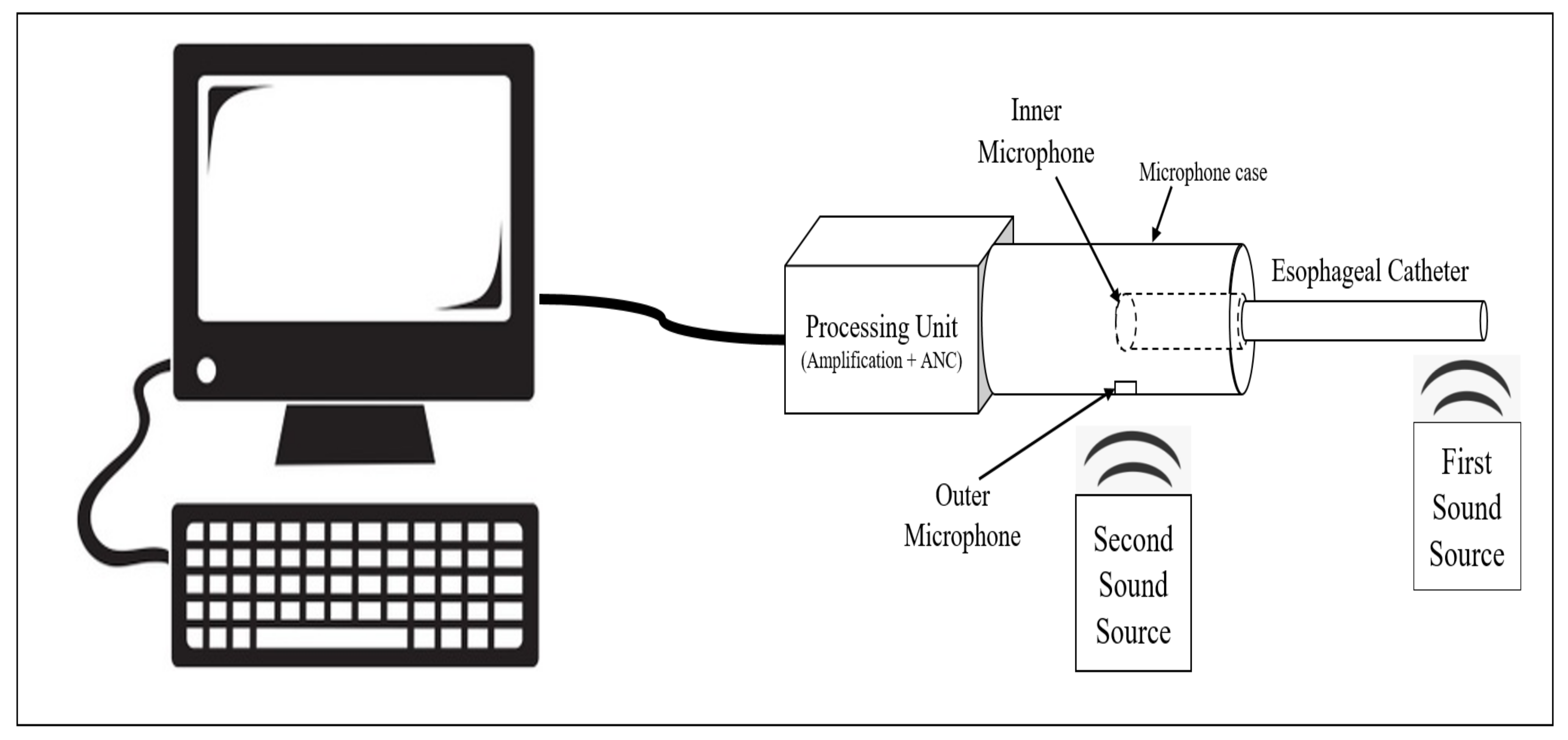
3.1. System Hardware
3.2. PDMS Microphone Case Results
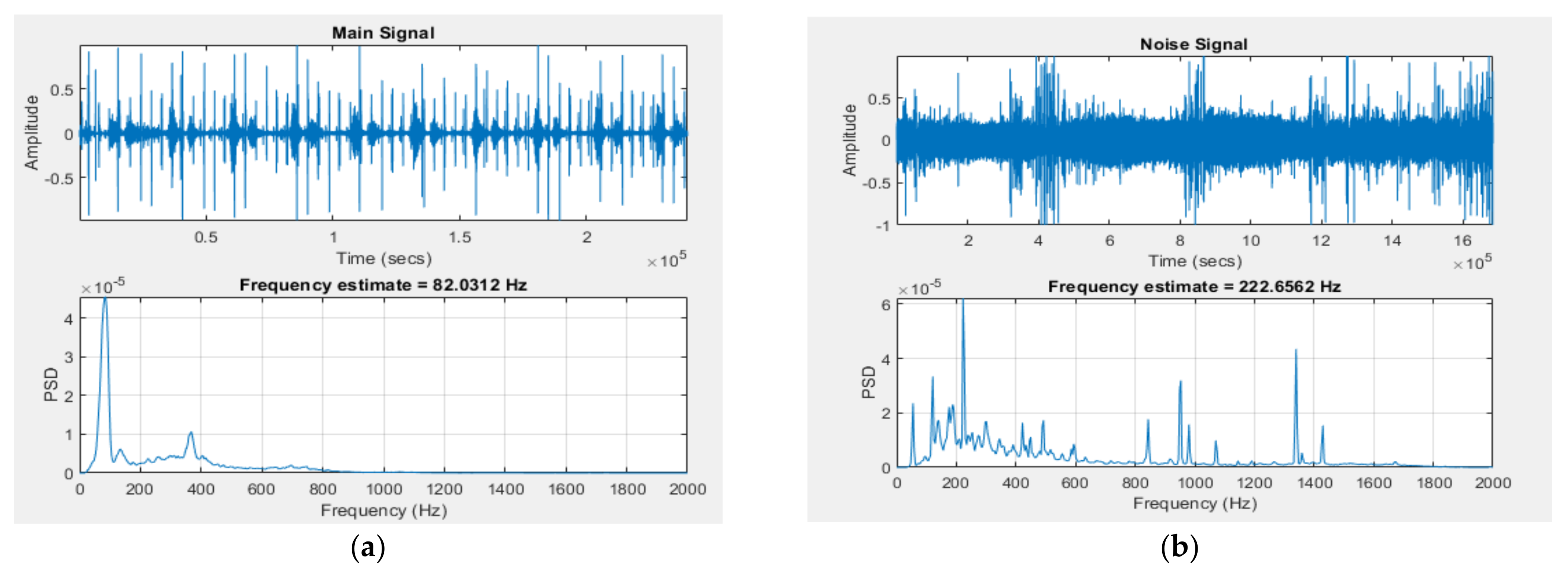
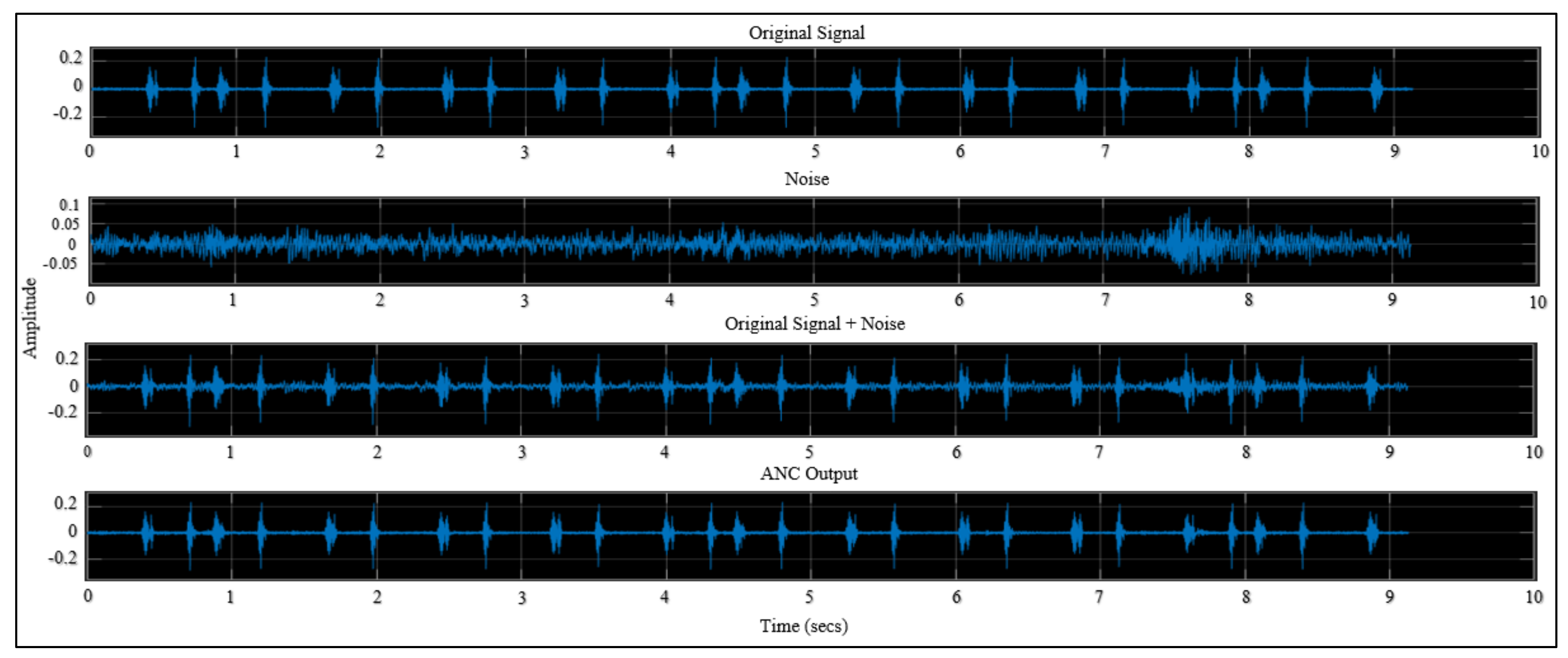
3.3. SIMULINK Model Results
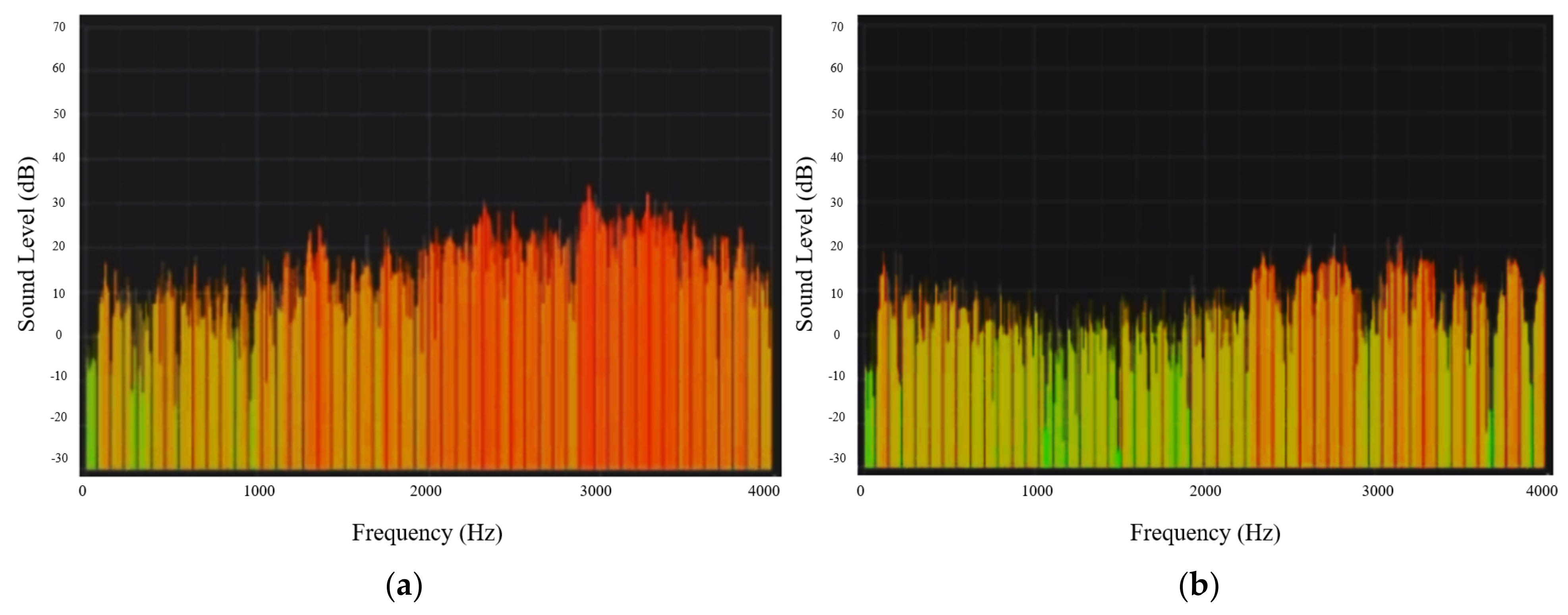
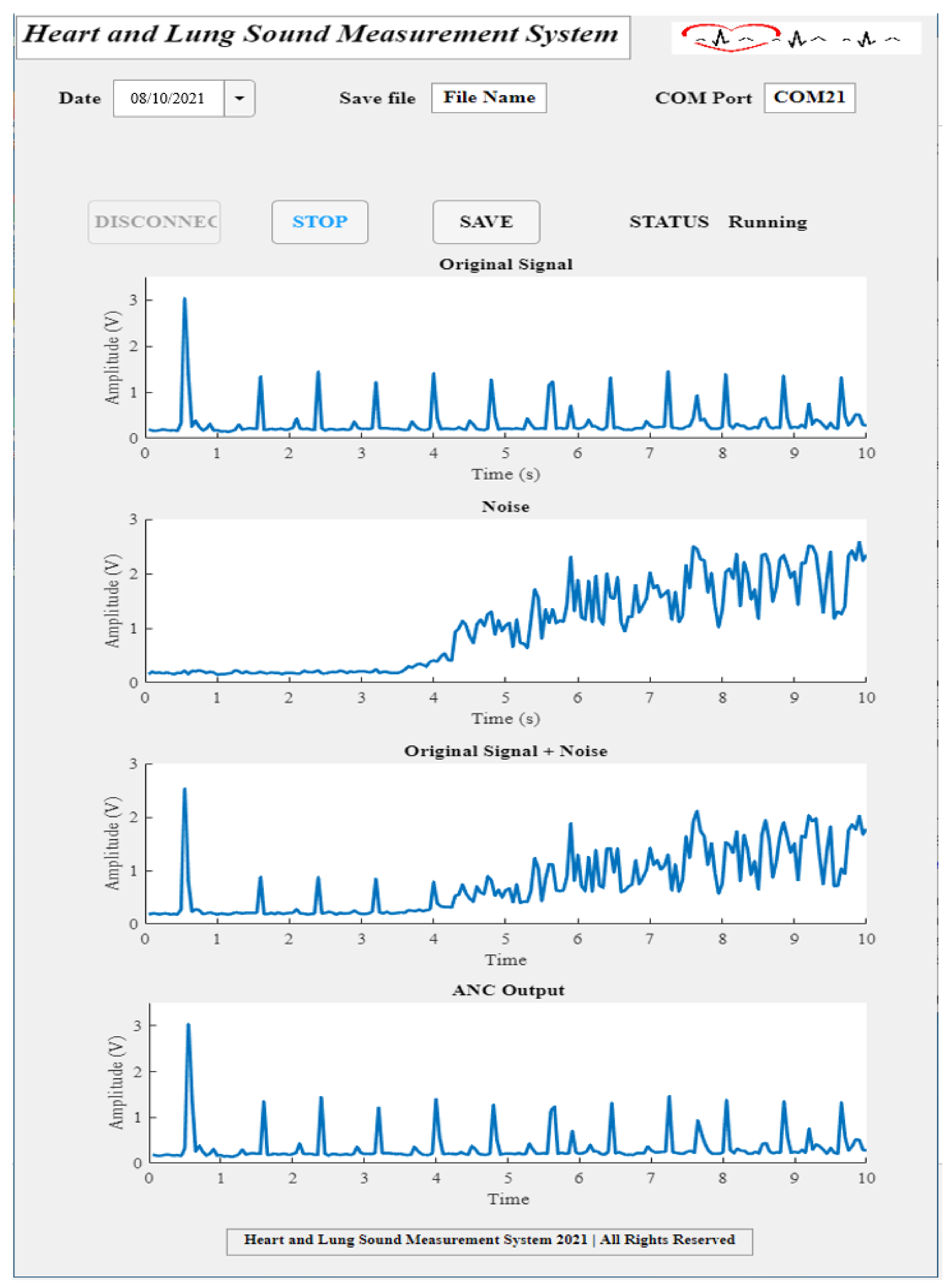
3.4. System Experimental Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rice, M.L.; Doyle, D.J. Comparison of phonocardiographic monitoring locations. In Proceedings of the 17th International Conference of the Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–23 September 1995; Volume 681, pp. 685–686. [Google Scholar]
- Shin, J.; Kim, Y.; Lim, S.; Cha, E.; Lee, T. Design technology in portable digital esophageal stethoscope. In Proceedings of the 7th International Conference on Networked Computing, Gumi, Korea, 26–28 September 2011; pp. 94–97. [Google Scholar]
- Moon, Y.J.; Bechtel, A.J.; Kim, S.H.; Kim, J.W.; Thiele, R.H.; Blank, R.S. Detection of intratracheal accumulation of thick secretions by using continuous monitoring of respiratory acoustic spectrum: A preliminary analysis. J. Clin. Monit. Comput. 2020, 34, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.J.; Kim, S.H.; Park, Y.S.; Kim, J.M.; Hwang, G.S. Quantitative Analysis of an Intraoperative Digitalized Esophageal Heart Sound Signal to Speculate on Perturbed Cardiovascular Function. J. Clin. Med. 2019, 8, 715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.S.; Moon, Y.J.; Kim, S.H.; Kim, J.M.; Song, J.G.; Hwang, G.S. Beat-to-Beat Tracking of Pulse Pressure and Its Respiratory Variation Using Heart Sound Signal in Patients Undergoing Liver Transplantation. J. Clin. Med. 2019, 8, 593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Moon, Y.J.; Kim, J.W.; Song, J.G.; Hwang, G.S. Prediction of Fluid Responsiveness by a Non-invasive Respiratory Systolic Time Interval Variation Using Heart Sound Signals in Recipients Undergoing Liver Transplantation. Transplant. Proc. 2017, 49, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Yao, D.; Xia, Y.; Zuo, K.; Yin, J.; Liang, H.; Zeng, Y.-P. The sound absorption properties of highly porous silicon nitride ceramic foams. J. Alloys Compd. 2020, 820, 153067. [Google Scholar] [CrossRef]
- Chen, W.; Hu, S.; Cao, H.; Huang, T.; Wu, X.; Lu, L.; Peng, J. Review on Research process of Sound reduction Materials. IOP Conf. Ser. Mater. Sci. Eng. 2019, 612, 052062. [Google Scholar] [CrossRef]
- Amares, S.; Sujatmika, E.; Hong, T.W.; Durairaj, R.; Hamid, H.S.H.B. A Review: Characteristics of Noise Absorption Material. J. Phys. Conf. Ser. 2017, 908, 012005. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Chen, J.; Hu, Y.; Jiang, Z.; Samjin, C. Heart Sound Measurement and Analysis System with Digital Stethoscope. In Proceedings of the 2009 2nd International Conference on Biomedical Engineering and Informatics, Tianjin, China, 17–19 October 2009; pp. 1–5. [Google Scholar]
- Gross, V.; Dittmar, A.; Penzel, T.; Schüttler, F.; von Wichert, P. The relationship between normal lung sounds, age, and gender. Am. J. Respir. Crit. Care Med. 2000, 162 Pt 1, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Varady, P. Wavelet-based adaptive denoising of phonocardiographic records. In Proceedings of the 2001 Conference 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey, 25–28 October 2001; Volume 1842, pp. 1846–1849. [Google Scholar]
- Jatupaiboon, N.; Pan-Ngum, S.; Israsena, P. Electronic stethoscope prototype with adaptive noise cancellation. In Proceedings of the 2010 Eighth International Conference on ICT and Knowledge Engineering, Bangkok, Thailand, 24–25 November 2010; pp. 32–36. [Google Scholar]
- Gordh, T. Heart-Volume Studies Iii. Phonocardiographic And Electrocardiographic Changes During Dilatation of The Heart In The Rabbit. Acta Anaesthesiol. Scand. 1964, 8, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.D. Noise in the operating room. Anesthesiology 2014, 121, 894–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, A.; Ouisse, M.; Dauchez, N. Silicone Foams for Sound Absorption: On the Link between Elaboration Parameters and Acoustic Performances; Research Gate: Mastricht, Holland, 2015. [Google Scholar]
- Atalla, N.; Amedin, C.; Atalla, Y.; Panneton, R.; Sgard, F. Development of New High Acoustical Performance Sound Absorbing Materials to Decrease Noise at Low Frequencies; Tech Rep A-370; IRSST: Montreal, QC, Canada, 2004. [Google Scholar]
- Haykin, S. Adaptive Filter Theory; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 1986. [Google Scholar]
- Lopez-Caudana, E. Active Noise Cancellation: The Unwanted Signal and the Hybrid Solution. Adapt. Filter. Appl. 2011, 49–84. [Google Scholar] [CrossRef] [Green Version]
- Thenua, R.A.J.; Agrawal, S.K. Hardware Implementation of NLMS Algorithm for Adaptive Noise Cancellation; Research Gate: Gwalior, India, 2010. [Google Scholar]
- Hadei, S. A family of adaptive filter algorithms in noise cancellation for speech enhancement. arXiv 2011, arXiv:1106.0846. [Google Scholar] [CrossRef] [Green Version]
- Quad, S.S. LM324, LM324A, LM224, LM2902, LM2902V, NCV2902. 2002. Available online: http://radioshop.by/datasheets/LM324-D.pdf (accessed on 6 September 2021).
- Kuo, S.M.; Morgan, D.R. Active noise control: A tutorial review. Proc. IEEE 1999, 87, 943–973. [Google Scholar] [CrossRef] [Green Version]
- Pelech, A.N. The physiology of cardiac auscultation. Pediatr. Clin. N. Am. 2004, 51, 1515–1535. [Google Scholar] [CrossRef] [PubMed]
- Mamorita, N.; Arisaka, N.; Isonaka, R.; Kawakami, T.; Takeuchi, A. Development of a Smartphone App for Visualizing Heart Sounds and Murmurs. Cardiology 2017, 137, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.; Tan, R.S.; Chai, K.T.; Wang, C.; Ghista, D.; Zhong, L. The electronic stethoscope. Biomed. Eng. Online 2015, 14, 66. [Google Scholar] [CrossRef] [Green Version]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
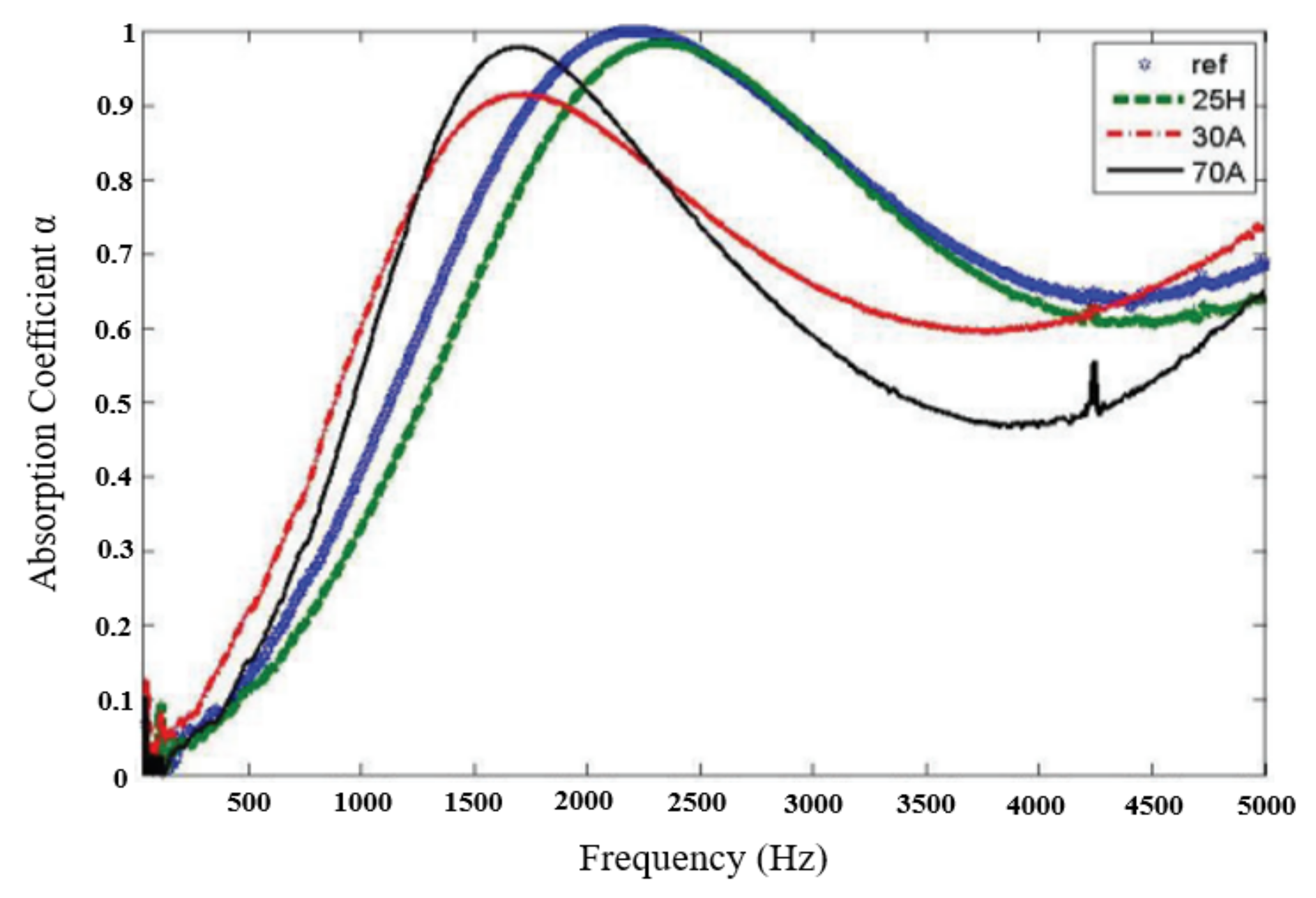
| Sample | % A | % B | Oil (% in Total Mass A + B) |
|---|---|---|---|
| ref | 50 | 50 | - |
| 30A | 30 | 70 | - |
| 70A | 70 | 30 | - |
| 5H | 50 | 50 | 5 |
| 25H | 50 | 50 | 25 |
| Parameter | Value | Unit |
|---|---|---|
| Directivity | Omni | - |
| Sensitivity | −38 ± 3 (12.6 mV/Pa) | dB |
| Standard operating voltage | 2 | Vdc |
| Max operating voltage | 10 | Vdc |
| Impedance | 2.2 | KΩ |
| Signal-to-noise ratio | >60 | dB |
| Frequency response | 15–16,000 | Hz |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed, N.; Kim, H.-S.; Kang, K.-M.; Mohamed, M.; Kim, S.-H.; Kim, J.G. Heart and Lung Sound Measurement Using an Esophageal Stethoscope with Adaptive Noise Cancellation. Sensors 2021, 21, 6757. https://0-doi-org.brum.beds.ac.uk/10.3390/s21206757
Mohamed N, Kim H-S, Kang K-M, Mohamed M, Kim S-H, Kim JG. Heart and Lung Sound Measurement Using an Esophageal Stethoscope with Adaptive Noise Cancellation. Sensors. 2021; 21(20):6757. https://0-doi-org.brum.beds.ac.uk/10.3390/s21206757
Chicago/Turabian StyleMohamed, Nourelhuda, Hyun-Seok Kim, Kyu-Min Kang, Manal Mohamed, Sung-Hoon Kim, and Jae Gwan Kim. 2021. "Heart and Lung Sound Measurement Using an Esophageal Stethoscope with Adaptive Noise Cancellation" Sensors 21, no. 20: 6757. https://0-doi-org.brum.beds.ac.uk/10.3390/s21206757